
Abstract
One of the major causes of erectile dysfunction (ED) is an endothelial vascular disorder. This meta-analysis is performed to determine the efficacy of aspirin on erectile function in men with vasculogenic ED. For this purpose, CENTRAL, MEDLINE, and reference lists of articles up to November 2019 were searched. Randomized controlled trials (RCTs) were selected that compared aspirin with placebo in men of any ethnicity with vasculogenic ED. A total of 58 trials were retrieved. Finally, two trials of 214 men fulfilled our selection criteria. High selection and detection bias were identified for one trial. The participants showed a significant improvement in erectile function when they took aspirin (mean difference: 5.14, 95% CI [3.89, 6.40], and I2 = 0%). Although the present meta-analysis suggested that aspirin has a significant effect on the improvement of erectile function, there were limited RCTs available on this topic and doses of aspirin varied. Additional studies are needed to support findings from this meta-analysis. Aspirin needs to be considered by practitioners when prescribing drugs for vasculogenic ED.
Background
Erectile dysfunction (ED), the most common sexual dysfunction in men, is defined as the inability to achieve or maintain an erection adequate for intercourse (Yafi et al., 2016). ED is caused by psychogenic and organic factors. Organic causes explain up to 80% of ED cases. Organic ED encompasses neurogenic, endocrinologic, vasculogenic, and medication or substance-induced factor. Vasculogenic ED is mostly caused by arterial or inflow disorders, rarely by venous outflow disorders, and is the most prevalent among all cases of organic ED (Ende, 1990).
The process of achieving and sustaining an erection is regulated by various molecules released on sexual stimulation. Nitric oxide (NO) released from nerves in the corpora cavernosa is one of these important molecules (Ralph, 2005). NO diffuses into the smooth muscle cells of cavernosa and increases the concentration of cyclic guanosine monophosphate (cGMP) in these cells (Francis et al., 2010). The high levels of cGMP then relax the musculature by decreasing calcium ion concentrations in these smooth muscle cells (Ghalayini, 2004). This whole mechanism increases blood flow and entraps more blood in penile tissues, hence strengthening the hydrostatic skeleton of the penis for an erection (Dean & Lue, 2005). However, the erection is affected by cGMP deactivation due to a cGMP specific phosphodiesterase (PDE) type 5 enzyme expressed abundantly in the cavernosa. Therefore, PDE5 inhibitors are the most widely used and effective group of medicines (e.g., sildenafil, avanafil, tadalafil, vardenafil) for the treatment of ED (Rosen & Kostis, 2003).
The NO pathway has other important functions in the body, such as preventing platelet aggregation, an increase in reactive oxygen species, ischemia, reperfusion injury, hypertension, and heart failure (Ahluwalia et al., 2016; Raddino et al., 2007). Cardiovascular diseases (CVDs) have a strong correlation with reduced NO production in the body, and hence with ED. The onset of ED is considered a sign of the onset of vascular diseases (Mobley et al., 2017). Most conventional medicines (diuretics, adrenergic antagonists, and calcium blockers) for CVD may aggravate ED (Chang et al., 1991; Simonsen, 2002).
Common factors for decreased bioavailability of NO in the body are old age, poor diet (namely, vitamin C deficient and arginine and fat-rich contents), oxidative stress, disease (e.g., sepsis, CVD, and nephropathies), sedentary lifestyle, and side effects from medications (e.g., antidepressants; Luiking et al., 2010; Raddino et al., 2007; Razny et al., 2011; Saroukhani et al., 2013). Conventional medicines and methods used for the treatment of ED are expensive (Tan, 2000), often unavailable in certain conservative countries or need a physician’s prescription, and may not be suitable for CVD patients, who may adversely interact with the treatments they are given (Herschorn, 2003; Simonsen, 2002). Conventional medicines for ED need to be taken before every sexual intercourse to ensure effective concentrations of the drug reach the penile vasculature through circulation (Huang & Lie, 2013). There is a dire need to identify a less expensive, easily available, and effective drug to treat vasculogenic ED.
In this regard, aspirin is a medicine available over the counter, is less expensive, and with negligible, minor, and rare side effects; it also has the potential to treat vasculogenic ED along with CVD (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013; Taubert, 2008). Aspirin increases blood flow in the vessels by not only inhibiting platelet aggregation activity but also by directly stimulating the activity of endothelial NO synthase to increase the production of NO for smooth muscle relaxation (Dzeshka et al., 2016). Previous studies reported an improvement in erectile function in men and animal models when cases of vasculogenic ED were treated with aspirin. The aim of this meta-analysis is to report the effect of aspirin on the improvement of erectile function.
Methods
The present meta-analysis was conducted by following the Cochrane Handbook for Systematic Reviews of Interventions. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) was used to evaluate the quality of the evidence (Guyatt et al., 2008).
Search Strategies
The Cochrane Central Register of Controlled Trials (CENTRAL; Issue 11, 2019) and MEDLINE (November 21, 2019) were searched using the terms “aspirin,” “erectile dysfunction,” and “sex.” The reference list of the selected studies and review articles were also screened to find unpublished or unidentified trails. Ongoing trials were located via the World Health Organization’s International Clinical Trials Registry Platform (ICTRP; http://www.who.int/ictrp/en/ and www.clinicaltrials.gov).
Eligibility Criteria
Randomized control trials (RCTs) published in English that compared the efficacy of standardly prescribed oral dosage of aspirin against placebos for the treatment of ED were selected. Sexual function was assessed by using a physician-assisted or self-administered International Index of Erectile Function (IIEF) questionnaire.
Study Selection
The titles and abstracts of articles were screened. The full text was subsequently screened if the article met the eligibility criteria. The eligibility of the studies was assessed independently by the authors, who documented the reasons for exclusion. Any disagreement regarding the study selection was resolved by discussion.
Data Extraction
Information of the author, year of the study, region where the study was conducted, characteristics of the subjects (age and ethnicity), methodology (number of participants and duration of follow-up), and occurrence of related adverse events was independently collected from the eligible studies using a form by the authors. The predefined primary outcome was the IIEF score of erectile function, whereas the secondary outcomes related to adverse events.
Risk of Bias Assessment
The risk of bias in RCTs was assessed using Review Manager 5.3 software (RevMan 2014) based on the randomization method, blinding, allocation concealment, blinding of outcome assessors, completeness of outcome data, the selectivity of outcome reporting, and other biases. The risk of bias was categorized as “high,” “low,” or “unclear.” Any disagreement was resolved by discussion.
Statistical Analyses
The treatment effect was calculated as mean differences (MDs) with 95% confidence intervals (CIs) for RCTs. Heterogeneity was assessed and reported using the random-effect model. It was first assessed at face value by comparing populations, settings, interventions, outcomes, and then by using the I² statistic. It was then interpreted according to the Cochrane Handbook for Systematic Reviews of Interventions (0%–40% = might not be important, 30%–60% = moderate heterogeneity, 50%–90% = substantial heterogeneity, and 75%–100% = considerable heterogeneity; Higgins, 2019).
A sensitivity analysis was performed to investigate the impact of risk of bias for sequence generation and allocation concealment of the included studies. If there were sufficient studies, we intended to construct funnel plots to assess the possibility of reporting bias, small study biases, or both.
Grading the Quality of Evidence
The GRADE approach was used to assess the quality of the evidence for the primary and secondary outcomes. The quality was classified as “very low,” “low,” “moderate,” or “high” based on the presence of risk of bias, inconsistency, indirectness, imprecision, and publication bias. GRADEpro software was used to visualize the quality of the evidence for each individual outcome, and the assessment was compiled with a Summary of Findings (SoF) table (GRADEpro 2014).
Results
Study Selection
A total of 58 studies were retrieved by searching electronic databases and screening the references of the retrieved studies. After removing duplicates, a total of 41 records were screened by their titles and abstracts. Finally, the full texts of two RCTs were assessed (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013; Figure 1).
Characteristics of the Included Studies
The RCTs (n = 2) had a total of 214 men. One of the RCTs was supported by educational grants (Saroukhani et al., 2013). The other did not receive any funding (Bayraktar & Albayrak, 2018). Table 1 summarizes the characteristics of the included trials.
Characteristics of Included Randomized Control Trials.

Note. BAD: bipolar affective disorder; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders-IV-Text Revision; dBP: diastolic blood pressure; ED: erectile dysfunction; IIEF: International Index of Erectile Function; MPV: mean platelet volume; PSV: peak systolic velocity; sBP: systolic blood pressure; SEP: sexual encounter profile; RCT: randomized control trial; VED: vasculogenic erectile dysfunction.
Participants
One of the RCTs was conducted on men (18–76 years old) with vasculogenic ED (Bayraktar & Albayrak, 2018), while the other included men (20–45 years old) that had developed vascular ED due to lithium carbonate therapy for the bipolar affective disorder (Saroukhani et al., 2013). None of the trials mentioned the setting from which the participants were recruited. The trials reported a total of 10 dropouts that did not follow up or violated protocol. The included trials randomized participants into two groups: placebo (control) and aspirin (intervention; Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
Intervention
Participants in the two RCTs were randomized into intervention and control groups. One of the RCTs used aspirin as intervention drugs through a 100 mg daily dose (Bayraktar & Albayrak, 2018), while the other prescribed an 80-mg dose three times a day (Saroukhani et al., 2013). The placebo group was treated similarly with tablets made of starch, containing the same appearance, taste, and ingredients as the aspirin tablets except for acetylsalicylic acid. Both trials assessed the outcomes after 6 weeks of intervention (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
Outcomes
The RCTs reported erectile function as the primary outcome by using the IIEF questionnaire (Bayraktar & Albayrak, 2018). The questionnaire was completed by the participants (Saroukhani et al., 2013) or a physician (Bayraktar & Albayrak, 2018). An IIEF score of <25 denotes the presence of ED, and the men were grouped according to their scores: mild (17–25), moderate (11–16), or severe (1–10).
Quality of the Studies
An assessment of the risk of bias in the RCTs is presented in Figures 2 and 3. Figure 2 presents the proportion of trials assessed with a “low,” “high,” or “unclear” risk of bias for each indicator. Figure 3 presents the risk of bias indicators for individual trials.
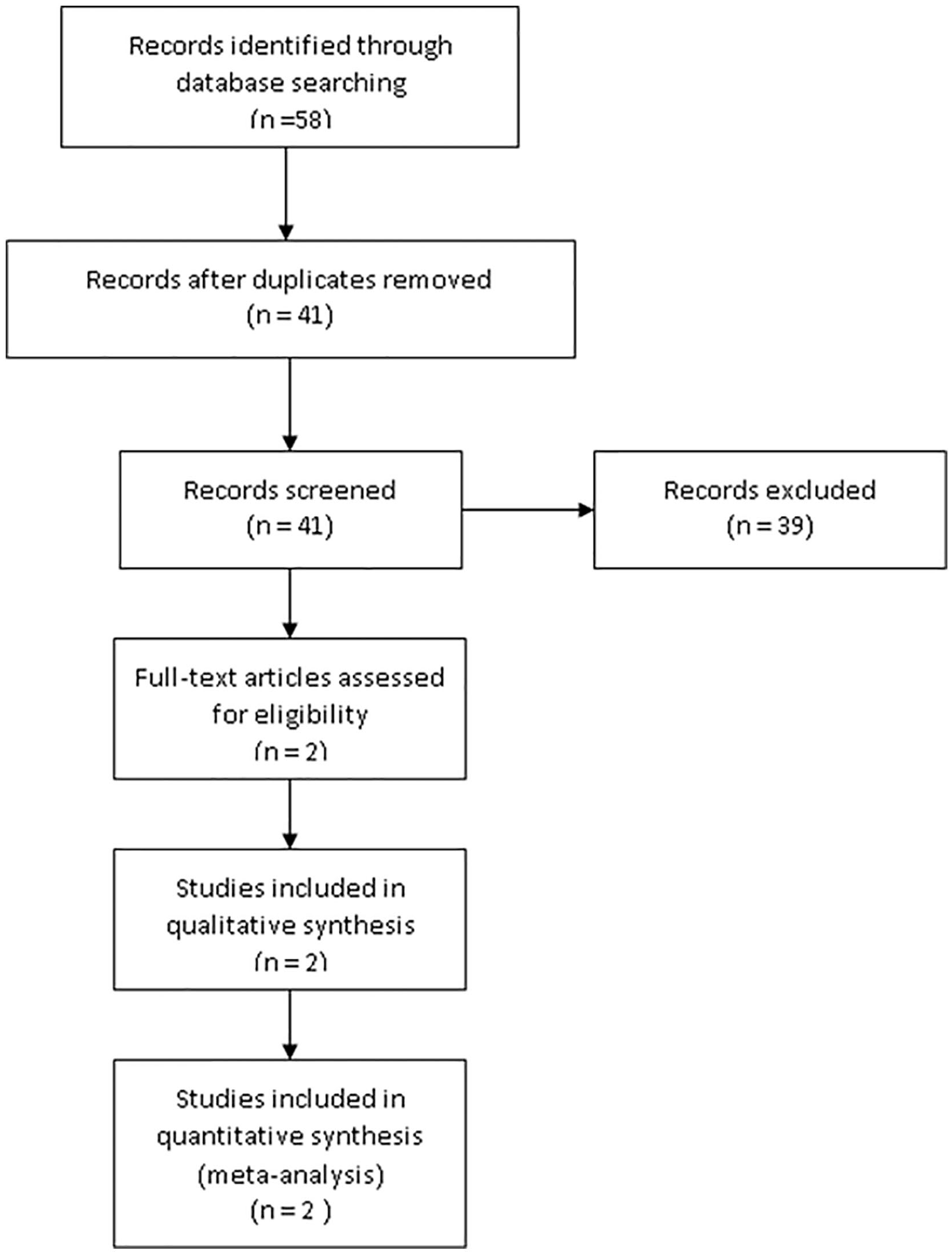
Flow chart of the study selection.

A graph of the risk of bias according to review authors’ judgments about each risk of bias item presented as percentages across all included studies.

A summary of the risk of bias according to review authors’ judgments about each risk of bias item for each included study.
Allocation
One of the trials randomized participants according to application order, which poses a high risk of bias (Bayraktar & Albayrak, 2018). The other trial conducted randomization through a computerized random number generator (Saroukhani et al., 2013).
Blinding
The placebo acted as a control group, and the person responsible for the participants’ care as well as the participants were blinded in both the RCTs, which were evaluated as having a low risk of blinding (Bayraktar & Albayrak, 2018). Placebo tablets were made of starch and with the same content as aspirin just without salicylic acid (Bayraktar & Albayrak, 2018). They were the same in appearance and taste as aspirin (Saroukhani et al., 2013). The outcome assessment of erectile function was done by using an IIEF questionnaire in a self-administered or interviewer-administered manner (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
Incomplete Outcome Data
One of the RCTs mentioned two dropouts (one from both the control and intervention groups) (Saroukhani et al., 2013), while the other reported six dropouts (four from the intervention and two from the control group) because they did not follow up (Bayraktar & Albayrak, 2018). One of the trials also reported two dropouts from the intervention group due to protocol violations (Bayraktar & Albayrak, 2018). The rate of withdrawal was low for both trials (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013) but differed between the intervention (two dropouts) and control (two dropouts) groups in one of the trials (Bayraktar & Albayrak, 2018).
Selective Reporting
Both trials reported the outcomes as specified in their methods section (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013). One of the trials was registered in the Iranian Registry of Clinical Trials (Saroukhani et al., 2013), while no information on registration was given in the other trial (Bayraktar & Albayrak, 2018). No other potential sources of bias were detected.
Efficacy in the Form of Erectile Function
RCTs
The effect sizes and CIs of the comparisons of aspirin for erectile function are presented in Figure 4 (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013). The pooled mean effect size was 5.14 (95% CI [3.89, 6.40]). The I2 statistic was 0%. Participants who received aspirin saw a significant improvement in erectile function compared to those receiving placebo for 6 weeks.

Individual and pooled effect size (mean difference and confidence intervals) of erectile function in men treated with aspirin compared to placebo according to the random-effect model.
Adverse Events
Adverse events reported in the RCTs were dyspepsia, abdominal burning, constipation, increased appetite, drowsiness, dizziness, tremors, nervousness, restlessness, skin rashes, and urinary retention with the use of aspirin. The frequency of the side effects did not differ between the two treatment groups. These events were mostly mild and did not affect the patients’ participation or completion of the studies (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
Sensitivity Analysis
For erectile function, there was no substantial change in the effect size and CI after removing the trial with a high or unclear risk of bias from the analysis.
Quality of the Evidence
The overall quality of the evidence was moderate (Table 2). The risk of bias was considered serious as one of the trials randomized in order of application and had allocation concealment bias. The impression was also considered serious due to small sample size in the trials. However, the inconsistency, indirectness, and publication bias were not serious. The effect was considered large according to the GRADE guidelines.
Summary of Findings.

Explanations.
One study has high selection and detection risk of bias.
One study has a small sample size.
Discussion
A comprehensive literature review was performed for this meta-analysis to determine the efficacy of aspirin to treat vasculogenic ED. The literature was lacking since only two RCTs were available for the present meta-analysis. Although the findings were significant and of clinical importance, as only two RCTs were included in this meta-analysis, the results may not explain all causes of ED. Furthermore, the association between the dose concentrations of aspirin that were used in the RCTs was not reported.
The quality of the RCTs was judged by the authors, who decided after reading each of the included studies in detail and engaging in thorough discussion. The trials were judged as having a “low,” “unclear,” or “high risk” of bias in all aspects. The lack of information on random sequence generation in one of the included trials could lead to treatment effect bias in the study and subsequently on the review that was done (Bayraktar & Albayrak, 2018). Similarly, one of the studies posed detection bias in the analysis as blinding of the outcome assessment was not reported (Bayraktar & Albayrak, 2018). There was no apparent selection bias, but only one trial reported the method of allocation concealment (Saroukhani et al., 2013). However, the performance bias (blinding of participants and personnel), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other biases were low in the included RCTs (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
The heterogeneity among RCTs was very low among the studies (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013). The overall level of evidence contributing to this review was assessed using the GRADE approach and was of high quality. Both the RCTs showed a significant improvement in erectile function, and the pooled effect of the present meta-analyses of both the RCTs suggests that treating vasculogenic ED with standard dosages of aspirin was very effective compared to taking placebos.
The two included RCTs reported common adverse events such as dyspepsia, abdominal burning, constipation, increased appetite, drowsiness, dizziness, tremors, nervousness, restlessness, skin rashes, and urinary retention with the use of aspirin. The frequency of the side effects did not differ between the two treatment groups. These adverse events were mostly mild and did not affect the patients’ participation and completion of the studies (Bayraktar & Albayrak, 2018; Saroukhani et al., 2013).
Although this meta-analysis shows strong evidence that using aspirin may significantly improve erectile function, there have been a few animal-based and human population-based and hospital-based studies that have suggested that aspirin may have no effect on or may increase the odds of ED (Kupelian et al., 2013; Li et al., 2019; Patel et al., 2016; Shiri et al., 2006). There were only two RCTs available for the meta-analysis. This limits our intention to perform a subgroup analysis based on the dosage of aspirins. We have included RCTs only based on the hierarchy and quality of evidence that they can provide. We would suggest for well-designed RCTs in comparison to a placebo group along with consideration of the five domains of risk of bias in future trials. If new trials on aspirin are available, an updated review on the effectiveness of aspirin for vasculogenic ED in men is suggested.
Conclusion
The present meta-analysis was done to include all RCTs that reported the efficacy of aspirin for the treatment of vasculogenic ED in men. The analyses suggested that erectile function is significantly improved by the intervention of aspirin compared to the placebo group. The availability of a few RCTs suggests there is a need for further trials on the efficacy of aspirin for vasculogenic ED in men in comparison to the placebo group in double-blinded RCTs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.