
Abstract
Recent reviews and observational studies have reported that patients with prostate cancer (PCa) are at increased risk of mental health issues, which in turn negatively affects oncological outcomes. Here, we examine possible explanatory variables of mental distress in a population-based cohort of men who have undergone radical prostatectomy (RP). Data were derived from a Maritimes-Canada online survey assessing patient-reported quality of life outcomes between 2017 and 2019 administered to 136 men (47–88 years old, currently in a relationship) who have undergone RP for their PCa diagnosis. The primary outcome was a validated assessment of mental distress, the Kessler Psychological Distress Scale (K10). Urinary function was assessed using the International Prostate Symptom Score, and relationship satisfaction was assessed using the Dyadic Assessment Scale. A multivariate logistic regression assessed the contribution of urinary function, relationship satisfaction, age, multimorbidity, additional treatments, medication for depression and/or anxiety, and survivorship time. A total of 16.2% men in this sample screened positive for mental distress. The severity of urinary problems was positively associated with increased mental distress (OR = 4.79, 95% CI [1.04, 22.03]), while increased age (OR = 0.87, 95% CI [0.78, 0.97]), relationship satisfaction (OR = 0.14, 95% CI [0.3, .077]), and current medication for anxiety, depression, or both (OR = 0.09, 95% CI [0.02, 0.62]) were protective factors. Survivorship time, the presence of additional comorbidities, or PCa treatments were not identified to be statistically significant contributions to the fitted model. Here, we report that RP survivors are prone to presenting with increased mental distress long after treatment. Screening for mental distress during RP survivorship is recommended.
Keywords
Prostate cancer (PCa) is the most commonly diagnosed cancer among Canadian men and radical prostatectomy (RP) remains the gold standard treatment for localized disease in men with PCa (Canadian Cancer Statistics Advisory Committee, 2019; Isbarn et al., 2010; Milonas et al., 2017). Given the high survival rates among patients undergoing RP (10-year PCa-specific mortality-free survival rates exceed 90%), a greater emphasis has been placed on understanding survivorship issues such as incontinence and mental distress (Donovan et al., 2016; Eton & Lepore, 2002).
A recent systematic review of the association between depression and PCa has highlighted that patients with PCa are at an increased risk of depression, which in turn has been documented to negatively affect oncological outcomes (Fervaha et al., 2019; Linden et al., 2012). In a recent study from Atlantic Canada, male survivors of PCa had more than double the odds of screening positive for depression and anxiety compared to males without a history of cancer diagnosis throughout their lifetime (control), a difference that did not emerge when men who were diagnosed with any other form of cancer were evaluated (Ilie et al., 2020). Similar results were reported in a national (Canada) population sample of males with a history of PCa when they were compared to men who never had PCa in their lifetime (Moodie et al., 2020). These results point to the need to further investigate possible contributing factors to the presence of mental health issues among PCa survivors (Fervaha et al., 2019; Watts et al., 2014).
Comparative studies report that men treated with RP for localized PCa have more urinary problems than men of the same age without the disease, an issue that has been reported to contribute to short- and long-term poor quality of life among these survivors (Litwin et al., 1995; Matthew et al., 2018). Urinary incontinence, erectile disfunction, or both, are common side effects of RP (Frey et al., 2014; Ramsey et al., 2013). While the removal of the diseased prostate is highly effective, RP does not always lead to a stabilization of these common side effects following surgery, with numerous studies reporting negative effects of urinary incontinence, erectile disfunction, or both, on sexual intimacy and relationship satisfaction (Garos et al., 2007; Hedestig et al., 2005; Katz, 2007). Research indicates that men who undergo RP are younger and have fewer comorbidities (Frey et al., 2014; Moul, 2004). Married men who undergo RP and stay married throughout their PCa journey are reported to live longer than single counterparts (Huang et al., 2018). To what extent, however, these side effects and patient characteristics relate to the presence of mental health issues among survivors treated with RP remains largely unknown.
In this study, we examine the relationship between current mental distress and age, urinary function, multimorbidity, the presence of additional active treatments, survivorship time, current intake of prescribed medication for anxiety, depression, or both, and relationship satisfaction, in a population-based cohort of adult men from the Maritimes, Canada, who received RP for their PCa diagnosis.
Methods
Procedure
The study’s analytic sample was based on 146 adult males (currently in a relationship) who resided in the Maritime provinces of Canada (ages 47–88, median = 67). Participants completed a PCa quality of life survey (approximately 20 min) online between May 2017 and December 2019, and identified having received RP for their PCa diagnosis (either alone or with additional radiation therapy and/or hormonal therapy; Ilie, 2018). Participants were recruited in urology and radiation oncology clinics throughout the Maritimes, and during community-based PCa support groups. A letter was sent to the patients’ homes, which included the link to the online survey. The survey response rate was 68%, and while considered normative for such studies it may be subject to nonresponse bias (Boak et al., 2015). Data were collected using Research Electronic Data Capture (REDCap), an online web application provided at Nova Scotia Health Authority designed to support data capture for research studies (Ilie, 2018). The survey was completed in the clinics at recruitment or were accessed from home using personal electronic devices (e.g., computers, iPad, tablet, or smartphone). Eligibility criteria included history of localized PCa diagnosis, any age, race, relationship status, ethnicity, socioeconomic status, ability to understand, write, and read English, current residence in Maritimes Canada, and possession of an email address. The survey took approximately 15 min to complete and assessed quality of life issues associated with the history of a PCa diagnosis. Survey procedures were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained electronically from all study participants, and was recorded on REDCap. The project (1021455) was approved by the Research Ethics Board of the Nova Scotia Health Authority, in Halifax, Nova Scotia.
Measures
Mental Health
The primary outcome was the assessment of mental health using the Kessler Psychological Distress Scale (K10), a well-validated global measure of mental distress, based on depression and anxiety symptoms within the past month (Kessler et al., 2002, 2003). The K10 has been used to assess mental distress across multiple settings and populations, and has been translated into more languages than any other mental health tool. Many national population surveys have successfully adopted the K10, including in the United States, Canada, and Australia as it has been established as highly reliable and valid when compared to other tools for screening for mental health (Cornelius et al., 2013; Furukawa et al., 2003; Kessler et al., 2010; Oakley Browne et al., 2010). The K10 items demonstrated a Cronbach’s α of 0.88 and an ordinal α of 0.92, indicating a high level of internal consistency. The Cronbach’s α for the scale we obtained in our study was .90. The items were measured using a five-point Likert scale ranging from 1 (none of the time) to 5 (all of the time). Scores on K10 range between 10 and 50, with scores under 20 indicating good mental health, 20–24 indicating mild, 25–29 indicating moderate, and 30 and above indicating severe mental disorder (Kessler et al., 2002, 2010). A categorical variable was created and used in all analyses, where 0 indicated a score below 20 (good mental health) and 1 indicated a score of 20 or above (screening positive for the presence of mild, moderate or severe mental distress).
Predictors
Urinary function was assessed using the International Prostate Symptom Score (I-PSS) questionnaire (also referred to as the American Urological Association [AUA] Symptom Index) based on the answers to seven questions assessing urinary symptoms (incomplete emptying, frequency, intermittency, urgency, weak stream, straining, nocturia; DeLong and Buckley, 2013; Morey et al., 1998). Responses for each of the questions ranged from 0: not at all; 1: less than 1 in 5 times; 2: less than half the time; 3: about half the time; 4: more than half the time; to 5: almost always. Scores ranging from 8 to 35 were coded 1 to indicate moderate to severe urinary function; scores 7 and below were coded 0 to indicate asymptomatic to mild urinary symptoms. I-PSS has good validity and reliability (Cronbach’s α of .80), and it is used commonly for assessing urinary function among PCa patients and survivors (DeLong and Buckley, 2013; Okamura et al., 2009). The Cronbach’s α for the scale we obtained in our study was .82.
Relationship satisfaction was assessed using the validated Dyadic Adjustment Scale (Spanier, 1976). Scores ranged from 0 to 151. Scores below 97 indicate relationship dissatisfaction and were coded 0; scores 97 or above indicate relationship satisfaction and were coded 1 (Graham et al., 2006; Jacobson et al., 1987). The Cronbach’s α for the scale was reported as .80 (Cuenca Montesino et al., 2013); in the current study, the observed value we obtained for Cronbach’s α was .95.
Covariates
Age (years), survivorship time since diagnosis (months), the presence of additional treatments to RP for the PCa diagnosis (coded 1; absence of additional treatments, 0), the presence of comorbidities in addition to history of PCa (coded 1; absence of additional comorbidities, 0), and the presence of current prescribed medication for anxiety, depression, or both (coded 1; absence of additional comorbidities, 0).
Statistical Analysis
A power analysis using G*Power 3.1. software was performed to evaluate the adequate sample size for the analyses we proposed. The analysis was based on a recent report indicating that 28% and 18% of patients following RP had moderate and severe urinary problems, respectively (Borges et al., 2019; Johansson et al., 2011). To ensure our sample was adequate for identifying a significant association between urinary symptoms and the presence or absence of screening positive for mental distress, we calculated our power based on these respective percentages and obtained recommended sample sizes of 318 and 131, respectively. All analyses were performed with SPSS V25. A multivariate logistic regression analysis assessed the association between the stated predictors and covariates and current mental distress status. Prior to conducting the analysis, the assumptions of logistic regression were tenable. Cross-tab analyses were used to first assess the association between screening positive for mental distress and predictors. A missing variables analysis revealed that 6.8% of the mental distress outcome variable data were missing. Little’s MCAR test was not statistically significant (p = .35), indicating that data were missing at random. Listwise deletion reduced the analytical sample to 136.
Results
A total of 16.2% (n = 22) men in our sample scored positive for current mental distress. The mean age of men in this sample was 67.29 (SD = 7.03). Most men in this sample were educated, having completed a bachelor degree or more (87.5%, n = 119), reported being of white ethnicity (97.1%, n = 132; 2.9%, n = 4, identified as Latino/Hispanic/Mexican, Asian/Pacific Islander, Middle Eastern/Arab, and other), and their household income in the past year was over 70K (CAN) (52.9%, n = 72). Table 1 describes the predictors’ characteristics of the analytical sample by mental distress status.
Demographic characteristics by Mental Distress status among men treated with Radical Prostatectomy for PCa Diagnosis from the baseline cycle of the Soillse Prostate Cancer Quality of Life Maritimes Survey (2017–2019), n = 136.
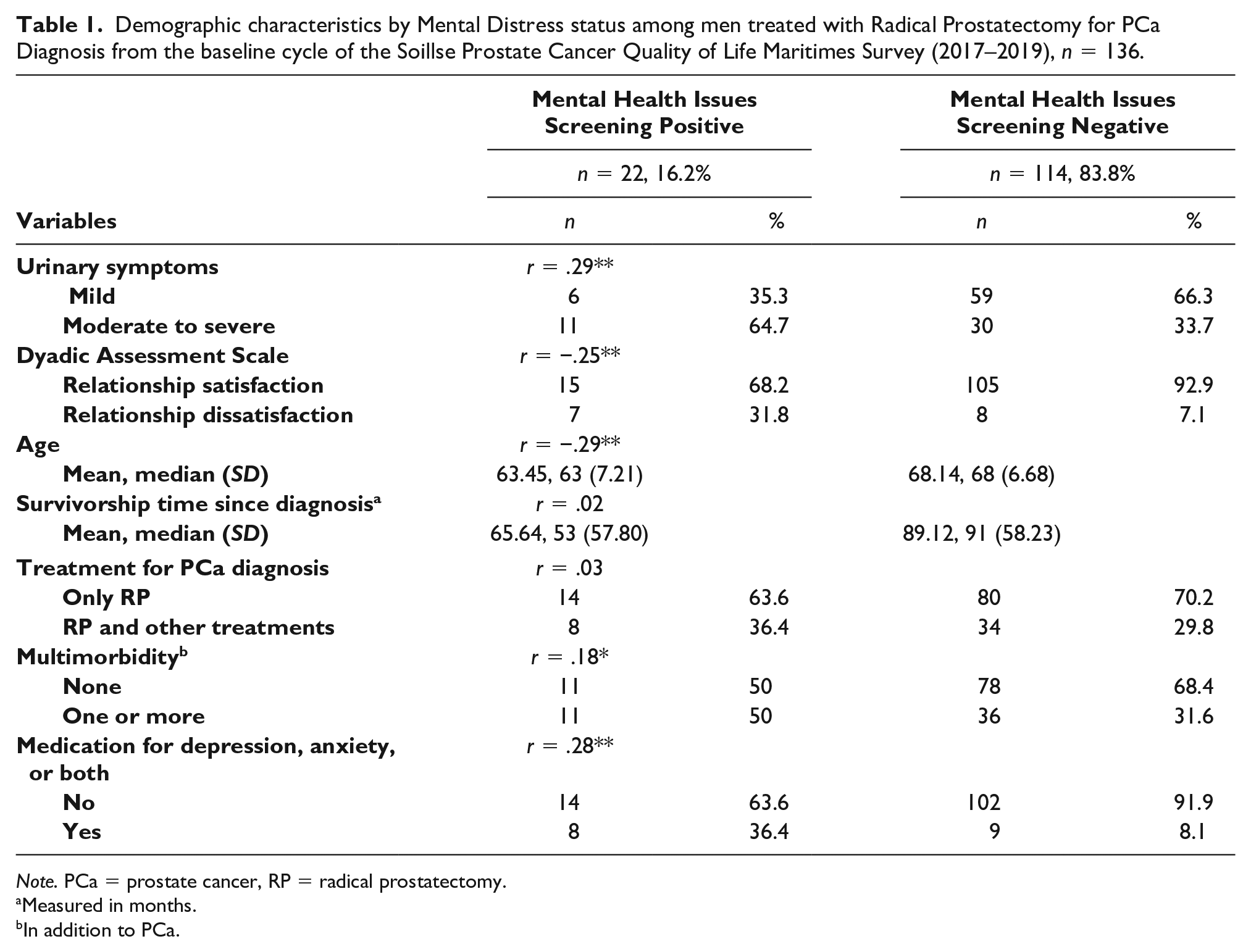
Note. PCa = prostate cancer, RP = radical prostatectomy.
Measured in months.
In addition to PCa.
The multiple logistic model was statistically significant, χ2(7) = 32.03, p < .001 indicating improvement over the null model. The Hosmer and Lemeshow test, χ2(8) = 8.22, p = .412, indicates a stable model with 86.7% correct cases classification (Nagelkerke R2 = 0.45; Cox and Snell R2 = 0.26). The odds ratio was 4.79 times higher (95% CI [1.04, 22.03]) for presenting with mental distress among survivors with moderate to severe urinary problems, compared to survivors with mild urinary problems (Wald χ2[1] = 4.05, p < .05), while the aforementioned variables were held constant. Older age (Wald χ2[1] = 6.75, p < .01) and relationship satisfaction (Wald χ2[1] = 5.13, p < .05) were protective factors for screening positive for mental distress by 0.87 (95% CI [0.78, 0.97]) and 0.14 (95% CI [0.03, 0.77]) for a one-unit increase, respectively. The presence of current intake of prescribed medication for anxiety, depression, or both (Wald χ2[1] = 5.99, p < .05) was also a protective factor (OR = 0.09; 95% CI [0.02, 0.62]). Survivorship time (Wald χ2[1] = 0.34, p > .05), multimorbidity (Wald χ2[1] = 0.59, p > .05), and additional treatments to RP for the PCa diagnosis (Wald χ2[1] = 1.65, p > .05) did not statistically significantly contribute to the fitted model.
Discussion
Advancements in RP over the past 20 years has led to increased survival but not without a cost given that patients are still at risk of surgical and postsurgical complications, which can lead to poor quality of life outcomes (Ku et al., 2009; Mooney & Mooney, 2011). Resent research identifies that men receiving active treatment for localized PCa are at a higher risk of developing mental health problems during survivorship compared to the general population or men with other forms of cancer (Fervaha et al., 2019; Ilie et al., 2020; Linden et al., 2012; Moodie et al., 2020). Research examining whether mental disorder is identified among RP survivors is scarce (Mooney & Mooney, 2011). In our study, 16% of RP survivors scored positive for mental disorder at the time of the survey. This percentage is comparable to that identified in the literature among PCa patients (Christie & Sharpley, 2014; Ilie et al., 2020; Moodie et al., 2020; Rice et al., 2018). Our results indicate that men who reported moderate to severe urinary problems had more than four times higher odds of screening positive for mental distress in this population. Older age, relationship dissatisfaction, and current intake of prescribed medication for anxiety, depression, or both were protective factors against screening positive for mental disorders. To our knowledge, this is the first study to examine the relationship between these predictors and a validated measure of mental distress in a PCa population of RP survivors. One study examining psychological distress over the span of 2 years since diagnosis in a sample of RP patients (n = 233) reported a higher rate of psychological distress (21%, 2 years postsurgery) among survivors than we report here. These researchers identified that among age, multimorbidity, urinary, bowel, and sexual functions, only improved bowel function emerged as a significant predictor of decreased psychological distress at 2 years (Occhipinto et al., 2019). Our results are not comparable to Occhipinto et al., given the different methodology, length of survivorship, and set of predictors. Results reported here unlike the study reported by Occhipinto et al. (2019) examined an older cohort of patients (7 years mean difference in the age of participants between the two studies) all of whom were in a relationship at the time they completed the survey. Other differences between the two studies include longer survivorship time (up to 5 years), control of survivorship time in the analyses, and inclusion of relationship satisfaction, the presence of additional treatments above RP, and the presence of current intake of medication for depression, anxiety, or both in the predictive model.
Voiding dysfunction, particularly incontinence, following RP has long been established as a major risk factor for depression (Pan et al., 2019), and results here support the existing evidence. Multidisciplinary treatment approaches determined by urologists, which include the expertise and training of pelvic floor physiotherapists or trained urodynamics nurses, are slowly becoming the treatment standard for urinary incontinence after RP (Strączyńska et al., 2019). More studies are emerging that support the effectiveness of pelvic floor muscle training as an effective treatment of urinary incontinence, after RP, even years after treatment, although randomized clinical trials in this area of research are scarce (Manassero et al., 2007; Strączyńska et al., 2019). It is possible that through the mechanism of pelvic floor training, men who improve their urinary function may also be preventing the emergence of mental health issues. Future studies assessing these causal pathways are warranted.
Younger survivors had higher odds of poor current mental distress compared to older survivors. These results may reflect the psychological impact of young age incontinence due to surgical side effects, alone or in combination with related side effects such as erectile dysfunction, which would be more impactful among younger compared to older men and may result in increased mental distress in the long term (Bill-Axelson et al., 2013; Eton & Lepore, 2002; Litwin et al., 1995).
Our results indicate that relationship satisfaction is a preventative factor of mental distress. This result is consistent with the literature (Ross et al., 2016). Previous research has identified that marital status and relationship satisfaction are both protective factors of mortality and poor quality of life, including certain aspects of mental health among PCa survivors (Bill-Axelson et al., 2013; Christie & Sharpley, 2014; Donovan et al., 2016; Eton & Lepore, 2002; Isbarn et al., 2010; Milonas et al., 2017; Occhipinto et al., 2019; Ross et al., 2016). To our knowledge, although important, there are no previous studies that have controlled for the presence or absence of current prescribed medication for anxiety, depression, or both, in studies examining mental health outcomes in this population.
In this study, we demonstrate that medication for depression, anxiety, or both is a protective factor against current mental distress. This is not surprising. Even though some men may reject the idea of seeking help for mental distress on the basis that it may be seen as a further sign of weakness, medication to help mitigate mental distress is usually effective (Donovan et al., 2016; Fervaha et al., 2019). Options for screening for mental distress should be made known to RP patients and survivors. It can be helpful to reassure men following RP that mental health interventions, if chosen, can help and may lead to better quality of life and improved health (Fervaha et al., 2019).
Though this study presents many insights into the PCa survivorship experience following RP, it is not without limitations. The cross-sectional, retrospective, and self-reported nature of the study are limitations, and data may be subject to recall bias. Causality cannot be inferred from the associative relationships examined here. The sample size was relatively small and survival bias may be a potential concern. Future studies of larger sample size using a mixed-method design may consider evaluating the contribution of ethnicity, the presence or absence of recurrence, and the interaction with other cancer diagnoses and/or comorbidities, which could play a significant role in the emergence of mental distress and mental health issues in this population.
Despite this study’s limitations, the insights gained from these data add a unique perspective to the existing body of literature about the contribution of urinary incontinence, age, relationship satisfaction, and the presence of current prescribed medication for anxiety, depression, or both for improving the psychological survivorship experience following RP.
Currently, there is a paucity of prospective data evaluating potential factors that contribute to the presence of increased mental distress among PCa patients, especially those treated with RP (Fervaha et al., 2019). Being able to identify contributing factors to the mental distress of this population is a priority and can help tailor care and patient education and empowerment programs in urology to assist those most in need during the cancer survivorship journey (Ilie et al., 2019). Regular mental distress screening during survivorship and treatment for urinary incontinence after RP for localized PCa may be warranted. Survivorship plans for PCa should consider incorporating the regular long-term collection of patient-reported outcomes and inform their plans with the science provided by the information given by the patients.
Footnotes
Acknowledgements
We would like to thank all participants who donated their time and their personal health history to this project, as well as clinicians who helped promote the survey to patients throughout the Maritimes. We thank the Dalhousie Research Medical Foundation (DMRF) and donors of the Soillse Research Fund for their support for prostate cancer quality of life research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data used in this research were made available by the Soillse Prostate Cancer Quality of Life Research Lab (GI), funded by the Dalhousie Research Medical Foundation (DMRF).