
Abstract
Low levels of health literacy are associated with poorer health outcomes. Both individual- and social-level factors have been identified as predictors of low health literacy, and men are known to have lower health literacy than women. Previous research has reported that men working in male-dominated occupations are at higher risk of accidents, injury, and suicide than other population groups, yet no study to date has examined the effect of gendered occupational contexts on men’s health literacy. The current article examined the association between occupational gender ratio and health literacy among Australian males. The Australian Longitudinal Study on Male Health (Ten to Men) was used to examine associations between occupational gender ratio (measured in Wave 1) and health literacy (measured in Wave 2) across three subscales of the Health Literacy Questionnaire. Multivariable linear regression analyses were used and showed that the more male dominated an occupational group became, the lower the scores of health literacy were. Results for the different subscales of health literacy for the most male-dominated occupational group, compared to the non-male-dominated group were: ability to find good health information, (Coef. −0.80, 95% CI [−1.05, −0.54], p < .001); ability to actively engage with health-care providers, (Coef. −0.35, 95% CI [−0.62, −0.07], p = .013); and feeling understood and supported by health-care providers, (Coef. −0.48, 95% CI [−0.71, −0.26],p = < .001). The results suggest the need for workplace interventions to address occupation-level factors as an influence on health literacy among Australian men, particularly among the most male-dominated occupational groups.
Background
In most countries across the world, the labor market is highly gender segregated by industry and occupation (Esping-Anderson, 2009; Klasen, 2017; WGEA, 2019). That is, women and men are unequally distributed across industries and occupations; some occupations may have a greater concentration of men relative to women and others may have more women relative to men. In Australia, women tend to be concentrated in the health-care and social assistance workforce as well as education and training, while men are concentrated in construction and manufacturing, mining, transport, agriculture, and fishing (WGEA, 2019).
There is evidence that health outcomes are patterned across occupational groups, with men working in male-dominated occupations at greater risk of poorer health outcomes and poorer health-related behavior. The evidence substantiating this is extensive and far reaching. In Australia, evidence from retrospective mortality studies (Milner et al., 2014; Milner and King, 2019) and a systematic review (Milner et al., 2013) has indicated that males employed in male-dominated occupations are at an elevated risk of suicide. Across the world, the construction industry is male dominated, and cohort data from male workers in the German construction industry identified an increased risk of fatal injuries and accidents compared to that for other workers (Arndt et al., 2004). In the United States, higher rates of hazardous health behaviors such as alcohol use and smoking were identified in a survey of male construction workers, compared to those of the general population (Strickland et al., 2017). Evidence from Finnish registry cohort data suggests that men employed in these occupations have lower use of antidepressants and report lower sickness absence than those in other occupational groups (Halonen et al., 2018). It is also known that men in male-dominated occupations are less likely than other men to see a mental health professional during times of emotional distress (Milner, King, et al., 2018a; Milner, Scovelle, et al., 2018b).
The patterning of health behaviors and outcomes in male-dominated occupations has been well described, but reasons for these associations are not clear. The concept of health literacy is important to consider when contextualizing health, health behaviors, and health-service engagement. Defined in numerous ways (see Sørensen et al., 2012 for a review), health literacy is commonly considered to represent a person’s knowledge, motivation, and competence to understand, appraise, access and apply health information in order to make judgments and decisions concerning health-care, disease prevention, and health promotion (Sørensen et al., 2012). Domains of health literacy include functional (e.g., education based on the communication of factual information on health risks and on how to use the health system), interactive (e.g., improving personal capacity to act independently on knowledge), and critical (e.g., cognitive and skills development outcomes that are oriented toward supporting effective social and political action as well as individual action) health literacy (Nutbeam, 2000).
Low levels of health literacy have been associated with a range of negative health outcomes including death and hospitalization due to cardiovascular disease (Fabbri et al., 2018), decreased use of preventative health services, reduced ability to correctly take medications and interpret health messages, and among the elderly, lower overall health status (Berkman et al., 2011), as well as increased lifestyle risk factors such as smoking and lack of physical activity (Adams et al., 2013).
Variations in health literacy have been observed across different groups in society. Previous research has indicated that low socioeconomic status, particularly low levels of education, is associated with reduced health literacy (Mantwill et al., 2015; Sørensen et al., 2015). Males have poorer health literacy compared to females (Clouston et al., 2017), and researchers have called for a greater focus on incorporating a gender lens in health literacy research (Peerson and Saunders, 2011).
Prior research indicates that greater conformity to masculine norms is associated with lower health literacy in men (Milner et al., 2019). Male-dominated work environments are settings in which masculine stereotypes are enacted and reinforced, in part because their occupational features shape expectations of heteronormative and masculine behaviors. Critically, the health literacy process of gathering, assessing, and using information for health occurs in the context of social, community, and workplace settings (Rowlands et al., 2015; Sørensen et al., 2012) and impacts on decisions made in these settings. This highlights the importance of considering occupational settings for assessing and building health literacy. While there is still much to learn about how gendered workplace expectations influence the health of men in male-dominated occupations, it is clear that workplaces offer a key setting for intervention. Further, there is evidence that workers are receptive to workplace interventions: Evaluations of a suicide prevention literacy program among construction workers indicated that men, particularly young men, believed that the workplace had a role in preventing suicide (King et al., 2019).
Despite a growing body of literature exploring the impact of occupational gender segregation on health outcomes for men, health literacy is rarely considered as a contributing factor, and indeed no previous study has examined differences in health literacy across gendered occupational groups. This is a critical gap, as understanding whether health literacy varies by occupational context may highlight opportunities to intervene in occupational settings to improve health literacy and ultimately improve health outcomes for men. The current study seeks to address this gap and examine health literacy among employed males. Drawing on a national longitudinal study of men’s health in Australia, the specific aim is to examine the extent to which occupational gender ratio is associated with three key components of health literacy: reported ability to find good health information, ability to actively engage with health-care providers, and feeling understood and supported by health-care providers. Based on prior evidence, it is hypothesized that as the gender ratio of males to females increases, there will be a decrease in reported health literacy.
Methods
Data Source
Data from Wave 1 (baseline) and Wave 2 (on average, 2 years post-baseline) of the Australian Longitudinal Study on Male Health (Ten to Men) were used. Ten to Men is a national longitudinal study of boys and men aged 10 to 55 years at Wave 1. The study contains data on a range of life domains, including demographic and socioeconomic characteristics, physical and mental health and well-being, health behaviors, and use and knowledge of health services. Sampling, recruitment, and data collection methods are described in detail elsewhere (Pirkis et al., 2017). Briefly, 104,884 households were contacted by fieldworkers at Wave 1. Successful contact was made with 81,400 households (78%), of which 33,724 (32 %) were confirmed to be potentially eligible for the study. Within these households, 45,510 eligible males were invited to participate, of whom 16,021 returned a Wave 1 survey and were included in the study (a response rate of 35%; Currier et al., 2016). Wave 1 was conducted between October 2013 and July 2014. Wave 2 was conducted between November 2015 and May 2016, with 76% of the original cohort participating. Ten to Men received approval from the University of Melbourne Human Research Ethics Committee and conformed to the principles embodied in the Declaration of Helsinki. All participants provided written consent. The flow of participants in the sample can be seen in Figure 1. The study was restricted to men aged between 18 and 55 years.

Sample selection. HLQ = Health Literacy Questionnaire.
Outcome Variable
Three scales of the Health Literacy Questionnaire (HLQ; Osborne et al., 2013) were included in the Ten to Men cohort in Wave 2. These scales are (a) Ability to find good health information (5 items, average inter-item covariance: 0.44, scale reliability coefficient: 0.94); (b) Ability to actively engage with health-care providers (5 items, average inter-item covariance: 0.53, scale reliability coefficient: 0.95); and (c) Feeling understood and supported by health-care providers (4 items, average inter-item covariance: 0.52, scale reliability coefficient: 0.91). Information on the development of the HLQ has been documented elsewhere (Osborne et al., 2013). Higher scores on each scale represent greater health literacy.
Exposure
Occupational Gender Ratio
Objective population data by occupation (ABS, 2016) were used to create a continuous measure representing a ratio of employed males to females across 44 occupations (i.e., the two-digit occupation codes of the Australian and New Zealand Standard Classification of Occupations; ABS, 2013). A categorical variable based on the ratio of males to females in an occupation was created: “not male-dominated occupation” (between 0.22 and 0.99 males to females), “slightly male-dominated” (1.00 to 1.11), “moderately male-dominated” (up to 2.48 males to females), “heavily male-dominated” (2.49 to 5.79), and “very heavily male-dominated” (5.80 males to females and greater). The occupations contained in each of these categories can be seen in supplemental Table S1.
In sensitivity analyses, a binary variable was created, dichotomizing occupational gender ratio: “not male-dominated occupation” (between 0.22 and 0.99 males to females) and “male-dominated” (1.00 or more males to females).
Covariatess
Variables that could be prior common causes of both health literacy and the occupational gender ratio were considered potential confounders, and included in models. All were measured at baseline and hence occurred prior to the reported outcome of health literacy (measured at Wave 2). These included age (18–24 years, 25–34 years, 35–44 years, 45–55 years), education (less than Year 12 [Year 12 is the highest year of secondary schooling in Australia], more than Year 12), relationship status (never married, widowed/divorced/separated but not divorced, married/de facto), country of birth (Australia or another), area of residence (metropolitan, inner regional, outer regional), and combined household income (scored from 1 representing $3,840 or more per week [$200,000 or more per year] to 12 representing $1–$189 per week [$1–$9,999 per year]). All confounders were analyzed as categorical variables, apart from income, which was assessed as a continuous variable.
Masculinity was considered as a potential prior cause of entry into a male-dominated occupation and health literacy. Analysis therefore controlled for conformity to masculine norms, using the Conformity to Masculine Norms Inventory (CMNI-22; Mahalik et al., 2003). Physical and Mental Health Component Summary scores of the SF-12 (SF-12; Ware et al., 2002) were included in the analysis, recognizing that baseline health status may affect both employment in certain types of jobs and a person’s reported health literacy.
Analysis
Multivariable linear regression analyses were conducted, regressing health literacy (Wave 2) on occupational gender ratio (Wave 1). These linear regression models, performed using the “regress” command in Stata, use the ordinary least squares (OLS) method to estimate the unknown parameters in linear regression models. OLS does this by minimizing the sum of the squares of the differences between observed and predicted outcome variables in the linear function.
The main exposure, the occupational gender ratio, was measured in Wave 1. Unadjusted models included exposures only (no confounders). Adjusted models including all confounders (measured in Wave 1) were then conducted. The Wald joint test of significance was used to test that the inclusion of the main exposure (the occupational gender ratio) in the model created a statistically significant improvement in the fit of the model. As noted earlier, a sensitivity analysis was conducted using a binary variable for occupational gender ratio (male dominated vs. non-male dominated).
Results
Average scores on the three health literacy variables in relation to the occupational gender ratio can be seen in Table 1. Across the three scales, there was a linear relationship between being in a male-dominated occupation and health literacy. The more male-dominated an occupation, the lower the score of health literacy. A description of the sample used in the study (across the three outcomes) can be seen in Table 2.
Mean of Three Scales From the Health Literacy Questionnaire by the Occupational Gender Ratio.
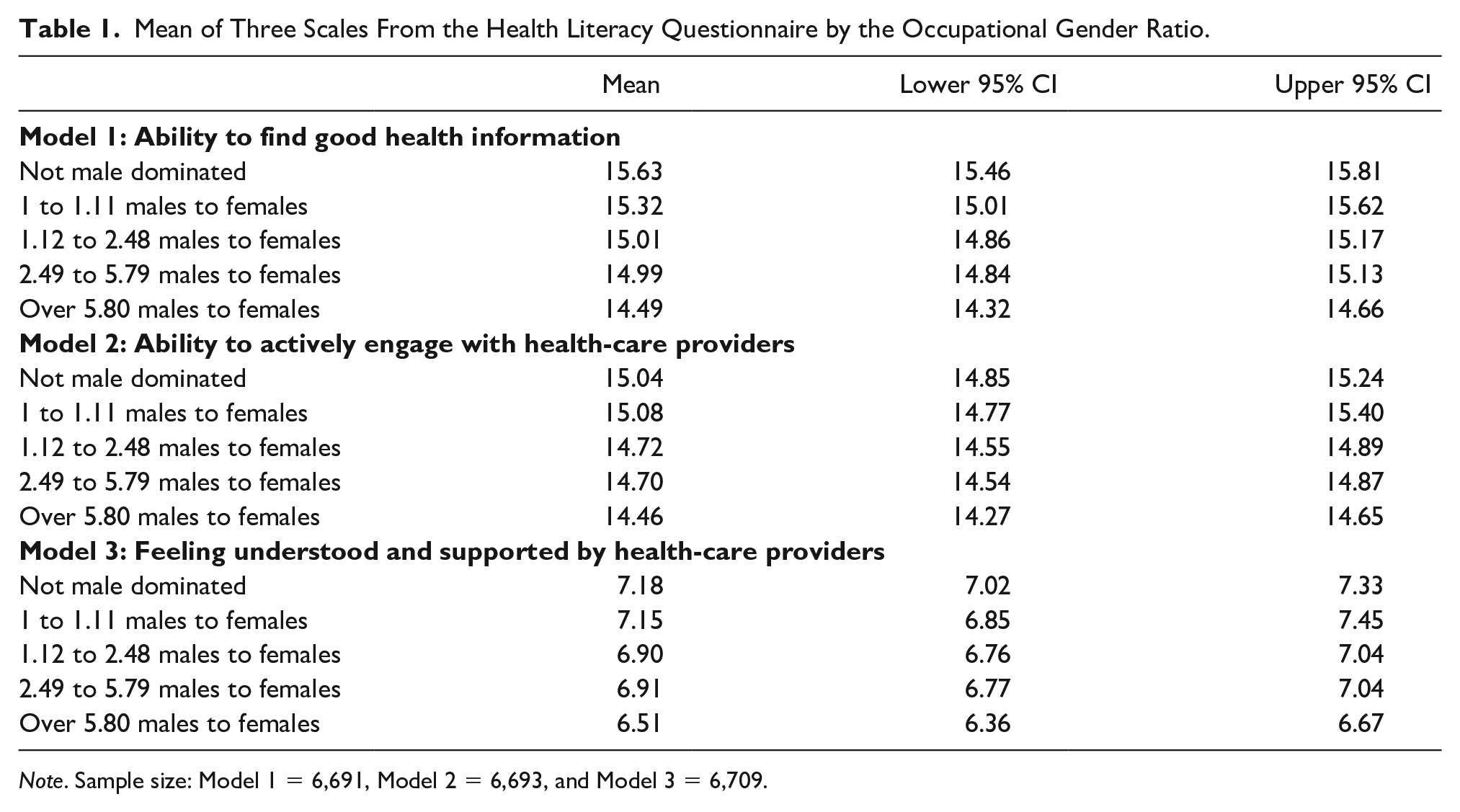
Note. Sample size: Model 1 = 6,691, Model 2 = 6,693, and Model 3 = 6,709.
Description of the Sample Used in the Three Analytic Models.

Note. Sample size: Model 1 = 6,691, Model 2 = 6,693, and Model 3 = 6,709. Note that income is analyzed as a continuous variable in the regression results, but categories are presented in the table. CMNI = Conformity to Masculine Norms Inventory; SF-12 = 12-item Short Form Survey.
Regression results can be seen in Table 3. For the adjusted results in Model 1 (ability to find good health information), being in a slightly male-dominated occupation (1 to 1.11 males to females) was associated with a decrease in health literacy (Coef. −0.57, 95% CI [−0.91, −0.23], p < .001) compared to being employed in a non-male-dominated occupation, the reference. There was a stepwise decrease in health literacy, with the greatest difference being observed for men in very heavily male-dominated occupations (over 5.80 males to females; Coef. −0.80, 95% CI [−1.05, −0.54], p < .001). A similar stepwise decrease in health literacy was observed for Model 3 (feeling understood and supported by health-care providers), but there was no difference between non-male-dominated occupations and the slightly male-dominated category. There was less evidence of a stepwise difference in Model 2 (ability to actively engage with health-care providers). However, the Wald test of significance supports the joint effect of significance for all three models. In sensitivity analysis, the binary variable representing “male-dominated” versus “non-male-dominated” occupations was significant for Models 1 (Coef. −0.35, 95% CI [−0.55, −0.15], p = .001) and 3 (-0.27, 95% CI [−0.45, −0.09], p = .003), and these effects were confirmed in the Wald test of joint significance. This binary gender occupational variable was not significantly associated with the “ability to actively engage with health-care providers” (Model 2), although results were in the same direction as the other two HLQ scales (Coef. −0.10, 95% −0.32 to 0.11, p = .348).
The Occupational Gender Ratio and Health Literacy Questionnaire, Adjusted and Unadjusted Models, and Regression Results.

Note. Adjusted models also include age, SF-12 (physical and mental health component summary scores), Conformity to Masculine Norms Inventory (CMNI-22), education, marital status, household income, country of birth, and region of residence. Sample size: Model 1 = 6,691, Model 2 = 6,693, and Model 3 = 6,709.
Discussion
These results highlight an association between gendered occupational contexts and health literacy among men, showing poorer health literacy among men employed in occupations where there are higher concentrations of other men. In particular, this study has identified that the more male dominated an occupational group is, the lower the health literacy scores across three domains: ability to find good health information, ability to actively engage with health-care providers, and feeling understood and supported by health-care providers. These three scales represent communicative and interactive health literacy and reflect the ability to extract information and derive meaning from different forms of health-related communication and to apply new information to changing circumstances (Sørensen et al., 2012). Importantly, the observed associations persisted, even after accounting for individually reported adherence to male gender norms (as measured through the CMNI-22), self-rated health, and a range of other social and economic circumstances.
Despite known associations between being in a male-dominated occupation and poorer health outcomes, it was previously not known whether men in male-dominated occupations have poorer health literacy than other groups of men. The results therefore highlight opportunities to intervene in occupational settings, particularly those that are male dominated, to improve health literacy, and ultimately improve health outcomes for men.
Our results indicating that men working in male-dominated occupations have poorer health literacy must be considered in the context of previous research that has demonstrated the effects of occupational gender ratio on mental health (Milner, King, LaMontagne, et al., 2018), suicide (Milner and King, 2019), and mental health service use (Milner, King, et al., 2018a; Milner, Scovelle, et al., 2018b). Other studies have suggested that health literacy is a mediator of the relationship between socioeconomic status and health outcomes (Stormacq et al., 2019). Therefore, improving the health literacy of individuals who are at risk of having both poorer health literacy and poorer health outcomes may offer a way to reduce inequities in health.
Given these results, it is important to consider the mechanisms through which occupational gender composition might impact health literacy specifically and poorer health outcomes more broadly. Gendered occupational contexts are thought to influence health literacy in two main ways: through selection into employment and through occupational features that shape and embed gender norms. Men who are working in male-dominated occupations may bring with them a unique set of risk factors that predispose them to poorer health literacy, including factors related to aspects of masculinity (e.g., the importance of emotional control and self-reliance) and other factors relating to childhood experiences (Bröder et al., 2017), employment history, education, and cultural factors (Rowlands et al., 2015).
Occupationally embedded gender norms may contribute to men’s poorer health literacy by discouraging engagement with health providers (Milner, King, et al., 2018a; Milner, Scovelle, et al., 2018b) and through expressed norms and behaviors at work. Such effects may be particularly pronounced in the most heavily male-dominated occupational groups, which may be exposed to masculine norms and behaviors that emphasize the importance of self-reliance, stoicism, and risky health behaviors. Further exploration of how health literacy, specific to the context of workforce gender segregation, impacts health outcomes is warranted.
This study further demonstrates the importance of bringing together research on occupational gender segregation, masculinity, and health to guide work on improving outcomes for men. Our results suggest that developing workplace health literacy policies in male-dominated occupations must consider the role of gender and dominant concepts of masculinity to enact substantive change. In a systematic review of research examining masculinity and men’s health and safety in high-risk male-dominated occupations, Stergiou-Kita et al. (2015) found that dominant masculinities can impact on the way men perceive and accept risks in the workplace, and further, how these risks are normalized in the context of the work setting. In some settings, this acceptance of risk is accompanied by an expectation that pain and injury will be tolerated and endured (Stergiou-Kita et al., 2015). Self-reliance is valorized, and masculinity is enacted by a resistance to assistance, authority, and occupational health and safety practices. Such theoretical perspectives raise important questions in relation to practical implications for improving the health of working men. For example, is improving health literacy for men contingent on couching health information in a stereotypical “male” context or would such an approach further entrench male gender norms that serve to create the problem in the first place? These ideas need further investigation.
Although gender desegregation of the workforce might offer the ultimate panacea for more equitable health outcomes for men and women, it is deeply entrenched in contemporary labor markets both in Australia and in many other parts of the world. In the shorter term, the key implication of this analysis is that workplace interventions to improve health literacy are needed in male-dominated occupations and sectors. Intervening in workplace settings to improve men’s health literacy is gaining traction (Larsen et al., 2015; Wong, 2012), and there are some promising workplace programs, particularly in relation to suicide prevention literacy in Australia (King et al., 2018, 2019). If workplaces, particularly those which are male dominated, become health literate, the health literacy of men who work in these occupations may improve, leading to an improvement in health outcomes. The benefits extend beyond the individual health benefits of workers; organizations that actively aim to build employees’ health literacy will not only improve the health of their employees but also likely reap economic benefits from healthier workers and healthier communities.
Limitations
One limitation of the current article is that only three components of the HLQ were collected in the Ten to Men survey—the full version of the scale assesses nine separate components. These items were only measured in Wave 2; hence, it is difficult to assess how health literacy may have changed over time or in response to other personal or health-related factors. The measure of health literacy used in the article does not recognize environmental health literacy and therefore places most emphasis on an individual’s ability to engage in the health system, rather than recognizing likely limitations in the health system itself. This is problematic as it does not recognize that an individual’s health literacy is embedded within the broader environment. In this study mental and physical health were conceptualized as potential confounders of the relationship between employment in a male-dominated occupation and health literacy; however, this relationship needs to be clarified, as it is likely that health consequences arise from low levels of health literacy (Berkman et al., 2011; Fabbri et al., 2018). Further waves of the Ten to Men study are needed to investigate these relationships. Other limitations of this article relate to generalizability, in that the Ten to Men sample is older, more likely to be Australian born, and more likely to live in regional areas (Currier et al., 2016) than the Australian population. Another limitation of the work presented here is retention into the study from Wave 1 to 2, which, while similar to other cohort studies (Wilkins, 2017), may have resulted in selection bias. Furthermore, the outcome and exposures were self-reported, resulting in possible dependent misclassification. Finally, the Ten to Men study is explicitly focused on men; thus, this article only includes men. Future research assessing how gendered occupational ratio impacts the health literacy of female workers is needed. These noted limitations are offset by the strengths of the article, which include its large sample size, prospective design, and the ability to control for a range of appropriate confounders.
Conclusion
This analysis provides evidence that men working in male-dominated occupations have poorer health literacy than men in non-male-dominated occupations. Health literacy interventions in workplace settings are needed, and targeting male-dominated occupations may deliver the greatest gains.
Supplemental Material
Supplementary_File_1 – Supplemental material for Health Literacy in Male-Dominated Occupations
Supplemental material, Supplementary_File_1 for Health Literacy in Male-Dominated Occupations by Allison Milner, Marissa Shields, Anna J. Scovelle, Georgina Sutherland and Tania L. King in American Journal of Men's Health
Footnotes
Acknowledgements
Tragically, Associate Professor Allison Milner died during the final revisions of this article. The authorship team wishes to honor the memory of Allison, whose intellect, wit, and passion for research will never be forgotten.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding provided by a Victorian Health and Medical Research Fellowship (AM), a National Health and Medical Research Council Partnership Project Grant APP1134499 (MS, AS), and an Australian Research Council Discovery Early Career Researcher Award DE200100607 (TK).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.