
Abstract
The aim of this study was to assess outcomes from a multilevel social network intervention to promote the health of Black men. Through a community–academic collaboration and using a participatory research approach, we implemented the intervention over 4 years in a 110-block area of an urban neighborhood. The project aimed to implement a neighborhood peer outreach and leadership network to strengthen social support of Black men and increase community and family engagement. Intervention activities included three 12-month intergenerational peer support groups (N = 46), a door-to-door outreach campaign (N = 186), media and communication efforts, and a community partner network. Primary outcomes for the peer support groups were measured using a pretest/posttest cohort design and included social support, perceived stress, social capital, and global self-esteem. Primary outcomes for the door-to-door outreach campaign were measured using a repeated cross-sectional design and included a sense of community, neighborhood social interaction, perceived neighborhood control, and self-rated health status. Significant findings from the peer support groups included an increase in social support overall (p = .027), driven by improvements in guidance, reliable alliance, and reassurance of worth; and an improvement in perceived stress (p = .047). Significant findings from the door-to-door outreach campaign included increases in neighborhood social interaction (p < .0001) and perceived neighborhood control (p = .036). This project provides evidence that a participatory approach to planning and delivering a health promotion intervention aimed at creating positive social spaces and enhancing social connections can result in significant outcomes and successful engagement of Black men.
Keywords
Startling disparities in health outcomes exist for Black men in the United States. Black men have the lowest life expectancy and highest mortality rate in the nation (Macdonald, 2013). For example, life expectancy at birth using 2015 data was 71.8 years for non-Hispanic Black men compared to 76.3 for non-Hispanic White men, and 78.1 for non-Hispanic Black women (Murphy et al., 2017). Even controlling for education, Black men with a high school education or more had higher all-cause mortality rates than their White counterparts (Gilmore et al., 2019). A review of chronic disease rates in Black men demonstrates vast disparities in almost every measure including death rates from heart disease, stroke, and diabetes (Office of Minority Health, 2019). Moreover, when compared to White or Latino men, Black men are less likely to seek professional care when in poor health, similar to seeking preventive services, and are also prone to delayed or poor medical attention irrespective of their insurance status (Holden et al., 2012; Ornelas et al., 2009; Tucker-Seeley et al., 2015).
While some of these disparities might be explained by lifestyle behaviors, understanding the interaction of behavioral and socioeconomic structures in a population is an important benchmark in the tackling of racial health disparities (Bryan et al., 2014; Hammond et al., 2011; Xanthos et al., 2010). Indicators of socio economic status (SES) such as income, education, or occupation not only influence health outcomes but are also strongly patterned by race to the extent that racial differences in SES are importantly associated with racial differences in health (Williams & Jackson, 2005). Black men tend to be more socioeconomically disadvantaged due to reduced access to quality education, disproportionate rate of incarceration, reduced chances of formal employment, as well as living in segregated neighborhoods rated as having low levels of opportunity (Macdonald, 2013).
A lived context of segregation, unemployment, poverty, and racism characterize the social isolation and marginalization of Black men in contemporary U.S. society (Berkman & Glass, 2000; Williams & Sternthal, 2010; Xanthos et al., 2010). As a result, Black men may live in social environments that expose them to joblessness, poverty, and civic disengagement, and hence a continuous cycle of social isolation and lack of social integration (Ornelas et al., 2009; Riphagen, 2008). Social integration, defined by close social relationships and the companionship and support provided therein, has been linked to health, exposure to stress, and the relationship between stress and health (House, 1987). A lack of social relationships has consistently been associated with all-cause mortality (Berkman & Glass, 2000).
The impact of these societal and social environmental factors places many Black men at a significant disadvantage with regard to health outcomes compared to more advantaged groups. Indeed, social injustice and other adverse social determinants of health have been identified as a major root cause of poor health outcomes among racial minorities (Ornelas et al., 2009; Riphagen, 2008). Participatory research and programs grounded in a social justice tradition and addressing the social determinants underlying health status, behavior, and social lifestyle can critically highlight social and environmental issues that influence health equity and sustainability among this marginalized population (Xanthos et al., 2010). In particular, there are features of a participatory research approach specifically intended to address issues of marginalization that are sometimes reproduced in academic research, rendering a participatory approach particularly appropriate for work with Black men. These features include giving authentic voice and decision-making power to the population of interest, inclusion in all phases of the research planning and implementation process, and attention to equitable and accessible dissemination approaches.
Specific to using a participatory approach to health promotion efforts among Black men, an initial step should involve incorporating men’s perceptions, attitudes, and priorities toward the factors influencing their health. A community-based participatory research (CBPR) approach can achieve this by encouraging critical dialogue on current issues and lived experiences with a goal to decipher ways of prioritizing and promoting social cohesion and support for, and among, Black men (Barnidge et al., 2010; Ferre et al., 2010; Hammond & Mattis, 2005; Watkins & Jefferson, 2013). The application of CBPR enriches interventions through the ideals of equitable participation, mutual learning, and community empowerment as well the conceptualization of research ideas into real and participatory community projects (Ferre et al., 2010; Smith et al., 2015).
CBPR has been applied widely in public health and related disciplines. Much of the CBPR literature specific to Black men is in the domain of sexual health and HIV prevention. Combined with the more limited literature outside that specific heath domain, available studies illustrate that CBPR is an effective strategy to engage with Black men about their health. Numerous descriptive studies have used CBPR to elucidate psychosocial and environmental factors important to Black men’s health-seeking behaviors and subsequent intervention design (Akintobi et al., 2018; Bharmal et al., 2012; Carter-Edwards et al., 2018; Chung et al., 2014; Ornelas et al., 2009; Ross et al., 2016; Trantham et al., 2015; Wilson et al., 2013; Windsor et al., 2018; Woods et al., 2004). Outside of the sexual health/HIV literature, few published studies report application of CBPR to intervention implementation and outcomes that engage Black men. One notable example is an oral health intervention (Hoffman et al., 2017) engaging low-income Black men based on formative participatory work (Akintobi et al., 2018) and resulting in significantly higher levels of knowledge on multiple oral health components.
There are different facets of tackling health disparities among Black men, especially when viewing those disparities from an upstream social ecological model. Community and social engagement among key stakeholders can improve relationships and create support for Black men to overcome social challenges (Debnam et al., 2012; Hossain & Roopnarine, 1994). Focusing on social engagement as a pathway to better health, several studies have reported significant associations between health behaviors and social support (Debnam et al., 2012; Holden et al., 2012; McFadden et al., 2014). There is a rich literature on the role of social support and social networks among Black men related to sexuality and HIV/AIDS, especially among Black men who have sex with men. The social context inherent in the experiences of these participants is not broadly applicable, however. There has been considerably less focus on Black males and the relationship between social engagement and/or social support in other health domains including overall health and wellness. Examples include studies that have identified associations between higher levels of social support and dental utilization (Stapleton et al., 2015) and colorectal cancer screening (Rogers et al., 2017). A photovoice study with Black men by Ornelas and colleagues reported that social capital and intergenerational mentoring were important factors for men’s health (Ornelas et al., 2009). A notable example is promoting health among Black men in barbershops, a long-standing venue for social interaction. Promoting men’s health in barbershops, including using barbers as peer mentors, appears promising for promoting cardiovascular health (Releford et al., 2010) and prostate cancer screening (Hill et al., 2017) among other health intervention topics (Linnan et al., 2014). Most of these studies focus on the social interaction between barbers and their clients as a means for education or behavior change in a specific health domain such as cancer, hypertension, or diabetes.
This project adds to the existing literature by implementing a participatory approach to intervention development and implementation, focusing on overall health and well-being, and extending to a neighborhood setting using door-to-door outreach seeking to engage Black men, especially those who are isolated and disengaged with their community. Using a CBPR approach and guided by a social network framework (Heaney & Israel, 2008), a multilevel social network intervention was developed to promote the health of Black men called No Longer an Island (NLI). This pilot intervention was implemented over 4 years in a 110-block area of a Midwestern city. This manuscript reports outcomes and key lessons learned from endeavoring to engage with the Black men who most needed positive social connections. The hypothesis was that men engaged in NLI would report significant positive changes in the individual-level outcomes post-intervention and that neighborhood block groups engaged in NLI would show increasing positive trends on community-level outcomes over the course of the intervention.
This article presents strategies that can be applied to leverage positive spaces for Black men to connect with one another and engage in intergenerational mentoring and positive social network activities. Failure to address the well-being of Black men is inextricably linked to a decline in well-being of Black families (Cowan et al., 2009). There is a need to build place-based support systems for men that foster resilience and empowerment in themselves, their families, and community (Heaney & Israel, 2008; Israel, 1982). By employing a place-based, multilevel social network intervention, this approach moves beyond a single-program intervention to impact the social environment and build individual and collective capacity for community change.
Methods
Community–Academic Partnership
A multiyear, ongoing community–academic partnership primarily between a grassroots community-based organization, a university researcher, and a local research center guided this project. The project began with a pilot grant focused on gathering a group of Black men together monthly for a year of facilitated discussions about lived experiences, social determinants of health, and health promotion planning for Black men. This group was called the Men’s Wellness Council. These discussions brought to light the tremendous isolation and pressure Black men experience and the need for safe spaces for men to connect and express their authentic selves. The primary recommendation emerging from this group was that the facilitated discussions should form the basis of a health promotion intervention for Black men in the neighborhood to promote social and community connectedness, foster intergenerational mentoring, and explore leadership opportunities. Another recommendation that emerged was the need to reach and engage Black men in the neighborhood who were the most isolated and most in need of positive social network connections. Further collaboration within the community–academic partnership and with the Wellness Council participants resulted in developing the intervention delivered in the current project. Black men who lived and/or worked in the neighborhood were hired to the project team to key roles in study implementation and had substantive roles in creating the study protocol and participating in dissemination of findings.
Intervention
NLI was a multilevel social network intervention informed by a long-standing community–academic partnership and engagement with Black men in the focus neighborhood. Using an iterative, participatory approach, the multidisciplinary project team translated recommendations from the Men’s Wellness Council into the NLI project. Specifically, the Men’s Wellness Council identified key action areas for promoting Black men’s health in their neighborhood. These action areas were as follows: (a) Develop spaces where Black men can express and explore authentic self-identity; (b) expand definitions of men’s health to include physical, emotional, mental, and financial well-being; (c) support mentorship efforts between men that extend across generations; and (d) strengthen grassroots outreach to engage men of all ages in productive service (Walnut Way, 2013). These recommendations served as the backbone of the NLI intervention activities.
The intervention structure was also guided by a conceptual framework for the relationship between social networks and health posited by Heaney and Israel (2008). This framework identifies five pathways linking social networks and social support to physical, mental, and social health. Consistent with this framework, intervention strategies were employed that focused on multiple aspects of the social network.
The intervention had four main activities, the outcomes of two of which are reported in this article. Primary intervention activities were facilitated peer support groups and door-to-door outreach. Peer support groups met 1–2 times per month for 12 months. Meetings lasted about 2 hr and each one began with a meal and fellowship. A Black man experienced in facilitating peer groups for men led the peer support groups. A toolkit created in the pilot phase guided the group discussions (toolkit available upon request). The toolkit was created, in collaboration with the Men’s Wellness Council, to develop group cohesion and focus the discussions on topics such as the lived experience of Black men and specific social determinants of health in Black communities. Three separate 12-month peer support groups were implemented over the course of 3 years.
The door-to-door outreach part of the intervention, called Porch-2-Porch (P2P), was designed to engage and connect Black men in the neighborhood. In four phases of about 3 months each, trained Black men from the project team knocked on doors looking to connect with interested men in specific segments of the neighborhood. Once a man was enrolled in the program, contact information was collected as well as information on personal skills and challenges, fatherhood experiences, and neighborhood assets and challenges. Areas of interest for neighborhood engagement were gathered. Necessary referrals according to needs identified including connections to peer support groups and other neighborhood activities were made. Each visit lasted 15–45 min. Follow-up visits were available upon request. Four phases of P2P outreach were conducted across the project duration.
To enhance development connections and engagement, participants in both the peer support groups and P2P were invited to networking and social events in between meetings and porch visits. As the intervention unfolded, opportunities were identified for participants to plan neighborhood events and engage in other types of neighborhood leadership.
The two other key intervention activities were convening a partner support network of organizations serving men in the neighborhood and a multimedia storytelling campaign intended to give voice to the stories of men in the neighborhood.
Recruitment
This intervention focused on a 110-block area of an urban, Midwestern city. Recruitment was conducted for the peer support groups via flyers, word of mouth, partner organization referrals, and P2P outreach efforts. Once a man expressed interest in the peer groups, he was referred to project staff for screening for inclusion criteria and collection of variables used for peer group composition. The inclusion criteria were Black men aged 18 years or older who live, work, or play in the neighborhood of focus. Project staff then composed groups from the pool of men screened as eligible. Groups were composed to ensure majority having residence in the neighborhood and with variation across age, marital status, and fatherhood status. Target group size was 15 men with alternates selected in case of declined invitations. Participants were provided with incentives worth $15 for attending at least one meeting per month.
Recruitment for P2P was geographically based with outreach efforts focusing on certain blocks and block groups of the 110-block neighborhood during different phases of outreach. These neighborhood segments were selected based, in part, on the effort to connect with men not currently engaged with the organization or neighborhood activities. Project staff knocked on doors in each block inquiring about adult men residing in the home. If one or more adult men were present, they were screened for interest in enrolling in P2P. Multiple visits were attempted on different days of the week and different times of the day in an effort to reach the most men.
Data Collection
Paper-and-pencil surveys were used to collect outcome data. Male project staff trained in informed consent and data collection processes conducted data collection. Peer support group participants provided written informed consent. P2P participants provided verbal informed consent. For those who were enrolled outside of survey waves, an approved waiver to document consent was obtained. For P2P participants enrolled during survey waves, consent was documented via completing the survey questions. The Institutional Review Board at University of Wisconsin, Milwaukee, approved the project (Protocol #14.137).
Peer support group surveys
Each peer support group was treated as a cohort for data collection and completed baseline and follow-up surveys. This method allowed for examining individual-level change before and after exposure to the peer group experience. Baseline was prior to the peer support group starting and follow-up was immediately following the last official peer support group meeting. Two surveys were used to measure peer group outcomes: the main outcome survey and the social network survey. The main outcome survey was self-administered with a project staff member reading the questions and response options aloud. The social network survey was interviewer administered. To reduce social desirability bias, the peer group facilitator and assistant facilitator did not collect any outcome data. The two surveys combined took 30–45 min to complete.
P2P neighborhood outcome survey
P2P used a repeated cross-sectional design to assess outcomes. For a segment of 2–4 weeks of each of the four P2P phases, every man enrolled in P2P completed a neighborhood outcome survey. This method allowed for capturing a snapshot of the targeted outcomes in the community over time. Outreach project staff administered the survey. The survey took less than 10 min to complete.
Measures
Intervention outcomes were identified through a logic model developed by the project team illustrating hypothesized links between intervention activities and their intended effects. A key method of encouraging participation in this process by all members of the project team was to have team members describe intended intervention effects in layperson terms. Once a list of these intended effects was compiled, the academic partner translated them into measurable outcomes, checking back with the project team to ensure the translation fit with the original meaning. The academic partner then identified potential measures for the selected outcomes in the literature and the project team reviewed those for content, length, and acceptability for the sample population. Collectively, the project team chose the measures that best fit those criteria. The academic partner then compiled the surveys from those selected measures.
Peer support group surveys
Primary outcomes for the peer support groups were social support, perceived stress, social capital, and global self-esteem. Physical and mental health were measured as distal outcomes. Other variables measured included sociodemographic factors, social network features, and civic engagement.
Social support was measured with the 24-item Social Provisions Scale (Cutrona & Russell, 1987) and perceived stress, with the 10-item Perceived Stress Scale (Cohen et al., 1983). Social capital was measured with the 28-item Sampson’s Collective Efficacy Scale (Sampson et al., 1997). This scale measures two dimensions of social capital: trust and social engagement. Global self-esteem was measured with the 10-item Rosenberg Self-Esteem Scale (Rosenberg, 1965). Physical and mental health was measured with a version of the SF-12 used by a statewide survey, Survey of the Health of Wisconsin, for possible comparative purposes with statewide data.
The social network survey measured social network features and civic engagement with the Social Disconnectedness and Perceived Isolation Scale (Cornwell & Waite, 2009). Social network features collected included size, range, frequency of contact, and number of contacts in home. Civic engagement included number of friends, frequency of organized group meetings, frequency of social meetings, and frequency of volunteerism. The perceived isolation scale items were not included in the survey because there were similar questions in other included scales.
P2P neighborhood outcome survey
Primary outcomes for the P2P survey were sense of community (6 items), neighborhood social interaction (4 items), and perceived neighborhood control (5 items). Each of these outcomes was measured using scales on the Community Social Dynamics survey (Parker et al., 2001). The survey also asked one question on self-rated health status.
Data Analysis
The unit of analysis in all cases was the individual participant. All analyses reported here used the R statistical analysis program. Specific packages used for specialized approaches are listed with the corresponding description.
Peer support group surveys
Twenty-two percent of variables had no missing data, and the remaining variables typically had fewer than five observations (of 69) missing. To ensure minimal loss of data, imputed missing values were multiplied using the mi package in R. This package uses approximate Bayesian models for stability in imputation and permits specification of appropriate imputation distributions for categorical variables. All results reported were combined across 10 imputed data sets.
Differences in demographic variables between baseline and follow-up surveys were evaluated using chi-square tests for categorical variables and t tests for continuous variables. To evaluate changes in outcome scales (health, collective efficacy, self-esteem, perceived stress, and social provision), both t tests unadjusted for covariates and linear regression were used, accounting for potential confounding by demographic variables.
Social network survey
Unadjusted comparisons of social network and civic engagement variables over time were made using unequal variance t tests and Fisher’s exact test for independence of categorical variables.
When assessing associations between time of survey administration and civic engagement variables with adjustment for demographic factors, ordinal regression was used with a probit link, with the ordinal package in R. To assess associations between social network variables and time of survey administration with adjustment for demographic factors, Bayesian generalized linear models (GLM) were used with the bayesglm package in R. Finally, associations of social network and civic engagement variables with other outcomes were evaluated by adding them to the adjusted linear regression models and evaluating their contribution to the model.
P2P neighborhood outcome survey
There was very little missing data for any variable in the neighborhood survey. If the response to the entire scale was missing for a participant, that participant was dropped from analyses of that scale (this occurred for one participant with the perceived neighborhood control scale). Otherwise, missing values were filled in with the modal response for that variable (1–3 observations for each variable across all time points).
The trend in each scale was evaluated using linear regression techniques. Due to the small number of time points and some evidence of a nonlinear trend, each time point was treated as a category in order to evaluate the presence of any changes in level. Contrasts were then used to evaluate differences between early and late time points.
Results
Peer Support Group Surveys
The three peer support groups each met over the course of 13–14 months. Each group held 15–16 official meetings and each group had 12–16 members who attended at least two meetings (15, 16, and 12 members, respectively). Individual members attended between 2 and 16 meetings with an average of 7 meetings attended per person. Meeting attendance ranged from 4 to 12 members per meeting with an average of 7 attendees per meeting.
Forty-six men completed the baseline main outcome survey. Of those, 34 men completed the baseline social network survey. Table 1 presents sample characteristics. Men ranged in age from 20 to 60 years with fairly even representation across decades of life (e.g., 20–29, 30–39). Men were predominately Black (n = 45, 97.8%) and non-Hispanic (n = 44, 95.7%). More than half reported being single/never married (n = 27, 58.7%) and having an annual household income less than $20,000. About one third reported being employed full-time (n = 16, 34.8%) and another third being unemployed (n = 15, 32.6%). Men reported an average of 4.6 social contacts, with an average of 3.6 interactions with each contact each week. Most reported contacts were family (n = 64, 41.8%) or friends/associates (n = 69, 45.1%).
Sample Characteristics of Those Completing the Baseline and Follow-Up Peer Group Surveys.

Note. Differences between groups in categorical variables tested with chi-square tests of independence; differences in quantitative variables tested with two-sample t tests.
Twenty-three of the peer support group participants completed the follow-up main outcome survey and 15 participants completed the follow-up social network survey. Several differences were observed in the characteristics of the groups who completed the baseline and follow-up surveys (Table 1). There was strong evidence for a difference in the age distribution and the employment status of the two groups, and moderate evidence for differences in the proportion with pregnant partners and the household income of the two groups. The analyses adjusted for these factors when making inferences about differences in outcome measures between the two groups.
Adjustment for potential confounding factors did not substantially alter inferences about changes in outcome measures (Table 2). After accounting for age, education, employment, household income, marital status, number of children, and whether the respondent had a pregnant partner, an improvement was observed in social support overall (β = 5.20, p = .027), driven by improvements in guidance, reliable alliance, and reassurance of worth. There was also an improvement in perceived stress (β = −3.41, p = .047), with a drop of about 3.4 points on the perceived stress scale. There was moderate, though nonsignificant, evidence of improvements in collective efficacy (β = 2.82, p = .104) and self-esteem (β = 2.19, p = .087). Given the small sample sizes, these are promising results.
Observed Scale Values (Mean [SD]) for Baseline and Follow-Up Surveys With Change in Outcome Measures Between Baseline and Follow-Up Groups

Note. Adjusted model includes age, education, employment, marital status, race, ethnicity, number of children, partner pregnant (Y/N), and household income.
Results from the social network survey provided evidence for an increase in the number of friends from the baseline to follow-up survey and that unemployment was associated with lower civic engagement almost across the board excepting social encounters (data not reported). No significant changes from baseline to follow-up for other social network measures were found and neither were significant relationships between social network variables and the primary outcome variables after adjustment for demographic factors.
P2P Neighborhood Outcome Survey
One hundred eighty-six men enrolled in P2P. Men had lived in the neighborhood for an average of 14 years (range = <3 months to 63 years). Most of the men reported being single (n = 142, 76.5%) and Black/African American (n = 184, 98.9%). Men ranged in age from 18 to 89 years with 40.8% being 18–29 years old (n = 76) and 47.9% being 30–59 years old (n = 89). Most of the men reported achieving a high school degree (n = 81, 43.3%) with 28% reporting some college (n = 52). Of the 186 men enrolled in P2P, 102 completed the P2P outcome survey across the five waves of data collection with approximately 20 men per survey wave (range = 19–21 men per survey wave). Only men enrolled in P2P during one of the five survey waves were invited to take the survey.
In general, a slight drop in scale scores was seen from Winter 2014 to Fall 2015, with a rebound to an equal or higher level in the final three time periods (Figure 1 and Table 3). Regression results indicated that there was a significant difference between observations in 2016 compared to earlier waves for neighborhood social interaction (t(97) = 4.12, p < .0001) and for perceived neighborhood control (t(96) = 2.13, p = .036), but not for sense of community (t(97) = 0.81, p = .42) or self-rated health (t(95) = −0.83, p = 0.41). The average improvement in neighborhood social interaction for 2016 relative to Winter 2014/Fall 2015 was 3.1 points (SD 0.75), while the average improvement for perceived neighborhood control was 1.25 points (SD 0.59).
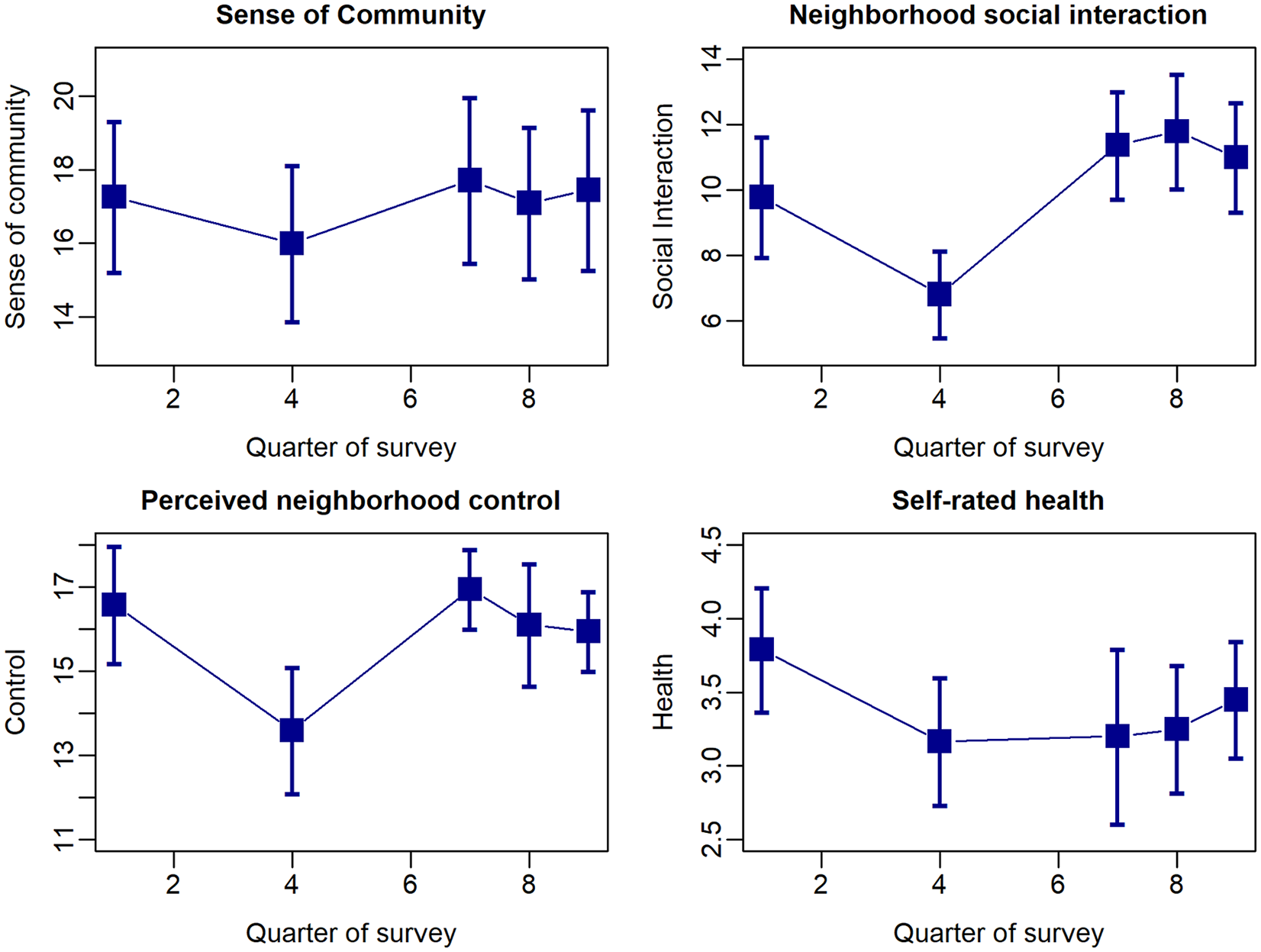
Trends in scale scores over time; 95% confidence intervals for the mean score at each time point are indicated by vertical bars. Quarter 1 is Winter 2014.
Mean and Standard Deviation (SD) of Scale Scores From the Porch-2-Porch Survey.

Note. Independent samples taken at five time points after the start of the intervention.
Discussion
This project provides evidence that a participatory approach to planning and delivering a health promotion intervention aimed at creating positive social spaces and enhancing social connections can result in successful engagement of Black men. Two hundred twenty-eight Black men were enrolled in the study, some of whom were socially isolated, actively involved in criminal justice proceedings, and/or navigating access to basic needs of daily life. With the support of the community organization partner, the field staff supported every man they interacted with by making needed connections and assisting in seeking of resources. By going out in the neighborhood door-to-door, men were reached who needed the project connections and may not have been exposed to or responded to passive recruitment efforts.
The intervention resulted in significant positive findings at both the individual and neighborhood level. At the individual level, the men in the peer support groups reported significantly higher levels of social support and significantly lower levels of perceived stress from baseline to post-intervention. Peer groups started out with structured facilitation from the group leader and project-organized outings to encourage group cohesion. Over the course of the year, peer groups transitioned to more peer-level mentoring and leadership opportunities. By the end of the year-long experience, peer group members had begun organizing their own outings (e.g., attending sports events), specifying topics for the peer group meetings, and organizing community events (e.g., community basketball event, healing circles for violence survivors, youth mentoring) including garnering funding for some of those events.
While many studies engaging Black men examine social support as an independent variable, few published health promotion interventions for Black men were found that examined social support as an outcome variable. The Young Black Men, Masculinities, and Mental Health (YBMen) Facebook project (Watkins et al., 2017) is an intervention that used a private online forum and group facilitation techniques to promote social support related to mental health. In a qualitative evaluation of the YBMen pilot (Watkins et al., 2017), one of the key themes that emerged related to what the men liked about the intervention was that the format allowed men to build new relationships and feel supported. Interestingly, one of the key themes that emerged related to what the men disliked about the intervention was the lack of face-to face meetings. A qualitative descriptive study examining Black men’s resilience also reported a key theme of creating healthy and supportive environments as important to overall health (Teti et al., 2012). Data related to this theme included men reporting that they could not find positive sources of support. Promoting positive social support plays an important role in Black men’s health, especially for those men who are socially isolated or disengaged. NLI provides a community-based, intergenerational approach to positively impact social support for Black men.
Perceived stress has been examined as an important predictor of Black men’s health in numerous studies, especially in the context of racism and social determinants of health (Pieterse & Carter, 2007; Williams & Sternthal, 2010; Xanthos, 2009; Xanthos et al., 2010). Fewer published interventions for Black men have specifically focused on reducing perceived stress as an outcome. One example is Color It Real (Zellner et al., 2016); a 7-week sexual health, substance use, and perceived stress intervention for young Black men and women. Using the same perceived stress measure as NLI (Cohen et al., 1983), Color It Real reported a significant decrease in perceived stress from baseline to post-intervention in the intervention group and significant changes in specific items between the intervention and control groups (Zellner et al., 2016). The NLI project adds to the literature showing initial results that peer support groups for men may be a method for reducing perceived stress.
In addition to the promising results from the peer support groups, lessons learned from delivering this aspect of the intervention in a sample of men bearing the burden of many structural inequities may be informative to other practitioners and researchers. Despite significant and varied experience on the study team, multiple challenges emerged in retaining participants after the initial meeting. Most prominently, these included deep distrust of projects classified as research, encounters with the criminal justice system preventing further attendance, and participant death. Anticipating this issue by having trusted community-side project staff play key leadership roles in recruitment and consenting; holding more introductory meetings (at least 2–3) before the first official peer group meeting; and allowing for new member matriculation to the group during the first 2–3 months would help both prevent project delays and unexpected resource allocation to achieve minimum numbers in peer groups.
Another lesson learned was related to survey completion. Specifically, participants lacked interest in completing surveys even though they were still engaged with the peer groups, and there was a reluctance to fill out the social network survey with adequate detail about contacts’ names. The key strategy that emerged to enhance survey completion, besides emphasizing the importance of evaluation to ensure continued project funding, was to allow participants to make appointments to fill out surveys individually at the community-based organization rather than during the designated survey completion time. Participatory evaluation methods to explore acceptable and meaningful evaluation outcomes would be very useful to future research and programmatic efforts.
Enhancing the peer support groups with an effort to increase neighborhood-level connectivity through the door-to-door outreach campaign indicated promise for increasing neighborhood social interaction and perceived neighborhood control. Improving the neighborhood social environment could have health impacts. There is a growing scientific literature examining features of the social environment including social capital, collective efficacy, and civic engagement as health promoting (Cohen et al., 2008; Letcher & Perlow, 2009). Meaningful civic engagement has been associated with increased social capital/collective efficacy (Goth & Smaland, 2014), which, in turn, has been associated with numerous health outcomes including mental health, crime, obesity, and mortality related to heart disease (Cohen et al., 2008). Civic engagement has been associated with mental health in other studies through pathways including social support, perceived power, and sense of community (Landstedt et al., 2016). A community outreach approach to connect and engage men aligns with the recent recommendations by Graham and colleagues for recruiting low-income Black men to health promotion programs (Graham et al., 2018).
Implementation lessons from the door-to-door outreach campaign included realizing that even experienced race- and gender-matched field staff, often known to residents, needed time to develop initial rapport on a block. Identifying a block ambassador proved effective where possible. The study team quickly realized that some of the most important project outcomes were those that were not being measured. For example, 34 men were connected to jobs and/or internships, 11 men were assisted in returning to school or certified training, and 18 men were assisted with job readiness support via project partners. Participants organized themselves in civic engagement efforts big and small including hosting healing circles at a local school and organizing to have the city install speed bumps on a busy street. While these outcomes were not a priori stated health outcomes for the project, they were directly related to the men’s health and documenting them proved important.
Limitations
These data provide a useful framework for engaging Black men and affecting positive individual- and community-level change. Limitations of the study design included not randomizing to condition and not having a control or comparison group. Randomization in this participatory research context would only have been possible if another valued and unrelated intervention could have been delivered or a crossover design was used; neither was possible within the resource constraints of this study. In terms of having a comparison group, the feasibility of administering surveys to a group of men not receiving the intervention was not possible for this pilot study. The small sample of men in the peer support groups completing both the pre- and post-intervention surveys should be considered. This issue was addressed statistically by controlling for factors that differed between the group of men that completed only one survey time point and the group completing both survey time points. Of particular relevance to researchers and practitioners was the difficulty in getting otherwise engaged men to complete surveys. Having used multiple methods to increase completion, this issue requires further study.
Conclusion
Effective strategies for engaging Black men in health promotion efforts are critical to addressing disparities in mortality and other health indicators. Key to that effort is engaging Black men in an authentic and participatory way to ensure that health promotion efforts meet the needs and preferences of the audience—especially men who are isolated or whose daily lives challenge robust community engagement. Interventions that enhance the strength and positivity of Black men’s social networks through peer mentoring, intergenerational support, and connections to resources—leaving behind the structure and connections for continued support and engagement—hold promise for addressing long-standing inequities in Black men’s health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the UW School of Medicine and Public Health from the Wisconsin Partnership Program through a Lifecourse Initiative for Healthy Families large implementation grant.