
Abstract
This article examined associations between male-dominated occupations and substance use disorders in young adulthood, accounting for adolescent experiences of work intensity (more than 15 hr a week at 16 to 17 years of age) and substance use (i.e., smoking, heavy drinking, cannabis, and illicit drug use). The moderating effects of biological sex and coming from a family with a low socioeconomic status (SES) were also assessed. Data were from a 10-year prospective study of community-based youth aged 12–18 in 2003 (T1; N = 662; 48% male; Mage = 15.5, SD = 1.9). Their occupations at ages 22–29 were categorized so that higher scores indicated more male-dominated occupations. Young adults in male-dominated occupations (more than 75% males) had lower education, worked in less prestigious occupations, and earned higher hourly wages than those in the other gendered-occupation groups. Work intensity in high school was associated with substance use at ages 18–25 and substance use was also associated with alcohol- and cannabis-use disorder symptoms and illicit drug use in young adulthood (ages 22–29). Adding to these effects, employment in a male-dominated occupation was associated with more cannabis-use disorder symptoms for the low, but not the high SES group. Public health messages need greater focus on preventing substance use disorders among individuals employed in male-dominated jobs in young adulthood. Efforts to promote self-assessment of problematic substance use and motivation to change may be particularly important for young workers.
Keywords
Many youths use substances at low levels, but a substantial proportions report symptoms of substance use disorders by early adulthood (Thompson et al., 2018). Males are at greater risk for problematic substance use than females (Leos-Toro et al., 2017; Stone et al., 2012); however, the gendered contexts and developmental trajectories that explain this heightened risk are not well studied. This lack of knowledge limits public health approaches to this health inequity. Although there are many studies of the risk and protective factors related to substance use in adolescence and young adulthood (Lee et al., 2014; Stone et al., 2012), the socializing effects of male-dominated work contexts on health and substance use disorders has only begun to be recognized (Roche et al., 2015; Smith & Koehoorn, 2016).
This study is grounded in life-course developmental and gender socialization theories and posits associations between employment in male-dominated occupations and substance use disorders in young adulthood (ages 22–29). Life course theory specifies risk (and often protective) factors that increase (or decrease) the likelihood of homotypic or heterotypic adaptive or maladaptive outcomes across developmental transitions (Smith et al., 2018). Gender socialization theory examines the effects of both biological sex and social influences (e.g. gendered-segregated work) have on health and wellbeing (Ristvedt, 2014). The effects of work intensity (working more than 15 hr a week in high school) and substance use (i.e., smoking, heavy drinking, cannabis, and illicit drug use) in adolescence on employment in male-dominated work and substance use disorders (alcohol and cannabis) and illicit drug use in young adulthood are assessed. The moderating effects of biological sex and living in a family with low socioeconomic status (SES) are tested.
Work in adolescence is often characterized by minimum wage jobs, with considerable churning through short-term positions (Staff et al., 2009). Extensive work during high school has been labeled “work intensity” which has been variously assessed as more than 20 hr a week in some studies (Staff et al., 2010), and more than 26 hr per week, in others (Kaestner et al., 2013; Wu et al., 2003). Work intensity predicts increases in delinquency, substance use, reduced time for school work, and lower commitments to postsecondary education (Staff et al., 2009).
Kaestner et al. (2013) argue that many behavioral indicators may explain the association between work intensity and adolescent substance use. Adolescents with poor academic performance may “select into” early employment, rather than persisting in high school. Benefits of adolescent work may include heightened work experience and higher early adult wages (Staff et al., 2009). Adolescent work may be related to their efforts to reduce family financial strain and economic stress (Lewis Brown & Richman, 2012; Richman et al., 1997). Research findings on the effects of family SES on the association between work intensity and types of substances used are inconsistent (Breslin & Adlaf, 2005). Further research on the impact of family SES on the prospective associations between work intensity and substance use and their consequences for occupational choices and substance use disorders in young adulthood is needed.
Previous reviews of adolescent career development (Luke & Redekop, 2014; Porfeli & Vondracek, 2009) posit that adolescents, especially males, who work more than 20 hr a week while going to high school (i.e., high work intensity) are more likely to be employed in gender-segregated work and experiences gained in these occupations may circumscribe future occupational options and promote substance use. Work in male-dominated jobs may provide youth with substantial expendable incomes and exposure to a culture of traditional masculinity norms (e.g., endurance, self-sufficiency, and comradery) that can include permissive alcohol or substance use norms (Roche et al., 2015). Research also indicates that work-related health risks in male-dominated jobs can contribute to health inequities in males (Ristvedt, 2014). Individuals working in construction, oil or mining industries, transportation, and trades can be exposed to disadvantages related to the structural dimensions of this work. These can include a lack of personal control, intermittent or seasonal work, irregular hours, time pressures, social isolation, injuries, and harsh environmental conditions (Ross & Mirowsky, 2013). Injuries and pain experiences may be also greater for individuals in more physically demanding, male-dominated jobs and underlie self-medication attempts. However, empirical studies of gender-segregation in young adult occupations and its association with prior and concurrent substance use are lacking
In the current study, following Smith and Koehoorn (2016), the National Occupational Classification System (Statistics Canada, 2012) was used to classify gender-segregation in young adult occupations (i.e., at ages 22–29). Based on past theory, work intensity in high school is expected to be associated with substance use and with an increased likelihood of selecting into male-dominated occupations, alcohol and cannabis use disorders, and illicit drug use in young adulthood. To test this theory, structural equation modeling (SEM; Bollen & Curran, 2006) is used to examine data from a large community-based cohort (ages 12–18 at baseline) of Canadian youth who were followed biennially across a decade (2003–2013) in six assessments (T1–T6). Specifically, a longitudinal theoretical model is tested, hypothesizing that work intensity in high school (i.e., at ages 16–17, coded from data at T1–T3) and subsequent substance use (coded at T4, ages 18–25) is associated with subsequent employment in male-dominated occupations and problematic substance use (i.e., alcohol and cannabis disorder symptoms and illicit drug use) in young adulthood (coded at T6, ages 22–29). T1 substance use is controlled in this model. The moderating effects of biological sex and of coming from a low versus high SES family on these pathways are examined subsequently.
Method
Participants and Procedures
Data are from a 10-year longitudinal study of community-based youth who were aged 12–18 in 2003 (T1; N = 662; 48% male; Mage = 15.5, SD = 1.9). Households (n = 1,036) with an eligible youth (aged 12–18) were identified from a random sample of 9,500 telephone listings; 662 youth provided written consent to participate (parental consent was also collected for those youth under 18). At each wave, data were collected in individual face-to-face or Skype interviews in the youth’s home or another private place. Sensitive items (e.g., substance use) were self-administered to enhance privacy and increase responding (see Leadbeater et al., 2012 for full study details). Participants were 85% Caucasian (n = 561), 4% Asian (n = 28), 4% mixed/biracial (n = 25), 3% Aboriginal (n = 20), and 4% other (n = 28; e.g., Black, Hispanic, or other) and were from economically diverse family backgrounds (Leadbeater et al., 2012). Retention rates at each wave were 87% (T2, N = 578), 81% (T3 N = 539), 69% (T4 N = 459), 70% (T5 N = 469), and 72% (T6 N = 478). Youth lost to follow-up were more likely to be male (T1: 48% n = 320 vs. T6: 45% n = 215; χ2 (1, 662) = 8.77, p = .003) and to be from lower SES families (T1 SES: M = 5.97, SD = 1.96) than youth who were retained (T1 SES: M = 6.69, SD = 1.71; F(1, 659) = 21.72, p < .001). The University of Victoria’s Human Research Ethics Board approved this study (Approval # 09-292).
Measures
Covariates
Sex was measured as self-reported sex (male = 0; female = 1). For SES, participants reported their parent(s)’ occupation which was coded using the Hollingshead Occupational Prestige Status Scale (Bornstein et al., 2003; Hollingshead, 2011). The highest rating for either parent’s occupations was used. Scores range from 1 to 9 (1= menial service workers, homemakers; 2 = unskilled workers; 3 = machine operators and semi-skilled workers; 4 = smaller business owners (<$25,000), skilled manual laborers, craftsmen; 5 = clerical and sales workers; 6 = technicians, semi-professionals; 7 = managers, minor professionals; 8 = administrators, lesser professionals; and 9 = higher executive, major professional). For the moderation analyses, participants were grouped as 0 = low SES (i.e., Hollingshead ratings 1–5) or 1 = high SES (i.e., ratings 6–9). Table 1 presents differences in parent education, full-time employment, and financial strain in these two groups. As expected, compared to the high prestige group, the parents in the low SES group had lower education, were less likely to work full-time work, and had problems in paying for necessities. Slightly fewer males (44%) than females comprised the low group. Baseline (T1; ages 12–18) heavy episodic drinking and cannabis use were also used as covariates in the analyses.
Family SES Differences in High Versus Low Groups Based on Hollingshead Scores for Parent Occupations at Time 1.

Work Intensity (Assessed for All Youth at Ages 16–17)
Using data from waves T1–T3, reported number of hours worked per week for each participant when they were either 16 or 17 years old was coded as a dichotomous variable with “0” = worked less than 15 hours per week or “1” = worked 15 hours or more hours per week. Research in the United States used a cut-off of 20 hr per week to denote high-intensity work in high school (Staff et al., 2010); however, in the current sample, only 8% of youth worked 20 hr a week or more. A cut-off of 15 hr per week represented the top 20th percentile of youth and provides adequate power for analyses.
Substance Use (Assessed at T4; Ages 18–25)
Heavy episodic drinking (HED) was assessed as “How often in the past 12 months have you had five or more drinks on one occasion?” (Thompson et al., 2014); and cannabis use as “How often did you use marijuana (cannabis, hashish, hash, THC, pot, grass, weed, reefer) in the past 12 months?” Using both formal and street names, participants were asked how often they used each of six illicit drugs in the past year: hallucinogens, amphetamines, club drugs, inhalants, cocaine, and heroin. Response choices for all substances were 0 = never, 1 = a few times a year, 2 = a few times a month, 3 = once a week, and 4 = more than once a week. Due to low rates of endorsement of illicit drugs at T4 and T6, the highest response for any illicit drug was used. Youth also indicated how many cigarettes they smoked in the past week (0 = none, 1 = one per week, 2 = less than half a pack (2–9), 3 = less than a full pack (10–19), and 4 = a full pack or more (20+)). Confirmatory factor analysis supported the latent structure of adolescent substance use variable (i.e., including smoking, HED, cannabis use, and illicit drug use) using data at T4 (root mean square error of approximation (RMSEA) = 0.02 [90% CI = 0.00, 0.10], comparative fit index (CFI) = 1.00, standardized root mean square residual (SRMR) = 0.01).
Gender-Segregated Occupations (GSO, Assessed at T6; Ages 22–29)
Occupations held at T6 were categorized following Smith and Koehoorn (2016), using the National Occupational Classification System (Statistics Canada, 2012). Higher scores indicate occupations employing a greater percentage of males than females: 0 = highly female-dominated (i.e., occupations where only 25% or less are male; e.g., childcare providers, nurses), 1 = moderately female-dominated (i.e., occupations where 26–50% are male; e.g., clerical occupations, retail, and sales), 2 = moderately male-dominated (occupations where 51–74% of workers are male; e.g., managers and supervisors), and 3 = highly male-dominated (occupations where 75% or more of workers are male; e.g., trade, transport and equipment operators, and computer programmers).
Educational achievement reflected the highest level achieved by T6 (1 = high school or less, 2 = some training college or trade, 3 = trade certificate or diploma, 4 = Certificate or Diploma, 5 = Bachelor degree or higher).
Full-time employment was classified as: 0 = part-time or not currently working or as 1 = full-time.
Occupational prestige of participants’ T6 occupation was coded using the Hollingshead Occupational Status Scale (Bornstein et al., 2003; Hollingshead, 2011). Please supply reference details or delete the reference citation from the text Participants reported the average number of hours worked per week and their hourly wage for their primary job at T6.
Problematic Substance Use at T6
Using the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998), participants responded no (0) or yes (1) to 10 items reflecting DSM-5 diagnostic criteria (American Psychiatric Association, 2013) for alcohol- and cannabis-use disorders (e.g., used more than planned, had to increase use to get the same effects, experienced withdrawal symptoms, tried to stop several times, or used despite experiencing mental health or relationship problems). The total number of symptoms was used; however, youth reporting two or more symptoms meet the diagnostic criteria for a substance use disorder (American Psychiatric Association, 2013; Thompson et al., 2015).
Planned Analyses
SEM were examined using Mplus version 8.2 (Muthén & Muthén, 1998). Given both continuous (i.e., substance disorder symptoms) and ordered categorical (i.e., work intensity, substance use frequency, and male-dominated occupation) variables were specified in the model, weighted least squares estimation was used for missing data. Standard SEM fit indices including RMSEA ≤ 0.08, CFI ≥ 0.90, and SRMR ≤ 0.05 were used to assess model fit (Bollen & Curran, 2006). Models account for T1 sex, age centered, family SES, and adolescent (T1; ages 12–18) HED and cannabis use.
Four mediation paths were tested using the joint significance test (MacKinnon et al., 2002) using the MODEL CONSTRAINT option in Mplus (Muthén & Muthén, 1998–2017). In sum, the joint significance test assesses whether the product of the regression coefficients of Y on M (b) and M on X (a) are significant (mediation joint test = a*b). The four mediation paths include: (1) the indirect path from work intensity to male-dominated occupation via substance use, and (2) the indirect paths from substance use to (a) alcohol disorder symptoms, (b) cannabis disorder symptoms, and (c) illicit drug use via male-dominated occupation.
The moderating effects of biological sex and SES were tested separately using the chi-square difference test and GROUPING and DIFFTEST options in Mplus (Muthén & Muthén, 1998–2017). The chi-square difference test compares a less restrictive (H1) model where parameter estimates are allowed to be free across groups (i.e., sex—males and females and SES—low and high) to a nested (H0) model where the hypothesized path of the model are constrained to be equal across groups. A significant chi-square different test indicates that the constrained model (H0) is a worse fit to the data than the less restrictive model (H1) and group differences exist in the hypothesized path.
Results
Descriptive Analyses
Table 2 presents descriptive statistics for the total sample and by gender-segregated occupation groups. Groups did not differ in their adolescent substance use, frequency of work intensity, family of origin SES, or their cohabiting or being married status at T6. Correlations between study variables can be found in supplemental Table S1. At T6, youth in high male-dominated occupations had lower education than those in high female-dominated occupations; they worked in less prestigious occupations than in moderately female-dominated occupations; earned the highest hourly wage of all groups; and reported more cannabis-use disorder symptoms than those in high female-dominated occupations.
Means (or frequencies) of Study Variables Grouped by Young Adult (T6; ages 22–29) Male-Dominated Occupation.
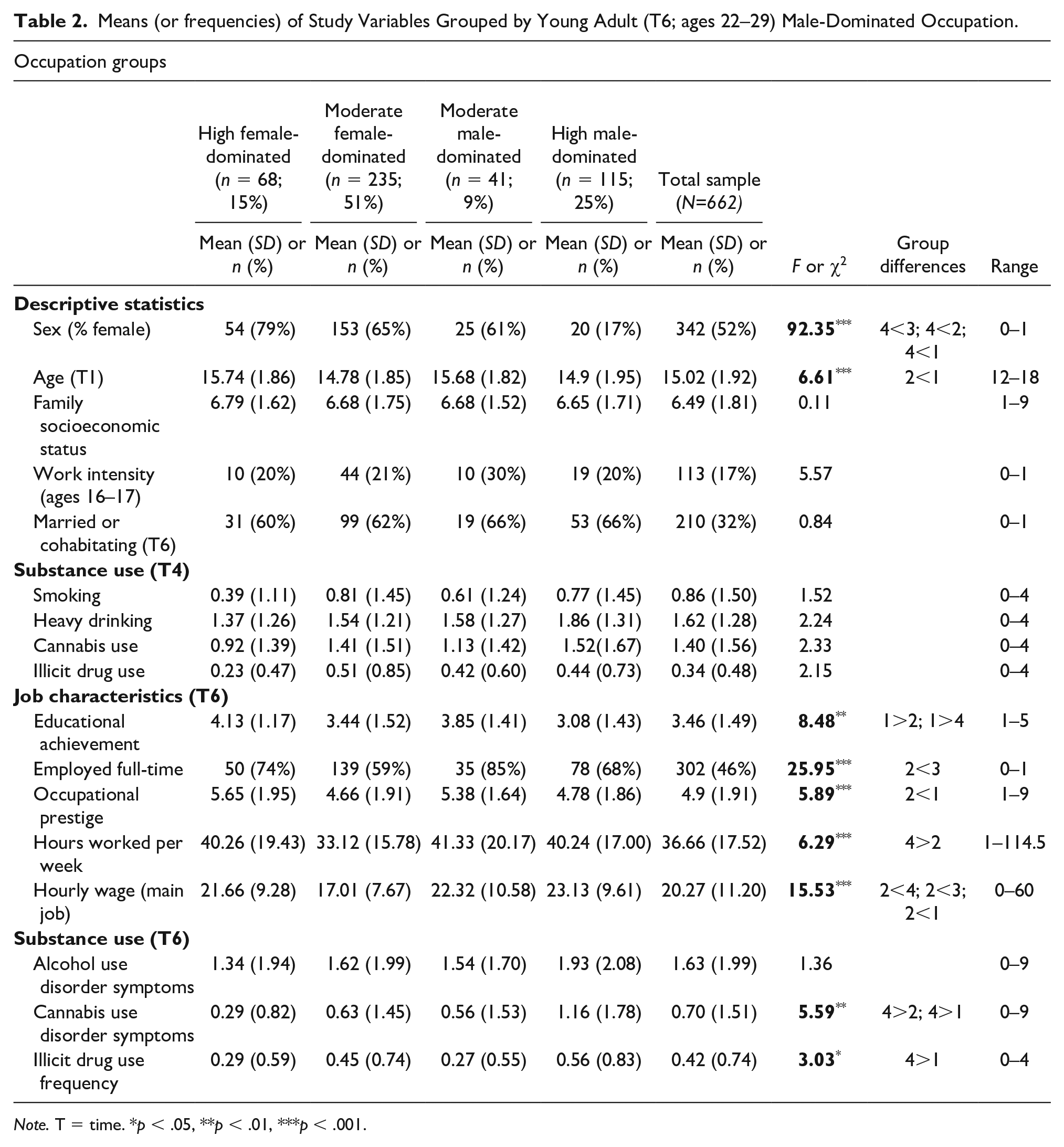
Note. T = time. *p < .05, **p < .01, ***p < .001.
Full Sample
Table 3 presents the standardized estimates and standard errors of the T1 (ages 12–18) covariates on each model variable. Of note, sex was related to T4 substance use and T6 GSO, with males using more substance and being employed in more male-dominated occupations. Age at T1 was related to work intensity, substance use at T4 and GSO; participants who were older at T1 reported higher levels of work intensity, more substance use in early young adulthood, fewer male-dominated occupations and more cannabis use disorder symptoms in young adulthood. As expected, heavy drinking in adolescence was related to more substance use at T4, but also fewer cannabis use disorder symptoms at T6. Adolescent cannabis use was related to more substance use at T4, higher employment in male-dominated occupations, and more cannabis use disorder symptoms, but less illicit drug use, in young adulthood.
Standardized Estimates (Standard Errors) of Covariates in the Path Model for the Total Sample.

Note. T = time; SES = socioeconomic status. *p < .05, **p < .01, ***p < .001.
Figure 1 presents findings for the hypothesized path model for the full sample. The model demonstrated adequate fit to the data (RMSEA = 0.08 [90% CI = 0.07, 0.09]; CFI = 0.91; SRMR = 0.05). Work intensity of more than 15 hr a week at ages 16–17 (T1–T3) was positively associated with subsequent substance use at T4 (ages 18–25; β = 0.19, SE = 0.06, p = .002). The path from adolescent work intensity to male-dominated occupations was not significant (β = 0.07, SE = 0.08, p = .356). As expected, T4 substance use was strongly associated with later (i.e., T6; ages 22–29) alcohol- and cannabis-use disorder symptoms and illicit drug use (see Figure 1). Being employed in a more male-dominated occupation was positively associated with cannabis-use disorder symptoms in young adulthood (T6; ages 22–29; β = 0.17, SE = 0.06, p = .004), but not alcohol-use disorder symptoms or illicit drug use in the full sample. Joint significance tests of the mediation pathways were not significant (p’s > .05; estimates are not reported, contact the authors for details).

Associations between adolescent work intensity, early young adulthood substance use, young adulthood gender-segregated occupation, substance use disorder-related symptoms, and illicit drug use for the full sample. The moderating path (dashed line) of for low (high in parentheses) SES for GSO to CUD-related symptoms is shown. RMSEA = 0.08[90% CI = 0.07, 0.09]; CFI = 0.91; SRMR = 0.05. Standardized estimates are shown. Note. GSO = gender-segregated occupation; AUD = alcohol use disorder; CUD = cannabis use disorder. Model adjusts for sex, age, family socioeconomic status, and adolescent heavy drinking and cannabis use.
The chi-square difference test for the weighted least squares estimator compared changes in model fit resulting from freeing (H1 model) and imposing (H0 model) equality constraints across paths to assess differences for males and females and for youth from high versus low SES. None of the paths differed by sex (p’s >.05). Low and high family SES groups differed on one hypothesized path (χ2(1) = 9.75, p = .002). Employment in a male-dominated occupation predicted cannabis-use disorder symptoms for the low (β = 0.53, SE = 0.12, p < .001), but not for the high (β = 0.10, SE = 0.07, p = .122), family SES group (Figure 1).
Discussion
Consistent with life course development and gender socialization theories, longitudinal pathways are hypothesized between work intensity (at ages 16–17) and substance use (T4, ages 18–25) and with subsequent young adults’ (T6, ages 22–29) employment in male-dominated occupations and their problematic substance use (i.e., alcohol- and cannabis-use disorder symptoms and illicit drug use). The moderating effects of biological sex and family SES were also tested. The proposed theoretical model was partially supported; work intensity was associated with adolescent substance use, which in turn, was related to substance use disorders in young adulthood. Work intensity in high school did not predict subsequent employment in male-dominated work. However, employment in a male-dominated occupation in young adulthood was associated with greater cannabis use disorder symptoms for youth from lower, but not higher, SES families. Models did not differ by biological sex.
As expected, work intensity in adolescence was moderately associated with substance use in early young adulthood (T4; ages 18–25). In the full sample model, after accounting for SES, T1 age, sex, and T1 substance use, neither adolescent work intensity nor adolescent (T4) substance use was associated significantly with employment in male-dominated occupations in young adulthood. It is possible that this effect would be specific to engagement in high-intensity work in male-dominated occupations in adolescence. Occupational choices are multiply determined and unobserved variables including educational ability, occupational opportunities, and personal motivation may be mediators of the proposed links between high-intensity work and subsequent circumscription of adolescent careers toward male-dominated occupations (Porfeli & Vondracek, 2009).
Overall these findings point to the potential influence of employment risks that may have developmentally timed effects on problematic substance use in late adolescence and young adulthood. High-intensity work in adolescence was related to substance use at ages 18–25. In addition, employment in male-dominated occupations in young adulthood (which was related to cannabis use disorders in young adulthood for youth from low SES families) may be implicated in the paths to early-onset substance use disorders. The association between adolescent work intensity and subsequent substance use has been reported in previous research (Bachman et al., 2011; Staff et al., 2009). Youth who works more than their peers in high school may have more expendable income, greater exposure to adults of legal drinking age, and less commitment to schooling (Staff et al., 2010). Contrary to career development theory (Luke & Redekop, 2014; Porfeli & Vondracek, 2009), adolescent work intensity was not related to employment in male-dominated occupations in young adulthood. Many of the high school students in the current sample were employed in minimum wage jobs in retail or the fast-food industry and there may be less gender segregation in these types of jobs (Statistics Canada, 2013). It is possible that the effects of work intensity operate indirectly through their effects on high school success, which, in turn, limit adolescent occupational choices and opportunities for postsecondary education (Staff et al., 2009). Substance use in adolescence, and possibly its associated lifestyles, were moderately predictive of young adult substance use problems. The findings are also consistent with the research showing adolescent substance use predicts future problematic use (Levine et al., 2017) and occupational problems (Thompson et al., 2019).
For youth from low-income families, employment in more male-dominated work environments was associated with more symptoms of cannabis use disorder after controlling for the substantial effects of prior substance use. Working in male-dominated jobs was not associated with alcohol use disorders or illicit drug use. Alcohol is the most commonly used substance and is the preferred substance of men (Health Canada, 2012) and it may not differentiate among men engaged in different work contexts due to its widespread acceptance and use. Socialization in male-dominated working environments with permissive drinking or substance use norms may add to the likelihood of cannabis use disorders (Lemle & Mishkind, 1989; Willott & Lyons, 2012). While no previous research has examined these associations in young adults, a systematic review of risk factors related to alcohol use among workers in male-dominated industries reported that problematic alcohol use was associated with high-stress jobs, low occupational status (unskilled and manual workers), and work environments that have permissive drinking norms (Roche et al., 2015). It is also possible that pain from injuries or muscle demands drive substance use for some youth, whereas work stress, seasonal employment, social isolation, or poor future prospects are associated with substance use for others. Youth in male-dominated jobs also had higher incomes at ages 22–29 (and possibly more work experience and expendable income) than all other groups, but they were less educated and had lower prestige jobs indicating their future prospects may be limited.
Limitations
Generalizability of the findings is limited by the predominantly Caucasian, Canadian sample of youth. Data are also self-report, which could lead to under-reporting of substance use due to social bias; however, all measures were highly consistent across each of the six assessments, suggesting the self-reports were reliable. Attrition by T6 included more males than females and youth of lower socioeconomic status limiting the power for analyses (e.g., power may be insufficient to assess the effects of gender-segregated occupations by sex as there were very few females in male-dominated jobs). It may also be important for future research to investigate ways in which biological sex and employment in gender-segregated work interact to influence substance use disorders for female-dominated jobs (Roche et al., 2015).
Conclusions
Research on the developmental paths that precede young adult males’ higher risk for substance use disorders is needed to guide public health and prevention approaches for resolving this gendered health-inequity. Over the past several years, policy makers in Canada have incentivized apprenticeships and youth work in the trades in high school—“requiring 900 hours to the ITA [Industry Training Authority] by December 31 of the school year the student turns 19” (Government of British Columbia, n.d.). This high level of paid work experience in high school may expose young adults to permissive substance use norms and limit long-term occupational prestige.
The consequences of this health inequity can be severe. Cannabis use disorders and illicit drug use are evident in youth as young as 22–29 years and pathways to more severe drug problems need to be investigated. For example, the recent British Columbia (BC), Coroner’s retrospective investigation of 872 individuals who died from illicit drug overdoses in BC (Services, 2018) identified that the majority of those who died were men (81%), unmarried (65%), aged 30–49 (49%), and unemployed (56%). These deaths were related to earlier histories of substance use and abuse as well as employment in male-dominated occupations. Of those who were employed, 55% were in male-dominated trades and transport and 21% were in female-dominated service industry work.
In this randomly recruited, community-based sample, adolescents who worked more than 15 hr per week in high school were more likely to be using illicit substances than those with fewer than 15 hr of work per week. Youth using more substances as adolescents were at greater risk of reporting symptoms of alcohol and cannabis disorders and illicit drug use as young adults. Youth from lower SES families who were employed in predominately male-dominated occupations were more likely to report higher cannabis-use disorder symptoms as young adults. Continued research is needed to better understand adolescents’ career choices for male-dominated jobs, as well as how male-dominated occupations may contribute to higher cannabis use problems (e.g., social isolation, disrupted relationships, job stress, permissive norms, and seasonal work). Nevertheless, many steps to reduce these risks are possible. Reframing the narratives linking masculinity (stoicism and self-reliance) and social drinking (or recreational cannabis use) to focus on the need to prevent problematic use may increase awareness of this health inequity. It is also necessary to reduce stigmas and moral judgements against substance use and substance use disorders in male-dominated work and to enhance the ability of individuals to self-assess their problematic use concerns and motivation to change, as well as to increase availability of confidential, work-based interventions for young adults.
Supplemental Material
Supplemental_material – Supplemental material for Male-Dominated Occupations and Substance Use Disorders in Young Adulthood
Supplemental material, Supplemental_material for Male-Dominated Occupations and Substance Use Disorders in Young Adulthood by Bonnie Leadbeater, Megan E. Ames and Alejandra Contreras in American Journal of Men’s Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Victoria Healthy Youth Survey study has been financially supported by grants from the Canadian Institute for Health Research (#43275; #79917; #93533; #130500).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.