
Abstract
Erectile dysfunction is common in adult men, particularly those with hypertension and diabetes. The present study determines the effectiveness of angiotensin receptor blocker (ARB) drugs on erectile function in hypertensive male adults. For this purpose, CENTRAL and MEDLINE and reference lists of the articles were searched. The randomized controlled trials (RCTs) were selected that compared ARBs with conventional therapy or no treatment in men of any ethnicity who were presented with hypertension and/or diabetes. A total four trials that had 2,809 men were included. Three trials reported adequate random sequence allocation, two reported adequate blinding. Attrition bias is low in one of the included studies. All three studies are of low risk of selective reporting bias. There was an improvement in sexual activity with ARBs (valsartan) (mean difference (MD): 0.71, 95% Confidence Interval (CI) 0.66 to 0.76, I2 statistic = 0%). However, the erectile functions did not increase significantly in ARBs (losartan or telmisartan) treated men as compared to control or placebo (n = 203 vs n = 232; MD: 1.36; 95% CI: −0.97 to −3.69; I2 statistic = 80%). These results suggested that ARBs significantly improved sexual activity among hypertensive men. However, the erectile function was not significantly improved in ARBs treated men as compared to the control or placebo-treated. There were limited studies available. Hence, additional studies are needed to support findings from this review. ARBs should be considered when prescribing antihypertensive drugs to men.
Keywords
Erectile dysfunction (ED) is an inability to achieve or maintain an erection sufficient for sexual intercourse. It can occur at any age, but it is more common in older men. Hypertension alongside its medication is the most common comorbidity of ED as 67%–68% of hypertensive men have some degree of ED (Kloner, 2007).
This association of ED and hypertension is explained by an age-related loss of smooth muscles from peripheral vasculature and corpora, hypertension-related endothelial dysfunction, and/or upregulation of the renin–angiotensin system (RAS) (Clavijo et al., 2014; Jin, 2009; Kloner, 2007).
Angiotensin II (Ang II) is the main effector of RAS that regulates important physiologic functions. An abnormal increase in Ang II levels induces vasoconstriction, endothelial dysfunction, vascular remodeling, and insulin resistance, leading to the development of assorted diseases such as hypertension, atherosclerosis, cardiac hypertrophy, and diabetes (Jin, 2009).
Many organs and tissues, such as heart, brain, kidney, blood vessels, and penis also contain components of the RAS, functioning in a paracrine manner (Bader & Ganten, 2008). Tissue RAS synthesizes Ang II locally and is modulated independently of systemic RAS. The Ang II levels were 30% higher in the cavernous blood than that in systemic blood (Becker, Uckert, Stief, Scheller, et al., 2001; Becker, Uckert, Stief, Truss, et al., 2001). Local Ang II may have direct effects on erectile function as shown by angiotensin II intracavernosal injection, which causes the spontaneous erection to be terminated (Baumhakel et al., 2008). It may be due to the regulation of neuronal impulses from the sacral spine or the brain itself (Llisterri et al., 2001).
The previous studies suggested that Ang II stimulates angiotensin receptor type I (AT1) that may increase intracellular calcium, inhibit myosin light chain phosphatase, increase oxidative stress, and decrease the bioavailability of nitric oxide (NO) in cavernosal smooth muscles that increase muscle tone and keep the penis in the flaccid state (Jin, 2009).
According to previous studies, the prevention of ED may be secondary to the correction of hypertension. Antihypertensive drugs such as diuretics, adrenergic antagonists, and calcium blockers either have no effect or worsen erectile function, while angiotensin receptor blockers (ARBs) have no significant negative effects but beneficial effects (Doumas & Douma, 2006; Fogari et al., 1998, 2001, 2002; Manolis & Doumas, 2008). ARBs are a group of drugs, which are used to treat high blood pressure and heart failure. ARBs block the action of Angiotensin II by preventing it from binding to AT1-receptor. In a trial, Angiotensin II injected into corpora cavernosa terminates spontaneous erection, while the intracavernosal injection of losartan has the opposite effect (Doumas & Douma, 2006). There are studies that reported that the treatment of hypertensive patients with ARBs resulted in the improvement of sexual activity and erectile function (Doumas & Douma, 2006). In a trial done on diabetic rats, renin–angiotensin system components were upregulated and resulted in increasing concentrations of angiotensin II. In the study, losartan is administered that blocked the effect of Angiotensin II causing subsequent downregulation of AT1 expression and Angiotensin II generated locally, and partially restored erectile function (Yang et al., 2009).
Inhibition of the renin–angiotensin system may help improve erectile function by inhibition of the effects of angiotensin II in the corpus cavernosum (Baumhakel et al., 2008). Another way to reduce the effect of Angiotensin-II that proven to improve erectile function is by using angiotensin-converting enzyme inhibitors (ACEi). However, ARBs being tolerable in patients intolerant to ACEi are favored (Bohm et al., 2010). Previous studies also reported that ARBs caused lower rates of adverse events (i.e., cough, angioedema, headache, respiratory infection, dizziness, and fatigue) comparable to placebo and lower than ACEi, diuretics, and other antihypertensive agents (Abraham et al., 2015).
Summarized information on the effect of angiotensin receptor blocker drugs, such as valsartan and losartan on sexual activity improvement besides their hypotensive effect might help hypertensive patients and with erectile dysfunction along with the practitioners to pick the best treatment. The aim of this meta-analysis is to report the effect of ARBs on the improvement of erectile dysfunction in hypertensive men.
Methods
This meta-analysis was conducted by following the Cochrane handbook for systematic reviews of interventions and GRADE assessment for quality of evidence.
Search Strategies
The Cochrane Central Register of Controlled Trials (CENTRAL) (latest Issue) and MEDLINE (1966 to present) were searched by using the terms “angiotensin receptor blocker, erectile dysfunction, sex.” The reference list of identified studies and review articles were also screened in order to find unpublished or unidentified trails by electronic searches. Furthermore, the ongoing trials were searched through the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (http://www.who.int/ictrp/en/ and www.clinicaltrials.gov).
Eligibility Criteria
Only open-labeled and blinded studies published in English on randomized control trials (RCTs) that compared the efficacy of the standard prescribed oral dosage of at least one ARB against conventional therapy or placebo for treatment of erectile dysfunction in newly or previously diagnosed hypertensive and/or diabetic men were considered. The men were previously either on any antihypertensive drug or not. The sexual function was assessed by using a physician-assisted or self-administered questionnaire.
Study Selection
The titles and abstracts were scanned from the searches and obtained full-text articles when they appeared to meet the eligibility criteria, or when there was insufficient information to assess eligibility. The eligibility of the studies was assessed independently by authors and documented the reasons for exclusion. Any disagreement on the study selection was resolved by discussion and sometimes authors of that study were also contacted for further clarification.
Data Extraction
Information about the study setting, the region where the study was conducted, participant characteristics (age, sex, and ethnicity), methodology (number of participants randomized and analyzed, duration of follow-up), type of drug use, method for diagnosing erectile dysfunction, medication used to treat erectile dysfunction and its complications, and occurrence of related adverse events was collected from eligible studies by using a form by authors independently. The predefined primary outcomes were the frequency of sexual activity and erectile function. Whereas, the secondary outcomes were plasma testosterone level and adverse events.
Risk of Bias Assessment
The risk of bias was assessed based on random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, completeness of outcome data, the selectivity of outcome reporting, and other biases. The risk of bias was categorized into high, low, and unclear. Any disagreement in this regard was resolved by discussion.
Statistical Analyses
The treatment effect was calculated as mean differences (MDs) with 95% confidence intervals (CIs). The heterogeneity was assessed and reported by using the fixed-effect model or random effect model according to the degree of significant clinical or statistical heterogeneity in Review Manager 5.3 software (RevMan 2014). The heterogeneity was first assessed at face value by comparing populations, settings, interventions, and outcomes and then by using I² statistic. The heterogeneity was interpreted according to the Cochrane Handbook for Systematic Reviews of Interventions as 0% to 40% might not be important, 30% to 60% may represent moderate heterogeneity, 50% to 90% may represent the substantial heterogeneity, and 75% to 100% would be considerable heterogeneity.
The subgroup analyses of the duration of hypertension and age of the patients could not be included due to limited numbers of RCTs available for this meta-analysis. A sensitivity analysis was performed to investigate the impact of risk of bias for sequence generation and allocation concealment of included studies. If there were sufficient studies, we intended to construct funnel plots to assess the possibility of reporting bias or small study biases, or both.
Grading the Quality of Evidence
The quality of evidence was assessed for primary and secondary outcomes, according to the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach, classified as very low, low, moderate, or high. The GRADE approach specifies four levels of quality, the highest of which is for randomized trial evidence. It can be downgraded to moderate, low, or even very low-quality evidence, depending on the presence of risk of bias, inconsistency, indirectness, imprecision, and publication bias. The GRADEpro software was used to reflect the quality of evidence for each individual outcome and the assessment is being phased in together with the “Summary of findings” (SoF) table (GRADEpro 2014).
Results
Study Selection
Initially, a total of 113 records were retrieved through electronic searches and three additional records through other sources (Figure 1). After removing duplicates, 78 records were screened sequentially for titles and abstracts whereas full texts of only seven articles for eligibility. Three articles were excluded with reasons:(i) no comparable groups because compared with or without sexual dysfunction (Grimm et al., 1997); (ii) no placebo control group (Dusing, 2003) and (iii) nonrandomized control trial (Subramanian et al., 1996). Finally, four trials for qualitative and quantitative synthesis were included and analyzed (Bohm et al., 2010; Chen et al., 2012; Della Chiesa et al., 2003; Fogari et al., 2002).

Flow chart of the study selection.
Characteristics of Included Studies
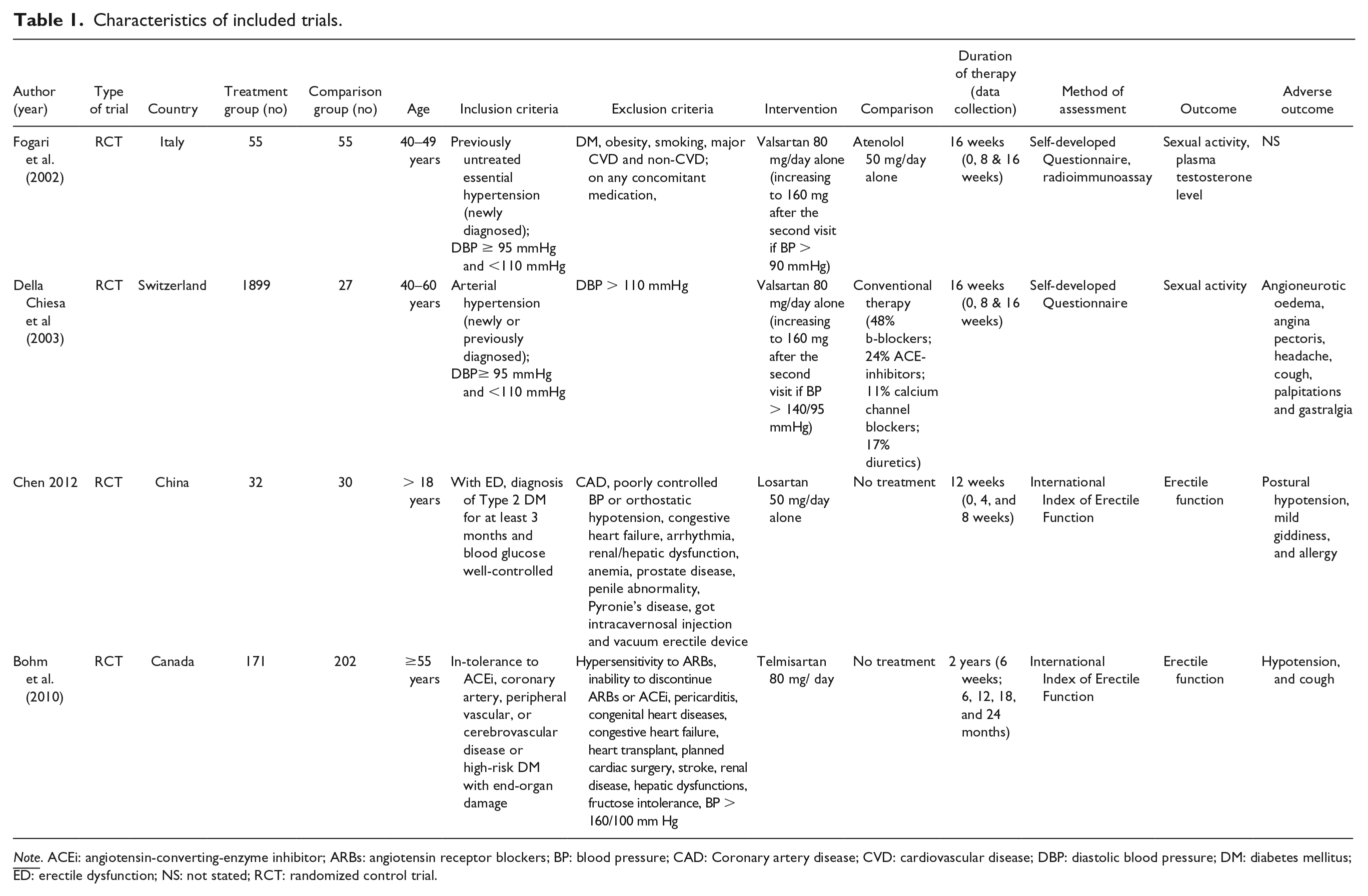
The included four trials had a total of 2,809 participants. Three of the trials were supported by educational grants (Bohm et al., 2010; Chen et al., 2012; Della Chiesa et al., 2003). One trial did not report any funding (Fogari et al., 2002). Table 1 summarizes the characteristics of the included trials.
Characteristics of included trials.
Participants
Two of the trials were conducted on patients with hypertension, both newly diagnosed and with a previously known history of high blood pressure (Della Chiesa et al., 2003; Fogari et al., 2002). One trial was conducted on diabetic men (Chen et al., 2012). Whereas, another trial was conducted on CVD patients with diabetes (Bohm et al., 2010). None of the trials mentioned the setting from which the participants were recruited. Furthermore, two trials involved patients with ED (Bohm et al., 2010; Chen et al., 2012), one trial involved only patients without any previous sexual dysfunction (Fogari et al., 2002) and another trial did not mention whether included patients were with or without sexual dysfunction (Della Chiesa et al., 2003). One trial reported 26 dropouts due to loss of follow-ups during visits or refused to take the drugs (Della Chiesa et al., 2003) and another trial mentioned dropouts of 19 taking telmisartan and 31 taking placebo (Bohm et al., 2010). The included studies randomized participants either into four groups (control: diabetic-ED, diabetic-ED on Tadafil 5 mg, diabetic-ED on losartan, and diabetic-ED on Losartan and Tadafil) (Chen et al., 2012), three groups (receiving 80 mg valsartan, valsartan and hydrochlorothiazide, and conventional therapy) (Della Chiesa et al., 2003), or two groups (receiving valsartan 80 mg, and atenolol 50 mg or telmisartan 80 mg, and placebo 80 mg) (Bohm et al., 2010; Fogari et al., 2002).
Intervention
Participants in the trials were randomized into intervention and control groups. Two trials used valsartan as intervention drugs as an 80 mg daily dose and the dosage was increased if the blood pressure remained elevated on the next visit. Both of the trials assessed the outcomes at 8 weeks and 16 weeks (Della Chiesa et al., 2003; Fogari et al., 2002). One trial used losartan at the dosage of 50 mg daily and did not report any increase in dosage. The assessment was done at 12th week (Chen et al., 2012). Another trail used telmisartan 80 mg daily and assessments were done every 6 months (Bohm et al., 2010). Two trials were conducted for 16 weeks (Della Chiesa et al., 2003; Fogari et al., 2002) and one trial for 12 weeks (Chen et al., 2012). Whereas, another trial was conducted for 2 years (Bohm et al., 2010).
Outcomes
Two trials reported sexual activity contributing to the primary outcome. Both trials assessed the outcome using self-developed questionnaires (Della Chiesa et al., 2003; Fogari et al., 2002). The questionnaire was filled up by the treating physicians (Della Chiesa et al., 2003) or by the participants themselves (Fogari et al., 2002). Two trials measured the outcome as the erectile function that was assessed by using a self-administered questionnaire of the International Index of Erectile Function (IIEF) (Bohm et al., 2010; Chen et al., 2012). Chen et al. (2012) measured erectile functions in terms of sexual encounter profile (SEP) questions, that is, SEP-2 and SEP-3 and the global assessment question (GAQ) (Chen et al., 2012).
Quality of the Studies
The assessment of the risk of bias is presented in Figures 2 and 3. Figure 2 presents the proportion of studies assessed as the low, high, or unclear risk of bias for each risk of bias indicator. Figure 3 presents the risk of bias indicators for individual studies.

A graph of the risk of bias according to review authors’ judgments about each risk of bias item presented as percentages across all included studies.

A summary of the risk of bias according to review authors’ judgments about each risk of bias item for each included study.
Allocation
Three trials did not describe the method of randomization used (Chen et al., 2012; Della Chiesa et al., 2003; Fogari et al., 2002) that posed an unclear risk of bias. Only one study described randomization through a central automated telephone service (Bohm et al., 2010).
Blinding
Conventional therapy remained as a control group in one of the trials (Della Chiesa et al., 2003). The person responsible for participants’ care and participants were blinded in two trials (Bohm et al., 2010; Fogari et al., 2002) but the outcome assessment was done by patient self-assessed sexual activity for a month (Fogari et al., 2002) and erectile function according to IIEF (Bohm et al., 2010). Blinding was not done in the remaining two trials (Chen et al., 2012; Della Chiesa et al., 2003) and the outcome assessors were either physicians for sexual activity (Della Chiesa et al., 2003) or patients themselves evaluated erectile function by using the IIEF-5 (Chen et al., 2012).
Incomplete Outcome Data
Two trials did not report any withdrawal; hence judged it as an unclear risk of attrition bias (Chen et al., 2012; Fogari et al., 2002). One trial mentioned no withdrawal, hence judged it as a low risk for attrition bias. A study mentioned 26 dropouts (Della Chiesa et al., 2003), while another reported 50 dropouts (Bohm et al., 2010). Furthermore, two of the studies also received incomplete outcome data (Bohm et al., 2010; Della Chiesa et al., 2003). One of these studies imputed incomplete data by using standard methods (Bohm et al., 2010) whereas, another excluded incomplete questionnaires from the final analysis (Della Chiesa et al., 2003).
Selective Reporting
All four trials reported the outcomes as specified in their methods section (Bohm et al., 2010; Chen et al., 2012; Della Chiesa et al., 2003; Fogari et al., 2002).
Other Potential Sources of Bias
No other potential sources of bias were detected.
Efficacy in the Form of Sexual Activity
The effect sizes and CIs of the individual comparisons of ARBs for sexual activity are presented in Figure 2. These two trials reported sexual activity after 16 weeks of the intervention of valsartan (Della Chiesa et al., 2003; Fogari et al., 2002). The effect size measured as MD varied from 0.71 (95% CI: 0.66–0.76) to 0.78 (95% CI: 0.53–1.03). The pooled mean effect size was 0.71 (95% CI: 0.66–0.76). The I2 statistic was 0%. Participants received valsartan significantly improved their number of sexual activity per week (Figure 4).

Individual and pooled effect size (mean difference and confidence intervals) of sexual activity in men treated with ARB (valsartan) compared to control (conventional therapy or atenolol) according to the fixed-effect model.

Individual and pooled effect size (mean difference and confidence intervals) of erectile function in men treated with ARBs (losartan vs telmisartan) compared to control (no treatment) or placebo-treated according to the random effect model of erectile function.
Efficacy in the Form of Erectile Function
The effect sizes and CIs of the individual comparisons of ARBs for erectile function are shown in Figure 3 (Bohm et al., 2010; Chen et al., 2012). The effect size varied from 0.32 (95% CI: –0.56 to 1.20) to 2.72 (95% CI: 0.78–4.66). The pooled mean effect size was 1.36 (95% CI: –0.97 to 3.69). The I2 statistic was 80%. Participants received one of the ARBs (losartan or telmisartan) did not improve erectile function significantly compared to those receiving placebo or control for 2 years or 12 weeks, respectively (Figure 5).
However, the percentages of positive answers to SEP-2 (successful penetrations) were higher (p < .05) in the losartan treatment group (65.6%; 95% CI: 49.2–82.1) than the control group (40.0%; 95% CI: 22.5–57.5) after intervention for 12 weeks. Similarly, the percentages of positive answers to the SEP-3 (intercourse completions) were also higher (p < .05) in the losartan treatment group (59.4%; 95% CI: 42.4–76.4) as compared to the control group (33.3%; 95% CI: 16.5–50.2). Furthermore, the GAQ indicated that the losartan (62.5%; 95% CI: 45.7–79.3) was superior (p < .05) to the control (16.7%; 95% CI: 3.3–30.0) in improving erections in diabetic men.
Efficacy in the Form of Plasma Testosterone Level
One trial involving 110 participants also reported plasma testosterone levels after 16 weeks of the intervention that were 18.3 nmol/L and 13.8 nmol/L (mean difference (95% CI) 4.50 (2.78, 6.22), fixed effect, p < .00001) for valsartan and the comparison group of atenolol, respectively (Fogari et al., 2002).
Adverse Events
Adverse events were reported in three studies. These include common events such as postural hypotension, mild giddiness, allergy, headache, cough, palpitations, and gastralgia with the use of ARBs. These adverse events were mostly mild and did not affect patients’ participation and completion of the studies (Bohm et al., 2010; Chen et al., 2012; Della Chiesa et al., 2003). One major adverse event (angioneurotic edema of the mouth) occurred in one patient, but the event disappeared with no further symptoms after stopping the medication (Della Chiesa et al., 2003).
Sensitivity Analysis
For all sexual activity outcomes, there was no substantial change in the effect size and CI after removing the trial with an unclear risk of bias for allocation concealment.
Quality of Evidence
The overall quality of evidence was moderate (Table 2).
Summary of findings.

Discussion
For the present meta-analysis, a comprehensive literature review was performed to determine the effectiveness of ARBs to treat ED. There were limited numbers of trials available for this meta-analysis. Four trials were included that is why the findings of this meta-analysis might not be applicable to ED of all etiologies. Nevertheless, the findings are of clinical importance in hypertensive and/or diabetic men. This review could not identify an association between the lower and higher dosage of ARBs used in the improvement of ED as the findings in patients who took a higher dosage after the first assessment period were not reported separately.
The quality of trial evidence was moderate. The included trials were judged as having a low, unclear and high risk of bias in all domains. The judgment was based on authors who made decisions after a detailed reading on the included trials and after a proper discussion. There was no evidence of selective reporting bias, although it cannot objectively be excluded as only one of the trials published a protocol (Bohm et al., 2010). The lack of information on random sequence generation in three of the included trials could lead to treatment effect bias in the study and subsequently on the review done (Chen et al., 2012; Della Chiesa et al., 2003; Fogari et al., 2002). This may also be contributed by the lack of blinding of participant and outcome assessor in two of the included studies (Chen et al., 2012; Della Chiesa et al., 2003). The rate of attrition was fairly low and one of the included studies carried out the intention-to-treat analysis. A little heterogeneity was found among the studies reported the sexual activity as an outcome (Della Chiesa et al., 2003; Fogari et al., 2002), while a huge heterogeneity (80%) among the studies reported erectile function as the outcome (Bohm et al., 2010; Chen et al., 2012). The overall level of evidence contributing to this review as assessed using the GRADE approach is of moderate quality.
Sexual activity, one of the outcomes of the present meta-analysis suggests that treating hypertensive men with standard dosages of one of the ARBs (valsartan) is effective to improve erectile function. Although the 95% CI was wide in the findings of the outcome, the outcome remained significant. However, in case of erectile function, one of the two included studies reported a statistically significant improvement of erectile function in diabetic men treated with losartan from baseline as compared to no difference in the control group, but the pooled effect size was not significantly higher in ARBs (losartan or telmisartan) treated diabetic and/or hypertensive men when compared to control or placebo groups.
These discrepancies may be due to the large heterogeneity (I2 = 80%) attributed to fewer studies, the use of the different types of ARB (losartan or telmisartan), and different durations of intervention (16 weeks vs 2 years) (Bohm et al., 2010; Chen et al., 2012). On the other hand, the studies that reported improved sexual activity due to valsartan treatment compared it with atenolol (beta-blockers) or conventional therapy (beta-blockers, diuretics, or calcium channel blockers) (Della Chiesa et al., 2003; Fogari et al., 2002). These beta-blockers, diuretics, or calcium channel blockers are known to lower erectile functions in men (Kloner, 2007). Therefore, a positive effect could be due to the deterioration caused by atenolol and other conventional therapies in comparison groups, not the improvement of erectile function due to ARB (valsartan) in treatment groups.
From the reported incidence of adverse events, the common side effects were postural hypotension mild giddiness, cough, allergy, headache, palpitations, and gastralgia. These side effects were reported by three of the included trials (Bohm et al., 2010; Chen et al., 2012; Della Chiesa et al., 2003). But, one trial reported the occurrence of one major adverse event, namely angioedema of mouth, which disappeared after stopping of study medication (Della Chiesa et al., 2003).
Though there is an evidence that using ARBs may improve sexual activity, it is suggested to further test the efficacy of ARBs for various sexual functions in hypertensive or diabetic men in comparison to the true placebo group in the double-blinded RCTs.
Limitations
There are a few limitations of this meta-analysis suggest a careful interpretation of the results. The included studies had limited information on blinding. There could be a selection bias and publication bias. The included studies were few and with small sample size. There could also be a certain bias because comparison and experimental groups were on different types of antihypertensive agents and ARBs, respectively.
Conclusion
ARBs significantly improved sexual activity among participants in the intervention group. However, the erectile function was not significantly improved in ARBs treated men as compared to the control or placebo-treated. The results of plasma testosterone levels were also limited due to a small number of included trials. Therefore, these discrepancies of the finding suggest further careful testing of the ARBs for different sexual functions in hypertensive and diabetic men in the true placebo-double-blinded trials.
Footnotes
Acknowledgements
The authors would like to thank Amran Mamat and Nurul Azurah Mohd Roni, librarians from Hamdan Tahir Library, for their assistance with database searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.