
Abstract
Male circumcision (MC) plays a significant role in reducing new HIV infections, particularly in high prevalence countries. This cross-sectional study assesses the prevalence of MC and attitudes toward MC among youth aged 15–18 years in The Bahamas, a medium HIV prevalence country. The survey included 797 young men who completed a questionnaire on MC. Data analyses included chi-squared tests.
The self-reported prevalence of MC among youth was 16.7% (121/759). Most of the circumcised youth were circumcised as infants, 84% (107/121) were pleased with their circumcision, and 71% would recommend it to others. For uncircumcised youth, 35% (189/533) would consider voluntary male circumcision (VMC) and 26% would recommend MC to others. In all scenarios, circumcised youth were more likely to be positive about MC. Among uncircumcised young men, being older (17–18 years compared to 15–16 years) was the only variable statistically associated with considering MC or recommending MC. After being presented with information on the benefits of MC for HIV prevention, the number of men who were positive about MC increased.
Most of the young men in this cohort would consider VMC for reducing HIV incidence. Also, many stated that, if they had a male child, they would have him circumcised. The attitudes of these youth emphasize the need to provide information on HIV in addition to general health benefits of MC if there were to be a sustainable MC program within this population.
Male circumcision (MC) is an effective method of reducing the incidence of HIV (Morris, Krieger, & Klausner, 2017; Williams et al., 2006). In many jurisdictions, particularly in high prevalence settings, it is an important and integral component of strategies to significantly reduce new HIV infections (Sharma et al., 2018; Weiss, Dickson, Agot, & Hankins, 2010). To be most effective, the approach must be multifaceted and adapted to the specific location and local conditions (Brooks et al., 2010). Factors to be considered include but are not limited to socioeconomic factors, knowledge and attitudes, and access to health care (Rodriguez et al., 2019).
Three randomized control trials (RCT) in Africa have demonstrated that voluntary MC reduces the risk of men contracting HIV by more than 50% (Chemtob et al., 2015; Mehta et al., 2013; Siegfried et al., 2003). More than 6 years later, follow-up studies continued to demonstrate a net benefit of MC in reducing the incidence of HIV within these settings (Mehta et al., 2013). According to a 2007 Cochrane review (updated from 2003), there is strong evidence that MC reduces HIV acquisition by 38%–66% within 24 months in heterosexual men (Siegfried et al., 2003; Siegfried, Muller, Deeks, & Volmink, 2009). It has been estimated that MC could avert 2.0 million new HIV infections and 0.3 million deaths over a 10-year period in sub-Saharan Africa (Williams et al., 2006). In Kenya, multiple cross-sectional studies have demonstrated that, with increased antiretroviral therapy (ART) and VMC, HIV incidence declined from 11.1 per 1000 person-years in 2011–2012 to 5.7 per 1000 person-years in 2012–2016, mainly due to MC (Borgdorff et al., 2018).
Results from other studies demonstrate that there may be a broader medical benefit of MC for the reduction of HIV transmission, including reduction in high risk human papillomavirus infection and genital warts, even within low prevalence settings (Smith et al., 2010; Tobian & Gray, 2011; Wamai et al., 2011; Warner et al., 2009). While there are no RCTs of MC in lower HIV prevalence settings, a cross-sectional study attributed lower prevalence of HIV in Israel because of its higher prevalence of MC (prevalence of MC is over 90%) when compared to the Netherlands and France, where MC is less than 10%. All countries had similar behavioral and economic situations (Chemtob et al., 2015).
Among some people, there remains the fear that MC will increase sexual risk compensation (increased number of sex partners, unprotected sex, etc.), which may then increase the incidence of HIV and other sexually transmitted infections. However, in the Kenyan and Ugandan trials, no significant differences were identified between circumcised and uncircumcised men with regards to increased risk behaviors (Bailey et al., 2007; Gray et al., 2007). There were some statistical differences between circumcised and uncircumcised men in the South African trial in the number of sexual contacts at the 12-month visit (p < .001) and at the 21-month visit (p = .0015), although this did not impact the protective effect of MC (Auvert et al., 2005).
MC is not routinely practiced in The Bahamas, as is the case with the rest of the Caribbean, and it is not supported by government programs (Duncan, 2010). Additionally, there are few people who practice religious MC. Data on MC are not routinely collected and conflicting information exists on the prevalence of MC for the region. Based on the relatively small number of Jewish and Muslim people in The Bahamas, it has been estimated that the prevalence of MC may be as low as 0.2% (Morris et al., 2016). Information from WHO shows an estimated prevalence of MC at less than 20% in the region (World Health Organization & UNAIDS, 2008). A few small studies in the Caribbean have reported MC rates between 5% and 14% in Jamaica and the Dominican Republic (Brito, Caso, Balbuena, & Bailey, 2009; Figueroa & Cooper, 2010; Walcott et al., 2013).
There is a paucity of information on young people’s general knowledge and attitudes toward MC in the Caribbean. Male youth are constituents of one of the key populations at risk for HIV infections in the Bahamas. This age group is the only group that has seen an increase in new HIV infections over recent years. Of most concern, cases among males in this age group tripled between 2006 and 2015 (Johnson, 2016). Youth perspectives on MC are important for deciding whether there can be a sustainable MC program, as they would be the target for a VMC program and would also soon be responsible for decision making for MC for their infants. Young men’s decision pathways on MC may be related their current knowledge and understanding about circumcision (Lane, Bailey, Luo, & Parks, 2018).
There are a number of issues and barriers to promoting VMC for HIV incidence reduction. The purpose of this study was to explore the practicality and acceptability of MC as a component of a program aimed at “getting to zero” new HIV infections in the Bahamas. It is important to note that circumcision was identified as one of the output strategies under Priority Area 6 of the Bahamas National HIV/AIDS Strategic Plan 2016–2021 (Ministry of Health Commonwealth of The Bahamas, 2016). The current study has been conducted to assess the prevalence of circumcision among Bahamian male youth, their satisfaction with being circumcised, the attitudes of young males, circumcised and uncircumcised, toward circumcision, including future sons, and the impact of health risk education on those decisions.
Methods
The Bahamas is made up of over 700 islands and cays spread over an area of more than 100,000 square miles. The majority (85%) of the population (estimated at 391,232 in 2014) reside in New Providence and Grand Bahama. This study is based on data from the “Getting to Zero HIV Infections” study of male circumcision in The Bahamas, a mixed-methods study conducted between 2014 and 2015 (George, Brennen, Roberts, Rabie, & Read, 2012). The established statistical division sampling frame was used to recruit participants. Permission was first obtained from the Ministry of Education to conduct the study. Individual school administrators were then approached for approval to utilize their sites. Approval was given to recruit the Health and Family Life classes to minimize academic disruptions. After the study coordinator reviewed the study with students, they were invited to complete the paper-and-pencil survey. Students who refused to participate were given general non-academic material to work on so that they would not be singled out for refusing to participate and participating classmates would not be interrupted. Once completed, the study coordinator thanked participants and facilitated a Q&A that followed each class. The survey was originally designed for young men, but due to stakeholder-expressed needs and the nature of the classrooms (coed), recruitment included males and females from high schools within the four major islands of The Bahamas. This analysis reports only the young men.
The study was done with the support of The Bahamas National HIV/AIDS program (NAP). The program has a well-established presence throughout The Bahamas and a trusted network of supporters. Established working relationships between The Bahamas Ministry of Health (MOH), NAP, and the Ministry of Education were utilized to recruit in-school youth between the ages of 15 and 18 years. The MOH and Ministry of Education work closely together on an ongoing, successful Focus on Youth (Deveaux et al., 2007) prevention research program in The Bahamas involving parents and children in improving sexual health communications. As such, there was an already established group of research assistants who assisted with study administration.
The study survey questions and interview scripts were adapted from “Circumcision: A Situation Analysis” (World Health Organization, 2009) to reflect the particular nuanced Bahamian social milieu. In addition to general demographic information, the survey included 10 items on abstinence and sexual behavior, 4 items on HIV testing, and 35 items on knowledge and attitudes toward MC. The survey took 20–35 min to complete. Participants were informed by the study team that the study was not about receiving circumcision. The study was approved by the University of Ontario Institute of Technology (REB 12-001) and The Bahamas Ministry of Health National Ethics Committee (HEA/27/26).
Descriptive statistics were conducted for all variables. The prevalence of MC was assessed based on self-reports. Prevalence is the number of young men who report circumcision divided by the number of men in the sample. Circumcision was defined as self-reported affirmative response to the question “Are you circumcised?” Those who reported no or I do not know were categorized as “no.” The outcome variables of interest for this analysis were whether young men would consider future circumcision; despite their young age, whether their future intention would be to have their sons circumcised; and whether they would recommend circumcision to others. The outcome variables were dichotomized into “yes” versus “no.” Chi-squared tests were conducted. Participants were free to disregard any question that they did not feel comfortable in answering; hence the denominator may change per question.
Before and After Information on MC
Participants were asked for their opinion on circumcision before and after presenting the following: Recent studies show that male circumcision reduces the risk of becoming infected with HIV. Being circumcised is not enough on its own to protect against HIV and circumcised men should continue using condoms when having sex.
The next statement on the general health benefits of circumcision followed:
Circumcision also has other health benefits. Baby boys have a lesser chance of developing infections; boys and men won’t have problems with the foreskin becoming too tight around the penis, and this decreases the chance of getting infections under the foreskin, and some sexually transmitted diseases.
Results
All 1553 students who were present in the classrooms participated in the study. Of these 51.3% (797) were males. Table 1 presents the general characteristics of the males in the sample. Age ranged from 15 to 18 years, median age being 16 years. Most participants were born in The Bahamas with less than 10% born in other countries (Haiti 1.0%, USA 4.7%, Jamaica 3%, other 1%). For those born outside of The Bahamas, 54.3% (43) had lived in The Bahamas for more than 10 years, 24% (18) had been residing for 6–10 years, and 18.7% (11) were there for 0–5 years.
Demographics Factors of School-Aged Young Men in the Sample (N = 797).

Prevalence of Self-Reported MC
Of the 797 males in the sample, 95.2% (759) answered the question on male circumcision status. There were 121 who reported “yes,” 602 reported “no,” and 36 reported “I do not know” to that question. Responses were dichotomized as “yes” versus “no.” The prevalence of self-reported male circumcision was 16.7 (121/723; 95% CI [14.1, 19.7]), when those who reported “I do not know” are excluded. There was no statistical difference in sexual debut between circumcised and uncircumcised males (p = .22). Characteristics of the sample relating to circumcision are shown in Table 2. Most reported that they were circumcised as infants (53.0%, 61/119) or as a child (34.8%, 40/119). Circumcision was mostly done at medical institutions (77.3%, 92/119) and the majority of young men were pleased with their circumcision status (85.7%).
Information Related to Male Circumcision of Young Males in the Sample.*
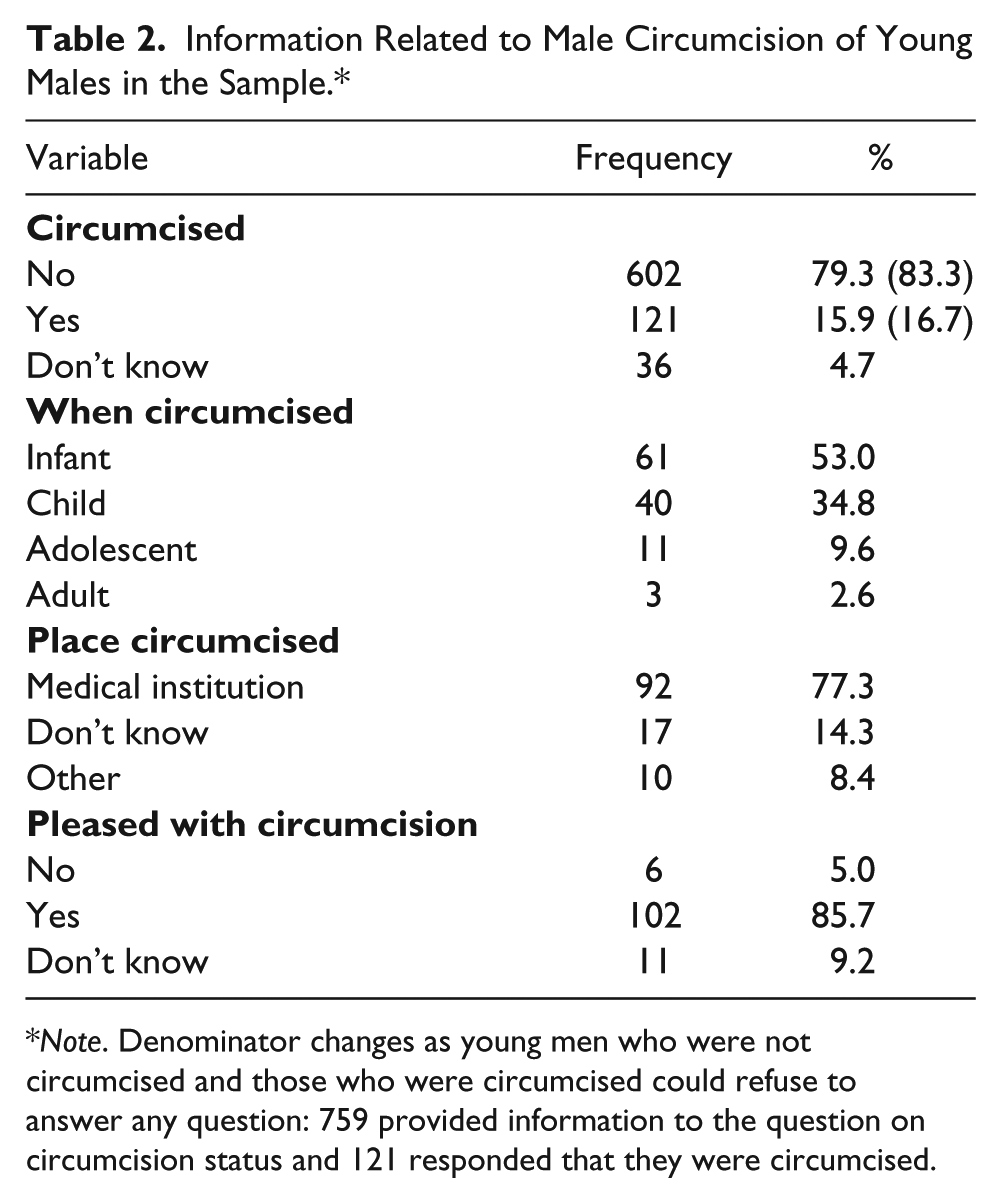
Note. Denominator changes as young men who were not circumcised and those who were circumcised could refuse to answer any question: 759 provided information to the question on circumcision status and 121 responded that they were circumcised.
Attitudes Toward MC
Of the 602 uncircumcised young men, 533 responded to the question about whether they would consider being circumcised. Of this group, 35.5% (189/533) said “yes,” they would consider circumcision; 49.5% (264/533) said “no,” they would not; and 15% were undecided. Table 3 compares the attitude of circumcised to uncircumcised males. With regards to wanting their future sons circumcised, circumcised young men were more likely to want their sons circumcised than uncircumcised young men (90.8%, 109/120 vs. 47.2%, 268/568; p < .001). When information on the benefits of MC was presented, circumcised men were more positive with regards to information on HIV (p < .0001), but there were no statistical differences between circumcised and uncircumcised men with regards to other health benefits of MC.
Attitude Toward MC Among Circumcised and Uncircumcised Young Men.*
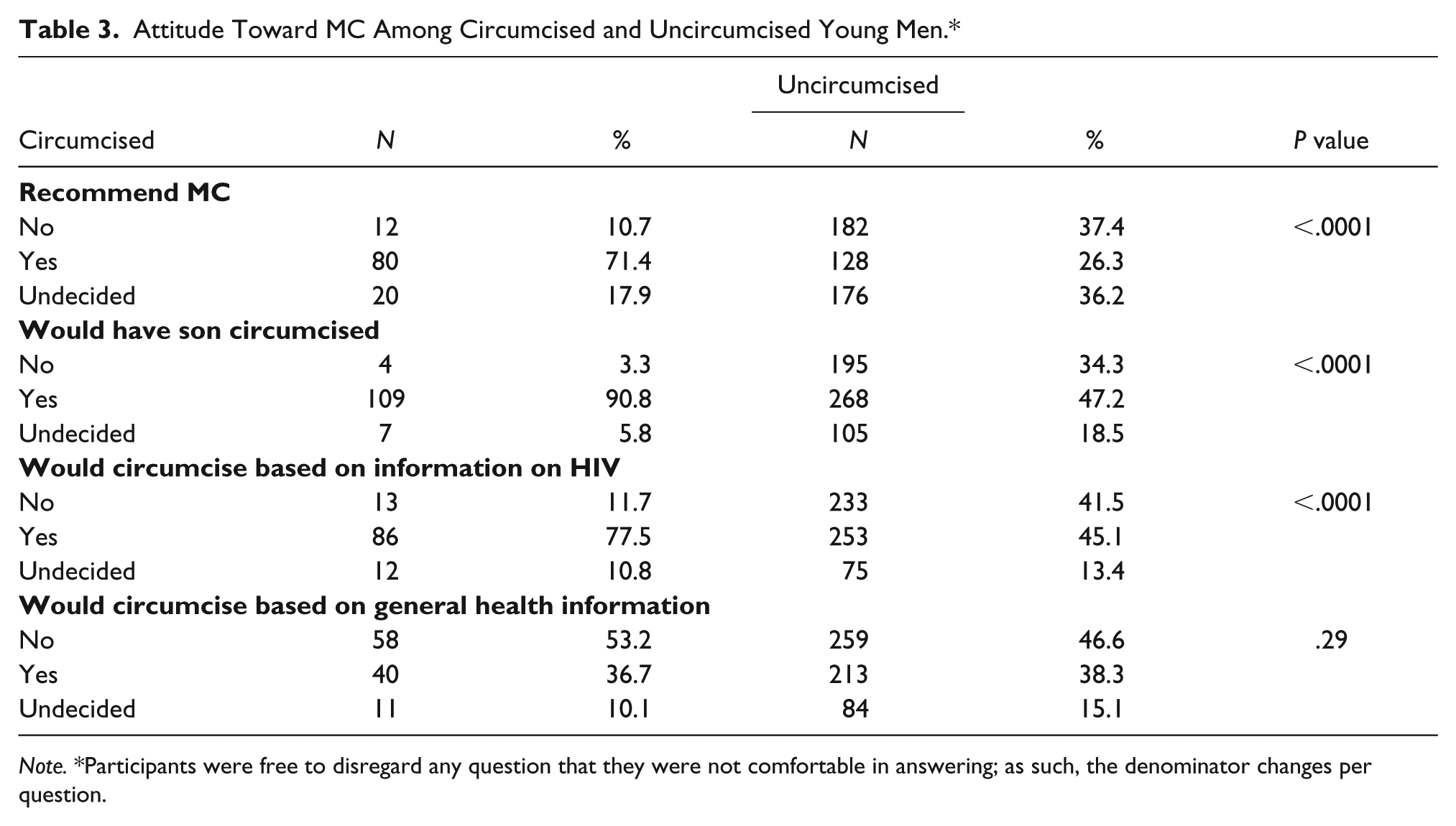
Note. *Participants were free to disregard any question that they were not comfortable in answering; as such, the denominator changes per question.
Factors Associated With Considering Circumcision, Recommending or Having Sons Circumcised, by Circumcision Status
To determine which factors were associated with young men
In testing the association between young men’s future decision to circumcise their sons with demographic variables, age appeared to have little association with that decision (for both circumcised and uncircumcised young men). Finally, among circumcised men, being older age (17/18 years; p = .04) was associated with “recommending male circumcision to others” but this was not the case for uncircumcised men when testing that association to others and demographic variables. Neither place of residence, religious service attendance, nor place of birth were associated with recommending circumcision.
Decision on MC After Information About HIV Prevention
Following the provision of information regarding the importance of male circumcision in HIV prevention, 255 of the uncircumcised young men who had originally said they would not consider voluntary circumcision responded (see Table 4). Of these, 22% (56/255) reported they would now consider being circumcised. However, 14.2% (26/183) of those who had a favorable attitude then said “no” and 45.6% (36/79) of the previously undecided then said “yes.” Chi-square test comparing before and after attitude was significant (p < .0001). Through analyses of the data, the significant total change to considering circumcision after presentation of the HIV information appeared to be led by those who were previously undecided.
Uncircumcised Males’ Attitudes Toward MC Before and After Information on HIV and Other Health Benefits of MC.

Opinion on MC After Information on Other General Health Benefits of Circumcision
Of the uncircumcised young men, 29.2% (75/257) who had originally said “no” to MC changed their opinion to “yes.” However, 41.8% (76/182) who originally said “yes” then said “no,” and of those uncircumcised who were originally undecided, 46.8% (36/77) changed to “yes.” Chi-square test comparing before and after attitude was significant (p < .0001). Through analyses of the data, the significant total change to considering circumcision after presentation of the HIV information appeared to be led by those who were previously undecided.
General Opinions About MC
A series of questions were asked about general opinion of MC which could impact the uptake of a circumcision program or be associated with risk compensation. Chi-squared analyses comparing circumcised to uncircumcised males are shown in Table 5. Uncircumcised men were more likely to believe that circumcision will lead to infection of the penis, result in excessive blood loss, and that a foreskin is needed but also that it helps to keep the penis clean (p < .001). On the other hand, circumcised young men were more likely to believe that MC improves manhood, results in longer sex, that condoms are not needed to protect them from HIV (p < .001).
Young Men’s Opinions on Male Circumcision.

Note. *Chi-squared test.
Discussion
The self-reported prevalence of MC among young men aged 15–18 years in The Bahamas is about 16.7%. This is a lower prevalence than the 20% estimated by medical practitioners for the general male population in The Bahamas (George et al., 2012) but higher than that reported in Jamaica and the Dominican Republic where estimates were between 5% and 14%, based on self-reporting (Figueroa & Cooper, 2010; Walcott et al., 2013). While the prevalence in our sample is also based on self-reporting, there is evidence that MC self-reports provide good measures of true MC rates (Odoyo-June et al., 2018).
While reasons for circumcision were not within the scope of this study, there is evidence that infant circumcision may be requested by parents based on their education, knowledge of circumcision, belief in the benefits of MC, and HIV knowledge (Mavhu et al., 2011). Parents may choose to circumcise their sons because of their personal beliefs of the benefit of circumcision, such as having their boys look like their dads (Waldeck, 2003) since there is a cost associated with this procedure. In the Caribbean, social standing and time lived away (migration) in areas where circumcision is the norm may also influence decisions on MC. Although the study collected information on the nationality of participants, it did not collect information about their parents’ migration pattern and so this hypothesis could not be tested. Future studies should explore the reasons parents choose to circumcise their children and the impact of migration patterns on MC.
The few studies on the psychological impact of male circumcision in early childhood demonstrate that boys were generally pleased with their circumcision (Morris et al., 2012). This study observed similar findings where 85% of the circumcised young men were pleased with their circumcision. This information is reassuring since some researchers have postulated that circumcision may have a negative impact on Caribbean young men’s self-esteem and may lead to stigmatization, bullying, and social alienation (Palitza, 2008).
Peer influence has an important impact on uptake of healthy behavior including MC uptake (Lane et al., 2018). This study suggests that both circumcised and uncircumcised young men would likely recommend circumcision to their peers, an important decisional factor in male circumcision uptake (Zanolini et al., 2016). This support for MC occurred before they were informed of the health benefits of MC and suggests that many young men in The Bahamas already have a positive view of MC. While most studies on peer influence in MC decisions discuss the influence of female partners (Carrasco, Wilkinson, Kasdan, & Fleming, 2018; Kaufman et al., 2018), one study reported that males have an important influence on each other toward MC (Macintyre et al., 2014). However, the investigator posited that there could also be negative peer pressure to comply to a new peer norm. In this study, young men were not asked to provide the source of information on MC although high school youth in The Bahamas are exposed to a Health and Family Life Education course which includes information on HIV.
When young men were provided with information on the benefits of VMC in reducing risk of HIV, almost a quarter who had originally responded “no” said they would consider circumcision. Also, almost half of those who were previously undecided about MC reconsidered the personal importance of MC. Based on these results, it can be theorized that educating young men on the health benefits of MC will improve their likelihood of future MC uptake. This change in attitude toward circumcision based on health benefits information is higher than what was reported in a small study clinical study in Jamaica, where 35% would consider circumcision after being told of the benefits (Figueroa & Cooper, 2010). In another study, in Jamaica, consideration for MC increased from 25% to 45%, after been given information on the benefits of MC (Walcott et al., 2013). Also, in a study from the Dominican Republic, consideration of MC increased from 29% to 67% after men were informed of circumcision benefits (Brito et al., 2009). It should be noted that the ages of participants in all the above studies were older than this study’s school-aged young men. Based on a review of the literature, no other study using a comparable school-aged group asked about young men’s willingness to be circumcised. This information is important as it indicates that, with only minimal educational information, young men would be willing to be circumcised to protect their health.
When asked about their having their future infants circumcised, the majority of circumcised young men responded that they would have their sons circumcised. This was not a departure from their favorable view of MC. However, almost half of the uncircumcised young men also desired this intervention for their sons. While most of these young men may not have begun parenthood, it is not unreasonable to pursue such inquiry since many young people in the region start parenthood at a young age and may be called upon to make the decision on circumcision for their sons. It is encouraging that, with the additional knowledge on the benefits of MC for the protection from HIV, the proportion of young men who favored MC also increased.
A series of questions about MC circumcision were included which could impact the uptake of a MC program or be associated with risk compensation or increased risk behaviors (Kalichman, Eaton, & Pinkerton, 2007). Many of the opinions suggest that circumcised men may be at risk for HIV if they were to act on those opinions. For example, they were more likely to believe that circumcised men do not need condoms to protect them from HIV. Further, some opinions such as MC proves manhood and that women prefer men who are circumcised may also increase their likelihood for risk compensatory behaviors (Eaton & Kalichman, 2007). The fact that uncircumcised men are more likely to respond that the head of the penis should be covered and that circumcision may lead of infection of the penis suggests that these opinions or beliefs may need to be challenged to improve VMC adoption (Carrasco, Wilkinson, Kasdan, & Fleming, 2019). However, uncircumcised young men’s opinion that circumcision improves hygiene while being a mediating moment to improve VMC should not be used in such a way to stigmatize or marginalize men who are not willing or ready to adopt VMC (Mavundla, Netswera, Toth, Bottoman, & Tenge, 2010). As such, there is a need to improve MC knowledge particularly among men who are circumcised or considering circumcision to prevent increased risk behavior.
Based on the knowledge, attitudes, and response to information given to high school young men, the introduction of circumcision into the health promotion approach of The Bahamas HIV/AIDS Strategic Plan should be feasible. The approach should target both infant circumcision and voluntary male circumcision for older males. In general, the young men who participated in the survey had a favorable attitude toward MC, with those who already were circumcised being satisfied and many of those who were not indicating that they would consider VMC. Also, importantly, the provision of health benefits information resulted in a significant number of individuals changing their attitudes toward VMC. In addition, many indicated that they would have future sons circumcised.
There are limitations to this study. This was a self-reported study and participants were free to disregard questions that they did not feel comfortable in answering. As such, the denominator changed per question, which could suggest some social desirability bias. The study was designed for young men to self-report circumcision and self-reporting may be biased. However, it is believed that this bias may be minimal since there were no differences in general attitude toward circumcision among circumcised young men compared to uncircumcised young men. No difference in the prevalence of MC between Bahamian born and foreign born was identified; however, we may have missed an important language/cultural group—the Haitian population. While many of the participants were born in The Bahamas, a large percentage may have been from Haitian parents, but the questionnaire did not ask about their parent’s place of birth. A study specifically targeting this population may be needed.
Conclusion
Based on the responses of the young men who participated, it is likely that many young men in The Bahamas would participate in a VMC program and this would be an important additional tool in “Getting to Zero” HIV infections in The Bahamas. Most of the young men in high school would consider circumcision as part of a strategy for reducing HIV incidence. It is clear that the provision of accurate information about health benefits of MC is key to the success of a MC program.
Introduction of circumcision promotion as a strategy for reduction of HIV infections needs to include both VMC, to target the currently sexually active men, but also infant circumcision for future prevention. It should be emphasized that MC is only one component of “getting to zero” new HIV infections. The program must include HIV testing and access to care with treatment to reduce viral load, pre-exposure prophylaxis and post exposure prophylaxis programs, as well as education about safer sex and condom use (Kurth, Celum, Baeten, Vermund, & Wasserheit, 2011).
Footnotes
Acknowledgements
The authors thank The Bahamas AIDS Foundation, Bahamas National AIDS Program, and students within the MBBS program at UWI School of Clinical Medicine and Research, Bahamas for supporting this study. This study has been presented in part as an oral presentation at the 2018 Caribbean Public Health Conference (CARPHA), St. Kitts, West Indies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Foundation for AIDS Research (CANFAR), Toronto, Ontario, Canada [grant number 4, cycle 24]; and a Canadian Institutes for Health Research New Investigator Award.