
Abstract
The experience of being bullied in childhood or adolescence affects health into adulthood and is a public health crisis. Particularly affected are sexual minority young adults who are at the greatest risk for severe and violent bullying, HIV seroconversion, and onset of a substance use disorder. Although the scholarly work in the area of bullying victimization has made great gains over the past few years via improved sampling and methodological rigor, most of the focus of health research in this area has been on prevention efforts. The purpose of the current study was to inform the development of a transdiagnostic integrated treatment platform that will focus on mental and physical health outcomes that include sexual risk taking and substance abuse. This study involved conducting four focus groups with HIV-uninfected gay and bisexual men, aged 18 to 26 years, in order to examine treatment needs and preferences and further develop an evidence-based intervention. Four themes emerged from the analysis of transcripts: (a) learning about bullying and psychopathology, (b) coping with bullying, (c) experiencing psychopathology as a consequence of bullying, and (d) tailoring psychosocial interventions to address health sequelae linked with bullying. These themes provided a solid foundation to develop and test an intervention to address key health risks among men who have sex with men (MSM) with a history of being bullied and recent sexual risk taking and substance abuse.
There is convincing evidence that the experience of being bullied as a child or adolescent has serious adjustment and public health consequences that entail great costs to society (Olweus, 2013). Bullying may be defined as the repeated use of a written, verbal, or physical act, gesture, or combination thereof, directed at another individual that causes physical or emotional harm, or damage to his or her property, places the victim in reasonable fear of harm or property damage, creates a hostile environment for the bullied individual, and includes cyberbullying (Olweus, 2013). The prevalence of bullying victimization is disproportionately higher among sexual minorities relative to other groups (Berlan, Corliss, Field, Goodman, & Austin, 2010; Katz-Wise & Hyde, 2012; Kosciw, Greytak, Palmer, & Boesen, 2014; Mustanski, Newcomb, & Garofalo, 2011; Schuster et al., 2015), with some reports as high as 90% within the past year (Berlan et al., 2010; Kosciw et al., 2014; Mustanski et al., 2011). Bullying victimization is most impactful among young sexual minority men (i.e., gay, bisexual, and other men who have sex with men [MSM]) and is more often physical and violent for MSM who have the highest level of bullying victimization relative to other gender and sexual orientation groups (Berlan et al., 2010; Katz-Wise & Hyde, 2012; Mustanski et al., 2011; Schuster et al., 2015). One binational study reported that being bullied was linked with health outcomes that are worse than other forms of child maltreatment (Lereya, Copeland, Costello, & Wolke, 2015). Bullying victimization among MSM is associated with higher rates of externalizing problems such as substance use and abuse (Huebner, Thoma, & Neilands, 2015; Sinclair, Bauman, Poteat, Koenig, & Russell, 2012), sexual risk behaviors (Bontempo & D’Augelli, 2002; D’Augelli, Grossman, & Starks, 2006; Schneider, O’Donnell, Stueve, & Coulter, 2012), and internalizing problems such as psychological distress, depression, anxiety, suicidality, and post-traumatic stress disorder (PTSD; Berlan et al., 2010; Katz-Wise & Hyde, 2012; Sinclair et al., 2012). Recent prospective longitudinal studies reported that negative physical health outcomes (e.g., increased stress hormone levels) are associated with past bullying and last into emerging adulthood (Copeland, Wolke, Angold, & Costello, 2013; Copeland et al., 2014; Wolke, Copeland, Angold, & Costello, 2013). Further, another recent multinational longitudinal study reported deviations in normal brain development among those with a chronic history of being bullied (Quinlan et al., 2018).
Emerging adult MSM compose the group most at risk for being bullied, most at risk for HIV (Centers for Disease Control and Prevention, 2012), and most at risk for the development of substance use problems (Flentje, Heck, & Sorensen, 2015; Green & Feinstein, 2012; Woodford, Krentzman, & Gattis, 2012). Despite this overwhelming health burden, to date no tailored intervention has been developed to address the confluence of these problems among this at-risk population. The majority of extant interventions to decrease substance abuse, sexual risk associated with HIV seroconversion, and distress among MSM have only had modest effects, attributed in great part to almost all models of intervention not fully addressing the impact of comorbid psychiatric disorders (Goldbach, Tanner-Smith, Bagwell, & Dunlap, 2014; Knight, Shoveller, Oliffe, Gilbert, & Goldenberg, 2013; Lyons, Bieschke, Dendy, Worthington, Georgemiller, 2010; Meltzer, Vostanis, Ford, Bebbington, & Dennis, 2011; Paul, Stall, & Davis, 1993). One strategy to increase the efficacy of these interventions is to address the complex needs of at-risk MSM by developing integrated treatment platforms with evidence-based transdiagnostic approaches to address the psychosocial problems and subsequent health risks that occur in the context of this syndemic (Boroughs, Ehlinger, Batchelder, Safren, & O’Cleirigh, 2018; Crepaz et al., 2006; Herbst et al., 2005, 2007; Johnson, Carey, Chaudoir, Reid, 2006; Lyles et al., 2007; Pachankis, 2015). The experience of being bullied, a chronic stressor, is related to a complex set of health outcomes in need of this type of intervention.
The current study set out to evaluate the needs and treatment preferences among a sample of men from this population and the aim of this study was to collect qualitative data, via focus groups, from a demographically diverse sample of HIV-uninfected emerging adult MSM to learn about the treatment needs of this population including the links between a history of being bullied and health risk behaviors. In addition, preexposure prophylaxis (PrEP) knowledge, interest, and readiness were a key emphasis of these focus groups conducted in order to develop a feasible and acceptable integrated treatment platform for HIV-uninfected emerging adult MSM with high-risk substance and sexual risk and a history of being bullied.
Method
Study Design
This study was the first phase of a two-phase funded study conducted to develop a tailored psychological intervention to address health problems among emerging adult MSM. From September 2015 to January 2016 purposive homogeneous sampling was used to recruit a sample of HIV-uninfected emerging adult MSM with a history of being bullied and current distress. Four focus groups were conducted to identify accessibility barriers and optimal treatment delivery for an MSM-affirming intervention for victims of past bullying. Focus groups were conducted within a community health-care center located in the Northeastern region of the United States. At each focus group, the facilitator read aloud to participants an approved statement that explained the study/focus group procedures, risks and benefits of participation, privacy and confidentiality, and compensation. Informed consent was obtained verbally at the beginning of each focus group in lieu of a signed consent form to maintain participant anonymity (see questioning route in Appendix A). At the conclusion of each focus group, a short quantitative assessment was given including demographic items (e.g., age, racial/ethnic identity, sexual identity), lifetime bullying history (e.g., verbal, violence), and substance use and sexual behavior in the previous 3 months (see Table 1). All focus groups were facilitated by the principal investigator and the study coordinator and all were audio recorded. Following a review of the data after the fourth focus group, data collection ended as saturation was attained (see Guest, Namey, & McKenna, 2017; Saunders et al., 2018). Participants were compensated $50. The study was approved by the Partners Human Research Committee (IRB00000858) and the Fenway Institutional Review Board (747385-2).
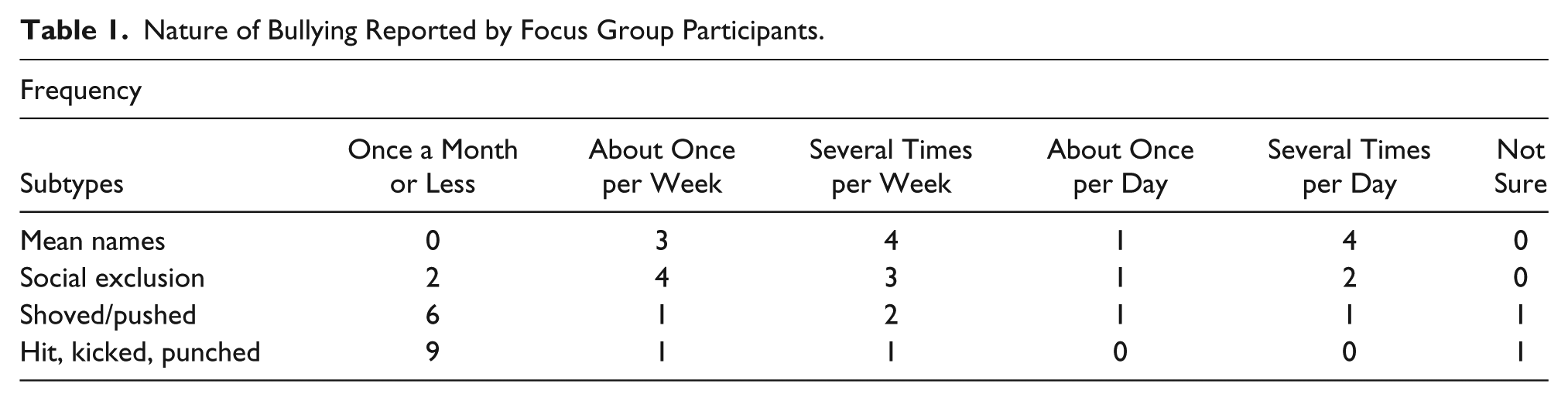
Nature of Bullying Reported by Focus Group Participants.
Recruitment and Screening
Traditional print recruitment methods were used together with social media approaches to recruit the sample. For example, flyers were placed throughout medical and mental health service waiting areas and in primary care and other treatment rooms of Fenway Health, a community health center that focuses on lesbian, gay, bisexual, and transgender (LGBT) health. Direct recruitment from LGBT groups at local colleges and universities complemented these efforts. Other recruitment efforts included community outreach to a variety of organizations, online postings, advertising through Craigslist and Facebook, and advertisements on mobile applications used primarily by gay and bisexual men (e.g., Grindr, Growlr).
Prospective participants were given a brief telephone screen to determine eligibility. Eligibility criteria included the following: (a) self-reported as an HIV-uninfected MSM (identified as mostly straight, gay/homosexual, bisexual, and/or reported having ever engaged in receptive or insertive anal intercourse or oral sex with a same-sex partner) and was born male aged 18 to 29 years; (b) had engaged in one or more acts of condomless anal (insertive or receptive) or vaginal intercourse in the past 3 months; (c) had engaged in problematic substance use defined as at least one self-reported episode of illicit substance use (inclusive of any Schedule I substance, regardless of state-issued prescription, or nonprescription use of any Schedule II–V drug), polysubstance use (use of one or more substances concurrently including alcohol), or one episode of risky alcohol use (defined as consuming three or more drinks within a 3-hr period) in the past 3 months; (d) a history of being bullied and associated distress; and (e) the ability to understand English and comprehend all study procedures.
Sixty-nine telephone screenings were conducted, of which 30 individuals were eligible. Reasons for exclusion included (participants may have multiple reasons) the following: does not identify as MSM (n = 3), self-reports as HIV positive (n = 4), outside of target age range (n = 18), no sexual risk (n = 15), no bullying history (n = 2), or did not meet problematic substance use criterion (n = 7).
Procedure
To assess the nature of bullying victimization, participants were asked how often they were bullied during the worst 2 months that occurred at any time between grades 1 and 12 using a modified Olweus Bully/Victim Questionnaire (BVQ; Solberg & Olweus, 2003). One participant said “a few times a month,” four said “several times a week,” six said “daily,” and one did not respond. Referring to this same 2-month period, participants were asked how often they were (a) called mean names, (b) excluded from peer social activities, (c) shoved or pushed, and (d) hit, kicked, or punched (see Table 1 for participant responses).
Development of focus group questioning route
Collaborative discussion between the principal investigator and behavioral research team members in addition to relevant literature related to bullying history, accessibility and acceptability of MSM-affirming evidence-based treatments, and qualitative principles led to the development of a semistructured interview (see Appendix A). The research team, in consultation with other experts, prepared five questions with multiple probes subsumed under each question to structure the focus groups. Supported by more specific prompts in each domain, the interview focused on (a) proximal impacts of bullying and teasing, (b) distal impacts of bullying and teasing, (c) feasibility and acceptability of prevention/intervention, and (d) communicating about sexual behavior and PrEP with medical providers.
Data Analysis
The first and third authors conducted each focus group, which were audio recorded and delivered securely to a professional transcription service. The data were transcribed verbatim with resulting transcripts that were reviewed by the principal investigator and the study coordinator to protect transcription fidelity. In order to code the data, an inductive thematic analysis was used where codes and themes identified were data driven with little or no predetermined theory, structure, or framework to analyze the data (Braun & Clarke, 2006).
The overarching research questions were the following: (a) How are young adult MSM affected by a history of being bullied? and (b) How might this population benefit from a tailored psychosocial intervention?
Using a qualitative data analysis software, Dedoose 7.5.9, an iterative approach was implemented to review and code transcripts from the focus groups. General research questions formed the foundation of the focus groups in order to help guide the coding. A six-phase approach was used for conducting a thematic analysis as outlined by Braun and Clarke (2006). In Phase 1 of the analysis, all transcribed data was read and reread, recording any initial ideas and first impressions of the data. During Phase 2, important features of the data were coded across the entire dataset that may have been relevant to the research questions. Codes that were redundant or overlapping with other codes were combined or merged together. In Phase 3, codes were examined, analyzed, and sorted to identify potential overarching themes that focused on broader patterns in the data. Each main (or candidate) theme represented a collection of subthemes and extracts of data that had been clustered together as codes. In the fourth phase of the analysis, main themes were reviewed and refined at two levels. At the first level, themes were checked to see if they matched the coded extracts. At the second level, themes were checked to see if they “worked” in relation to the entire dataset. Themes were reworked as necessary before generating a thematic “map” of the analysis. During Phase 5, the scope and focus of each theme was defined and refined to determine which aspects of the data were captured by each theme. In the last phase, the final themes were reported along with data extracts (or quotes) that reflected the breadth and depth of each theme in order to tell a compelling “story” about the data.
Results
Participant Characteristics
The participants were emerging adult MSM (N = 12) ranging from 18 to 26 years of age (Mage = 22.75 years, SD = 2.59). Passive assent was attained for each focus group participant; thus, the informed consent was read orally to participants and they gave verbal consent to participate. This allowed participants to remain anonymous in their responses given the sensitive nature of the questions and probes that were asked. Following each focus group, participants completed a demographics form. Therefore, no demographic information was linked with participant responses.
Across all focus groups, three participants identified as African American, one as Asian American, six as Euro American, and four as Latino (two Latino White and two Latino without any racial category identified). One participant had a high school or general education diploma, five were currently matriculated in college or university, four had a baccalaureate degree, and two were post-baccalaureate graduate students.
Health risks were assessed anonymously. Participants reported binge drinking alcohol once a month or less in the past 3 months (n = 3), binge drinking one time per week in the past 3 months (n = 5), binge drinking several times per week in the past 3 months (n = 2), and no alcohol use in the past 3 months (n = 2). Participants reported marijuana use daily (n = 2), once a month or less (n = 2), several times per week (n =1), several times per day (n = 1), or no marijuana use in the past 3 months (n = 6). Two participants reported use of hallucinogens and two participants reported cocaine use one time per month (or less) in the past 3 months.
In using Braun and Clarke’s (2006) approach, narratives were analyzed and four themes were identified that related to MSM’s bullying experiences and subsequent psychopathology and the treatment needs of this population in order to guide the development of a psychosocial intervention. Themes identified included (a) learning about bullying and psychopathology, (b) coping with bullying, (c) experiencing psychopathology as a consequence of bullying, and (d) tailoring psychosocial interventions.
Narrative Themes
Learning about bullying and psychopathology
This first theme described where and/or how participants learned about the adverse mental health outcomes and health risk behaviors associated with a history of being bullied (see Figure 1). Some participants described learning about the impacts of being bullied vicariously through their peers who were involved in bullying and then experienced emotional and/or psychological problems. For example, one participant who witnessed a friend experiencing negative health outcomes as a result of being bullied described: “I had friends who’ve had eating disorders, who’ve had various psychological, emotional, mental health problems because they were bullied so badly throughout adolescence and childhood and even then on.” Here, the participant specifically identified an eating disorder as a mental health problem that was perceived to be a result of his peer being bullied at a younger age. Similarly, other participants attributed a variety of their peers’ specific mental health problems (e.g., anxiety, depression) to being bullied.

Thematic map of the first theme.
Participants identified school (e.g., course work) as a vehicle for learning about the connection between bullying and mental health outcomes. Through their course work, participants were able to receive reliable and valid information regarding how individuals are negatively affected by bullying. For instance, one participant recalled learning about bullying while at university: “A lot of it I learned during my undergraduate studies. I was a psych major. Took a lot of courses on social problems, social inequality, abnormal psych, you know, just things about psychiatric disorders and problems.” Further, another participant explained: “For me it’s a mixture of health—of self-experience as well as my psych and personality class.” These quotes indicated that information regarding the proximal and distal influence of childhood bullying may be disseminated through behavioral health or social science courses.
Some participants also identified the Internet and other media sources as
powerful and pervasive sources of information regarding the effects of
bullying. One participant recalled a news story about a teenager who had
committed suicide as a result of being bullied:
“and then also a lot of media exposure. And so, to kind of
give context behind that, I came out as a freshman in high
school, and three days later, Tyler Clementi committed suicide
and that started the LGBT—really it started the LGBT suicide
epidemic, which was covered by the media from October 2010
throughout about March 2011.”
The participant remembered increased media coverage of a trend in suicides among members of the LGBT community who were bullied. As well, some participants discussed learning about the link between bullying and psychopathology through access to Internet websites (e.g., youtube.com, gayguys.com). For example, one participant stated: “I’ve seen many videos and like ‘It gets better’ and all of those kinds of YouTube videos too, and news stories of kids killing themselves with suicide or something like that.” Here, the participant identified that YouTube could be used as a source of learning, with suicide again being a possible consequence of bullying.
Coping with bullying
The second theme that emerged involved efforts to cope with a history of
being bullied that characterized participants’ engagement in coping
behaviors to deal with the psychological distress of being bullied (see
Figure 2). Two
different methods of coping emerged from the narratives. The first method
was adaptive coping strategies, which involved participants seeking social
support from peers and parents to help them deal with being bullied. One
participant discussed the importance of having supportive parents to help
him cope with experiences of bullying:
“My parents were always very intuitive, as far as, you know,
if something was affecting me and my sister negatively right
there, so. And they were, you know, very supportive in that
instance and I think the biggest burden I beared, before really
telling them what was going on, was just, I’d been kind of
popular in elementary school, and it was a pretty big
transition, when middle school happened, and, you know, the
whole social order shook up, and, you know, I think there was a
bit of shame that I carried, by that happening at first; I
didn’t really want to disclose, but honestly if I hadn’t had
supportive parents, I mean that could have been a nightmare,
could have lasted much longer.”
Another participant recalled receiving social support from not only his
mother but also his friends:
“And it kind of took me—my mom, like, kind of sitting me
down, like, “What’s wrong,” and me just like blurting it all
out. That made me realize that she was kind of there to be
supportive. And then like, as years go by, like the friends that
I got during the years, I would feel comfortable with telling
them.”

Thematic map of the second theme.
Taken together, these stories indicated that when young adult MSM have the ability to elicit support from their parents and/or peers to cope with bullying, the negative impact of bullying may be mitigated in both valence and duration.
Conversely, a second method identified through the analysis of the narratives
was maladaptive coping strategies, which involved engaging in health risk
behaviors such as substance use, sexual risk taking, and self-harm. Although
adaptive coping represents a healthy strategy for those who have been
bullied, some participants turned to maladaptive coping, which may have
served a similar function in managing distress from the previous experiences
of being bullied. For example, one participant shared an instance of
maladaptive coping by avoidance:
“I’m probably the youngest one here; I’m only 18. So I’ve
only been out for a couple of years now, and a lot of the
bullying happened before I was out so a lot of the coping
mechanisms that I took were sort of trying to just deny it, deny
myself, pretend that that wasn’t who I was, and try to act like
the other guys and try to be not what they said I was and I
guess that was just how I coped was just trying to tell myself
that I wasn’t what they were telling me I was.”
Another participant discussed maladaptive coping such as engaging in
self-harm and self-medication:
“Well, I guess I’ll preface this with a trigger warning for
self-harm. In the past, there—I did have a lot of self-harm
issues, a lot of self-medication issues and that was a coping
mechanism in late adolescence. . . . And at this point, I guess
I use sort of, like, marijuana as a coping mechanism, at this
point, as well.”
There were also some coping behaviors discussed among participants that may
be considered both adaptive and maladaptive. That is, the strategy may help
reduce emotional and/or psychological problems in the short term (adaptive)
but do not reduce bullying in the long term (maladaptive). For example, some
participants described engaging in various forms of distraction (e.g.,
listening to music, exercising, working) in order to keep their mind
preoccupied to avoid thinking about being bullied, as well as avoiding
physical spaces where bullying was likely to occur (e.g., school hallways,
locker rooms) and avoiding other people in general to reduce the threat of
being bullied. One participant discussed distracting himself through
electronic devices:
“I think—because when I think of bullying, I think of being
bullied, I think of being annoyed. So, to translate that into,
like, now, if I’m ever feeling annoyed, I think, I kind of just
kind—I don’t want to say, shut off from the world, but I just
kind of, I go on Netflix, watch TV, or play some video games, or
do something to just, kind of not have to think about it fully
at the moment.”
Moreover, another participant recalled rerouting his usual trip home in order
to avoid being bullied:
“Yeah. I, I remember this one time, I actually had to
readjust my route to go home, to the point where, like, I was
spending an extra 10 minutes walking home, just to avoid a
certain area. . . I had to like, adjust my route, to where I was
like, cutting through, like, the back area of this like strip
mall, to like, where like, the trucks gathered and whatnot,
so—which was dangerous, because, you know, homeless people went
back there. But it was like, I’d rather deal with them than
like, deal with like, the pressure of—of dealing with that
again, you know, so.”
Overall, these narratives suggest that individuals may be using adaptive and maladaptive coping strategies to reduce some of the emotional and psychological distress from being bullied. This is consistent with previous literature suggesting that individuals who are targets of bullying may engage in a range of coping behaviors (Newman, Holden, & Delville, 2011). Participants did not mention a psychosocial (or related) intervention as a method for dealing with the psychopathology linked with a history of being bullying. Although seeking social support from parents and/or peers may be an adaptive coping strategy for reducing symptoms associated with being bullied, support alone may do little to address the underlying psychopathology. This may create a need within the MSM community for the development of an intervention that not only addresses the psychosocial problems but also simultaneously reduces the likelihood that these individuals will seek out harmful, maladaptive coping behaviors.
Experiencing psychopathology as a consequence of bullying
The third theme that emerged from the data was “experiencing psychopathology
as a consequence of bullying.” This included various adverse mental health
outcomes and health risk behaviors that individuals may experience as a
result of being bullied (see Figure 3). This was the most robust
theme explored within the focus groups. Participants were especially attuned
to the impact of bullying on internalizing problems, which are negative
emotional problems that are focused inward (e.g., depression, anxiety, PTSD,
social withdrawal, low self-esteem), and behavioral problems that are health
risks (e.g., self-harm). For example, one participant recounted:
“I was very withdrawn, didn’t have that many friends. I had a
few, but I just kept everybody at arm’s length at most and never
really volunteered information if possible. Just didn’t speak
much. Very—not even just introverted, but very withdrawn. Just
did not speak to anybody, didn’t engage with anybody, never
made—like, initiated contact or conversation with anybody
because I was afraid of people, especially the other people
around my age.”
Participants’ narratives also identified externalizing problems, which
include negative behaviors focused outside of oneself such as substance use
(e.g., alcohol, marijuana) and sexual risk taking. One participant recalled:
“Well like I just mentioned how I drink too much. I mean
like, it’s hard to maintain a 3.5 to stay in your graduate
degree when you’re black out drunk Monday, Tuesday, and
Wednesday because you only have class on Thursdays and Fridays.
And it’s doubly as hard to go to work in the morning when you’re
hung over and sneaking out to the bathroom to drink, so there’s
that.”
Some participants identified the connection between some of the problems they
were experiencing and their history of bullying. One participant stated:
“I have anxiety, I think we’ve all touched on that, we all
have some sort of anxiety, depression, bipolar disorder. And
those three, are kind of like, they always, you know, interloop
with one another, and those can all be led back to like being
bullied as a child, or being bullied as, you know, young
teens.”

Thematic map of the third theme.
Taken together, these stories are consistent with the vast (and mostly quantitative) literature on psychological maladjustment that is linked with victimization (e.g., Arseneault, Bowes, & Shakoor, 2010; Copeland et al., 2013; Kelly et al., 2015). Although some participants appeared to be aware of the fact that being bullied is linked to psychological distress, most of them were not able to establish (or were unsure of) the link between their current reported symptomatology and the experience of being bullied in the past. Ideographic approaches, which assist those in treatment to understand their current health problems, may be a crucial element in the development of a psychosocial intervention for this particular population. Furthermore, the type of psychopathology participants experience currently (e.g., internalizing versus externalizing disorders) may also be an important treatment consideration. For example, an intervention for anxiety may require a different approach than an intervention for self-harm. Therefore, transdiagnostic interventions are particularly appealing for this population.
Tailoring psychosocial interventions
Finally, the theme “tailoring psychosocial interventions” characterized
aspects of treatment that participants may seek out and would prefer in
order to accommodate or address their mental health needs (see Figure 4).
Participants’ narratives identified a number of different treatment needs
that revolved around receiving psychotherapy. Participants felt that the
mental health concerns linked with their past history of being bullied
should be approached individually. That is, individuals should seek specific
treatment that includes a match between therapist and client on
characteristics such as ethnicity and sexual orientation and that treatment
should be organized around the type of disorder the individual is currently
experiencing. For example, one participant stated:
“Just seeing someone who’s like me, so as a black gay man, I
would love to, I would love to talk to someone who was black and
gay, because they—it’s something to connect with, and my
experience as a black gay man is completely different than
someone else’s experience as a white gay man, or Latino gay man,
or Asian gay man. . . . If I’m trying to be at ease, or it’s
like, to be counseled, or, like, to feel comfortable with
someone, I would rather start with someone who has the same
similarities as me.”

Thematic map of the fourth theme.
The explicit preference for client–therapist match appears to be an important aspect of therapy for this participant. In particular, feeling comfortable with the therapist because they belong to a similar demographic background may be key a treatment need for some MSM.
In addition to a preference for individual therapy, participants also
discussed the idea of group therapy that would involve a group of people of
different ethnicities and sexual orientations coming together to share their
experiences. Some participants felt unsure about taking part in group
therapy. One participant discussed a reluctance to share sensitive
information in front of others:
“I think it’s—it will be easier for somebody to talk and
whatnot, one-on-one type of thing, because they’ll feel like
they can express themselves more than kind of being ashamed of
what they did or what they haven’t done with other men or
whatnot.”
Conversely, other participants felt positively about group therapy as it
could contain a mix of men and women of various ethnicities and sexual
orientations whom one could seek out for social support. One participant remarked:
“I feel like it would be a lot better because you would feel
support from multiple people who are not in the same background
as you. It would feel good, I guess, to have support from people
who are straight, or girls, and just things like
that.”
Although some participants liked the idea of group therapy, they preferred
the groups to be sorted by gender and sexual orientation. As one participant described:
“I think the more you contextualize it though, if you have
like gender-specific groups or age-specific groups, it’s more
validating. Like right now we’re all, I’m assuming, you know,
gay men and that part—that’s made it even more validating, but I
think mixing genders and sexual orientations might take away
from it a little bit.”
Furthermore, regardless of the composition of the groups, some participants
appeared to emphasize shared experiences and how it may be beneficial to
talk and listen to others with similar life circumstances. One participant explained:
“It helps. Like it’s a group setting but it definitely helps
you feel more secure in yourself, you know, because you listen
to everybody else talk about deep things and it’s like, damn,
everybody went through kind of similar things to me, I mean, I’m
not the only person who’s f***** over.”
Taken together, these stories suggest that a psychosocial intervention may involve individual or group therapy depending on the treatment preferences of those seeking clinical services.
In addition to participants identifying that they wanted an individual or
group therapy format, they also felt that beyond an individual or group
approach, treatment should be consistent. That is, although participants
were not in agreement about the frequency of therapy, there appeared to be a
common understanding that therapy should be scheduled and part of a routine
that occurred at least once a month. For example, one participant revealed:
“I mean, I’d say [treatment should be] at least a minimum of
once a month. Like if you’re going to do it, you’ve got to
dedicate yourself to it, so don’t just do it right now because
you’re stressed out because that’s treating an effect and not
the underlying cause, so it’s important that you stick to some
type of routine otherwise you’re just like wasting your time and
your therapist’s time.”
This participant emphasized the role of the client in the therapeutic process by placing responsibility on the client to be committed to therapy in order to realize treatment gains.
Although the development of an intervention to address problems stemming from
bullying appeared to be a significant treatment need discussed in the focus
groups, some participants felt that the benefits of therapy needed to be
communicated to the public so that people are likely to seek out treatment
if necessary. For instance, one participant described:
“It’s just a matter of explaining what benefits it has. Like,
just making the benefits known . . . going to counseling just
doesn’t have a good rap. You know, like, people are like, “Oh,
you’re going to counseling, you must have some serious
problems.” You know, it’s a terrible stereotype. So, if we could
just, you know, show the benefits, like, just make the benefits
and awareness of, like, the good things that counseling can do
for people more known . . . if you’ve been through this [being
bullied] if you go to counseling, this is what you can get out
of it, and it could really benefit your life. It could, you
know, turn things around for you.”
Disseminating the effectiveness and benefits of therapy may be a crucial treatment need for individuals with a history of being bullied to increase the likelihood that they will seek out an evidence-based treatment.
Finally, a mobile application that can be downloaded to smart phones was also
identified as a potential component of a psychosocial intervention.
Specifically, daily self-monitoring to capture distress and health risk
behaviors in real time was appealing to this sample of young adult MSM. In
one example, a participant reasoned that while having a mobile app may be a
good idea to incorporate into an intervention, he expressed a concern about privacy:
“While I like the convenience of being able to do it on a
phone, I think that could be appealing for a lot of, of MSM,
potentially, I think that, you know, there’s also a certain
vulnerability. I mean, if this [cognitive behavioral therapy]
homework involves disclosing, or writing down, anything that’s
very personal or sensitive to you, I’d be very reticent to do
that on my phone right there, given that, you know, people get
hacked all the time. . . . I think that, you know, with some
discretion, it’s a good idea, for sure.”
For MSM with a history of being bullied, particularly those in the emerging adult age cohort, integrating a mobile application into an intervention may be a treatment need that may help with treatment access, implementation, and adherence.
Discussion
The current study examined how a diverse sample of HIV-uninfected young adult MSM were affected by a history of bullying victimization and how this population may benefit from the development of a feasible and acceptable psychosocial intervention to address the negative mental health outcomes and health risk behaviors associated with a history of being bullied. Four themes were identified from the discussions with MSM: (a) learning about bullying and psychopathology, (b) coping with bullying, (c) experiencing psychopathology as a consequence of bullying, and (d) tailoring psychosocial interventions. Narratives shared across the four focus groups suggested that these young adults with a history of bullying victimization may have experienced adverse mental health outcomes and engaged in health risk behaviors; however, causal links cannot be inferred. Furthermore, the results also highlight the long-term outcomes from a history of being bullied to the extent that some of these men were experiencing symptoms that may have persisted long after they were bullied. Both of these findings are consistent with previous research that has examined bullying as a potential precursor to a wide range of short-term and long-term psychosocial problems (Arseneault et al., 2010; Kelly et al., 2015).
Another shared theme across focus groups was that participants were unaware of the links, documented in the scholarly literature, found between a history of being bullied and health problems. Compared with other developmental traumas (e.g., childhood sexual abuse or physical abuse), this is perhaps an important unrealized treatment need (i.e., psychoeducation at the individual prevention and intervention levels and public service information) to increase awareness about these links so that clinicians are able to address a history of being bullied as a potential predictor of presenting psychopathology or other health problems.
Some participants spoke about concerns related to therapist match and the idea that they may benefit from a treatment provider who shares characteristics with the patient. This may be an idiosyncratic preference, or it may have some link with treatment adherence and outcome. Some research suggests that specialized cultural competence training to work with MSM, and other sexual and gender identity minority populations, is important for reaching these underserved groups (Boroughs, Bedoya, Safren, & O’Cleirigh, 2015).
Discussion from the focus groups also provided feedback about treatment preferences of these young adult MSM and ways to improve the implementation and quality of the integrated treatment platform that is currently under further development. For instance, it was clear that participants wanted the treatment to be tailored to meet their individual needs (e.g., client–therapist match on ethnicity and/or sexual orientation, individual versus group therapy) in order to address specific mental health problems. Furthermore, once an intervention is developed and tested, disseminating the availability and benefits of the tailored intervention for adult MSM with a history of being bullied may be crucial to helping this population with some of their current symptomatology associated with past bullying victimization. Although much of the public focus is on prevention, which may help to reduce exposure to this significant trauma and its associated health sequelae, less attention has been focused on the development of interventions in general and tailored interventions more specifically. The authors hope this work will stimulate interest among clinical health researchers and mental health professionals to work toward an evidence-based approach to address the health problems linked with bullying victimization.
Limitations and Future Directions
Despite the findings, there are limitations to this study. The sample comprised a specific subset of the population: young adult MSM between the ages of 18 and 26 years. Therefore, results may have limited generalizability to the broader community, but also to how these findings influence the development of the related psychosocial intervention. That is, the intervention developed from this research may only be effective at targeting the psychosocial problems of young adult MSM with a history of being bullied and it is not clear if such an intervention would need further modification to work among adolescents or older adults. Another limitation involves the sample size and sample composition. The sample composition reflects the study inclusion/exclusion criteria, which limited the results to those with a history of being bullied and problems with both substance use and sexual risk taking. Thus, the voices of those with a history of being bullied without those health concerns were excluded from these data. The smaller sample size, even for focus groups, reflects both saturation after the fourth focus group and a difficult-to-engage population.
Another limitation may be that some, or all, participants may have experienced other developmental traumas (e.g., child physical and sexual abuse) along with a history of being bullied that in some way contributed to their mental health and well-being. Evaluation of these other types of trauma were not included in the screening process or raised as a point of discussion in the focus groups. However, those other types of trauma are associated with similar internalizing and externalizing problems as those linked with bullying victimization (e.g., Boroughs, Valentine et al., 2015; Lereya et al., 2015). Therefore, future psychosocial intervention development may benefit from a broader exploration of other developmental traumas and how they may predispose some individuals to psychopathology and other health problems. This will improve such interventions by facilitating a flexibility to address multiple common traumas in childhood and adolescence.
One important limitation that may be further explored in future investigations is the role of PrEP and how it may be integrated into interventions for MSM who are at risk for HIV, given issues such as referral, cost, and adherence. The FDA approved Truvada as PrEP in 2012 for adults age 18 years and above, while approving its use among older adolescents, ages 15 to 17 years in 2018 (Holmes, 2012; U.S. National Institutes of Health, 2018). Given some literature on issues of stigma and shame associated with the use of PrEP by MSM (see Dubov, Galbo, Altice, & Fraenkel, 2018), the question of how to integrate PrEP education and support around these issues of shame remains.
Future research will involve studying the efficaciousness of the integrated treatment platform that is under development and developing an intervention that expands upon the current population to also include the needs of women and younger individuals with a history of being bullied and who may be experiencing psychosocial maladjustment and health risk behaviors. In addition, this work may provide a foundation for instrument development to quantify relationships among key variables.
Supplemental Material
Appendix_A._Project_RISE_Qualitative_Interview_Guide – Supplemental material for Developing HIV Prevention Interventions for Emerging Adult MSM With a History of Being Bullied: A Qualitative Study
Supplemental material, Appendix_A._Project_RISE_Qualitative_Interview_Guide for Developing HIV Prevention Interventions for Emerging Adult MSM With a History of Being Bullied: A Qualitative Study by Michael S. Boroughs, Daniel A. Provenzano, Avery D. Mitchell and Conall O’Cleirigh in American Journal of Men’s Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Harvard University Center for AIDS Research funded by the National Institute of Allergy and Infectious Diseases (P30 AI060354) to Dr. Boroughs. Some of Dr. O’Cleirigh’s time was supported by the National Institute of Mental Health (R01 MH095624). The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard University or the National Institutes of Health.
The authors dedicate this article to the memory of Avery DeVell Mitchell.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.