
Abstract
This study aims to evaluate follow-up activities completed by participants attending community prostate cancer (PCa) screening events. On-site surveys were collected from participants of 17 free PCa screening events from 2007 to 2011 in the St. Louis, MO metropolitan area. Follow-up action surveys were mailed to all on-site participants to assess medical (i.e., made an appointment with a doctor, got additional testing for PCa, made an appointment to be screened) and nonmedical activities (i.e., sought social support, health information-seeking, health behavior modifications) completed after the PCa screening event. Further, t tests and chi-square tests characterized participant information from the on-site survey and within each follow-up activity category for the mailed surveys. Among 1,088 on-site community PCa screening participants, the mean age was 50 years old, 94% were Black, and 30% responded to the mailed follow-up action survey. For the recorded follow-up activities, 65% of participants reported medically reported activities, of which “made an appointment to get a yearly physical” was the most common action (29%). Health behavior modifications were the most common nonmedically related activities (44%). Health information-seeking behaviors were the least reported follow-up action (22%). Men with higher incomes, married, with health insurance, and a primary care physician, most often participated in post-PSA screening activities, namely medically-related and social support activities. Understanding the most common activities completed by participants of a community PCa screening suggests the effectiveness of community events to re-engage underserved populations in the health-care system and provides insight on acceptable health promotion opportunities.
Prostate cancer (PCa) is the most frequently diagnosed cancer and the second leading cause of cancer mortality among men in the United States (DeSantis et al., 2016; National Cancer Institute; Siegel, Miller, & Jemal, 2017). Black men have the highest incidence and mortality rate of any racial or ethnic group in the United States from this disease (American Cancer Society, 2011). As advanced age is a risk factor for PCa, the U.S. Preventive Services Task Force recently recommended that health-care providers counsel and facilitate shared decision making with men between the ages of 55 and 69 years old about PCa screening and treatment options (U.S. Preventive Services Task Force, Grossman, et al., 2018). Although this recommendation does not offer specific recommendations for high-risk populations such as Black men, it does acknowledge that screening may have the potential to offer greater benefits for Black men (U.S. Preventive Services Task Force, 2018). There is growing interest to target men at high risk for PCa to promote screening and provide education to this population.
Previous studies report the effectiveness for community cancer screening programs as a mechanism to increase positive cancer screening behaviors, deliver targeted health education, and explain appropriate follow-up options for medically underserved and high-risk populations (Honeycutt et al., 2013; Horne et al., 2015; Torres, Richman, Schreier, Vohra, & Verbanac, 2017). In one community cancer screening program, 40% of men who received a prostate-specific antigen (PSA) screening test had a prompt follow-up with the local physician (Ashorobi et al., 2015). Community cancer screenings have been successful at reaching high-risk populations; however, little is known about the nonmedically related health promotion and health education activities completed by participants following a community cancer screening event.
An understanding of medical and nonmedical community cancer screening follow-up activities can inform researchers and health-care providers about health education and promotion activities that may be effective options for outreach interventions. Using data from PSA screenings coordinated by an academic-community cancer-specific partnership, the objective of this study is to assess follow-up activities completed by the participants, and examine predictors of medical and nonmedical activities taken after community PCa screening events.
Methods
Study Sample and Design
The Program for the Elimination of Cancer Disparities (PECaD) is an academic–community partnership comprised of researchers and physicians from Washington University School of Medicine in St. Louis, Barnes Jewish Hospital, and community stakeholders from the St. Louis metropolitan area (Thompson et al., 2015). PECaD programs facilitate and promote community-based participatory research and outreach through cancer-specific community partnerships. The Prostate Cancer Community Partnership provides free PCa screening events in partnership with community organizations at various community events throughout this region. The free PCa screening event targets men at high risk of PCa (i.e., has a family history of PCa, African American race, older age; American Cancer Society, 2018), and provides PCa education and health promotion materials from the National Cancer Institute and the American Cancer Society tailored for this population.
Data were collected from on-site participant surveys of men participating in 17 on-site community PCa screening events from 2007 to 2011. On-site participants provided written informed consent for follow-up contact information. After each screening event, participants with PSA levels <2.5 ng/ml received a postcard with their results. Based on the study oncologist’s recommendations, participants with PSA levels ≥2.5 ng/ml received a call or letter from a study oncologist regarding further action based on the participant’s screening and medical history. In 2011, all on-site participants received a mailed survey to assess medical and nonmedical follow-up activities completed after the PCa screening event. A self-addressed stamped envelope was included for participants to return the survey. Participants also had the option to complete the survey by telephone with a study staff member. Three weeks after survey mailings, study staff made three attempts at different times of the day to contact participants with incomplete or missing surveys. The study received approval by the Washington University Institutional Review Board (approval number: 201105114).
Measures
Sociodemographic, health care utilization, family history, PCa perception, and screening history data were collected on in-person surveys. Sociodemographic variables included: date of birth, race, age at last screening event, education, income, type of insurance, and marital status. Additional variables included: primary care doctor status (Do you have a primary care doctor?), family history of PCa (Do you have a first-degree relative with a diagnosis of prostate?), perception of having PCa (How likely do you feel that you will develop prostate cancer in the future?), time since your most recent PSA (When was your last PSA test at community event or physician’s office?), first year receiving a PCa screening at a PECaD community screening event, and total number of PECaD community screening events attended to date.
Post-PCa screening activities were measured in terms of medical and nonmedical activities. Medical activities included: made an appointment with a doctor; got additional testing for prostate cancer; made an appointment to be screened for another cancer; made an appointment for yearly physical. Nonmedical follow-up activity items included: social support (talked to spouse/partner about PSA results, sought guidance from a spiritual leader, joined a health-related support group); health information-seeking (visited a library for information, looked online for information about prostate cancer); and health behavior modifications (changed physical activity or diet). Data were also gathered from men reporting no participation in the recorded medical and nonmedical activities.
Data Analysis
Survey data were entered into the Research Electronic Data Capture (REDCap) version 7 database. Descriptive statistics were conducted to compare responders versus nonresponders to the mail-in survey. Participation in each category of follow-up action was assessed. Further, t tests were used to compare continuous variables and chi-square tests were used to compare categorical demographic variables within each follow-up action category. Data were analyzed using SAS 9.3.
Results
Table 1 presents the study population characteristics. Among the 1,088 men participating in the on-site PSA screenings, the mean age was 50 years old. The majority of these men were Black (94.1%, n = 732), and attended the community screening in either 2007 or 2008 (57.4%, n = 622). Half of the participants resided either in the St. Louis County or St. Louis City area (50.7%, n = 622). Of the on-site participants who responded to the mail-in survey (30.2%, n = 329), the mean age for respondents was 52 years old. There were no significant differences between respondents and non-respondents in race, most recent PSA, or area of residence.
Characteristics of Men Attending a PCa Screening Event in St. Louis, Missouri Metropolitan Area From 2007 to 2011.

Note. PSA = prostate-specific antigen; PCa = prostate cancer; SD = standard deviation. aNumbers may not sum to column total because of missing data. ^Fisher’s exact test used for analyses with low cell counts. *One person completed survey but did not participate in the PECaD event. **Two participants attended events but did not have labs.
Table 2 reports medical and nonmedical follow-up activities completed by participants after a community PSA screening event. Medically related follow-up activities were the most reported PSA screening follow-up action, with 64.7% (n = 213) of the mail-in respondents seeking additional medical services. The most frequent medically related activity was making an appointment to get a yearly physical, about 30% of the total population of mail-in respondents (n = 96). Among nonmedical activities, health behavior modifications were the most common (43.5%, n = 143), with 85 (25.8%) of the total mail-in respondent population modifying their diet. Talking to a spouse or partner about your test results was the most reported social support follow-up action (30.7%, n = 101). Approximately 20% (n = 62) of the follow-up survey respondents used on-line resources to seek health information about PCa. Collectively, using online and library resources health information-seeking actions online and the library were the least reported PSA follow-up action (22.2%, n = 73). About 25% (n = 79) of the survey respondents reported either not participating in any of the listed actions after their PSA screening or participating in activities other than those listed.
Medical and Nonmedical Follow-Up Activities of Participants After Attending a PCa Screening Event in St. Louis, Missouri Metropolitan Area From 2007 to 2011 (N = 329).
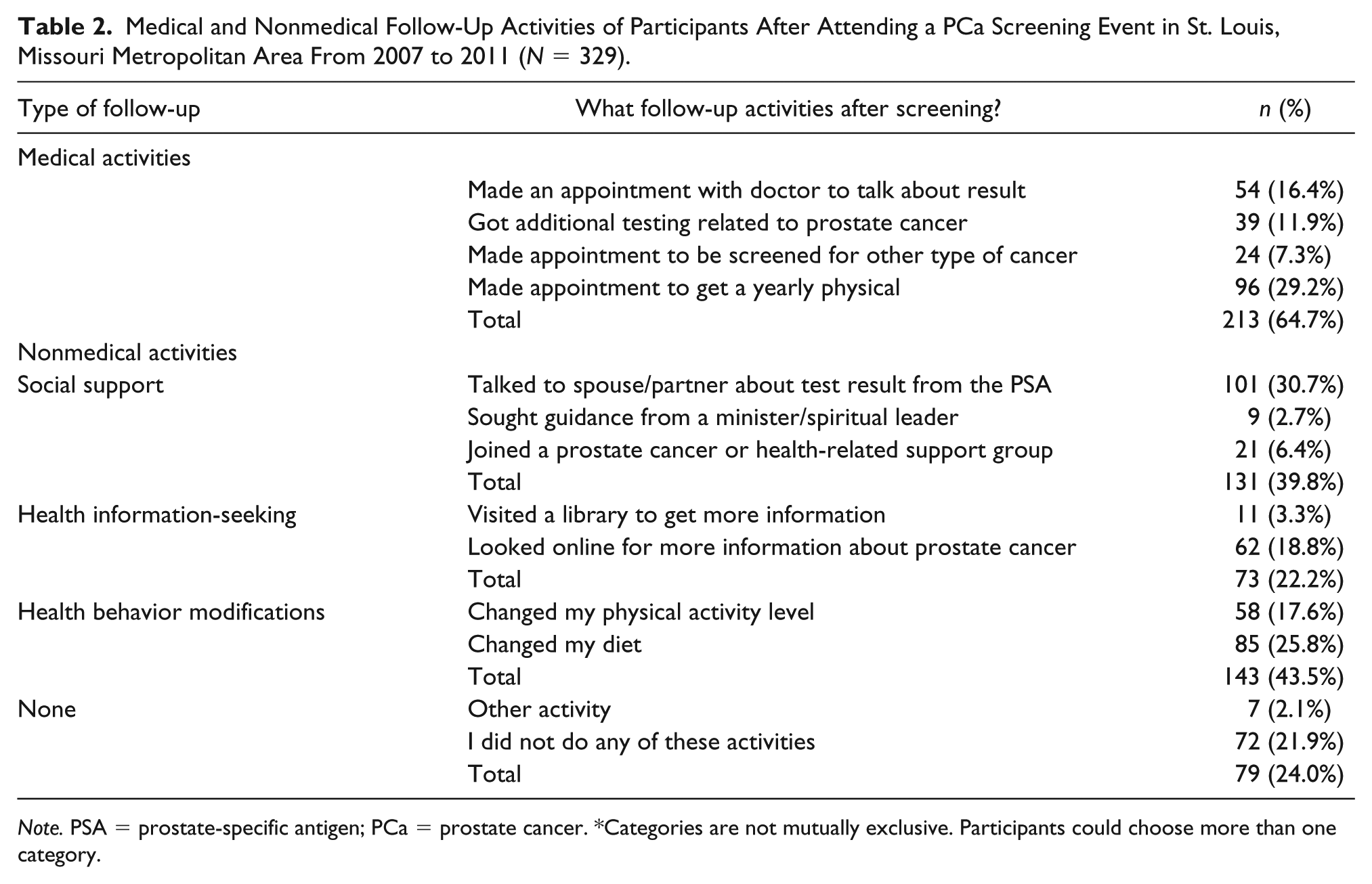
Note. PSA = prostate-specific antigen; PCa = prostate cancer. *Categories are not mutually exclusive. Participants could choose more than one category.
Descriptive characteristics of participants from each of the post-PSA screening activity categories are presented in Tables 3 and 4. Men completing a medically-related activity after the community-based screening compared to those who did not complete a medically-related activity were more likely to have higher incomes, be married, have health insurance, and have a primary care doctor (Table 3). Table 4 reports characteristics of men engaging in nonmedically related events following the PSA screening. Compared to participants that did not complete social support activities, those reporting social support activities were significantly more likely to have a higher income, be married, have health insurance, have a primary health-care provider, and more likely to perceive a risk of having prostate cancer. Men seeking health information following a PSA screening were more likely have a primary care doctor than those who did not report seeking health information after the screening event. Men participating in health behavior activities were significantly younger than men that did not (50 and 53 years old, respectively).
Descriptive Characteristics of Participants That Reported Medically-Related Activities After Attending a PCa Screening Event From 2007 to 2011 (N = 329).

Note. PCa = prostate cancer; SD = standard deviation. ^Fisher’s exact test used for analyses with low cell count.
Descriptive Characteristics of Participants That Reported Nonmedically-Related Activities After Attending a PCa Screening Event From 2007 to 2011 (N = 329).
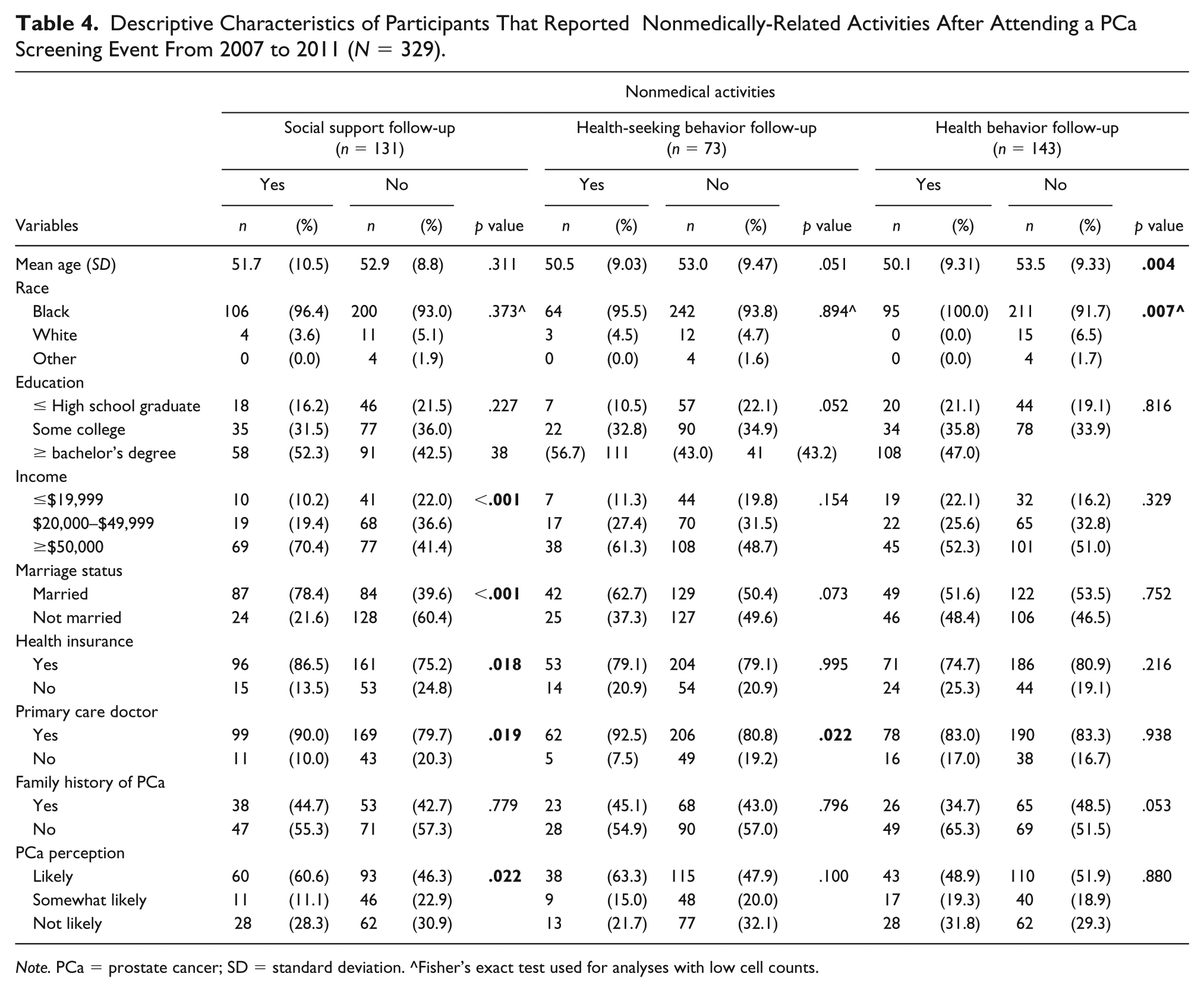
Note. PCa = prostate cancer; SD = standard deviation. ^Fisher’s exact test used for analyses with low cell counts.
Discussion
This study examined medically and nonmedically related activities completed by men after participating in a community-based PCa screening event. Medically related follow-up activities were the most common activity of men following the PSA community screening. These findings show that a community-based PSA screening event is a successful method of engaging high-risk populations in health care. Among nonmedically related activities, men most often modified their health behaviors, specifically they changed their diet. Almost one-third of the participants talked to their spouse or partner about their results. Men with higher incomes, married, health insurance, and a primary care physician, most often participated in post-PSA screening activities.
Other studies have observed that medically-related behaviors most often precede a screening or health fair (Lucky, Turner, Hall, Lefaver, & de Werk, 2011; Ormsby et al., 2017; Warnakulasuriya & Johnson, 1999). In an investigation of follow-up actions completed by participants of community-based healthy eye screenings, 69% of the participants with detected eye problems reported seeking medical treatment following the screening event (Ormsby et al., 2017). In another study, den Engelsen, Gorter, Salome, and Rutten (2013) investigated follow-up screening behaviors of participants tested for metabolic syndrome and reported 72% of the participants contacted their general physician. In both of these studies, participants were prompted during the screening to seek medical attention in the event of a positive result. Similarly, men participating in the PECaD community screenings were also prompted to seek medical advice in the event of a positive result. These findings support previous research that community health events may promote utilization of health-care services.
A smaller proportion of men sought PCa information from the internet or the library after attending the community PSA screening. Previous studies have reported high levels of medical mistrust for Black men (Hammond, Matthews, Mohottige, Agyemang, & Corbie-Smith, 2010; LaVeist, Nickerson, & Bowie, 2000). High levels of medical mistrust predict satisfaction in care and ultimately influence health-care utilization (LaVeist et al., 2000). The expectation based on these earlier findings is that a significant proportion of participants seek health information from alternative health resources such as online magazines or health-related websites in place of seeking health information from a physician. Implications from this finding support the increased use of reliable internet sources to supplement PCa information provided at community screening events. A strength of this study was the large proportion of Black men who attended the community screening and completed the mail-in follow-up surveys. As Black men are at a higher risk of developing and dying from PCa, this study supports previous findings that community-based cancer screenings are an effective mechanism to attract patients from high-risk groups (Ashorobi et al., 2015; Jandorf et al., 2006; Johnson, Nemeth, Mueller, Eliason, & Stuart, 2016; Ornelas et al., 2017; Patel et al., 2012; Torres et al., 2017). Ashorobi et al. (2015) used community health centers and a mobile screening bus to provide free PCa education and screenings to underserved communities. Similar to this study, the majority of this sample had no prior history of a prostate screening. Community-based screenings not only show promise for engaging men in screening behaviors, but can also be a source of cancer education for this high-risk population.
This study is among the first to report medical and nonmedical follow-up actions completed after a community-based PCa screening event targeting Black men. This study has several health promotion and health education implications. The high frequency of respondents who shared their PSA screening results with their spouse/partner supports PCa educational interventions targeting men and their partners. In a previous PCa communication study, interviews of married Black couples revealed shared perceptions, preferences, and practices related to PCa information seeking (Friedman, Thomas, Owens, & Hébert, 2012). Educational materials that concurrently target men at high risk of PCa and their partners are a promising strategy to motivate communication between men and their physicians. In this study, health behavior change was the most common nonmedical activity completed by men following the PCa screening; therefore, addressing cancer prevention through diet and physical activity modifications in a community-based screening event may be a beneficial approach.
A limitation of this study is the small proportion of the original population that were surveyed in the follow-up study. This retention rate is 30% and is lower than some studies (Shen, Xu, & Eisenberg, 2016; Wessels et al., 2011; Witt et al., 2014); however, there was no difference for most demographics between responders and non-responders. Secondly, post-PSA activities were based on retrospective self-reports, which may not accurately reflect all activities completed by participants. Self-reported bias is potentially further augmented by follow-up contact from study staff. Finally, the study sample included participants from 2007 to 2011. It is important to note that in 2008, the United States Preventive Services Task Force (USPSTF) had insufficient evidence to evaluate the benefits or and dangers for PSA screening for men <75 years old (U.S. Preventive Services Task Force, 2008). While the United States Preventive Services Task Force (USPSTF) did not recommend patient–provider discussions regarding PSA screening for men aged 55–69 years old until 2018, these findings must be interpreted in the context of the 2008 USPTF recommendations.
This current study adds to the literature on the effectiveness of community-based events on screening uptake in high-risk populations. Specifically, these results reveal the medically and nonmedically related activities completed by a mostly Black sample of men after participating in a PCa screening. This current study is important as it shows that men participating in a cancer-screening event are likely to seek their health-care provider and modify their health behaviors. This population of men revealed additional channels to improve PCa health promotion and education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the National Cancer Institute, 1 U01 CA114594-01, 1U54CA153460-01, and the St. Louis Mens Group Against Cancer. Washington University School of Medicine, the Barnes-Jewish Hospital Foundation, and Siteman Cancer Center also supported this research.