
Abstract
Many studies have explored the relationship between masculine norms and men’s health outcomes. There are few recent studies published on the relationship between masculine/instrumental and feminine/expressive traits and men’s health and well-being. The current cross-sectional study examines whether masculine/instrumental and feminine/expressive traits are associated to men’s health and well-being. Participants were 1,870 Spanish men, aged 21 to 64 years. Results from hierarchical multiple regression analysis indicated that the masculine/instrumental trait and the feminine/expressive trait were positively related to men’s psychological well-being and self-rated health, so that men whose self-concept includes both masculine/instrumental and feminine/expressive characteristics presented greater psychological well-being and better self-rated health. The feminine/expressive trait was associated with lower psychological distress yet only in case of men with low social support. Self-esteem and social support were important predictors of men’s health, in such a way that men who had high self-esteem and social support reported higher ratings of psychological well-being, better self-rated health, and less psychological distress. The implications of these findings for promoting men’s health and well-being are discussed.
Keywords
Research has reported differences between men and women in some health indicators. Male life expectancy is lower than female life expectancy (Eurostat, 2018; World Health Organization [WHO], 2018). Another area in which consistent differences between women and men have been identified is mental health, as revealed by population surveys and epidemiological studies. Men reported higher rates of antisocial personality and substance use disorders, whereas women reported higher rates of depression and anxiety disorders (e.g., Eaton et al., 2012; Seedat et al., 2009). Worldwide rates of male suicide rank higher than rates for women (WHO, 2014, 2018).
Psychological distress (PD) is a mental health outcome characterized by behavioral and psychophysiological symptoms that are not specific to a given mental pathology (Marchand, Drapeau, & Beaulieu-Prévost, 2011), and it stands as a widespread indicator of mental health and psychopathology in public health and in research and clinical settings (Drapeau et al., 2010). Depression and anxiety symptoms are the most frequent indicators of PD (Drapeau et al., 2010; McLachlan & Gale, 2018; Simms, Prisciandaro, Krueger, & Goldberg, 2012) although some others have been included, namely insomnia and somatic symptoms (Kessler et al., 2002; Simms et al., 2012). Research conducted over the past decade has made clear that PD increases risk of developing some diseases such as arthritis, chronic obstructive pulmonary disease, and cardiovascular disease, even at moderate and low distress levels (McLachlan & Gale, 2018); moreover, PD is associated with increased risk of mortality from several major causes, even at lower levels of distress (Russ et al., 2012).
Self-rated health (SRH) is a widespread method to assess health perceptions in populations, and it has been extensively employed in health research and practice as a marker of general health (El-Ansari & Stock, 2016; Lidström, Wennberg, Lundqvist, Forssén, & Waller, 2017). SRH has proved to be an important predictor of morbidity and mortality (Barger, Cribbet, & Muldoon, 2016; El-Ansari & Stock, 2016; Hu et al., 2016; Nielsen, 2016).
The biomedical health model, centered exclusively on illness and disease, has prevailed in the Western world in spite of the fact that, as early as in 1948, the WHO defined health not merely as the absence of illness or infirmity but, in a broader sense, as “a state of complete physical, mental and social well-being” (WHO, 1948, p. 16). This has been changing over the last decades, and psychological well-being (PWB) has achieved a prominent role. From this perspective, Ryff’s (1989) multidimensional model and measure of PWB is a widely used instrument, and research has supported the health protective role of PWB (Ryff, 2014).
Gender is recognized as an important social determinant of health (Fleming & Agnew-Brune, 2015), and is associated with and influences health-related behavior (Courtenay, 2000). Research on the relationship between masculinity-related constructs and men’s health and well-being has identified complex relationships, although the results may be determined by the substantial change that the masculinity construct has undergone since the 1960s to 1970s (e.g., Levant & Wong, 2017; Smiler, 2004). Former research focused on the relationship between sex role orientation and mental health, and meta-analysis made evident that masculinity had a positive relationship to adjustment, self-esteem, and mental health (Bassoff & Glass, 1982; Whitley, 1983, 1985). From the 1980s on, theoretical perspectives have been shifting toward the study of masculine social norms and the social construction of masculinity; in the United States, gender role conflict, gender role strain, and masculinity ideologies have stood prominently in the major theory positions and associated research (Levant & Wong, 2017). Research reviews published in the last decade generally conclude that conformity to masculine norms and gender role conflict are related to men’s psychological and interpersonal problems, which are negatively associated with men’s health and well-being (e.g., Gerdes, Alto, Jadaszewski, D’Auria, & Levant, 2018; Griffith, Gunter, & Watkins, 2012; O’Neil, 2008; Wong, Ho, Wang, & Miller, 2017), although results differed depending on the specific dimension analyzed (Gerdes & Levant, 2018; Griffith et al., 2012; Kaya, Iwamoto, Brady, Clinton, & Grivel, 2019; Wong et al., 2017).
Some important issues to consider in research about masculinity-related constructs and health are operationalization of masculinity, which varies between studies, and the different health measures that are made use of (Griffith et al., 2012; Wong et al., 2017). After examining the association between masculinity and health in 22 population-based studies, Griffith et al. (2012, p. S187) determine that “The associations between masculinity and health were complex and varied by construct and health outcome.”
Although masculinities can be diverse and influenced by culture variants, agency and communion are central traits in the cultural framing of gender (Eagly & Wood, 2017). As Haines, Deaux, and Lofaro (2016, p. 354) assert “Agency and communion have been the core dimensions used to characterize gender stereotypes as well as gender-relevant self-descriptions.” Masculinity is associated with an instrumental orientation, central to which is agency, in turn characterized by focusing on the self and oriented toward independence and the achievement of personal goals. On the contrary, femininity is related to an expressive orientation, to which communion, defined as focus on the other and an orientation emphasizing connection of self with others, is central (Bem, 1993). Gender stereotypes characterize women and men as complementary: men are perceived to be agentic but not communal, whereas women are perceived to be communal but not agentic (Kahalon, Shnabel, & Becker, 2018). But agency and communion are universal dimensions of human behavior and are basic dimensions of social motives and social judgments and behaviors (Locke, 2015).
The masculine/instrumental trait includes positive aspects of masculinity such as assertiveness, independence, self-reliance, or willingness to take risk, and research has reported that the masculinity trait was positively related to mental health (Bassoff & Glass, 1982), self-esteem (Whitley, 1983) and general adjustment, and negatively associated with depression (Whitley, 1985).
In today’s life, the concept of self-esteem is ubiquitous (Orth & Robins, 2014). Self-esteem is a relatively stable trait and refers “to an individual’s subjective evaluation of his or her worth as a person” (Orth & Robins, 2014, p. 381). Research had identified the relationship between self-esteem and physical and mental health (Orth & Robins, 2014; Orth, Robins, & Widaman, 2012; von Soest, Wagner, Hansen, & Gerstorf, 2018). Longitudinal research has indicated that high self-esteem predicts success and well-being in important life domains (Orth, 2017; Orth & Robins, 2014). High correlations between self-esteem and masculinity have also been reported, although they are acknowledged to be distinct constructs (Whitley & Gridley, 1993).
Social support has been long known to exert considerable influence on health and well-being (Santini, Koyanagi, Tyrovolas, Mason, & Haro, 2015; Siedlecki, Salthouse, Oishi, & Jeswan, 2014; Thoits, 2011). High social support has been related to SRH across countries (Kumar, Calvo, Avendano, Sivaramakrishnan, & Berkman, 2012); while lower levels of social support were associated with increased PD (Saikkonen, Karukivi, Vahlberg, & Saarijärvi, 2018).
The main objective of this study was to investigate in a large sample of Spanish adult men whether masculine/instrumental and feminine/expressive traits among males are related to health and well-being, operationalized in this research as PWB, PD, and SRH. A secondary goal was to examine the relevance of self-esteem and social support in the health and well-being of adult men. Since agency, characterized by focus on the self, is central to masculinity, and communion, characterized by focus on others and by forming connections, is a central characteristic of femininity, the interactions between masculinity and femininity with self-esteem and social support were investigated. Based on previous research, we propose the following hypotheses:
Men with higher scores on the masculine/instrumental trait will have greater PWB, better SRH, and less PD.
Men with higher self-esteem will present greater PWB, better SRH, and less PD.
Men with more social support will report greater PWB, better SRH, and less PD.
Method
Participants
The participants consisted of 1,870 men from the Spanish general population. Their ages ranged between 21 and 64 years (M = 40.43, SD = 12.86) and men had different educational levels and different occupations: 9.5% (n = 177) were still students, 35.5% (n = 663) were blue-collar workers, 32.7% (n = 612) white-collar workers, 20.7% (n = 388) were professionals, and 30 (n = 1.6%) did not report their occupation. As regards marital status, 39.4% (n = 737) were single, 54.1% (n = 1011) married or living with a partner, 5.8% (n = 108) separated or divorced, 0.3% (n = 6) widowed, and 8 men (n = 0.4%) did not specify their marital status. Less than half of men (46.0 %) (n = 861) did not have children, and the rest had from 1 to 8 children, though most commonly they had two (27.7 %) (n = 518) or one (16.5 %) (n = 308), and 16 men (n = 0.9%) did not report if they had children.
Measures
Dependent variables: PWB, PD, and SRH
PWB was measured with the Spanish version of the Ryff’s Psychological Well-Being Scale proposed by Van Dierendonck, Díaz, Rodríguez-Carvajal, Blanco, and Moreno-Jiménez (2008). This scale consists of 38 items; the authors identified a factorial structure consisting of six factors (self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth) and one underlying second-order well-being factor. The items were scored on a 6-point Likert scale from 1 (strongly disagree) to 6 (strongly agree), and higher scores indicating greater PWB. For the present study, the second-order well-being factor was used and this factor demonstrated a good internal consistency (α = .92).
Participants’ PD was assessed by using the subscales of anxiety and insomnia, severe depression, and somatic symptoms of the 28-item version of the General Health Questionnaire (GHQ-28; Goldberg & Hillier, 1979). It is a self-report instrument that assesses present and recent complaints and measures somatic, anxiety and insomnia, and severe depression symptoms. Items were scored according to the Likert-type scale that assigns a weight to each score, from 0 (less than usual) to 3 (much more than usual). Following an exploratory factor analysis, factor score was computed and used in subsequent analyses as PD measure. Higher scores indicated higher levels of PD, and for the present sample the Cronbach’s α reliability test of 21 items on the three subscales was .90.
SRH was assessed on a 5-point ordinal scale answer to the question “How would you rate your overall health at the present time?”, with the possible choices being “very good,” “good,” “moderate,” “bad,” and “very bad.” Scores were assigned from 0 (for very bad) to 4 (for very good), so high scores indicated better SRH.
Independent variables: Masculine/instrumental and feminine/expressive traits, self-esteem, and social support
The Bem Sex Role Inventory (BSRI, Bem, 1974) was used to assess masculine/instrumental and feminine/expressive traits. The BSRI is a self-report inventory that assesses people’s endorsement of socially desirable personality traits that are stereotypically associated with men and women. BSRI consists of 60 items formed by adjectives or short sentences, 20 of which refer to characteristics traditionally regarded as masculine, which make up the masculinity scale; 20 characteristics traditionally regarded as feminine, which make up the femininity scale; and 20 items formed by characteristics attributable to both genders. The masculinity scale reflects an instrumental or agentic orientation, whereas the femininity scale reflects an expressive or communal orientation (Helgeson, 2015). The response format is a 7-point Likert scale ranging from 1 (never or almost never true) to 7 (always or almost always true). Higher scores in the masculinity scale indicate greater levels of men’s endorsement of the masculine/instrumental trait, and higher scores in the femininity scale indicate greater levels of men’s endorsement of the feminine/expressive trait. All items were translated into Spanish and back into English by the research team plus two bilingual persons, a native English-speaking professional translator, and a native speaker of Spanish. For the current sample, the Cronbach’s α reliability of the 20 items on the masculinity scale was .82, and of the 20 items on the femininity scale was .79.
Self-esteem was assessed by using the Spanish version of the York Self-Esteem Inventory (YSEI; Rector & Roger, 1993), an inventory that measures global self-esteem. The scale is comprised of 58 items which reflect various evaluative self-domains, including personal, interpersonal, familial, achievement, physical attractiveness, and the degree of uncertainty across the domains. Items were rated on a 4-point Likert scale ranging from 0 (never) to 3 (always); higher scores indicate greater levels of self-esteem. For the present sample, the Cronbach’s α coefficient for the self-esteem factor was .94.
Social support was measured by using the Social Support Scale (Matud, 1998). It consisted of 12 items, rated on a 4-point Likert scale ranging from 0 (never) to 3 (always), which gather information about the possibility of access to other persons who can support with affective, economic, labor, familiar and advice/guidance needs. These areas are grouped into a second-order factor whose Cronbach’s alpha for the current sample was .91.
Two demographic variables were included in the analysis: participants’ age, which was treated as a continuous variable, and educational level, which was approached as an ordinal variable with seven levels. Scores were assigned from 1 (for basic education) to 7 (for 5-year university degree), so high scores indicated a greater educational level.
Procedure
This study is part of larger research on gender and health in Spain, which was positively evaluated by the Ethics Committee on Animal Research and Well-Being of the University of La Laguna (study approval number 2015-0170). All participants were volunteers, and were not remunerated for their participation. To avoid systematic biases, access to the participants was through various work centers and educational centers, both public and private, located all over the Spanish autonomous communities and by having recourse to the social net of psychology and sociology university students trained in administering those tests, who received course credits for that task. Questionnaires and SRH questions were filled out manually by each individual after verbal reported consent was obtained, and no names or any other data identifying the participant were used. The American Psychological Association ethical standards in the treatment of the sample were complied. For the purposes of this study, only those sample male participants with ages between 21 and 64 years were included in the analysis.
Data analysis
General descriptive statistics were computed to describe the demographic characteristics of the participants. Bivariate association between the study variables was calculated by using Pearson r correlation coefficient. To achieve the objectives and to test the study’s hypotheses, hierarchical multiple regression analyses were conducted. The criterion considered was the score in PWB in the first regression, the score in PD in the second, and the score in SRH in the third regression analysis. Logarithmic transformations were used on PD to reduce skewness. In each regression analysis, age and educational level were included in Step 1 to control their effect. The remaining predictor variables were expressed in mean deviation form, and interaction was the product of these mean-centered variables (Aiken & West, 1991). At Step 2, masculinity and femininity scores were entered. At Step 3, self-esteem, and interactions of self-esteem with masculinity and with femininity were included. And, at Step 4, social support, and interactions of social support with masculinity and with femininity were added to. Significant interactions were explored using Aiken and West’s (1991) guidelines of one standard deviation above and below mean. Statistical analyses were carried out using the software IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY).
Results
Pearson r correlations among the three health measures included as dependent variables in this study were statistically significantly, although only the correlation coefficient between PWB and PD was large (r = −.50, p < .001) in terms of magnitude of effect size according to Cohen (1988). SRH was positively associated with PWB (r = .28, p < .001) and negatively associated (r = −.34, p < .001) with PD.
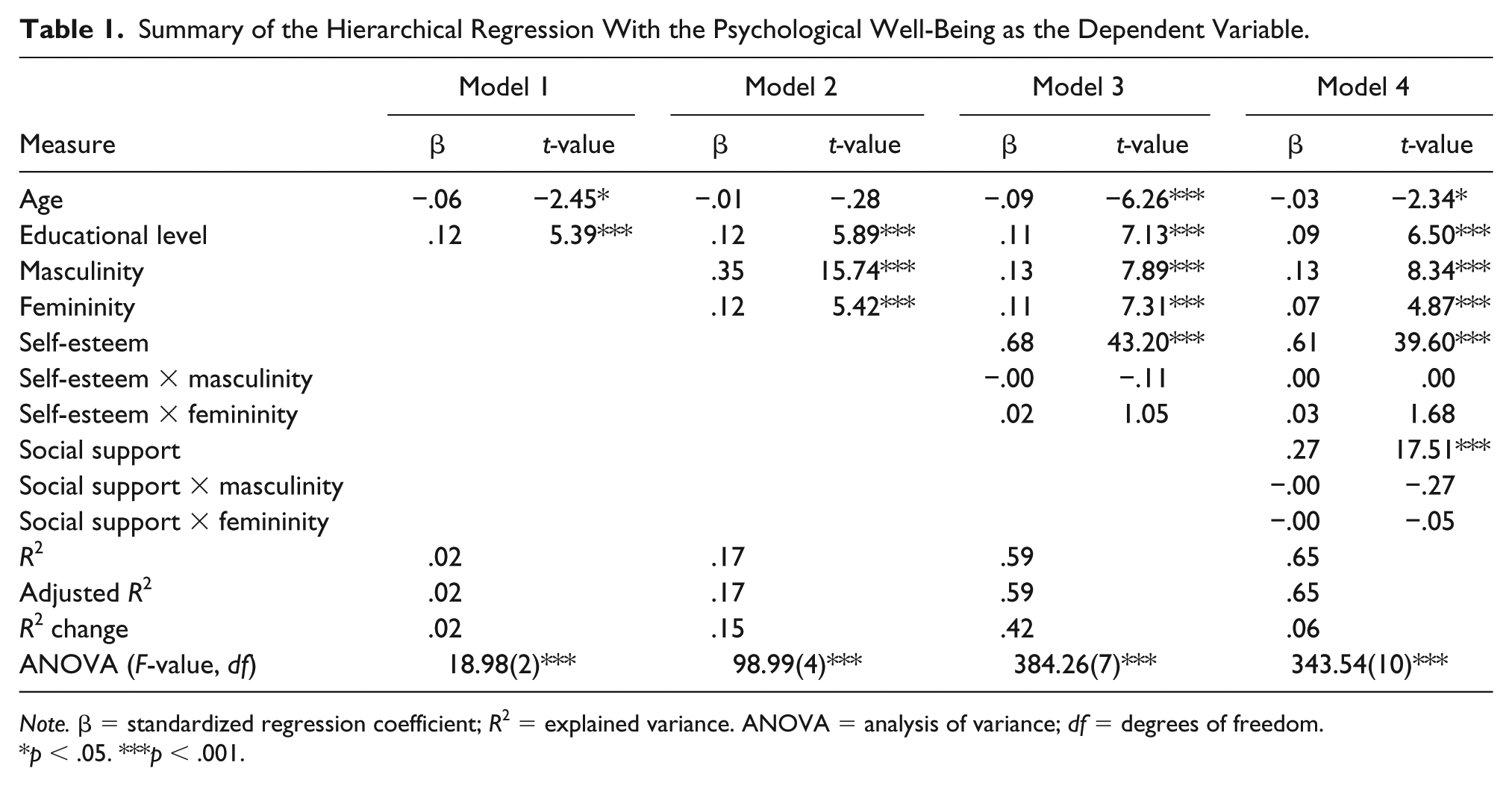
Table 1 presents the standardized regression coefficients (β) with their corresponding t values, and the F and R2 values for the four regression models with the PWB as the dependent variable. Results identified that R for regression was significantly different from zero at the end of each step. In Model 4, with all IVs in the equation, R2 = .65, p < .001; the adjusted R2 value of .65 indicated that 65% of the variability in men’s PWB is predicted by self-esteem, social support, masculinity, femininity, educational level, and men’s age.
Summary of the Hierarchical Regression With the Psychological Well-Being as the Dependent Variable.
Note. β = standardized regression coefficient; R2 = explained variance. ANOVA = analysis of variance; df = degrees of freedom.
p < .05. ***p < .001.
After Model 1, with age and educational level in the equation, R2 = .02, p < .001. The change in R2 from Model 1 to Model 2 identified that masculinity (β = .35, p < .001) and femininity (β = .12, p < .001) play a significant role in men’s PWB. The addition of self-esteem and the interactions of self-esteem with masculinity and with femininity in Model 3 resulted in an important increment in R2 (R2 change = .42, p < .001), although the interactions were not statistically significant. The addition of social support and the interactions of social support with masculinity and with femininity (Model 4) also yielded an increment in R2 (R2 change = .06, p < .001) but interactions were not statistically significant.
Beta values in Model 4, with all IVs in the equation, proved that self-esteem was the variable most associated with men’s PWB (β = .61, p < .001). The second most relevant variable was social support (β = .27, p < .001); masculinity was the third most relevant variable (β = .13, p < .001), followed by educational level (β = .09, p < .001), femininity (β = .07, p < .001), and age, although the β value for age was very low (β = −.03, p < .05).
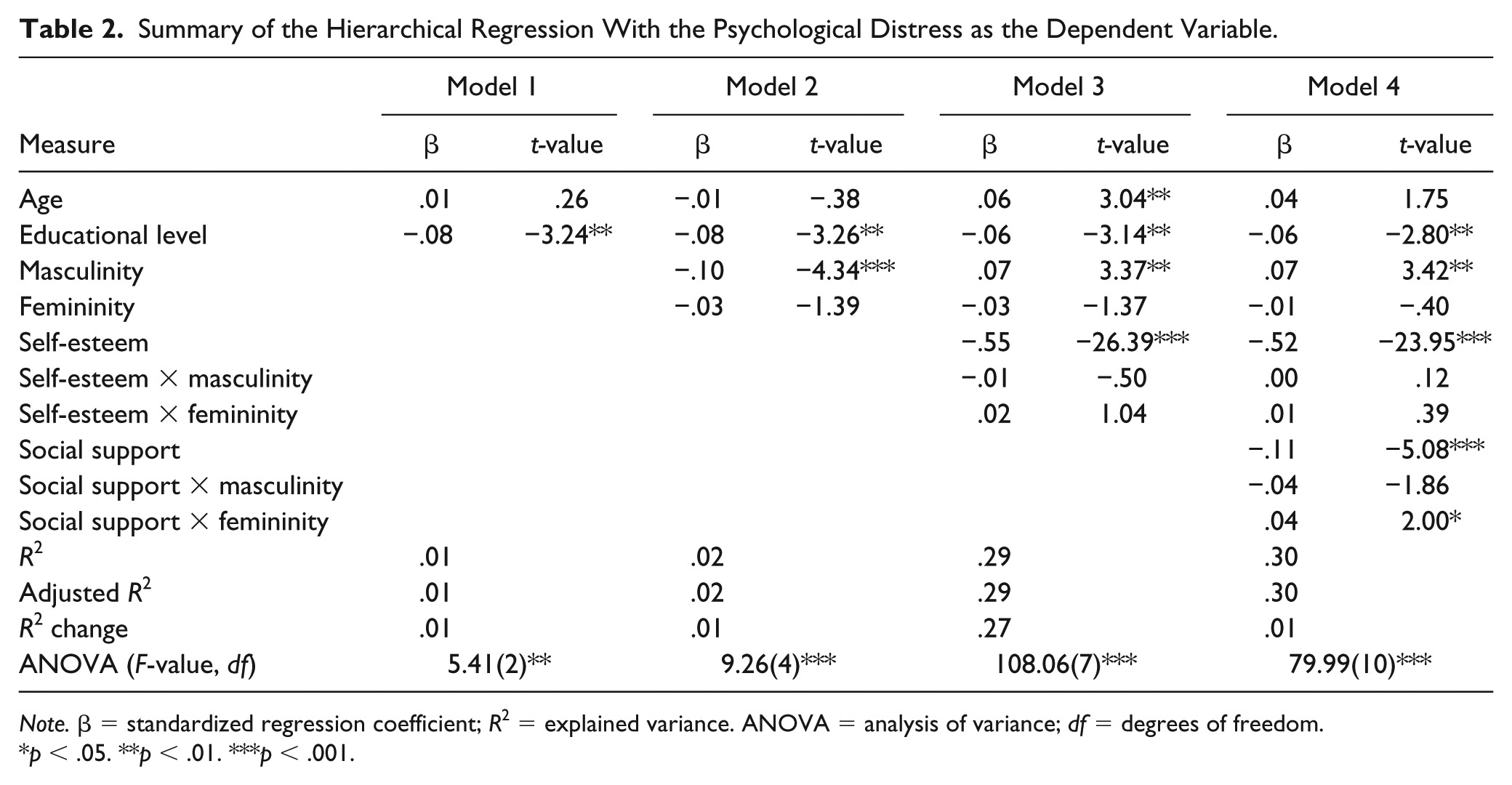
Table 2 displays the results of the four regression models with the logarithm of PD as the dependent variable. R was significantly different from zero at the end of each step. The inclusion of self-esteem and the interactions of self-esteem with masculinity and with femininity in Model 3 increased the adjusted R2 to .29 (R2 change = .27, p < .001); it had a noticeable effect on the association between masculinity and PD, although the interaction of self-esteem with masculinity was not statistically significant. In Model 4, social support and the interaction between social support and femininity were identified to be statistically significant. As can be seen in Figure 1, although men with high social support (1 standard deviation above the mean) presented less PD than men with low social support (1 standard deviation below the mean), femininity was significantly associated with PD only in the case of men with low social support. Post hoc regressions for probing interaction made evident that for men with low social support (n = 331) femininity was an important predictor of PD, F(1, 329) = 7.52, p = .006. The adjusted R2 was .019, β = −.15, p = .006, and r = −.15. R for regression in men with high social support (n = 338) was not statistically significant, F(1, 336) = 2.99, p = .09. The adjusted R2 was .006, β = .09, p = .85, and r = .09.
Summary of the Hierarchical Regression With the Psychological Distress as the Dependent Variable.
Note. β = standardized regression coefficient; R2 = explained variance. ANOVA = analysis of variance; df = degrees of freedom.
p < .05. **p < .01. ***p < .001.

Two-way interaction of social support and femininity predicting men’s psychological distress symptoms.
Model 4, with all IVs in the equation, predicted 30% of the variability in (log of) PD. The final model rendered that the higher levels of self-esteem, social support, educational level, and femininity in men with low social support, were associated with lower levels of PD; high masculinity was related to higher levels of PD.
The principal results of the regression models with the SRH as the dependent variable are presented in Table 3. After Step 1, with age and educational levels in the equation, R2 = .08, p < .001. The changes in the R2 from Model 1 to Model 4 indicate that masculinity, femininity, self-esteem, and social support play a significant role in the men’s SRH, although the interactions between masculinity and femininity with self-esteem and social support were not statistically significant. Collectively, 16% of the variance in SRH was accounted for by all of the variables in the model. The beta values in the final model indicated that age was the variable most associated with SRH, with better SRH in younger men. Other relevant variables in SRH were self-esteem, masculinity, social support, femininity, and educational level, which were associated with better men’s SRH.
Summary of the Hierarchical Regression With the Self-Rated Health as the Dependent Variable.

Note. β = standardized regression coefficient; R2 = explained variance. ANOVA = analysis of variance; df = degrees of freedom.
p < .01. ***p < .001.
Discussion
Many studies have explored the relationship between masculine norms and related constructs and men’s health/well-being outcomes (e.g., Gerdes et al., 2018; Gerdes & Levant, 2018; Milner, Kavanagh, King, & Currier, 2018; Wong et al., 2017). There are few recent studies published on the relationship between positive aspects of masculinity and men’s health. The main objective of this study was to examine the relationship between masculine/instrumental and feminine/expressive traits among males and health, operationalized as PWB, PD, and SRH, in a large community sample of adult Spanish men. The first study’s hypothesis predicting that men with higher scores on the masculine/instrumental trait would have greater PWB, better SRH, and less PD, was not fully supported. The findings of regressions analysis indicated that masculine/instrumental and feminine/expressive traits were significantly associated with the three health measures, although the percentage of variance explained by each of the traits differed and changed in the different regression models, particularly when self-esteem was added to prediction. This suggests that the relationship between masculine/instrumental and feminine/expressive traits and men’s health is complex and can be mediated and/or moderated by other variables.
As for the regression analysis with PWB as the dependent variable, after adjustment for age and educational levels, the beta value for masculine/instrumental trait decreased when self-esteem and the interactions between self-esteem with masculinity and with femininity were added to the equation; however, interactions were not statistically significant. Although the interactions weren’t either statistically significant, the beta values for feminine/expressive trait lowered when social support and the interactions between social support with masculinity and with femininity were added to the equation. Eventually, beta values in the final model indicated that both masculinity/instrumental and femininity/expressive traits were significantly associated with men’s PWB, although the relationship was stronger for masculinity than for femininity. These findings converged with and expanded on existing literature (Whitley, 1983). Although the effect size was smaller than for masculinity, Whitley’s meta-analysis revealed that, in some studies, femininity in men was also positively associated with general adjustment and self-esteem (Whitley, 1983). In addition, other studies had revealed that agentic traits and values were associated with well-being (Bassoff & Glass, 1982; Pietraszkiewicz, Kaufmann, & Formanowicz, 2017).
Regression analysis findings with log of PD as the dependent variable also highlighted that the relationship between masculine/instrumental and feminine/expressive traits with mental symptomatology is complex. After adjustment for age and educational levels, the beta value for masculine/instrumental trait was negative but when self-esteem and the interactions between self-esteem with masculinity and with femininity were added to the equation, the beta value for masculinity was positive. The reason for this change in the beta value for masculine/instrumental trait when self-esteem was added to the prediction of PD should be examined in future research. In the latter model, the interaction between social support and femininity was statistically significant and post hoc analysis identified that femininity is a protective factor against distress only in men with low social support.
The secondary goal of this study was to examine the relevance of self-esteem and social support in the health and well-being of adult Spanish men. The study results yielded that self-esteem was the strongest predictor of both, PWB and PD, and was the second most important predictor of SRH, after lower age. The second hypothesis, predicting that men with more self-esteem would present greater PWB, better SRH, and less PD was supported. The present findings converge with previous findings on the positive relationship between self-esteem and physical and mental health (Orth, 2017; Orth & Robins, 2014; Orth et al., 2012; von Soest et al., 2018).
Social support was an important predictor of men’s health, too. Study results made evident that men who had more social support reported greater PWB, better SRH, and less PD, so the third study hypothesis was supported. These results agree with those of other studies which have realized associations between social support and lower levels of PD (Saikkonen et al., 2018), and greater health and well-being (e.g., Kumar et al., 2012; Siedlecki et al., 2014).
Some limitations in this study should be considered. The first one is that this is a cross-sectional design; therefore, no cause–effect inferences can be made. The sample, though large and with men with very different demographic characteristics, is a convenience sample. Another limitation to consider is that all the participants lived in Spain, which may restrict the generalization of results with respect to other countries. Femininity was associated with better men’s health and well-being, although to a lesser extent than masculinity; yet there is no certainty about the existence of any levels and/or combinations of the masculine/instrumental trait and the feminine/expressive trait that are more optimal for men’s health and well-being.
The present study was also limited by the demographic variables included in the analyses. The inclusion of variables such as occupation, marital status, or children would have increased the knowledge of the relevance of these variables in men’s health and well-being. Eventually they were not included in this study because, in addition to not being directly related to the objectives of the work, initial analyzes proved that the number of children and marital status were significantly associated with age, and occupation with educational level. Since such variables may be important in men’s social support, well-being, and self-esteem, their study should be addressed in future research.
In addition, further studies are needed to examine the complex relationships that seem to exist between the masculine/instrumental trait and self-esteem when it comes to predicting PWB and, above all, distress.
Conclusion
Findings in this study identified that those men who scored high on the masculine/instrumental trait were more likely to have better SRH and to have more PWB. But these health outcomes were also associated with men’s high feminine/expressive trait, although the effect size was smaller than for masculinity. Thus, men whose self-concept included both, instrumental and expressive characteristics, are more likely to have better SRH and greater PWB. These results are relevant to policy makers and service providers interested in promoting men’s health and well-being and in enhancing gender equality.
Despite the social changes that have taken place over the last decades in developed countries, gender stereotypes do persist (Drake, Primeaux, & Thomas, 2018; Haines et al., 2016), and essentialist considerations of gender as difference still linger in popular culture, media, and scientific writings (Shields, 2013). As this author contends, essentializing discourses abiding in popular culture are absorbed in scientific discourses and gain scientific authorization via research; and, most important, these results circulate back again to popular culture, so the cycle continues. In order to break this cycle, the transfer of research results reporting empirical data about the realities about men is of the utmost importance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Ministry of Economy and Competitiveness of Spain (Reference: PSI2015-65963R, MINECO/FEDER, UE).