
Abstract
Based on longitudinal data from the Health and Retirement Study, this study assesses the importance of marital status in explaining racial disparities in all-cause mortality during an 18-year follow-up among White and African American men aged 51 to 61 years in 1992. Being married was associated with significant advantages in household income, health behaviors, and self-rated health. These advantages associated with marriage at baseline also got translated into better survival chance for married men during the 1992-2010 follow-up. Both marital selection and marital protection were relevant in explaining the mortality advantages associated with marriage. After adjusting for the effect of selected variables on premarital socioeconomic status and health, about 28% of the mortality gap between White and African American men in the Health and Retirement Study can be explained by the relatively low rates of marriage among African American men. Addressing the historically low rates of marriage among African Americans and their contributing factors becomes important for reducing racial disparities in men’s mortality.
One of the central themes in social epidemiology concerns racial disparities in health and mortality. In 2006, life expectancy at birth was 78.2 years for non-Hispanic Whites and 73.2 years for African Americans (Heron, Hoyert, Xu, Scott, & Tejada-Vera, 2008). It was estimated that, had the racial gap in mortality been eliminated, an excess of 83,570 deaths in the United States could have been prevented in the year of 2002 alone (Satcher et al., 2005). Mitigating racial disparities in mortality becomes important for improving the well-being of African Americans as well as the whole U.S. population.
An important contributing factor to racial disparities in mortality could be the historically low rates of marriage among African Americans. In 2012, only 43.2% of African American households were headed by a married couple, as compared to 78.6% among non-Hispanic White households (U.S Census Bureau, 2014). The retreat from marriage has been more substantial among African Americans than among Whites during the past half century. In 1960, 61% of Black adults were married; by 2008, that share had dropped to 32%. The corresponding change among Whites was from 74% in 1960 to 56% in 2008 (Pew Research Center, 2010). Despite marriage decline in both racial groups, such a magnitude of divergence in marriage between Whites and African Americans has given rise to the outcry “Is marriage for White people?” (Banks, 2011).
The central hypothesis in this study is that the substantial gap in marriage rates between White and African American males has contributed to racial disparities in mortality. The reason is that, relative to being unmarried, marriage is generally associated with advantages in health among both Whites and African Americans. These advantages tend to benefit men more than they do women (Backlund, Sorlie, & Johnson, 1996; Pappas, Queen, Hadden, & Fisher, 1993; Sorlie, Backlund, & Keller, 1995; Waite, 1995; Williams & Umberson, 2004).
Literature Review
Racial Divergence in Marriage Rates and Its Causes
The past five decades witnessed a substantial retreat from marriage in the United States. According to an analysis by the Pew Research Center, only 9% of adults aged 18 to 24 years in the United States were married in 2010, compared to 45% in 1960. Among adults aged 25 to 34 years, 44% were married in 2010, compared to 82% in 1960 (Taylor et al., 2011). This historical retreat from marriage is closely related to a series of interrelated economic, social, and cultural shifts in the 20th century that have altered the meaning of marriage and redefined the roles of men and women in society (Oropesa & Landale, 2004; Smock, 2004). On one hand, increasing access to education and participation in the labor force has given women the economic independence needed to stay single. Such a trend was further facilitated by structural transformations in the U.S. economy that have been tilted toward the service sector over time, creating more job opportunities for women than for men. In response to the upgrading of the U.S. economy, young men and women have to spend more time in their education, which has resulted in delays in marriage or no marriage at all. On the other hand, concurrent with the decline of marriage and the rise of new forms of families is a shift in public opinion of marriage. In 2010, about 4 of every 10 American adults believed that marriage was obsolete, as compared to 29% in 1978 (Pew Research Center, 2010).
Note, however, that the decline in marriage has been more substantial among African Americans than among Whites, resulting in racial divergence in marriage over time. According to a study by Koball (1998), there was a racial crossover in men’s marriage timing during the 20th century. Before World War II, the median age at marriage for White men was later than that for African American men. Since World War II, African American men have, on average, married later than White men. Furthermore, there is evidence suggesting that racial divergence in marriage rates might have become more apparent during the second half of the 20th century. As indicated in Figure 1, among White males aged 15 years and older in 1950, the proportion of those who were married was 68%, as compared with 64% among African American males. The corresponding proportions dropped to 56.9% and 39.4%, respectively, by the year of 2010. As a result, the racial gap in terms of marriage expanded from about 4% in 1950 to 17.5% in 2010.
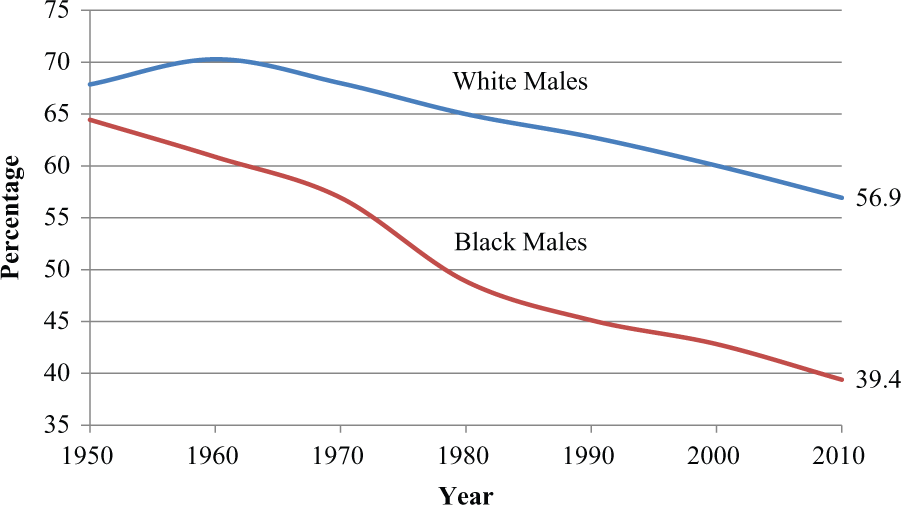
Percentage of Currently Married Among Males 15 Years or Older by Race: 1950-2010.
Despite the attention that it has received, the divergence of marriage rates by race largely remains an enigma (Raley, 2000). Several reasons have been proposed to explain the historically low marriage rates among African Americans. One of them traced all the way back to slavery. As slaves were traded, family ties among African Americans were often disrupted, resulting in disorganization of African American families and concordant cultural values that tend to be receptive to family separation and instability (Frazier & Glazer, 1966). After the abolishment of slavery, more attention has been paid to the lack of economic opportunities for African American males. One widely cited explanation is a hypothesis put forward by Williams Julius Wilson (1987) that relates low marriage rates among African Americans to the loss of employment opportunities for African American males. As the postindustrial U.S. economy is upgrading its structure in the context of globalization, more and more jobs have shifted away from the traditional manufacturing sector, such as the automobile, rubber, and steel industries, which has disproportionally reduced job opportunities for African American males. The loss of traditional “breadwinner” identity for many African American males, in combination with the high incarceration rates (Tucker & Mitchell-Kernan, 1995), has substantially shrunk the pool of eligible bachelors among African Americans (Schoen, 1995).
Meanwhile, immigration to the United States since the 1960s might have negatively affected wages and job opportunities for African American males. On the basis of data from the 1960-2000 U.S. censuses, Borjas, Grogger, and Hanson (2006) reported that the employment rate of Black men fell from 74.9% in 1960 to 67.9% in 2000. The corresponding drop, however, was far more substantial among Black high school dropouts, from 72.1% to 42.1%. The study identified a strong correlation among immigration, Black wages, Black employment rates, and Black incarceration rates. As immigrants disproportionately increased the supply of workers in a particular skill group, the wage of Black workers in that group fell, the employment rate declined, and the incarceration rate rose. It was also reported that although the wage effect of immigration was similar for Black and White men, the negative employment effect and the positive incarceration effect were larger for Blacks.
There is evidence that welfare policies might have unintentionally incentivized many low-income African Americans to opt for cohabitation rather than getting married. One of the primary goals of the 1996 Personal Responsibility and Work Opportunity Reconciliation Act was to end the dependency of needy parents on government benefits, in part by promoting marriage. However, the act may have unintentionally decreased the incentives to be married by giving women greater financial independence via the program’s new emphasis on work (Bitler, Gelbach, Hoynes, & Zavodny, 2004). Teitler, Reichman, Nepomnyaschy, and Garfinkel (2009) examined the impact of welfare participation on transitions to marriage among mothers who have had a nonmarital birth. Their findings suggested that while welfare participation reduced the likelihood of transitioning to marriage, this occurred only when the mother was receiving benefits. Once the mother left welfare, past receipt had little effect on marriage. The authors further inferred that the negative association between welfare participation and subsequent marriage reflected temporary economic disincentives rather than an erosion of values.
Marriage and Health
It has been well established that, relative to their nonmarried counterparts, married persons tend to have a significant advantage in health. Numerous studies have consistently revealed that mortality rates for married persons are lower than those for unmarried persons (Lillard & Panis, 1996). The health advantages associated with marriage tend to benefit men more than they do women (Backlund et al., 1996; Pappas et al., 1993; Sorlie et al., 1995; Waite, 1995; Williams & Umberson, 2004). A plausible explanation for this gender difference pertains to social control and social integration in marriage and how this function of marriage may vary for men and women. Based on results from two national panel surveys, a study by Umberson (1992) identified that marriage is associated with substantially more efforts to control health for men than for women and those who attempt to control the health of spouses are more likely to be females than males. This means that married men, relative to their unmarried counterparts, are generally less likely to be involved in unhealthy or risky behaviors, such as smoking, alcohol abuse, speeding, delaying seeking health care, and so forth, because of their wives’ monitoring and prodding.
Three major explanations are relevant to account for the association between marriage and health. The first explanation is that healthier persons are more likely to get married and stay married, which is referred to as the selection hypothesis (Joung et al., 1998; Wood, Avellar, & Goesling, 2007). The second explanation, termed the causation hypothesis, argues that marriage itself confers social and economic benefits that protect health (Johnson, Backlund, Sorlie, & Loveless, 2000; Waite, 2000). As one of the fundamental institutions in human society, marriage constitutes an important pathway of social integration, social control, and social role attainment (Rendall, Weden, Favreault, & Waldron, 2011). Besides social support, marriage can protect health by reducing inflammation and increasing not only serotonin release to elevate moods but also encouragement to engage in healthy behaviors (Duncan, Wilkerson, & England, 2006; Meyler, Stimpson, & Peek, 2007; Robles & Kiecolt-Glaser, 2003; Thoits, 2011). Economic benefits of marriage include pooled assets, increased efficiency at home through specialization, economies of scale, access to spousal health insurance, and shared household labor (Becker, 2009; Bernstein, 2008; Stimpson, Wilson, & Peek, 2012; Vespa & Painter, 2011). It was argued that some of these social and economic benefits are uniquely associated with marriage and usually cannot be readily obtained from other types of domestic relationships, such as cohabitation (Waite, 2000). The third explanation lies in the stress model in accounting for marital advantages in health, which claims that strains associated with marital dissolution compromise health of the divorced, the separated, and the widowed, resulting in differences in health status between the married and the unmarried (Liu & Umberson, 2008; Williams & Umberson, 2004).
Since health selection before marriage and protection by marriage itself can both result in health and mortality disparities across marital status categories, it becomes challenging to disentangle the two effects from each other and infer which contributes more to the health advantages associated with marriage. This typically requires large-sample longitudinal data with information on premarital health, as well as detailed health records associated with marital statuses at the baseline and afterward. Previous studies have suggested that marriage per se or marital protection at least causes some of the higher levels of well-being for those married (Goldman, Korenman, & Weinstein, 1995; Marks & Lambert, 1998; McLanahan & Sandefur, 1994; Murray, 2000; Waite, 2000; Waldron, Hughes, & Brooks, 1996). It is the intention of this study to assess the protective effect of marriage and how racial differences in marriage rates have contributed to racial disparities in mortality among middle-aged and older males.
Method
Data: The Health and Retirement Study
The Health and Retirement Study (HRS) is an ongoing longitudinal study funded by the National Institute on Aging that collects information on demographics, health, disabilities, health behaviors, health care, employment, housing, assets, and other retirement-related factors, as well as changes in these profiles over time. To ensure its representativeness, the HRS utilizes a national-area probability sample of households in the contiguous United States, with oversamples of Blacks and Hispanics. Institutionalized persons are excluded from the survey population (Heeringa & Connor, 1995). The first wave of data collection started in 1992, soliciting information from 9,601 respondents who were between 51 and 61 years old. The response rate was 81.6% (Kapteyn, Michaud, Smith, & Van Soest, 2006).
The longitudinal design of the HRS allows for the merge of the 1992 baseline data with the 2010 tracker and exit file for information on vital status and its timing. This study focuses on the relationship between marital status at the baseline and subsequent mortality among White and African American males. The working sample in this study includes 3,065 White males and 653 African American males who were between the ages of 51 and 61 years in 1992 and who were followed through 2010 with complete information on vital status and its timing.
Measures
The working HRS sample in this study selected only those who identified with “White/Caucasian” or “Black/African American” in the racial and ethnic categories listed. Mortality was measured during an 18-year period from 1992 to 2010 in the HRS sample. Respondents in the 1992 baseline were followed every other year for updated information. By the year of 2010, 26.7% of the baseline sample died (passive attrition), and 8.7% were lost for follow-up (active attrition). A comparison between those remaining in the sample and those lost due to active attrition suggested that the two groups were very similar to each other in terms of health status, household income, assets, and labor market status at the 1992 baseline (Cao & Hill, 2005). Records on mortality and its timing can be verified by linking mortality records in the HRS to the National Death Index for more detailed information, such as places and causes of deaths.
Marital status at the baseline is an important explanatory variable used to predict racial disparities in mortality. The initial coding for marital status in the HRS includes six categories: married, partner, separated, divorced, widowed, and never married. These categories were collapsed into two groups: married and unmarried. An important consideration in this recoding is to ensure enough cases in each marital status category after the racial breakdown.
Information from the HRS allows us to assess the protective effect of marriage against mortality net of the effect of marital selection in premarital health and socioeconomic status (SES). Four variables were used to characterize premarital health and SES: height, respondent’s years of education, father’s years of education, and mother’s years of education. Adulthood height—as a proxy for net intake of nutrition during growing years (Fogel, 1993; Riley, 1994)—has been widely used in the life course approach to health and mortality disparities later in life. The three variables on education can help us capture differences in premarital SES and family background, which in turn might influence the chance for respondents to get married.
This study used HRS baseline data to assess differences between the married and the unmarried among both White and African American males in terms of annual household income, health insurance coverage, health behaviors (e.g., smoking, frequency of alcohol drink, physical exercises), functional disability, and self-rated health. Household income was calculated by adding income from all sources, including salary and wages, dividends, rent, interests, and other sources, and was categorized into four levels: $20,000 or less, $20,001 to $40,000, $40,001 to $65,000, and more than $65,000.
Analysis
The first step in the analysis involves the use of a t test or chi-square test to assess if there are significant differences in selected variables between the married and unmarried among African American and White men in the sample. This was followed by our use of the life table method (Gehan, 1975) to estimate survival curves during the follow-up period. Cox proportional hazard (CPH) models (Cox & Oakes, 1984) were then used to assess racial disparities in risk of mortality and to evaluate the importance of marital status in explaining racial disparities in risk of mortality. These nested models allow for a test of the sensitivity of the observed racial disparities in mortality to the incorporation of additional variables. Mathematically, the CPH modeling can be expressed as follows:

An important assumption of the CPH analysis is the proportionality of hazard—that is, the effect of changing values for a certain explanatory variable on the hazard rate is constant, independent of time. This assumption was tested for all the explanatory variables in the CPH models by use of the sthphest command in STATA, a test that relates the Schoenfeld residuals to time. The test results indicate that the proportionality assumption holds for the explanatory variables used in the CPH analysis.
Results
Comparison Between the Married and the Unmarried Among White and African American Men in the HRS
Marriage rates at the HRS baseline were much lower among African American men than among White men. Of the African American men in the sample, 64.2% were married in 1992 (n = 419 of 653), as compared to 84.8% among White men (n = 2,600 of 3,065). The first step was to assess if there exists significant differences between the married and the unmarried in terms of our selected variables on SES, health insurance, health behaviors, and health in either of the racial groups at the 1992 baseline (Table 1). The second part of analysis in this section assessed if some of the differences in selected variables by marital status were significant in one racial group but not the other. Among African American men, being married was associated with a higher level of education, but this difference was not observed among White men in the sample.
A Description of Males in the Health and Retirement Study Sample in 1992 by Race and Marital Status.
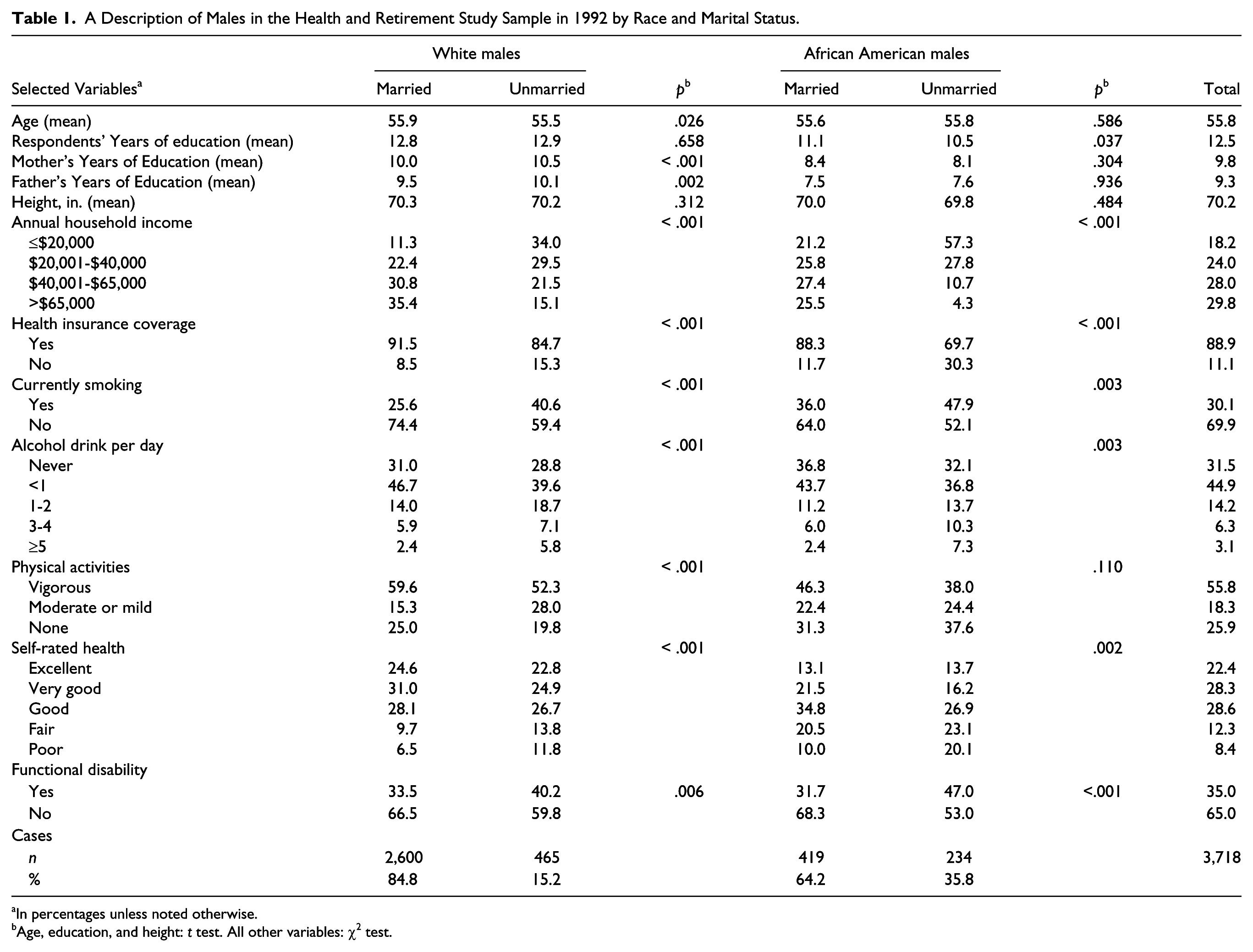
In percentages unless noted otherwise.
Age, education, and height: t test. All other variables: χ2 test.
One of the most significant differences between the married and the unmarried men lies in annual household income and health insurance coverage. In both racial groups, being married was associated with a substantially higher level of household income. Related to this difference was a corresponding difference in health insurance coverage: in both racial groups, married male respondents in the HRS were more likely than their unmarried counterparts to report health insurance coverage. Also note that the differences in income and health insurance by marital status seem to be more pronounced among African American males than among White males. For instance, 11.3% (n = 294 of 2,600) of married White men reported their annual household income to be $20,000 or less, as compared to 34% (n = 158 of 465) among unmarried White males. The corresponding percentages among African American men were 21.2% (89 of 419) and 57.3% (134 of 234), respectively.
Being married was associated with a healthier lifestyle in both racial groups. Relative to unmarried men, married men were less likely to smoke and to drink alcohol five or more times each day. Married men were also more likely to partake in vigorous exercise. An exception is that married White men were more likely to report having no physical activities as compared to their unmarried counterparts. This was different among African American men, where being married was associated with a lower chance of physical inactivity.
Married men were also healthier than unmarried males at the HRS baseline. Close to 12% (n = 55 of 465) of unmarried White men rated their health poor, as compared to 6.5% (n = 169 of 2,600) among married White men. An even more substantial gap can be observed among African American men. Among 419 married African American men in the sample, 10% reported poor health, as compared to 20.1% among unmarried African Americans (n = 234). In terms of functional disability, the prevalence rate was 47% (n = 110 of 234) among unmarried African American men and 31.7% (n = 133 of 419) among married African American men. A similar association, though to a lesser extent, can also be observed among White men.
Marital Status and Mortality Among White and African American Men in the HRS
The survival curves in Figure 2 reveal substantial disparities in mortality by race and marital status. Within either marital status category, White men had survival rates higher than those of their African American counterparts. In either racial group, being married, relative to being unmarried, was associated with lower mortality. This association, however, turned out to be more pronounced among White men than among African American men; 68.4% of White men (n = 1,778 of 2,600) who were married in 1992 survived to 2010, as compared 52.6% among unmarried White men (n = 245 of 465). The corresponding percentages among African American men were 57% (n = 239 of 419) and 46.2% (n = 108 of 234), respectively. Despite overall racial differences in mortality, married African American men had a lower mortality rate during the 18-year follow-up than did unmarried White men.

Mortality by Race and Marital Status Among Males in the HRS.
The marriage-mortality association as revealed in Figure 2 was then examined in a multivariate framework under different model specifications (Table 2). Results based on Model 1 suggest that when only the effect of age is incorporated into the analysis, the elevated risk of mortality for African American men, relative to White men, is 61% (odds ratio [OR] = 1.61; p < .001). On the basis of Model 1, four variables were added in Model 2 to assess the effect of marital selection in premarital SES and health on mortality. After controlling for the effect of age, respondents’ education, parents’ education, and height, the mortality risk for African American men becomes 38% higher than that for White men (OR = 1.38; p < .001), a substantial reduction from the original 61% in Model 1.
Marital Status at Baseline and Racial Disparities in Risk of Mortality During 1992-2010 Among Males in the Health and Retirement Study (N = 3,718).
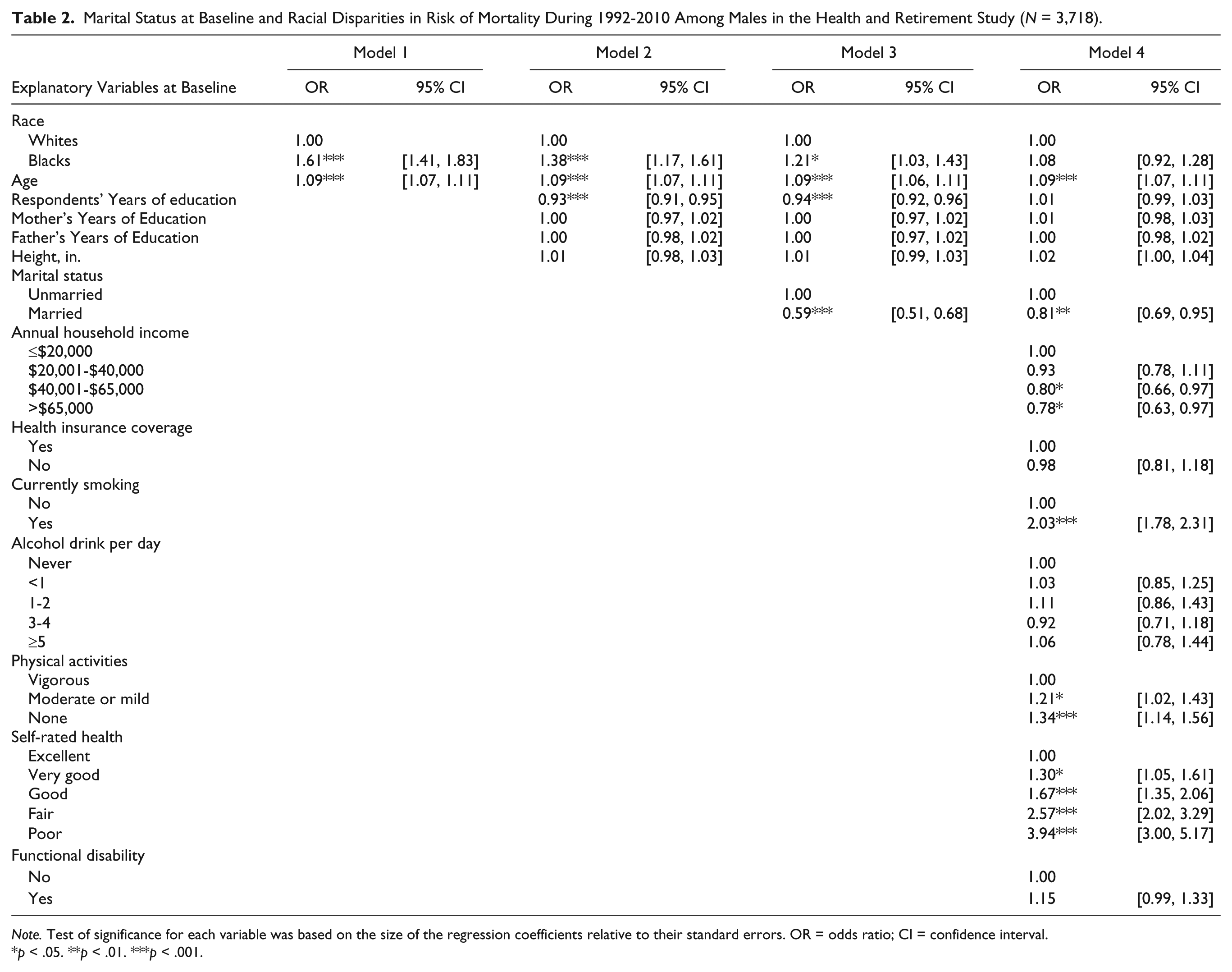
Note. Test of significance for each variable was based on the size of the regression coefficients relative to their standard errors. OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
The only difference between Models 3 and 2 is that marital status was added as a new variable in Model 3. With this change, the elevated risk of mortality associated with African American men, relative to White men, became further reduced to 21% (OR = 1.21; p < .05). After controlling for all selected explanatory variables in Model 3, the mortality risk for married men is 41% less than that for unmarried men (OR = 0.59; p < .001).
A comparison between Models 2 and 3 in terms of racial differences in mortality risk allows us to infer the importance of marriage in explaining mortality disparities between White and African American men in the HRS. Based on the point estimates, differences in marital status between the two groups contributed to 17% (1.38 − 1.21) of the initial gap of 61%. This means that, after adjusting for the effect of selected variables characterizing premarital SES and health, differences in marital status between White and African American men explained 28% (0.17/0.61) of the mortality gap.
Model 4 is the full model where additional variables on household income, health insurance, smoking, alcohol drink, physical activities, self-rated health, and functional disabilities have all been incorporated into the analysis. Racial differences in mortality are no longer statistically significant (OR = 1.08; p > .05). Being married is still associated with lower risk of mortality (OR = 0.81, p < .01). Higher household income, more physical activities, and better self-rated health were also associated with lower risk of mortality, whereas men who were smoking at the baseline were associated with higher risk of mortality than those otherwise.
A notable change between Models 3 and 4 is that the protective effect of marriage against mortality becomes substantially smaller and less significant in Model 4. Since some of the protective effects of marriage could have been mediated through income, baseline health, and health behaviors, the observed effect associated with marriage can be mitigated once these additional variables have been taken into analysis.
Limitations of the Study
Several limitations of this study are noteworthy. First, the number of variables in the HRS that can be used to characterize premarital SES and health is small, which has somewhat restricted inference of the effect of martial selection in premarital SES and health on the overall mortality advantages associated with marriage. While adulthood height has been used as a proxy of nutritional intake during years of growth, it provides little clue about premarital disease history. Second, in consideration of the relatively modest sample size of African Americans in the HRS, marital status was categorized only into “married” versus “unmarried,” without differentiating “unmarried” into more detailed categories such as divorce, widowed, never married, and so forth. While this coding strategy helped to simplify our analysis, it prevented us from having a more detailed look at marital status and assessing how racial differences in detailed marital status categories contributed to their differences in mortality. Finally, this study used information on marital status at only the 1992 baseline without considering changes in marital status over time and if these changes have contributed to the observed mortality disparities between White and African American men. Despite these limitations, this study represents a rare effort in assessing the contribution of racial divergence in marriage rates to corresponding disparities in mortality among a nationally representative sample of males aged 51 to 61 years at baseline.
Discussion
The 20th century witnessed a historical retreat from traditional marriage in the United States. This retreat, however, has been far more severe among African American men than among White men. Given the well-established association between marriage and health, such a divergence in marriage between White and African American men can have profound implications to health and mortality disparities between the two groups. While a substantial body of literature has focused on changes in marriage and their contributing factors, so far little attention has been paid to how these trends have contributed to racial disparities in health and mortality. Based on nationally representative longitudinal data from the HRS, this study assessed the importance of the racial gap in marriage rates in explaining racial disparities in risk of mortality among middle-aged and older men. The rich information from the HRS allows for an analysis of the relative importance of marital selection versus marital protection in accounting for the mortality advantages associated with marriage.
Findings from this study reveal a substantial divide in economic well-being, health behaviors, and health by marital status among both White and African American men. In each group, being married was associated with significant advantages in household income, health behaviors, and self-rated health. Furthermore, these advantages associated with marriage at the baseline got translated into better survival chance for married men during the 1992-2010 follow-up. Both marital selection and marital protection were relevant in explaining the mortality advantages associated with marriage. Our findings suggest that the protective effect of marriage still holds after taking into consideration the effect of selected variables on premarital SES and health, which reinforces marital protection, or the causation hypothesis (Johnson et al., 2000; Murray, 2000; Waite, 2000).
One of the most important findings of this study is that racial differences in marriage rates have contributed to corresponding differences in mortality risk among middle-aged and older males. About 28% of the racial gap in mortality among males in the sample can be explained by racial differences in baseline marital status after adjusting for the effect of selected variables on marital selection in premarital health and SES. This literally means that had the marriage rate among African American males been the same as that among White males, the observed gap in mortality risk between the two groups could have been reduced by 28%.
Such a finding points to the need of addressing the historically low rates of marriage among African Americans as one of the potential ways of reducing racial disparities in health and mortality. The retreat from marriage among African Americans does not necessarily mean that marriage is no longer valued by the majority of African Americans; on the contrary, there is evidence that a more important barrier to marriage among African Americans would be the mismatch between marital aspirations and the lack of social and financial readiness for marriage. Based on data from the Fragile Families and Child Wellbeing Study, one study examined why low-income unmarried parents who said that they planned to marry at the time their child was born did not follow through on their plans. The findings suggested that most of the discrepancy resulted from parents’ perceived social and economic barriers to marriage. Specifically, unmarried parents have a long list of financial and relationship prerequisites that they believe must be met for them to wed (Gibson-Davis, Edin, & McLanahan, 2005). These findings were also confirmed by a review of research on social and economic barriers to marriage among low-income Americans, which suggested that disadvantaged men and women highly value marriage but believe that they are currently unable to meet the high standards of relationship quality and financial stability necessary to sustain a marriage and avoid divorce (Edin & Reed, 2005). It was further argued that because disadvantaged men and women view some degree of financial stability as a prerequisite for marriage, policy makers must address the instability and low pay of the jobs that such men and women typically hold, as well as devise ways to promote home ownership and other asset development to encourage marriage.
The economic and financial barriers to marriage have not only reduced chance of marriage among economically disadvantaged African Americans but also discouraged marriage among better-off African Americans. Today, middle-class African American women are among the most unmarried groups in the United States (Banks, 2011). The substantial gap in educational attainment between African American men and women has negatively affected marital compatibility between the two groups. According to Banks (2011), for each African American man with a bachelor degree, there are two African American women with the same level of education. This achievement gap means that for many well-educated African American women who would like to get married, they might have to either marry African American men who are not as well educated or marry out of their race to other males with similar or better education. In this sense, policy formulations and implementations seeking to improve educational attainment among African American males would be important to revive marriage among African Americans.
Another significant barrier to marriage among African American males lies in the exceedingly high rates of incarceration that they have been exposed to. As a group, African American males are six times more likely than White males to be incarcerated and 2.5 times more likely than Hispanic males (U.S. Bureau of Justice Statistics, 2012). While incarceration per se poses a direct threat to mental and physical health, some of the strongest negative effects of incarceration on health will not manifest until after release from prison. One of the most significant struggles confronted by African American inmates is their reintegration into society after release (Schnittker, Massoglia, & Uggen, 2011). Systematic interventions would require not only reducing crime rates but also establishing postrelease programs that facilitate the reintegration of former inmates into their family and local community.
In a free society, the decision of whether to marry or not, as well as whom and when, is usually a personal issue. What has been demonstrated in this study is that such a personal decision, when aggregated to the population level, can have a profound impact on health disparities. As society becomes more plural and tolerant to alternative modes of family formation, people are no longer compelled to marry or stay married as they used to be. From the perspective of reducing health disparities, an understanding of the statistical aspect of marriage may prove valuable as people ponder on their personal relationships. For that purpose, premarital educational programs on relationship and marriage will not only help people make informed decisions but might also facilitate reducing racial disparities in health and mortality. On the basis of a comprehensive meta-analytic review of premarital programs aiming to reduce marital distress and dissolution, Carroll and Doherty (2003) reported that premarital prevention programs are generally effective in producing immediate and short-term gains in interpersonal skills and overall relationship quality and that these improvements are significantly better among dating or engaged couples who participated in the programs than those otherwise. However, as the authors pointed out, most literature on the effectiveness of premarital prevention is based almost exclusively on young European American middle-class couples who are marrying for the first time. An important step forward would be to tailor extant programs to meet the needs of diverse groups of people who would benefit from these programs. According to findings from our study, one of the priority groups should be African Americans, who are simultaneously the most unmarried and the most disadvantaged when it comes to mortality disparities in the United States.
Based on information on marital status at the 1992 baseline of the HRS, the present study adopted a static approach to assessing the importance of marriage in explaining racial disparities in mortality. A worthy step for future research is to longitudinally assess how changes in marital status affect health on an individual basis and whether the effect differs significantly across racial groups. For example, marital dissolutions as a result of divorce or spousal death could have a differential impact on health and well-being across racial groups owing to racial differences in other confounding or buffering factors, such as economic resources, social support, welfare policies, and so forth. Understanding the dynamic linkages between marital status and health would be important for future policy interventions that seek to reduce racial disparities in health and mortality through promoting marriage among African Americans.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.