
Abstract
The benefit of routine prostate cancer screening is currently under debate; however, many experts recommend that men with elevated risk for the disease discuss the potential risks and benefits of screening with their health care team. Psychological factors have been negatively associated with preventive health behaviors such as cancer screenings. The purpose of this study was to investigate the impact of depressive and trauma-related symptoms on prostate cancer screening behaviors and relevant health care perceptions among a sample of U.S. military veterans, as veterans are at higher risk for prostate cancer, depression, and posttraumatic stress disorder than the general population. Participants (n = 350) were a national sample of predominantly Caucasian (84.6%) male U.S. military veterans (60.5 years ± 8.9) who completed an online questionnaire regarding past prostate cancer screening engagement, as well as validated measures of depression, posttraumatic stress disorder, and perceived barriers and benefits to prostate cancer screening. Results indicate that greater depressive symptoms, trauma-related symptoms, and perceived barriers were associated with lower rates of past prostate cancer screening among this veteran sample and that greater depressive and trauma-related symptoms were associated with greater perceived barriers to prostate cancer screening. As prostate cancer screening recommendations continue to evolve, it is important for health care providers not only to discuss pros and cons of screening with high risk men but also to consider the impact of psychological distress on the decision-making process.
Prostate cancer is the second most common form of cancer in the United States, with an estimated incidence of 241,740 new diagnoses in 2012 (American Cancer Society, 2012a) or approximately 25% of all male cancer diagnoses (Jemal et al., 2009). Data from the Veterans Affairs (VA) Central Cancer Registry indicate that the incidence of prostate cancer is higher among veterans receiving care through the VA Healthcare System, accounting for approximately 33% of all male cancer diagnoses (Zullig et al., 2012). This difference may be due to factors such as increased age of veterans who receive care through the VA (as compared to the general population) or the presence of an additional risk factor—exposure to Agent Orange (AO), an herbicide used in Vietnam. Although many studies have identified a significant association between incidence of prostate cancer and AO exposure in Vietnam Veterans (Akhtar, Garabrant, Ketchum, & Michalek, 2004; Chamie, de Vere White, Lee, Ok, & Ellison, 2008), this finding has not been universal (Pavuk, Michalek, & Ketchum, 2006). Others have reported that AO exposure is associated with a more aggressive form of prostate cancer once the diagnosis has been made (Ansbaugh, Shannon, Mori, Farris, & Garzotto, 2013; Li et al., 2013; Shah et al., 2009). The Department of VA recognizes AO exposure as a risk factor and encourages veterans with prostate cancer exposed to AO to apply for disability compensation and VA health care benefits.
A diagnosis of prostate cancer and associated treatment can have pronounced implications for health-related quality of life; physical, emotional, and social functioning; and mortality (Eton & Lepore, 2002; Torvinen et al., 2013). The introduction of the prostate-specific antigen (PSA) blood test in the 1980s to screen for prostate cancer led to a significant increase in overall prostate cancer diagnoses, particularly early-stage prostate cancer (Grossfeld & Carroll, 2001). Many question the benefits of routine screening in the absence of symptoms and/or identified risk factors, given the relatively slow growing nature of this type of cancer and long-term side effects of treatment. Current research remains equivocal, with some studies finding no decreased risk of mortality associated with prostate cancer screening (e.g., Andriole et al., 2009), whereas others have reported a significant reduction in risk of death from prostate cancer (e.g., Schroder et al., 2012) and an estimated threefold reduction in metastatic cases of prostate cancer as a result of screening (Scosyrev, Wu, Mohile, & Messing, 2012).
Recommendations about prostate cancer screening vary and have recently evolved, given the questionable decrease in mortality after treatment, particularly when weighed against the potential harms associated with treatment (e.g., urinary incontinence, sexual difficulties, etc.). The U.S. Preventive Services Task Force now recommends against PSA screening in all men (U.S. Preventative Services Task Force, 2012), whereas several other prominent organizations, including the American Cancer Society (American Cancer Society, 2012b), the American Society of Clinical Oncology (Basch et al., 2012), the American College of Physicians (Qaseem, Barry, Denberg, Owens, & Shekelle, 2013), and the American College of Preventive Medicine (Lim & Sherin, 2008) recommend a process of shared decision making between the patient and physician that includes consideration of life expectancy and general health, along with the risks, benefits, and personal values of the individual patient. The presence of known prostate cancer risk factors, such as African American race and family history of prostate cancer, should be taken into account in the decision to undergo prostate cancer screening (American Cancer Society, 2012b). The prevalence of prostate cancer in African American men is 56% to 312% higher than that of other racial groups in the United States (Howlader et al., 2010), and the incidence of prostate cancer among men with blood relatives previously diagnosed with prostate cancer is higher than the incidence among those men without a family history, depending on the number and degree of relatives affected (Kicinski, Vangronsveld, & Nawrot, 2011). As mentioned above, exposure to AO can also be considered as an additional risk factor for veterans. As information accumulates about the risks and benefits of prostate cancer screening, men, particularly those at elevated risk, should engage in shared decision making with providers about this important issue. 1
Rates of depressive and trauma symptoms are significantly higher among veterans (Hoge et al., 2004) than among the general population (Centers for Disease Control and Prevention, 2010; Kessler, Chiu, Demler, Merikangas, & Walters, 2005). Little is known about the impact of depression and/or posttraumatic stress disorder (PTSD) on prostate cancer screening. The authors identified only one study examining the impact of distress on screening; in their article, Buckley, Mozley, Bedard, Dewulf, and Greif (2004) reported that veterans with PTSD (depressive symptoms were not assessed) were less likely to engage in prostate cancer screening. No known studies document the effect of depression or depressive symptoms on prostate cancer screening. The literature, however, does demonstrate that psychological factors do affect other preventative health screenings. Depressive symptoms have been associated with lower rates of screening for breast (Aggarwal et al., 2008; Ludman et al., 2010; Price et al., 2010; Vigod, Kurdyak, Stewart, Gnam, & Goering, 2011), cervical (Kaida, Colman, & Janssen, 2008), and colorectal cancer (Kodl et al., 2010), whereas veterans with PTSD engage in preventive health behaviors, such as colorectal cancer screening and regular exercise, significantly below health care guidelines (Buckley et al., 2004; Zen, Whooley, Zhao, & Cohen, 2012). Furthermore, depression and PTSD are associated with both medication noncompliance and missed medical appointments, other indicators of disengagement in one’s health care (Osterberg & Blaschke, 2005; Spoont, Sayer, & Nelson, 2005).
The purpose of this study was to investigate the relationship between depressive and trauma symptoms on prostate cancer screening behavior and relevant health care perceptions among U.S. military veterans. This population is of particular interest given the higher rates of depression and trauma and because Vietnam-era veterans may be at increased risk for prostate cancer due to AO exposure. This combination of increased risk and decreased engagement in preventive health behaviors suggests that veterans with depressive and/or trauma-related symptoms may be particularly vulnerable to delayed detection of prostate cancer.
Hypotheses are guided by the health belief model, a well-researched framework that explains and predicts health behaviors. Briefly, the health belief model suggests that engagement in health services is influenced by a combination of factors including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy (Rosenstock, Strecher, & Becker, 1988). Modifying factors, including psychological status, can affect the above-mentioned six factors, influencing behavior, as well as perceived benefits and barriers. Therefore, it was hypothesized that veterans with greater depressive and trauma symptoms would be less likely to engage in prostate cancer screening and would report more barriers to prostate cancer screening and fewer perceived benefits. In addition, it was hypothesized that veterans without a history of prostate cancer screening would perceive fewer benefits and greater barriers to screening.
Method
Participants
Participants were 460 male veterans with access to the Internet who responded to a solicitation to participate in an anonymous, online survey. Exclusion criteria included being female, nonveteran, under the age of 40, or having a history of prostate cancer; 56 participants were deemed ineligible because of these criteria. An additional 54 participants were excluded due to missing data from primary depression and PTSD outcome measures, resulting in a final sample size of 350.
Participants ranged in age from 41 to 89 years (M = 60.5; SD = 8.9) and lived in 47 states across the United States. The sample was primarily Caucasian (n = 296, 84.6%), married/partnered (n = 245, 70%), and well-educated (n = 279, nearly 80% with at least some college or vocational school). Regarding access to health care, nearly 87% (n = 303) of participants reported having a regular doctor, either through private insurance or through the VA hospital system; nearly 59% (n = 205) of participants had private (non-Veterans Health Administration) insurance; and 54% (n = 189) of participants had both a regular doctor and private insurance (see Table 1).
Demographics.

Note. VA = Veterans Affairs; PSA = prostate-specific antigen; DRE = digital rectal exam.
Measures
Demographic variables (age, marital status, occupation, income, education, race, family history of prostate cancer, military history, exposure to AO, medical history, information about health care/insurance status, geographic location, and access to the Internet) were assessed via a self-report questionnaire.
Prostate Cancer Screening Behavior
Participants were asked if and when they had a digital rectal exam (DRE) and a PSA test. Both the exam and the test were briefly described in the questionnaire (e.g., “A Digital Rectal Examination is when the prostate is felt by a health professional by inserting a gloved finger into the rectum and gently pressing on the prostate to feel for lumps” and “A Prostate Specific Antigen (PSA) Test is where blood is drawn and tested for a protein linked to the prostate gland”). These questions have been asked in studies of prostate cancer screening by others (Bloom, Stewart, Oakley-Girvans, Banks, & Chang, 2006; Myers et al., 2000).
Patient Health Questionnaire–8 (PHQ-8; Kroenke & Spitzer, 2002)
This is an 8-item measure of depressive symptomatology designed to be used with a general (nonpsychiatric) population and is based on 8 of the 9 criteria for DSM-IV diagnosis of major depressive disorder. Participants were asked to rate on a scale from 0 (not at all) to 3 (nearly every day) how often they were bothered by each symptom over the past 2 weeks. Summed responses yield a total score, and higher scores signify greater depressive symptoms. A PHQ-8 score ≥10 is a suggested cutoff that may be indicative of a depressive disorder or the presence of depressive symptoms, although authors recommend that confounding factors (i.e., bereavement, substance abuse, or medical causes) be further investigated (Kroenke et al., 2009). For the current study, Cronbach’s coefficient alpha was .95.
PTSD Checklist–Civilian Version (PCL; Weathers, Litz, Herman, Huska, & Keane, 1993)
The PCL is a self-report measure consisting of 17 items that parallel the DSM-IV posttraumatic stress disorder criteria. Participants are asked to rate on a scale from 1 (not at all) to 5 (extremely) the degree to which they have been bothered by each symptom in the past month. Summed responses yield a total score, and higher scores signify greater PTSD symptoms. The PCL has excellent test–retest reliability, r = .96 (Weathers et al., 1993) and concurrent validity compared with structured clinical interview of PTSD, r = .79 to .93 (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996; Keen, Kutter, Niles, & Krinsley, 2008). A cutoff score of between 50 and 60 is recommended depending on the population sampled (Keen et al., 2008; Weathers et al., 1993). Cronbach’s coefficient alpha for this study was .97.
Perceived Barriers of Prostate Cancer Screening Scale (Barriers Scale; Weinrich, Reynolds, Tingen, & Starr, 2000)
The Barriers Scale is a 15-item measure consisting of items that may interfere with screening behavior. Respondents are asked to rate each potential barrier (i.e., costs too much, no insurance coverage, fear of examination, etc.) on a scale from 1 (not at all) to 5 (extremely) to indicate the degree to which each barrier applies to them. Summed responses yield a total score, and higher scores signify more perceived barriers to prostate cancer screening. Total scores on this measure predicted participation in free prostate cancer screenings in the study by Weinrich et al. (2000). This scale has demonstrated internal consistency (α= .90; Weinrich et al., 2000). Cronbach’s coefficient alpha for this study was .89.
Perceived Benefits of Prostate Cancer Screening Scale (Benefits Scale; Tingen, Weinrich, Heydt, Boyd, & Weinrich, 1998)
The Benefits Scale is a 7-item measure of patient’s beliefs of how prostate cancer screening may benefit their health. Respondents are asked to rate each statement (e.g., “A prostate check up could help find cancer early, a prostate check up could help me live longer,” etc.) on a 1 (extremely unlikely) to 5 (extremely likely) scale to indicate how likely they think each benefit will be as a result of prostate cancer screening. Summed responses yield a total score, and higher scores signify more perceived benefits to prostate cancer screening. This scale is internally consistent (α= .90; Tingen et al., 1998). Cronbach’s coefficient alpha for this study was .93.
Procedure
All procedures were approved by the institutional review board at the research site. Participation in the proposed investigation was anonymous via a web-based survey hosted by Psychdata.com, a company that specializes in secure online data collection for the social sciences, on a secure server. Participants for the study were recruited through electronic announcements posted on internet listservs and websites for veterans (e.g., MyHealtheVet, a Yahoo! Group called “Veteran’s Issues,” The 11th Cavalry Veterans of Vietnam and Cambodia, etc.). Groups were identified by their expected membership base (i.e., organizations that comprised veterans, racially diverse veterans, African American men, etc.). Of the 29 online resources identified and contacted as options for recruitment, 34% agreed to post information related to the web-based survey. When organizations/groups agreed that the authors could solicit from their membership base, the request for participants was posted on the listservs/websites and consisted of a study description and a URL address linked to the study.
Interested participants self-selected to participate in the study and used their Internet browser to go to the posted URL. Once logged in, they were directed to the informed consent document. The investigation was described as an anonymous examination of veterans’ attitudes toward and knowledge of prostate cancer screening. Following their reading of the informed consent document, participants were directed to select a link at the bottom of the document indicating that they read and understood the informed consent document and agreed to participate. Participants then completed the above-mentioned questionnaires. On completing the electronic survey, participants were directed to a debriefing page with contact information for the investigators. Participants did not receive any incentives for participating in this study.
Data Analysis
Descriptive analyses were used to summarize demographic and clinical characteristics of the sample, including frequency of prostate cancer risk factors and prior screening behavior.
T tests were conducted to compare depressive and PTSD symptoms among veterans with and without past prostate cancer screening. Hierarchical multiple regression was used to test the hypothesis that greater depressive and PTSD symptoms would predict greater perceived barriers to prostate cancer screening and fewer perceived benefits to prostate cancer screening. Regression equations included demographic (age, race, level of education, marital status) and access to care (has a regular doctor, has private health insurance) variables to control for the impact of these variables.
Results
Descriptive statistics revealed that participants reported relatively high rates of past screening for prostate cancer (PSA, 75.7%; DRE, 94.3%), and nearly 60% of participants reported having at least one risk factor for prostate cancer (African American race, one or more blood relatives with a past diagnosis of prostate cancer, and/or AO exposure; Table 1). Questionnaire means indicate moderate depressive and subclinical trauma-related symptoms in the overall sample (Table 2).
Questionnaire Means.
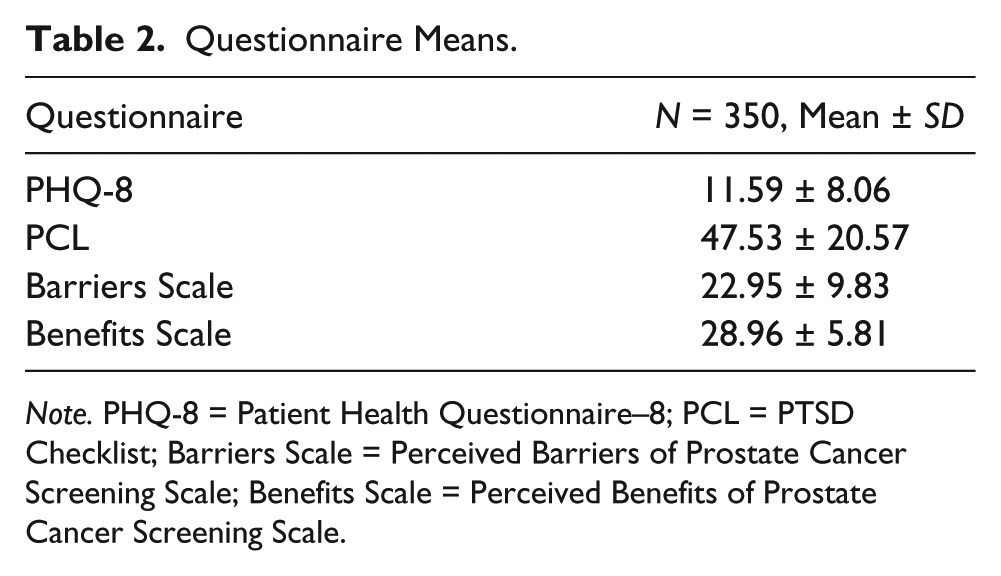
Note. PHQ-8 = Patient Health Questionnaire–8; PCL = PTSD Checklist; Barriers Scale = Perceived Barriers of Prostate Cancer Screening Scale; Benefits Scale = Perceived Benefits of Prostate Cancer Screening Scale.
Univariate t tests revealed that men without a history of DRE reported significantly higher scores on the PHQ-8 (M = 15.9, SD = 8.4), as compared to those who had a past DRE (M = 11.3, SD = 8.0), t(325) = 2.41, p = .02. Similarly, those who had never had a DRE reported significantly higher PCL scores (M = 58.4, SD = 22.4) than those who had a previous DRE (M = 47.0, SD = 20.4, t(345) = 2.30, p = .02. The same pattern was observed for PSA testing, such that men who had never had a PSA test reported significantly higher scores on the PHQ-8 (M = 15.3, SD = 8.4), as compared to those who had a past PSA test (M = 11.0, SD = 7.8), t(284) = 3.06, p = .002. Those who had never had a PSA test reported significantly higher PCL scores (M = 54.3, SD = 21.6) than those who had a previous PSA test (M = 46.3, SD = 20.5), t(300) = 2.22, p = .03. These findings indicate that greater depressive and trauma symptoms are associated with less prostate cancer screening (Figures 1 and 2).
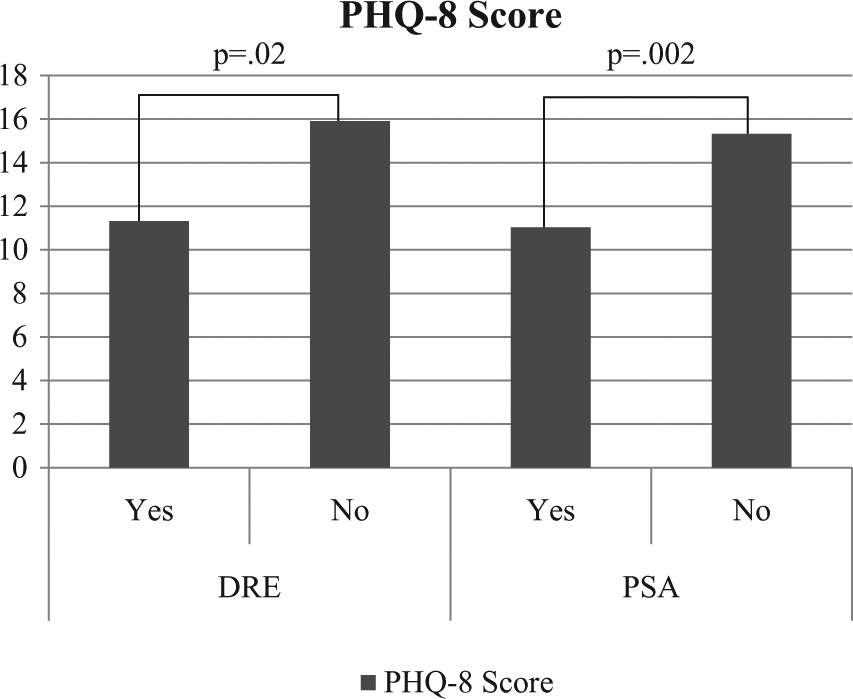
PHQ-8 scores by history of DRE and PSA.

PCL scores by history of DRE and PSA.
Results of additional univariate t tests indicated that participants who had never had a DRE reported significantly higher scores on the Barriers Scale (M = 29.4, SD = 10.1), as compared to those who had a past DRE (M = 22.4, SD = 9.6), t(338) = 3.25, p = .001. Participants who had never had a PSA test also reported significantly higher scores on the Barriers Scale (M = 28.2, SD = 10.9), compared with those who reported a past PSA test (M = 21.7, SD = 9.1), t(296) = 4.05, p < .001; see Figure 3. Scores on the Benefits Scale were not significantly different for participants with or without past prostate cancer screening (DRE: t[357] = .61, p = .61; PSA: t[311] = .76, p = .45), suggesting that perceived barriers are a stronger predictor of prostate cancer screening that benefits.
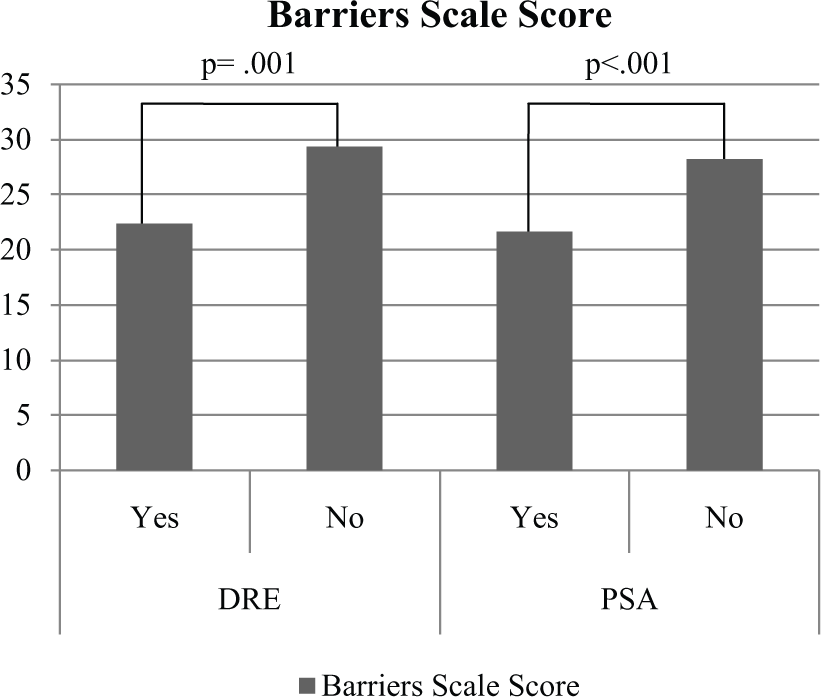
Barriers Scale scores by history of DRE and PSA.
Hierarchical multiple regression analyses indicated that PHQ-8 symptoms predicted scores on the Barriers Scale (r2 = .14, β = .20, t = 3.38, p = .001) but not on the Benefits Scale (r2 = .02, β = −.06, t = −.94, p = .35; Table 3). Similarly, hierarchical multiple regression analyses indicated that the PCL predicted scores on the Barriers Scale (r2 = .14, β = .17, t = 3.09, p = .002) but not on the Benefits Scale (r2 = .02, β = −.013, t = −.22, p = .83; Table 4). Greater depressive and trauma-related symptoms were associated with greater perceived barriers to prostate cancer screening but were not related to level of perceived benefit of prostate cancer screening.
Impact of Depressive Symptoms on Prostate Cancer Screening Perceptions.
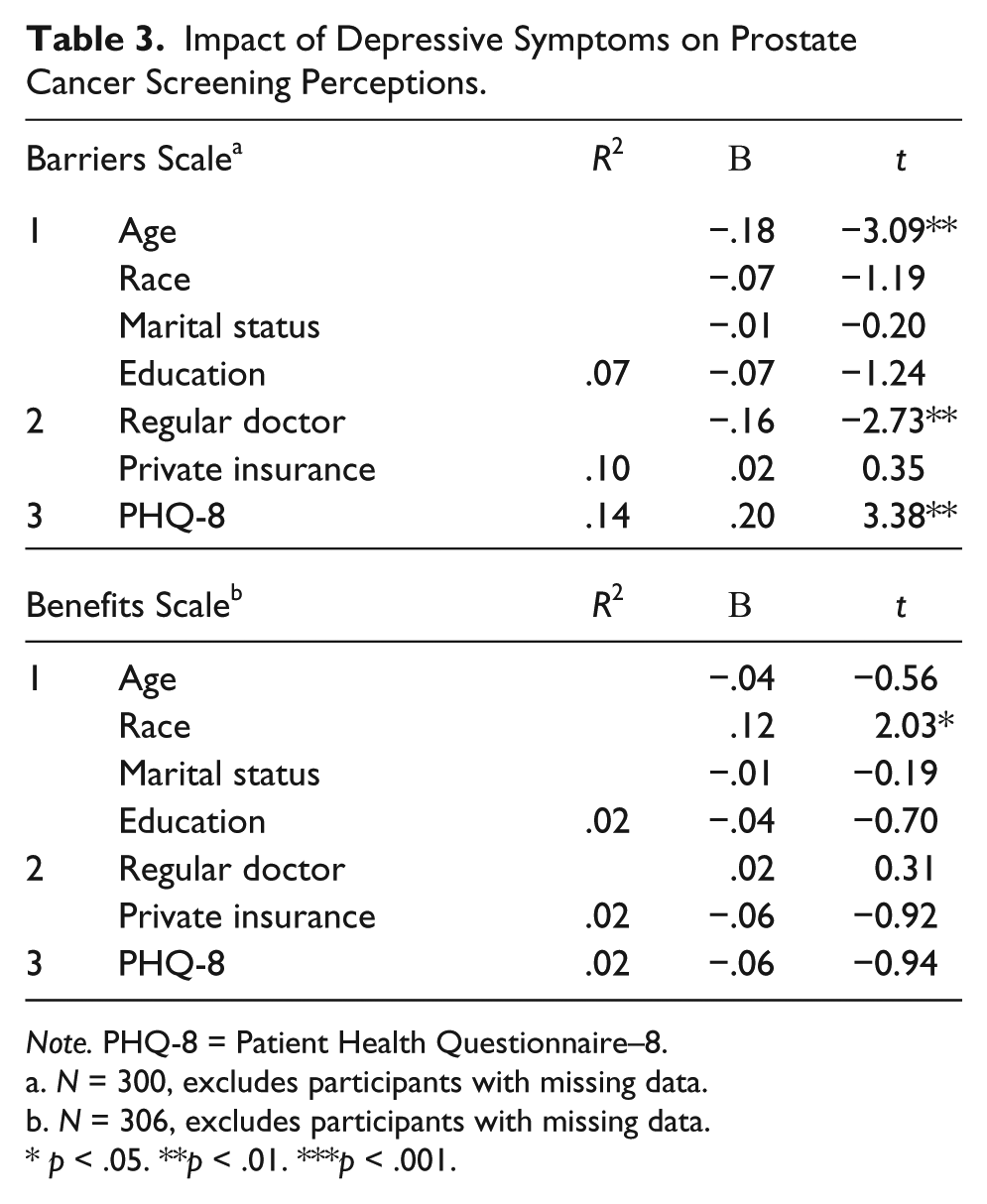
Note. PHQ-8 = Patient Health Questionnaire–8.
N = 300, excludes participants with missing data.
N = 306, excludes participants with missing data.
p < .05. **p < .01. ***p < .001.
Impact of Trauma Symptoms on Prostate Cancer Screening Perceptions.

Note. PTSD = posttraumatic stress disorder; PCL = PTSD Checklist.
N = 313, excludes participants with missing data.
N = 321, excludes participants with missing data.
p < .05. **p < .01. ***p < .001.
Discussion
Results of this study indicate that greater depressive and trauma symptoms are associated with lower rates of past prostate cancer screening among this veteran sample. These results are consistent with prior studies indicating an inverse relationship between depressive symptoms and other types of cancer screenings (e.g., Aggarwal et al., 2008, Ludman et al., 2010; Price et al., 2010) and are the first known findings to document the impact of both depressive and trauma symptoms on prostate cancer screening in military veterans. Results also indicate that a higher degree of perceived barriers to prostate cancer screening is associated with lower rates of past screening. This is consistent with research on the relationship between perceived barriers and other types of cancer screening (Gimeno-Garcia, Quintero, Nicolas-Perez, Parra-Blanco, & Jiminez-Sosa, 2009; James, Campbell, & Hudson, 2002) and suggests that perceived barriers may have affected past prostate cancer screening behavior. In addition, results indicate that greater depressive and trauma-related symptoms are associated with greater perceived barriers to prostate cancer screening, suggesting that veterans with mental health symptoms in this sample may be less likely to seek or follow through with future screenings.
Although controversy exists regarding prostate cancer screening, most believe that screening should be available to men who have reviewed the risks and potential benefits with providers, particularly those with documented prostate cancer risk factors. In the current sample, male veterans who had never been screened reported significantly more depressive and trauma-related symptoms than those who had been screened, and higher levels of distress predicted higher perceived barriers, indicating that psychological distress may be affecting the decision-making process. Given the impact of psychological distress on screening and perception of screening, it is critical that veterans be effectively counseled by providers to make an informed choice about prostate cancer screening, as well as other preventive health behaviors.
Surprisingly, the authors’ results did not demonstrate that depression and trauma-related symptoms were inversely associated with perceived benefits to prostate cancer screening. It may be that historical public health and/or VA initiatives have been effective in informing the public about the benefits of prostate cancer screening, such that psychological distress does not alter those perceptions. On close review, the authors also noted that some items on the Benefits Scale refer to perceived benefits that may be unrealistic to expect from prostate cancer screening (i.e., “A prostate check up could help me live longer,” “A prostate check up could help stop cancer from growing”) and may therefore not be realistic indicators of perceived benefits.
Similarly, the degree of perceived benefits was not associated with past prostate cancer screening behavior. Past research on the relationship between perceived benefits and cancer screening behavior has been equivocal. For example, in the breast cancer screening literature, some studies indicate a positive association between perceived benefits and mammography adherence (Fair, Monahan, Russell, Zhao, & Champion, 2012; Farmer, Reddick, D’Agostino, & Jackson, 2007), whereas other studies have reported no association between these variables (Russell, Perkins, Zollinger, & Champion, 2006). In addition, others have suggested that perceived barriers may have greater impact than perceived benefits on cancer screening behavior (Gimeno-Garcia et al., 2009).
This research examines an understudied, but critical, aspect of men’s health. There are no known studies that have looked at both depression and PTSD symptoms as a correlate of prostate cancer screening with a large, national sample of male veterans, a segment of the population that may be less likely to engage in preventive health care, including recommended screenings. Additionally, this study included AO as an additional veteran-specific risk factor for prostate cancer, a risk factor that is typically not considered when nonveteran agencies review guidelines for screening (Akhtar et al., 2004; Chamie et al., 2008).
Despite these notable strengths, there are several limitations that bear mention. Data presented are cross-sectional, and therefore, causal inferences cannot be made regarding the relationship between current psychological distress and prior screening behavior. Future studies should employ prospective methodologies to examine the relationship between depressive and trauma-related symptoms and chart-verified prostate cancer screening. Related, despite the interrelationships noted between psychological distress, perceived barriers to prostate cancer screening, and screening behavior, the current cross-sectional data were not appropriate for testing mediational models. A future prospective design would allow for testing of mediational models (i.e., perceived barriers to prostate cancer screening as a mediator in the relationship between psychological distress and screening behavior) to more fully elucidate the nature of the interrelationships of these variables. In addition, data from this study were collected between 2009 and 2010, when prostate cancer screening was more likely to be routinely offered at a medical visit; results should therefore be interpreted within that context. Screening guidelines have evolved greatly since data collection and are likely to continue to evolve.
The current findings should also not be generalized to other patient populations, as participants in this study were predominantly Caucasian male veterans who had access to and familiarity with computers and the Internet. Additionally, the vast majority of veterans in this sample (86.6%) had a regular doctor, and at least 40% accessed this survey through My HealtheVet (an online veteran health and wellness website sponsored by the Department of VA). Although a recent national survey of veterans’ use of the internet demonstrated that 54% of their sample of 3,408 veterans had used the Internet, only 29% had accessed the Internet for health-related purposes (McInnes, Gifford, Kazis, & Wagner, 2010). Furthermore, the majority of participants reported past prostate cancer screening. Therefore, these participants may represent a select group of computer-savvy, health care engaged veterans that is not representative of the veteran population at large. Although the authors had hoped to have a sample that was diverse, particularly in terms of racial diversity, the final sample was not diverse or representative. Only 6.3% of participants self-identified as African American; as race is an important risk factor in current prostate cancer screening guidelines, it would be important to replicate this study in the context of a larger African American veteran population, in which analyses of subgroups are possible. All measures were self-report and are not exempt from the problems associated with response bias. Finally, because the participants were anonymous, the authors were unable to verify the veracity of self-reported screening practices.
Though guidelines for prostate cancer screening are under debate and are apt to continue to evolve over the next several years, the current findings demonstrate the importance of attending to psychological symptoms in the context of prostate cancer screening. The current findings highlight the importance of providers attending to the impact of psychological distress on prostate cancer screening (as well as other preventative health behaviors), particularly in those veterans who have several risk factors for this cancer. Currently, VA medical centers conduct regular screenings for depression and PTSD to identify those with elevated distress for referral to mental health treatment. However, VA primary care providers may also benefit from education regarding the potential impact of psychological distress on preventive health care perceptions and behaviors so that they may appropriately tailor their conversations about health care screenings with veterans, particularly those with documented risk factors. In particular, the use of motivational interviewing techniques (Rollnick, Miller, & Butler, 2008) may be beneficial for those veterans who experience real or perceived barriers to screening to arrive at a decision about screening that is in alignment with their expressed values and preferences.
Footnotes
Authors’ Note
Andrea K. Busby, Ph.D. is now with Lifespan Physician Group, Behavioral Medicine Clinical Services, The Miriam Hospital, Providence, RI. Erin W. Ulloa, Ph.D. is now with Behavioral Health Service, Philadelphia VA Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported by a grant from the Veterans Health Administration Rehabilitation, Research, and Development Service (F4120).