
Abstract
No prior research has examined men’s opinions or preferences regarding receiving health education materials related to sexual violence. The objective of the current study was to investigate whether male veteran patients who have experienced military sexual trauma (MST) prefer gender-targeted versus gender-neutral printed health information and whether receipt of this information increased utilization of outpatient mental health services in the following 6-month period. In-person 45-minute interviews were conducted with 20 male veterans receiving health care services at a large Veterans Health Administration facility to evaluate opinions on a gender-targeted and a gender-neutral brochure about MST. An additional 153 veterans received psychoeducational materials through the mail and participated in the completion of a survey as part of a psychoeducational intervention. Our results demonstrate that male veterans prefer gender-targeted information about sexual trauma compared to gender-neutral information. Whereas veterans in the study had clear preferences for gender-targeted materials, receipt of information about MST (whether gender-targeted or gender-neutral) did not increase utilization of mental health care in the 6 months following receipt of these materials. These results demonstrated that materials about sexual trauma are acceptable to men and should be gender-targeted. Further research is needed to examine strategies to increase access to mental health care among male Veterans who have experienced MST.
Keywords
Military sexual trauma (MST)—a Department of Veterans Affairs (VA)–specific term that refers to threatening sexual harassment or sexual assault that occurred during military service (U.S. Code, Title 38 § 1720D)—is associated with a greater burden of mental health and physical health problems among both male and female veterans (Kimerling et al., 2010; Kimerling, Gima, Smith, Street, & Frayne, 2007; Turchik, Pavao, Nazarian, et al., 2012). Universal screening for MST was implemented in VA in 2002, and mandated free treatment for MST-related health issues—MST-related care—was implemented in 1995 (U.S. Department of Veterans Affairs, 2010). MST-related care is defined as any health care visit to treat a health condition that is determined to be “related to MST” by a clinical VA provider and is indicated as such by the provider in the Veteran’s electronic medical record. Among Veterans Health Administration (VHA) users, approximately 20% of women and 1% of men have reported MST (Kimerling et al., 2007). Although women are substantially more likely to report MST compared to men, the actual numbers of male and female VHA users who have experienced MST are similar because the VHA population is predominantly male.
However, despite screening and eligibility to receive free treatment for both male and female veterans, recent research has found that Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) male veterans who reported MST were less likely to use MST-related outpatient mental health services and had lower intensity of use than OEF/OIF female veterans who reported MST (Turchik, Pavao, Hyun, Mark, & Kimerling, 2012). No gender differences in overall mental health utilization were found in the study, only in relation to MST-related care. Similarly, VHA monitoring data for MST-related care indicates that among all VHA users with a history of a positive MST screen, a lower proportion of male Veterans use MST-related mental health care as compared to women (Office of Mental Health Services, 2011). This suggests that the potential gender disparity in use of MST-related mental health care is not limited to the OEF/OIF cohort. Qualitative data suggest that lack of knowledge about MST and MST care, stigma-related concerns (e.g., embarrassment/shame; fear of not being believed), and gender-related issues (e.g., belief that men are less affected than women; provider gender preferences; sexuality/sexual orientation concerns) are potential barriers to care for male veterans (Turchik, McLean, et al., 2013). These results are consistent with the broader, although limited, literature that suggests that concerns about masculinity, traditional gender role expectations, and sexual orientation may be particularly salient for male victims of sexual violence (Davies, 2002; Turchik & Edwards, 2012). Such findings suggest that informational outreach may be needed to increase awareness and access to MST services among men and highlight the importance of gender sensitivity in relation to sexual trauma.
Informational outreach and knowledge enhancement interventions are often used to increase access to care when limited or lack of knowledge has been identified as a barrier; such interventions have been found to be effective across a number of patient populations and issues, including colon cancer screening, posttraumatic stress disorder treatment, and smoking cessation (Lando, Hellerstedt, Pirie, & McGovern, 1992; Manne et al., 2009; Marcus et al., 2005; McFall, Malte, Fontana, & Rosenheck, 2000). Such knowledge enhancement interventions are generally most effective when targeted or tailored to the patient group (Noar, Benac, & Harris, 2007), and tailoring interventions may have the potential to reduce sociodemographic disparities, including gender, in health care (Jerant, Sohler, Fiscella, & Franks, 2011). Given the gender-related issues inherent to sexual trauma and the potential gender-related barriers reported in the qualitative study by Turchik, McLean, et al. (2013), a gender-targeted informational brochure may be preferred by male veterans who have experienced MST compared to a gender-neutral MST brochure that is widely distributed within the VA (MST Support Team, 2008). Gender sensitivity and the ability to take sex and gender differences into account are both important factors in preventing inequalities in health care (Celik, Lagro-Janssen, Widdershoven, & Abma, 2011). For instance, a brochure targeted at men could specifically include information about issues related to masculinity and gender roles that would not be addressed in a gender-neutral brochure.
Research has demonstrated the utility of gender-targeting outreach materials for other health issues such as breast cancer (Iredale, Williams, Brain, France, & Gray, 2007; Thomas, 2010; Williams et al., 2003) and weight and diet management (Simen-Kapeu & Veugelers, 2010). Particularly relevant is the research investigating issues related to breast cancer, which is typically thought of as a “female condition,” and most educational materials focus on women patients. However, research has demonstrated that men with breast cancer, especially younger men, would like more information targeted to men in patient educational materials (Iredale et al., 2007; Williams et al., 2003). Thomas (2010) notes that in conditions such as breast cancer, where there is a marked difference in prevalence among the sexes, it is not adequate to simply change the word “female” to “male” in educational materials, these brochures, leaflets, and other materials “should be sex specific and gender appropriate.” In addition to tailoring patient education, for some issues, interventions may also need to be gender-focused. For instance, research has found both sex and gender differences in smoking behavior, barriers to smoking cessation, and smoking cessation treatment outcomes, and therefore many smoking cessation interventions have been gender-targeted for men and women (Okoli, Torchalla, Oliffe, & Bottorff, 2011; Torchalla et al., 2012).
Gender sensitivity and the examination of gender-related issues have been identified as an important area of focus within both the VA (e.g., Vogt et al., 2001) and the wider health care system (Celik et al., 2011). Given the gender disparity in MST-related care utilization, the current study was designed to address gaps in the literature by developing gender-targeted health information about MST, exploring men’s opinions about the gender-targeted information, and assessing whether receipt of these materials increases utilization of MST-related mental health care among male veterans. Thus, the specific aims of the study were to (a) gather qualitative data from male veterans who have experienced MST in order to design a gender-targeted psychoeducational MST brochure, (b) quantitatively compare men’s ratings of a gender-targeted versus a gender-neutral psychoeducational brochure on MST, and (c) examine the effects of a psychoeducational mail-based pilot intervention on mental health care use and MST-related mental health care use over a 6-month time period following the intervention.
Method
Participants
The sample for this study was identified using VHA administrative data, and a total of 322 veterans met eligibility criteria. Criteria for inclusion in the overall study were being a male veteran, having screened positive for MST at any time during VHA care, having received at least one VHA outpatient encounter (i.e., any primary care, mental health, or day program health care outpatient visit) in FY 2009 or FY 2010 at VA Palo Alto Health Care System, and having not received any MST-related mental health care from VA Palo Alto Health Care System since FY 2006 when VA began tracking MST-related care. Veterans were also excluded from the current study if they were incapacitated (e.g., diagnosis of dementia, evidence of a conservatorship) or their medical diagnoses indicated they were legally blind. Please see Figure 1 for information about the interview and psychoeducational mail-based intervention subsamples.

Flowchart depicting study sample selection and allocation of participants to psychoeducational mail-based pilot intervention.
Interview Subsample
Of the overall eligible 322 Veterans, Veterans were further excluded from the interview subsample if their medical diagnoses indicated a severe hearing impairment or if the veteran lived more than 25 miles from the facility. Of the 322 veterans identified, 99 met eligibility criteria, and 50 veterans were randomly selected to participate in the interview phase of the study and were mailed letters of invitation. A total of 20 male veterans completed valid in-person interviews. The participants were an average age of 62 years, and the majority was White, served in the Army, and served during the Vietnam War era. For more information about the mailing procedures and demographics for this subsample, see Turchik, McLean, et al. (2013).
Psychoeducational Mail-Based Pilot Intervention Subsample
Of the initial eligible sample of 322 men, those who were not contacted during the interview phase of the study were included in the intervention subsample, leaving 272 men. Mailings were sent in subsequent waves to the 272 veterans, with each being sent up to 3 letters of invitation. Fourteen individuals who were invited to participate were later excluded due to having an invalid mailing address (10), being deceased (2), legally blind (1), or having a diagnosis of Alzheimer’s (1). However, of the 258 remaining individuals, 212 individuals responded, while 46 did not. Of those 212, 41 opted out of the study. Of the 171 individuals who opted in, 17 did not complete the survey, and 154 completed the survey (however, one participant’s data were later excluded due to finding out veteran was incarcerated at time of completion), leaving a final sample of 153 completed surveys. See Table 1 for demographics of this final sample. Independent-samples t tests and chi-square analyses were run to assess any differences between those who opted into the study and those who did not and between those who completed the survey and those who did not. No differences were found across age, race/ethnicity, or marital status between these groups (all ps > .05).
Participant Characteristics of Psychoeducational Intervention Sample (N = 153).
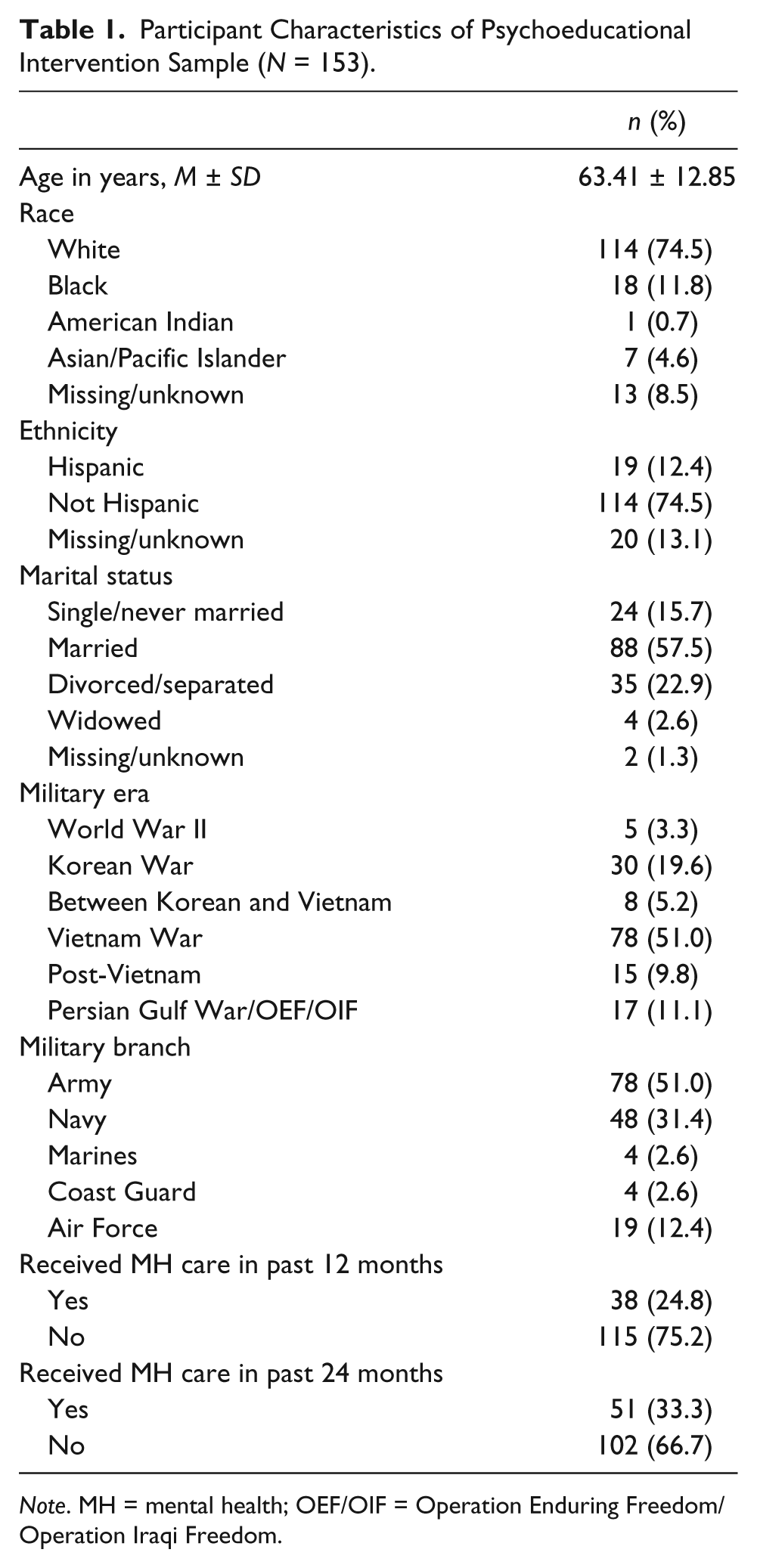
Note. MH = mental health; OEF/OIF = Operation Enduring Freedom/Operation Iraqi Freedom.
Key Archival Database Variables
All key variable data were obtained from VHA’s National Patient Care Database (clinical and administrative data from the electronic medical record of patients who use VHA), unless otherwise noted. Sociodemographic (age, race, ethnicity, marital status) information was obtained from the VHA National Patient Care Database, and military status and branch were obtained from participants’ survey responses.
History of MST was determined by an affirmative response to either of the two items from the national MST screen, which is part of VHA’s electronic clinical reminder and is composed of the following two items:
While you were in the military: (a) Did you receive uninvited and unwanted sexual attention, such as touching, cornering, pressure for sexual favors, or verbal remarks? (b) Did someone ever use force or threat of force to have sexual contact with you against your will?
Use of MST-related care was defined as whether or not the veteran had at least one face-to-face outpatient VHA mental health encounter that was designated as MST-related in the 6 months following receipt of the psychoeducational materials. After each VHA visit with a veteran who has a MST positive screen, clinical care providers must indicate whether the “visit was related to MST” in the electronic medical record. This determination is made by clinical judgment. Mental health care use was defined as whether or not the veteran had at least one face-to-face outpatient VHA mental health encounter (MST related or not) in the 6 months following receipt of the psychoeducational materials.
Procedure
The current study was approved by the local VA Research & Development Office and by Stanford University Institutional Review Board, which serves as the IRB of record for the local VA Medical Center.
Phase 1: Interviews
Each approximately 45-minute in-person semistructured interview consisted of three parts: (a) general demographic, military, and health care use questions; (b) open-ended questions about their knowledge of what services were available for MST and opinions on what obstacles some men may encounter when seeking services for MST; (c) questions regarding veterans’ thoughts and opinions about the design and effectiveness of two MST brochures. This article will only focus on data from the third part of the interviews (the results of the first two parts of the intervention and more information about interview methods can be found in Turchik, McLean, et al., 2013). In the final part of the interview, participants were asked to read and comment on two MST brochures: a gender-neutral version and a gender-targeted version. The gender-neutral brochure was in current use by VHA to provide information about MST and MST-related services (MST Support Team, 2008). The gender-targeted brochure for men was developed by the research team in consultation with the MST Support Team and was advised by current research literature (copy available by contacting the first author). Both brochures were of the same size and length and contained similar information regarding the definition of MST, how MST can affect individuals’ mental and physical health, availability of MST-related services, and relevant VA contact information. The gender-targeted brochure differed from the general one in that the images were only of men, and it included two additional sections, with one section addressing common questions or concerns men may have (e.g., being sexually assaulted does not change one’s sexual orientation; if a man has an involuntary or forced erection or ejaculation, it does not mean that the man wanted or enjoyed the assault) and another containing stories of male veteran survivors. The order of the brochures was counterbalanced. At the end of each interview, veterans were asked to compare both brochures and decide which they felt (a) provided the best information about MST for men and (b) was more effective in encouraging men to seek treatment for MST-related issues. These are the two interview questions of specific focus in this study.
Phase 2: Psychoeducational Mail-Based Pilot Intervention
Participants in the intervention subsample were randomly assigned to one of three conditions: control group, gender-neutral brochure group, and gender-targeted brochure group. The control group was asked to review and provide feedback on two unique influenza vaccination educational flyers that were in current use by the VA. The purpose of the control group was to aid in the examination of return rates and to serve as a baseline comparison group when examining mental health utilization over the follow-up period. The gender-neutral brochure group received the gender-neutral MST brochure and one influenza vaccination flyer with the same instructions, whereas the gender-targeted brochure group received the gender-targeted MST brochure for males and one influenza vaccination flyer. Each brochure/flyer was designed to offer education and resources on the respective topics. The gender-neutral and gender-targeted MST brochures are described above; minor edits were made in response to the interview phase to the gender-targeted brochure used in Phase 2.
Surveys
Each approximately 10-minute mailed survey consisted of three parts: (a) four military history background and VA health care use questions, (b) six questions about their opinions on an influenza vaccination flyer, and (c) six open- and close-ended questions about the two different MST brochures for the experimental groups or the influenza vaccination flyer for the control group. Five close-ended questions about the MST brochures were rated by participants on a 5-point Likert-type scale (e.g., 1 = poor to 5 = very good) regarding the brochure’s overall wording and text, overall pictures and graphics, how much the MST brochure addresses an issue that is important to male veterans, how likely they thought a male veteran who would benefit from MST-related services would seek treatment after reading the MST brochure, and overall rating of the MST brochure. The single open-ended question asked participants to provide any feedback on the MST brochure, including anything they think should be changed concerning the brochure.
Results
Interviews: Comparison of Gender-Targeted and Gender-Neutral MST Brochures
In comparing the two MST brochures during the in-person interviews, a greater number of veterans felt that the gender-targeted MST brochure presented the best information compared to the gender-neutral brochure (85% vs. 15%, p < .01) and would be more likely to encourage help seeking than the gender-neutral brochure (90% vs. 10%; p < .01).
Psychoeducational Mail-Based Pilot Intervention
There were no significant differences among the three groups in completion of the mailed surveys, with 55 returned from the control group, 47 from those who had received the gender-neutral MST brochure, and 51 from those who had received the gender-targeted MST brochure, χ2(2, N = 153) = 1.40, p > .05.
Comparison of Quantitative Ratings for MST Brochures
In comparing participants’ ratings on the gender-targeted and gender-neutral MST brochures across the mailing groups, participants’ ratings did not significantly differ on overall ratings of the wording and text, t(96) = .28, p > .05, or on the photos and graphics, t(96) = .56, p > .05. Participants’ ratings of the gender-targeted MST brochure were significantly higher than ratings of the gender-neutral brochure when asked to rate how well the brochure addressed an issue that is important to male veterans, t(96) = 2.10, p = .03, how likely participants think a male veteran who would benefit from MST-related services would seek treatment after reading the MST brochures, t(96) = 2.61, p = .01, and overall ratings of the brochure, t(96) = 2.22, p = .03. See Table 2 for means.
Comparison of Quantitative Ratings for Military Sexual Trauma (MST) Brochures.

p < .05. **p ≤ .01.
Use of VA Mental Health Care in the 6 Months Following Receipt of Mailed Psychoeducational Materials
The likelihood of using MST-related mental health care in the 6 months following receipt of educational materials did not significantly differ as a function of the type of materials received. Specifically, there were no significant differences regarding whether veterans initiated MST-related mental health care in the 6 months following receipt of the psychoeducational materials, χ2(2, N = 153) = 1.16, p > .05, with 9.1% (n = 5) of those in the control group, 6.4% (n = 3) of those in the gender-neutral brochure condition, and 3.9% (n = 7) of those in the gender-targeted condition receiving care. An analysis of covariance (ANCOVA) was also run to control for mental health visits in the year prior to study enrollment. There was no significant effect of condition type on MST-related care initiation over the 6-month period when controlling for mental health visits in the year prior to enrollment, F(2, 149) = 0.50, p > .05.
There were no differences between the three groups regarding whether participants used any mental health care services, χ2(2, N = 153) = .70, p > .05, with 16.4% (n = 9) of those in the control group, 10.6% (n = 5) of those in the gender-neutral brochure condition, and 13.7% (n = 7) of those in the gender-targeted condition receiving care. There was still no significant effect of condition type on mental health use over the 6-month period when controlling for mental health visits in the year prior to enrollment, F(2, 149) = 0.11, p > .05.
Discussion
The current study demonstrated that male veterans prefer to receive information about MST in the form of a gender-targeted brochure as compared to a more generic gender-neutral brochure. First, the majority of veterans during face-to-face interviews preferred the information in the gender-targeted brochure when directly comparing it to the gender-neutral brochure. This was also supported in a comparison of veterans’ ratings of each brochure among those veterans who completed mailed surveys. Although there were no differences in quantitative ratings of the brochures on design-related elements, veterans rated the gender-targeted brochure as both providing the best information as well as being more effective in encouraging men to seek treatment for MST-related issues. These findings are consistent with qualitative work demonstrating that female veterans also prefer gender-targeted information about MST (Turchik, Bucossi, & Kimerling, 2013) and that men with breast cancer prefer gender-targeted information (Iredale et al., 2007; Williams et al., 2003).
Men’s preferences for the gender-targeted brochure highlight the importance of exploring gender-specific informational resources for men, especially for certain behavioral health issues such as MST. Historically, most health information resources at VHA have been designed for male veterans who represented the vast majority of patients, whereas recent efforts have focused on ensuring that women are represented in VHA materials (U.S. Department of Veterans Affairs, 2013). Conversely, most health care resources concerning sexual assault have traditionally been designed for female patients. The current study suggests that gender-specific resources may be helpful given that there are likely some unique issues for male and female survivors of sexual assault, and for veterans, who have experienced MST specifically. For example, the gender-targeted brochure included statistics on male sexual assault and addressed concerns about sexual orientation and masculinity. It may be especially helpful for those male survivors who view sexual assault as a women’s issue; receiving gender-specific information helps highlight that they are not the only man who has experienced MST and may help reduce stigma. While it may seem more obvious to target informational materials and interventions related to certain health topics, such as sexual trauma or breast cancer, given that sex and gender differences are present in a myriad of conditions, researchers have suggested that this may be helpful for a wide range of health issues, including weight loss (Simen-Kapeu & Veugelers, 2010) and smoking cessation (Okoli et al., 2011; Torchalla et al., 2012).
Although male veterans preferred gender-targeted information about MST, the receipt of this information did not have an effect on whether veterans used mental health care over the subsequent 6-month period. In fact, those who received either of the MST brochures were not more likely than those in the control group to seek mental health care in the following 6 months. The current knowledge enhancement intervention was examined as a first step in attempting to increase access to mental health care for male veterans with MST as it is ideal in that it is brief and inexpensive. However, these results seem to indicate that (a) the current methodology was not able to adequately increase knowledge enhancement, (b) a knowledge enhancement strategy alone is not effective in increasing utilization rates in relation to MST, and/or (c) there were too few men who needed care in the study limiting our ability to detect differences.
It is possible that the current study was not able to affect utilization rates because the knowledge enhancement intervention was not powerful enough to do so. First, while the materials were targeted to veteran men, the materials were not individually tailored. Whereas targeted materials are an incremental advance over generic communication types, tailored materials specifically address those factors most relevant to an individual recipient (Kreuter, Strecher, & Glassman, 1999). While the primary aim of the current study was to design patient informational materials for men who have experienced MST that could be widely distributed in print form and accessed online—and individual tailoring was not feasible for our purposes—individual tailoring may be used in future research aimed specifically at increasing access. Furthermore, the current study relied on veterans to read and passively acquire the knowledge without any dialogue or communication with VA health care providers or researchers. The addition of a follow-up telephone call or receiving the brochure during a health care visit may have allowed veterans to ask questions and feel more comfortable in seeking help. For instance, an effective intervention by McFall et al. (2000) to increase posttraumatic stress disorder–outpatient care utilization among male veterans included both a mailed informational brochure and a follow-up telephone call, and it was found that those veterans who requested additional information during these calls were more likely to initiate treatment. Also, the current study did not assess for veterans’ need for MST-related care, and given that MST is a stressor, and not a diagnosis, some veterans likely do not want or need care related to MST. Finally, receipt of psychoeducational materials about MST by mail may not be the preferred modality of communication for many veterans. Future research should examine veterans’ communication preferences, including receiving information by mail, telephone, face-to-face, among waiting room materials, DVDs, website, e-mail, or secure messaging.
It may be that even though men found the information about MST acceptable and helpful, knowledge enhancement alone may not be enough to facilitate treatment seeking among men who have experienced MST. In addition to lack of knowledge, there are a number of factors that may serve as barriers or facilitators to help-seeking, including logistical and provider factors, stigma (Turchik, McLean, et al.,2013), gender-related preferences (Turchik, McLean, et al.,2013), veteran’s perceptions of the VA, trauma-related factors (Masho & Alvanzo, 2010; Monk-Turner & Light, 2010), and the veteran’s perceived need for care. The issue of stigma may be particularly salient, especially for men, and addressing this issue as well as other potential barriers may be needed to effectively increase help-seeking in this group.
Future research should focus on ways that may help decrease stigma and other barriers to MST-related care. In addition to interventions focusing on psychoeducation and outreach to increase knowledge (McFall et al., 2000), other promising interventions among veterans have focused on increasing access to care by enhancing intrinsic motivation for change using motivational interviewing techniques (Seal et al., 2012) and modifying negative cognitions and beliefs using cognitive-behavioral techniques (Stecker, 2013; Stecker, McGovern, & Herr, 2012). Both of these interventions were delivered by telephone, and such delivery can extend the reach of services to rural veterans and may be more acceptable to veterans who have stigma-related barriers to talking about mental health problems in-person (McGinty, Saeed, Simmons, & Yildirim, 2006). Such interventions may be ideal to examine in relation to increasing care among veterans who have experienced MST.
Limitations
While this study provides valuable information about male veteran’s preferences for information about MST, this study is not without its limitations. First, the sample size may have made it difficult to detect modest differences in treatment use; however, an examination of the raw data across groups does not suggest any differences in mental health care utilization trends across the three conditions. It may also be that 6 months was not an adequate follow-up period to see differences emerge across the three groups. Furthermore, the results of this research may not be generalizable to veterans outside VAPAHCS and/or to veterans seeking care outside the VA. Finally, as noted earlier, need for treatment was not assessed, and it is also possible that some participants already received past treatment that was not captured in the electronic medical record. The current study used random assignment, so while differences in perceived need were presumably similarly distributed across groups, not accounting for perceived need may have weakened the ability to detect differences in utilization.
Conclusion
Male veterans prefer gender-targeted information about sexual trauma compared to gender-neutral materials. However, the study also demonstrated that knowledge enhancement alone may not be enough to increase utilization of mental health care among this group, and future research is needed to better address the gender disparity in the utilization of MST-related mental health care. Research is needed to examine veterans’ preferences regarding how they would like to receive information regarding MST so that information can be adapted and presented in these modalities. Further examination of the barriers and facilitators of seeking help for sexual trauma is also needed to inform intervention efforts. Finally, future research should examine perceived need for care, an important variable to examine as many veterans who experience MST may not want or need services.
Practice Implications
The current study demonstrated that male veterans find it acceptable to receive printed information about MST and that they prefer to receive gender-targeted versus gender-neutral printed information. We believe that although this study only examined the preferences of male veterans, that these results likely generalize more broadly to men who have experienced sexual trauma, and suggest that providing information about sexual trauma is acceptable to men and should be done so in a gender-targeted manner.
Footnotes
Acknowledgements
The authors would like to thank Caitlin McLean, BS, for her assistance in preparing mailings and conducting interviews, and Meghan Saweikis, MS, for her data programming assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the VA Advanced Fellowship Program in Mental Illness Research and Treatment, VA Office of Academic Affiliations, National Center for Posttraumatic Stress Disorder, and the VA Palo Alto Health Care System. The views expressed are those of the authors and do not necessarily reflect the official policy or position of the Department of Veterans Affairs or the United States Government.