
Abstract
This study reports findings from the Black Women’s Perceptions of Black Men’s Depression (BWP) study, which included eight focus groups with Black women (N = 46) from southeastern Michigan. Four themes illustrated the impressions of Black women from different socioeconomic backgrounds: Black men’s depression is a cultured and gendered phenomenon, the role of Black women in Black men’s depression, intergenerational differences with how depression is handled by Black men, and the need (and ways) to reach Black men with depression resources. Results underscore not only the importance of understanding the kind of depression in Black men that meets criteria described by the Diagnostic and Statistical Manual of Mental Disorders (DSM) but also the psychological distress that may coexist with (or be separate from) DSM depression. Implications for interventions that educate, diagnose, and treat depression in Black men are discussed.
Previous studies have recognized the important role that women play in the health knowledge and behaviors of men (Clements, Parry-Langdon, & Roberts, 2006; Gomez, 2006; Hale, Grogan, & Willott, 2004; Lyons & Willott, 1999). However, despite the roles of women in the lives of men, studies have not adequately investigated Black women’s knowledge, attitudes, and behaviors regarding Black men’s depression for the purpose of improving the mental health of Black men. This study convened eight groups of Black women to discuss their experiences with (and knowledge and attitudes about) Black men’s depression, their relationships with Black men, and their thoughts regarding the barriers and facilitators to seeking treatment for depression among Black men. Given their important roles in the lives of Black men, Black women’s perspectives are useful in therapeutic relationships with Black men, as well as the development of interventions (such as educational websites, depression education workshops at churches or on college campuses, and/or support groups for depressed Black men) that aim to both inform and encourage Black men to increase their knowledge about depression, reduce the stigma surrounding depression, and educate Black men and members of their support networks about the value of seeking treatment for depression.
The current study reports findings from the Black Women’s Perception of Black Men’s Depression (BWP) Study. The BWP study data were collected during the summer of 2010 in southeastern Michigan and focused on obtaining in-depth information from Black women about their experiences with depression in Black men. Our aim was to use Black women as a resource for obtaining information about Black men’s depression to develop new ways to reach Black men. Using Black women as a channel through which scholars gain additional perceptions about Black men would allow us to tap into an aspect of Black men’s lives that has not been accessible through our previous work with Black men (Neighbors, Watkins, & Abelson, 2012; Watkins, Green, et al., 2007; Watkins & Neighbors, 2007). From a gender roles perspective, this approach is significant because of the influence that women have in the lives of men, generally, and with regard to their role in nurturing the health and well-being of their families, in particular (Lee & Owens, 2002; Purk, 2006). From a cultural perspective, this nurturing role is amplified for women of color, as the needs of people in communities of color tend to be in excess due to the history of oppression and social and economic challenges (Hill Collins, 2000; Parham, White, & Ajamu, 2000).
Three decades of research have presented a growing interest in gender relations and health (Bottorff, Oliffe, Robinson, & Carey, 2011). Specifically, research on the role of women in men’s health has included studies on the influence of women on men’s dietary behaviors (Allen, Griffith, & Gaines, 2013; Homish & Leonard, 2007), gender roles and relations in health research (Bottorff et al., 2011; Joseph, Kaplan, & Pasick, 2007), women’s thoughts on the sexual health and sexually transmitted disease testing of men (Oliffe et al., 2013), and women’s influence on substance use by their male partners (Homish & Leonard, 2007; Leonard & Homish, 2005; Westmaas, Wild, & Ferrence, 2002). Of the various angles at which the role of women in the lives of men has been examined, the role of female caregivers is presented most frequently in the literature, particularly with regard to the physical health of men. The role of women in men’s mental health is a less explored area, and many of these studies have reported findings from men and women outside the United States (see Chang & Horrocks, 2006; Oliffe, Kelly, Bottorff, Johnson, & Wong, 2011, for examples). A few studies have reported on mental health caregiving by males (Mays & Lund, 1999); however, reports on the experiences of female family caregivers dominate the literature (Guarnaccia & Parra, 1996; Rose, Mallinson, & Gerson, 2006; Suresky, Zauszniewski, & Bekhet, 2008).
While vital to our understanding of the health and well-being of families, studies on gender relations and mental health—particularly, the role that women have in the lives of their male friends and family members—rarely present the gender implications of male–female dynamics or discuss the gendered contexts of depression. Another characteristic these studies lack is a thorough evaluation of the similarities and differences in gender relations for mental health between women who care for men compared with women who care for women (Suresky et al., 2008). To prepare for the future development of interventions that focus on depressed Black men, it will be useful for us to improve our understanding of the role of women in the lives of depressed Black men and to learn more about Black women’s perceptions of the depression experienced by Black men. The intersection of gender and culture provides a unique perspective for studying the role of Black women in the lives of Black men.
As gender and culture intersect for Black families, the challenges of dealing with depression introduce another level of concern. For instance, since Black men tend to use their personal experiences and what they see in popular media to define depression instead of information from health care professionals (Watkins & Neighbors, 2007), and due to cultural pressures for Black men to solve emotional (and other) problems on their own rather than to talk about sensitive issues, they may be less likely than Black women to communicate with others about their mental health needs and challenges. One consequence of Black men being less likely to communicate their problems to others is that they may have difficulty with expressing the feelings they experience to health professionals (Kendrick, Anderson, & Moore, 2007; Watkins & Neighbors, 2007). Family and communal relations influence the development of depression and the responses to depression in Black men because these relations can sometimes implicate traditional masculine norms and exacerbate men’s fears of being perceived as weak (Bryant-Bedell & Waite, 2010; Head, 2004; Kendrick et al., 2007; Watkins & Neighbors, 2007; Watkins, Walker, & Griffith, 2010). Other men have been identified as useful social support for Black men with mental health needs (Plowden, John, Vasquez, & Kimani, 2006), but the role of women is less clear. Black women are clearly involved in the lives of Black men with depression, yet Black women are oftentimes left out of our scholarly discussions about ways to understand, intervene, and support the positive mental health of Black men. In an effort to understand the culture and gender formulations of depression for Black men—and to extend previous literature that suggests including broader social support networks in understanding and intervening with Black men—Black women should have more of a presence in discussions about depression etiology, diagnosis, and treatment in Black men. Black women should also be included in discussions about ways to reduce the stigma of depression in the Black community, educate Black men about depression, and how to seek help for it.
Method
Study Design
The impetus for this study derived from our interests in developing culturally sensitive and gender-specific depression messages (such as how to communicate appeal and language tone) and mediums (communication materials that are most preferred; e.g., flyers, brochures, web-content, videos, radio spots, billboards, workshops, and seminars) for Black men and members of their social support networks. This effort is part of our overall desire to better educate Black men and members of their social support networks about depression and the utility of depression treatment and to help clinicians intervene more effectively with depressed Black men. Asking Black women to discuss how depression has affected the Black men in their lives guided this area of study. Participants were recruited from three income brackets to determine if Black women’s perceptions were influenced by income group, and thereby, socioeconomic status. It was anticipated that participants would have varying degrees of interpersonal relationships with Black men and would share stories about their fathers, brothers, partners, and friends. The study team was interested in learning about ways in which Black women interacted with and responded to the needs of the Black men in their lives (while they are depressed) as well as Black women’s thoughts about their possible roles in the experiences of Black men (who may be depressed).
Qualitative inquiry via focus groups was the methodology used to improve our understanding of Black women’s perceptions of depression in Black men. Not only do focus groups capture the complexities of the thinking and behaviors of its members in greater depth than is possible in a quantitative survey, but also the group interaction and dynamics help elicit in-depth thought (Ulin, Robinson, & Tolley, 2005). During focus groups discussions brainstorming occurs, as participants can build off one another’s ideas. Another advantage for using focus groups for this type of inquiry is that the questions asked to the participants can be modified as information needs change or as ongoing evaluations reveal the need to alter the study protocol. Focus groups were used in this study to capture, in detail, the perceptions of Black women about Black men’s depression.
Participant Recruitment and Characteristics
Focus group participation was sought from Black women who wanted to discuss depression in Black men. The study team recruited Black women with varying household incomes. The flyers included language that encouraged Black women who knew a depressed Black man to call or email the project coordinator. Callers were screened using a brief questionnaire that asked them about their age, county of residence, total household income, and race/ethnicity. Participants were recruited for the study through direct person-to-person contact by individuals affiliated with the study and by asking people who had already been recruited for the names and contact information of other potential participants (Morgan & Krueger, 1998). The study team also used their contacts in the local colleges, universities, and community groups to recruit Black women who may be interested in the study. After focus group participants were recruited, the following steps were used to increase the likelihood that they would attend their scheduled focus group. First, participants were contacted 1 month to 2 weeks before the actual group, for screening and to assign them to their respective income group. Next, follow-up calls were made to participants the day before their scheduled group. All focus groups were composed of 4 to 10 participants. Two groups were held for each of four household income brackets (less than $19,999; between $20,000 and $59,999; more than $60,000; and “mixed income” groups that consisted of women from all income brackets).
Forty-six (N = 46) Black women participated in the study and were asked to complete a demographic questionnaire (see Table 1). Two thirds of the participants were between the ages of 20 and 35 at the time of the study. Sixty-seven percent had never been married, and 70% had either a college degree or some graduate or professional school training. Forty-three percent of them were employed full-time at the time of the study, and 61% had no health, medical, or mental health training. Though thirty-three participants (78%) reported that they had been depressed at some point in their lives, the Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001), a screening tool for detecting depression, was included in the demographic questionnaire and identified only three focus group participants (6.5%) who screened positive for depression in the past 2 weeks. The PHQ-9 depression criteria require that respondents indicate that (a) they had at least one of two major symptoms (having little interest or pleasure in doing things, or feeling down, depressed, or hopeless) more than half the day, nearly every day; (b) they have at least five total symptoms that occurred more than half the day, nearly every day (a single thought of suicide counts as a symptom); and (c) the symptoms made it at least somewhat difficult to function. A few of the women met criteria for subthreshold depression—some depression symptoms, but probably not enough to meet criteria for a current depressive disorder. The three who screened positive can be interpreted in the context of data from the National Survey of American Life (NSAL; Jackson et al., 2004), a large national survey of the mental health of Black Americans, which suggested that 3.2% of African American women out of about 2,300 met criteria for current depression (major depressive episode or dysthymia).
Characteristics of the Black Women Who Participated in the Focus Groups (N = 46).

Focus Group Protocol and Questionnaire
The lead investigator and project team developed the focus group questionnaire that elicited discussion on the following topics: (a) general knowledge about depression, (b) personal experiences with Black men who were depressed, (c) the unique aspects of depression in Black men, and (d) talking with Black men about depression. Focus group questions also addressed barriers and facilitators to men seeking treatment for depression, the role of social support networks, and stigma surrounding mental illness for Black men. The women were encouraged to discuss the potential challenges in their relationships with and providing social support to a Black man with depression. The lead investigator and project team pilot tested the focus group protocol and questionnaire with a “mock” focus group, which consisted of Black female graduate students and other university-affiliated Black women. The mock group underwent the same recruitment and screening procedures that were used to recruit and screen the women for the seven groups in the field. Responses to the questions were recorded and transcribed; the transcripts were read, and then project staff considered suggestions for improvement during project meetings. After minor modifications were made to the protocol and questionnaire, the lead investigator lead the study team in implementing the focus group protocol in the field to collect data for the seven scheduled focus groups. Since only minor edits were made to the protocol after the mock focus group was conducted, data from the mock focus group were included in the final analysis. An eighth focus group of “mixed income” women was conducted so that the results could include two groups for each income bracket.
Data Collection
The lead investigator (a trained and experienced focus group moderator) and an assistant (matched for race and gender) led the focus groups with Black women about depression in Black men. The moderator was responsible for guiding the focus group discussions and ensuring that all notes and audio recordings were appropriately labeled at the end of each focus group. The major responsibilities of the assistant were to ensure appropriate consent forms were distributed, signed, and collected and to take notes during the focus groups. All responses were kept confidential. The average length of each focus group was approximately 90 minutes. Dinner was served during the focus groups, and participants each received a $25 honorarium.
The Protection of Human Subjects
The lead investigator ensured that all phases of the study were performed ethically. There was minimal risk to study participants, and the institutional review board approved the project. At the beginning of each focus group, the moderator discussed the purpose of the study and the topic of interest. Participants were informed of the procedures used, the types of questions that would be asked, and their rights as participants. After providing this information, participants were asked if they understood what the study involved and if they would be willing to participate. Participants were then assured that all identifying or personal information would remain confidential throughout the process to protect their privacy. During the explanation of participant’s rights, confidentiality, and informed consent, the moderator obtained permission to audio record the discussions.
Data Management and Analysis
After focus groups were held, the audio recordings were transcribed by a hired transcriptionist, and the transcripts and audiotapes were analyzed by the project team. The analysis was guided using a qualitative team approach (Watkins, 2012a) supervised by the lead investigator. The study team used a spreadsheet technique to organize, manage, and analyze the data (Stockdale, 2002; Swallow, Newton, & Lottum, 2003). First, a word processing program was used to place all the data into a table with multiple rows and columns. Development of this spreadsheet or all-inclusive “data table” was the first step in the analysis process. The data table included eight column headings: transcript number, income group, questionnaire section, question asked, participant’s response, notes, code, and theme. After this data table was created, the team used a data reduction technique developed by the lead investigator, which involved using this all-inclusive data table to produce shorter, more concise data tables. To reduce the table, the study team reviewed the all-inclusive data table and made notes about areas of commonality and overlap across groups or between participants (e.g., transcript numbers, income groups) and then generated opinions about the relevance of certain quotes and the intersection of concepts. For this study, four different phases of the data reduction table were created, and each signified a more concise and concerted presentation of the data.
As a part of the data reduction technique, coding procedures were employed that allowed segments of raw text to be identified and compared to other segments and analyzed for embedded meaning. Meaningful text segments were used to identify categories, concepts, and themes important to the project goals and objectives. Data were analyzed using classical content analysis, which involved identifying the frequency of codes to determine which concepts were most cited throughout the data (Leech & Onwuegbuzie, 2008; Watkins, 2012a). Similarly, the study team used constant comparative analysis to generate a theory or set of themes deduced from narrative or textual data (Leech & Onwuegbuzie, 2007). The purpose of this phase of the analysis was to determine broad study themes and the overall impression of the study team about Black women’s experiences with depression in Black men. The study team worked individually, then collectively to “reduce” and code the data in a way that would lead to identifying the major themes of the study. The exploratory nature of this analysis was considered and influenced the study teams’ discussion of how the themes would be presented in this report, with an understanding that this article would provide an introduction to the work and that subsequent reports would provide a deeper examination of the broad themes presented here, as well as others.
Results
Focus group participants provided an enriched perspective regarding their experiences with depression in Black men. Most of the participants had never been married (Table 1) and talked primarily about their husbands, boyfriends, fathers, sons, brothers, and friends; rarely did they speak about other men such as their uncles, in-laws, or coworkers. To interpret the results in context, it should be noted that although Black women who were willing to talk about their experiences with depression in Black men were recruited, the study team left it up to the women to volunteer for the groups after learning about the eligibility criteria. In other words, the women did not have to confirm that they knew a Black man who had received a depression diagnosis from a clinician prior to admittance into the groups. Given the exploratory nature of this research, however, it was interesting to hear the women’s perceptions about depression in Black men, within their own contexts and understanding of the word “depression.” In a subsequent article, the nature of the participants’ understanding of “depression” will be addressed. However, for the purposes of this article, the results for Black women’s overall impressions of depression in Black men, based on their experiences, are presented.
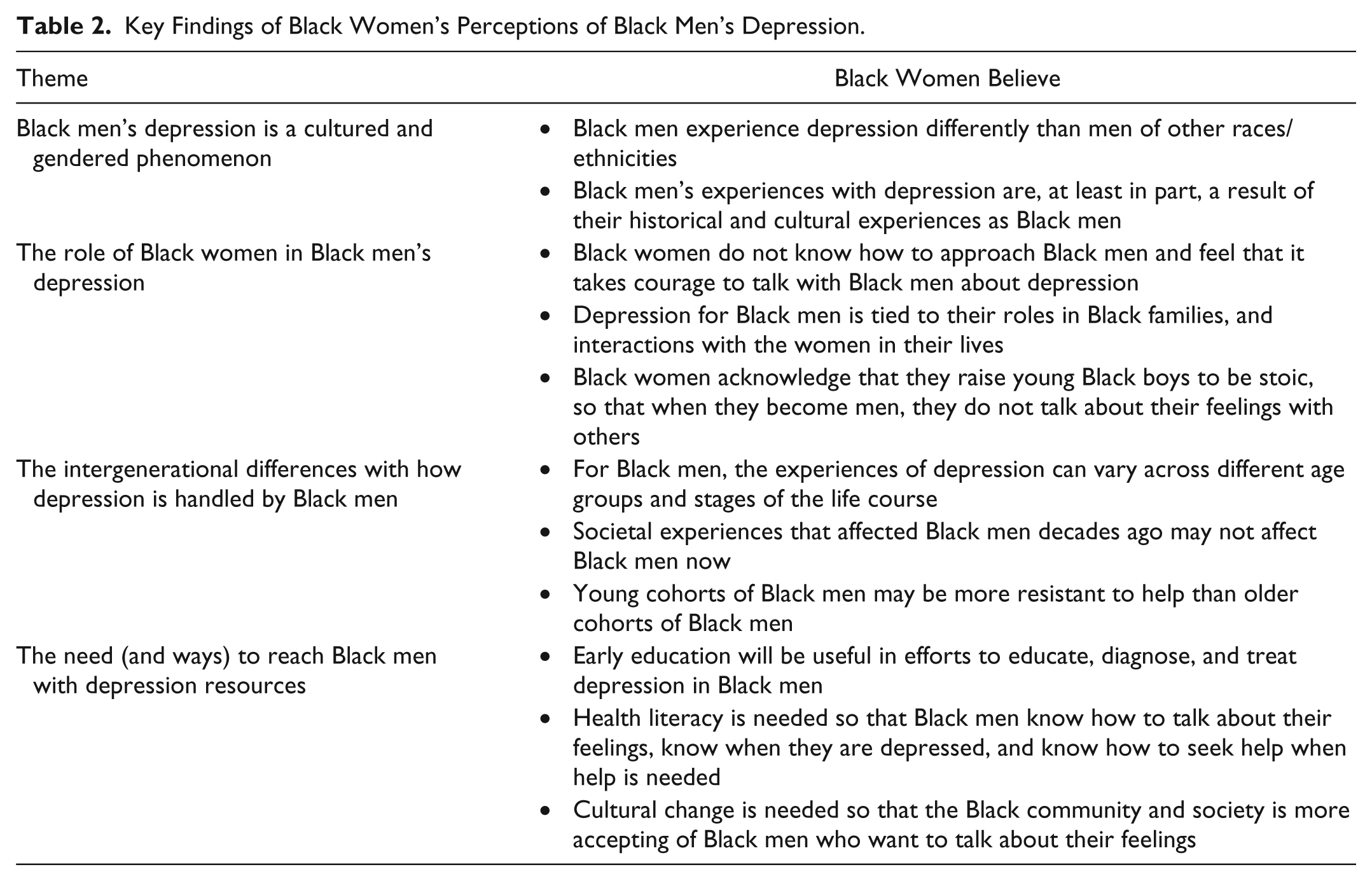
The decision to group participants by their income levels as opposed to grouping them by age, geographic location, or marital status is also noteworthy when interpreting these findings. This decision was an attempt to determine if differences would exist between and across groups with regard to their knowledge, attitudes, and beliefs about Black men and depression. However, with the exception of access to resources and educational differences, all the women seemed to relate similarly to Black men (and to one another). Instead of income-level differences, our analysis revealed slight age group and life stage differences regarding the way participants responded to the questions about Black men. A number of co-occurring themes emerged from the data, but for the purposes of this (an initial report from our analysis) four themes surfaced to characterize, in a more general sense, Black women’s perceptions of depression in Black men: Black men’s depression is a cultured and gendered phenomenon, the role of Black women in Black men’s depression, intergenerational differences with how depression is handled by Black men, and the need (and ways) to reach Black men with depression resources (Table 2). Details for these themes are presented below.
Key Findings of Black Women’s Perceptions of Black Men’s Depression.
Black Men’s Depression is a Cultured and Gendered Phenomenon
As the question-and-answer format of the focus groups evolved into full discussions about Black men’s depression, one of the most frequently discussed topics was the unique culture- and gender-related experiences of Black men. These discussions emerged when the overall differences between Black men and Black women were discussed. For example, some women described the experiences of depression for Black men broadly, as a college student in one of the mixed income groups said,
It’s just, they are living in a completely different world that I try to understand every day. I have two brothers, I have a father, and loved ones but I can never understand . . . so for their depression, it’s something completely different, it would have to be.
The focus group participants acknowledged that differences in depression between Black men and Black women existed; however, they were unsure about exactly what those differences were, or what those differences mean for Black men who are depressed. Some women underscored the history of Black men in America as the reason why Black men’s depression is so different than that of Black women. The women offered their opinions about how the legacy of slavery affects Black men in today’s society. For example, a woman from one of the mixed income groups stated:
Why can’t a Black man stay with a family? Well systematically, he was torn from his family and was not allowed the opportunity to really be a father or the head of the family. So it’s psychological, generational, their inability to perform and then to try to perform to the standards of the dominant culture, which continually, you know, tears him down.
Probed by the moderator, the women were encouraged to discuss their opinions about the differences Black men experience compared to men from other racial and ethnic groups. Several participants agreed that the unique experiences of Black men, particularly with regard to depression, mean that their images run the risk of being tainted, unlike the images of men from other racial and ethnic groups. As a woman from one of the high-income groups explained:
I think the White man or the Asian man or whomever would not have a problem talking to someone else about their issues or, you know, having a down moment. . . . [No one] devalues who they are as a person . . . it’s not a blemish on their character, it’s just something that happens. But, I think for our Black men it becomes a blemish on their character . . . maybe not in the way that people perceive them but . . . in the way they perceive themselves.
These types of comments led to discussions about the influence of men from other racial and ethnic groups on Black women’s perceptions of Black men, as well as the role of the Black community in Black men’s challenges with depression. Several women spoke candidly about the images of Black men—from both in and outside of the Black community. This point was also demonstrated through one woman’s plea to the other women in her group about what makes Black men’s experiences with depression such a cultured and gendered phenomenon:
As a community, we put on our Black men what they can’t be, and that’s vulnerable . . . although they may be experiencing depression in the same manner which men from other cultures or races are experiencing it, they’re not allowed to show it or let it manifest the way the other men can . . . they cannot afford that to be another strike against them in society’s eyes or in the eyes of the Black community or Black women or whoever.
Another topic that emerged during this discussion was that Black men must be strong, macho, and work twice as hard as men from other racial and ethnic groups in order to do well by society’s standards. Many participants agreed that despite the extra effort, Black men are not afforded the same advantages as other men. Women in the middle-income groups believed that Black men have unique experiences compared to men of other racial and ethnic groups because of society’s impressions of them. Specifically, the women noted that by virtue of Black men being both “black” and “male,” they are not supposed to experience hurt or express their emotions to others. Rather, they are supposed to keep their feelings suppressed.
The Role of Black Women in Black Men’s Depression
Participants were asked to discuss if they have a role in the lives of Black men who are depressed as well as what this role entailed. The women reported many feelings, ranging from their sense of obligation to anger and frustration with the idea that Black women have a responsibility to Black men to help shape and maintain their mental health. The most provocative discussions were the opposing sides about the role of Black women overall, as some women felt that it was the Black woman’s responsibility to take an active (and sometimes, lead) role in the health of Black men, particularly when it comes to depression. Meanwhile, other women thought that Black men should be urged to take responsibility for their own health issues. This point was further illustrated by a woman in one of the mixed income groups, who said,
It’s not the Black woman’s responsibility to take the Black man to the doctor. I mean the only thing you can do is educate them, provide them with the information and it’s really up to them to do it . . . we as Black women we’re not doing that with our male children or even with our men. We don’t hold them accountable . . . [we say to ourselves] well maybe it’s something I did, maybe that’s why he’s acting the way [he is acting] . . . no, it’s not about you, he needs to be personally responsible for his behavior . . . the Black superwoman is dead.
The idea of the “Black superwoman” received notable attention in the mixed-income groups and led to a discussion about Black men’s receptivity to receiving help from Black women. During this discussion, some of the participants thought that the Black men they knew would be receptive to help from other Black men, especially if they were counselors. The women also shared their thoughts about whether they felt prepared to help the Black men in their lives. For example, participants in the low-income group admitted that they try to avoid talking about depression with Black men because they “don’t know how to handle the situation.” These women admitted to caring about the Black men in their lives; but they do not know what to do about Black men’s depression.
Regardless of whether the participants felt that they had a role in the depressive experiences of Black men or not, many of them offered their opinions for why they do not talk with their men about depression. For a woman in one of the middle-income groups, discussing depression with Black men was a courageous decision, as she stated,
I don’t think I’ve ever had the courage . . . it takes a lot of courage and a lot of, um, I don’t even know . . . to approach someone that you care about and that you love about that word. . . . It’s what that word means, you know?
Meanwhile, another participant in one of the two middle-income groups underscored the stigma attached to depression among Black men and how this stigma influences her ability to talk to her husband about it. She said,
With Black men, the word depression is very taboo, it’s something that you don’t discuss in your household. . . . I just feel like I would insult my husband by asking him if he’s depressed. I mean I know the signs very well but I wouldn’t, I don’t think I would . . . be like “are you depressed?” You know, unless he got to the point where I felt like he was going to harm his self then yeah, I would step in and absolutely do something about it. But I just kind of let him deal with whatever he’s dealing with in his own way.
The idea that depression was not an issue unless her husband was in danger of harming himself is a testament to the way many participants felt about mentioning depression in the presence of Black men. Moreover, many participants said that depression is a topic that must be treated delicately and that approaching Black men inappropriately would not be a good idea. For instance, someone from one of the middle-income groups noted,
This is a very delicate issue. You can’t just go storming into it . . . and I think another aspect is that, as Black women, we can’t come across as though we’re trying to be the boss in that we’re trying to make them or force them to do anything.
The women were fearful that their approaches to discussing depression with Black men would deter the men from getting help, much less, talk about their depression with others.
The Intergenerational Differences With How Depression Is Handled by Black Men
Questions about Black women’s perceptions of Black men’s depression led to discussions about several participant-initiated topics (or, topics that were not listed in the focus group protocol or probed by the moderator). One participant-initiated topic of particular interest was respondents’ perceptions of depression in Black men in the context of generational similarities and differences. For example, a participant from one of the mixed-income groups spoke candidly about her observation of the generational differences with the men in her life. She said, “I have a son, 22, [with] whom I’m having a lot of problems and I’m very concerned that he may be suffering from depression because I believe his father was, my father [was], my brother [was].” Other women from this mixed-income group then shared their experiences with how depression varies across Black men of different ages, as well as how the trajectory of depression can change as a Black man ages. As one woman explained,
Something that’s interesting with my father is that [depression] had always been there . . . my mother told me that the therapist told her that these types of things don’t age well and I think he’s less capable of managing it the way he did when he was younger. [Back then] he had more energy, or more resources or whatever . . . [but now he] doesn’t have whatever it is to . . . deal with it anymore and I think it does have to do with his age.
Not only did participants discuss how the age of a Black man could influence his experience with depression but they also acknowledged their own age differences and how their ways of seeing the world influences their ability to feel comfortable talking openly about depression with Black men. For example, a participant in one of the middle-income groups declared,
I think age has a lot to do with it also, because I’m a little older and the people that I relate to are a little bit older and they are more comfortable with who they are that you know some of these conversations are able to go on.
This notion that a man might have a harder time dealing with depression as he gets older, but that his partner might feel more capable of and confident about talking about depression as she ages, was an interesting contrast. According to the women, the impact of age is not unidirectional but rather an exchange between men and women that is multifaceted. Comments like this segued into the types of resources that could be developed for Black men.
The Need (and Ways) to Reach Black Men With Depression Resources
During the focus groups, many women expressed the need for more education about depression for Black men and women. Each focus group ended with the moderator encouraging participants to think about ways to reach Black men (those potentially at risk and those not at risk) with depression resources. Responses were similar across income groups, as many women highlighted the importance of providing education to young Black men and teaching Black men how to talk about their feelings. During these discussions, some women offered strategies for how to talk to Black men, such as a woman in one of the high-income groups who said,
Give them the words to use so that they don’t have to become that angry Black man, or that functioning alcoholic. So they can just, you know, get help and deal with it, you know, and get to the point where they can move on.
Another woman from the same group felt that the ways in which Black men are approached should be revisited by Black women, as she noted,
We have to be a little bit more deliberate in the conversations we have. . . . I think we just need to have more conversations . . . [but] we have to tread lightly, can’t come in all guns a blazing, saying you know, “you’re depressed and you need to go to xyz.”
Other participants felt that dealing with depression was not just a Black men’s issue but an issue faced by the Black community as a whole. These participants discussed resolving depression in Black men by using the Black community as a setting for education and training programs. One woman said,
Everybody needs training—male and female—so that we can recognize [depression] in each other. . . . I think we need to go into our community and open up the issue a little bit more and get some knowledge on our people . . . so that [depression] can be recognized.
This knowledge that the women discussed is something that they agreed could be disseminated to Black men as early as possible, especially during their childhood. No specific programmatic ideas were discussed, but a woman in one of the middle-income groups explained,
If we could talk to them when they’re younger . . . if you’re given the tools when you’re younger maybe it won’t have to be a discussion about Black men, you know 30 years or 50 years from now because they’ll hopefully [be] equipped with the tools so that they don’t become depressed Black men.
While discussing depression resources, the participants also brainstormed about settings that could be useful in reaching Black men. For example, women in a middle-income group talked about working directly with Black families who have been affected by depression while others discussed how men’s church groups could provide safe spaces for men. Overall, participants expressed being both concerned about and interested in improving depression resources for educating and treating Black men.
Discussion
This study is the first report from the BWP study, a qualitative study conducted in southeastern Michigan. The purpose of the BWP study was to examine Black women’s perceptions of depression in Black men, with the goal of understanding depression and the experience of depression in Black men through the eyes of Black women. The BWP study presented an exploratory look into how Black women not only perceive depression in Black men but also their opinions about the manifestation, etiology, treatment of, and response to depression by Black men. Though previous studies have captured women’s roles as they relate to other aspects of men’s health (Allen et al., 2013; Homish & Leonard, 2007; Oliffe et al., 2013), these studies have not examined perceptions of men’s mental health through the eyes of women. In particular, Black women’s impressions of Black men’s mental health have been virtually unexplored. The current study helps fill these gaps by offering a Black women’s perspective for how depression is experienced by Black men.
Despite the hours of focus group data that were collected for the BWP study, the four themes discussed in this article emerged from the authors’ interpretation of the most significant ideas presented during the focus group discussions. First, the idea that depression in Black men is a cultured and gendered phenomenon highlights the importance of using an intersectional approach to working with depressed Black men and their families—attending to the influences of both gender and culture. Previous reports have demonstrated the importance of intersectionality in Black men’s depression by using conceptual models to frame social determinants that will improve future approaches by researchers and practitioners who work with Black men (Cooper, 2006; Watkins, 2012b; Watkins & Neighbors, 2012). More targeted, informed, and focused approaches that demonstrate an understanding of the unique challenges and contexts faced by Black men are likely to have the most immediate and beneficial effects on depressed Black men and members of their social support networks.
Although previous studies underscore the individual factors that affect depression in Black men, they do not provide details regarding the interpersonal or relational factors that contribute to how Black men experience and deal with their depression. The current study is an initial attempt to fill this gap in the literature, as our findings consider the relationships that Black men have with Black women, and how women believe depression is experienced by Black men. In fact, the role of Black women in the depressive experiences of Black men was another prominent theme from the BWP study. Though the women could not agree on whether they had a responsibility to help Black men who may be depressed, their disagreements were not bound by income bracket or age. The BWP study was conducted in the context of income group differences among Black women, but differences across income groups were minor for the four themes presented in this article.
There was no agreement regarding the role that women have in Black men seeking help for depression. However, several participants questioned the role of Black women in the etiology of depression in Black men. This was best represented by one participant who said,
We’re the foundation, we’re the backbone of families, and we get things done. . . . I think some[times] depression [occurs] in Black men because we as Black women are so strong. We are so, so strong and we do so many things that they feel like they are not “the man” and they can’t live up to that.
Beyond the actual experiences of depression for Black men, the data reported here also underscore how depression in Black men influences their relationship with Black women. Participants believed that depression prevents Black men from assuming their roles and responsibilities to their families and to themselves. They agreed that Black women (who are already juggling other responsibilities) are oftentimes forced to assume the responsibilities of Black men. However, Black women are hesitant to assume additional responsibilities because they feel overwhelmed and/or unable to help or because they believe that some of the responsibilities—such as the decision to seek help—should be assumed by the men themselves.
Though the focus groups were guided by a questionnaire, participants often raised points that were not initiated by the moderator. Examples of this are the participants’ perceptions of intergenerational differences with how depression is handled by Black men. Unlike the other three themes presented in this article—which were either prompted by a question or probed by the moderator—the ways that Black men of various ages present, discuss, and manage depression emerged as an important topic that originated from the participants’ reflections. Our finding that age is a determinant in depression identification and intervention is consistent with previous studies on Black men and depression (Griffin, 2000; Love & Love, 2006; Roy, 2006; Utsey, Payne, Jackson, & Jones, 2002; Watkins & Neighbors, 2007; Woodson & Koo, 1999). For example, previous studies underscored psychosocial models of development that suggest Black men move through stages during the life cycle, including early adulthood, middle adulthood, and old age or late adulthood (Bowman, 1989; Watkins, 2012b). Other age-related trends were revealed with regard to depression in Black men, though due to space limitations, these trends will be addressed in subsequent reports. Also noteworthy from our study findings is the idea that the women feel the need to “tread lightly” or discuss depression with Black men in a delicate manner. Income group differences were not obvious for the women’s feelings about using a gentle approach when talking with Black men about depression, but this concept needs a thorough examination in future studies.
The BWP study goal was to understand Black men’s depression from the perspective of Black women. The women were not asked to confirm that their men were ever diagnosed with depression by a clinician, nor were these men screened for depression by the study team. Some of the men discussed during the focus groups may have had other mental health problems, or may have been experiencing stress or distress, as opposed to, or in addition to, diagnosable depression (which has been highlighted by previous studies; Watkins, 2012b; Watkins & Neighbors, 2007). The study team decided to be more inclusive because the goal of the study was to understand “depression” from the perspective of community members, since understanding depression as community members perceive it is a useful step in the path to understanding ways to improve mental health outcomes for Black men. This “community definition” of depression—particularly for the Black men discussed in the current study—likely includes both clinical depression (i.e., DSM-IV-TR major depression, dysthymia, bipolar disorder, or adjustment disorder with depressed mood) and other, nondiagnosis specific states (such as stress and psychological distress)—all of which are important to understand when framing programmatic efforts that target Black men who are experiencing poor mental health.
One of the study goals was to understand not only the depression that has been described by the DSM but also the psychological distress that may coexist with DSM depression, or be separate from DSM depression, but that is familiar to Black families. The stress or distress that may be a response to challenges such as unemployment, a legacy of slavery, or demoralization following an experience of discrimination complicates the willingness of Black men to seek help for depression and the ability of clinicians to treat depressed Black male patients. Therefore, it is important for clinicians to understand the context in which DSM depression exists for Black men. Understanding and empathy by clinicians who work with Black men can be important for creating a successful therapeutic alliance. The data from this study will help with efforts to educate Black men about DSM depression and help us learn more about how to deal with factors that accompany and complicate DSM depression care and entry into care by Black men. Clearly more needs to be done to engage men in conversations about their feelings, in general, and depression, more specifically.
Limitations
There are a number of limitations that come with the qualitative design that was used in this study. For example, since the purpose of focus groups is to provide in-depth information about a particular phenomenon, it was not our intent to generalize these findings to a larger population. The rigor of our methods do allow for our findings to be transferable (Ulin et al., 2005; Watkins, 2012a) to community settings that include Black women with demographics and characteristics similar to the women in the current study sample. On a related note, since the focus groups were held in institutions of higher learning, some of the participants who participated in the lower income focus groups were college students. Therefore, our findings are not particularly reflective of the perceptions of low-income, noncollegiate Black women from our geographical setting. Next, the information that was obtained in this study is a reflection of Black men through the eyes of Black women. Indeed, there are certain biases that must be considered when using secondary sources to acquire information. Therefore, while our study provides interesting information about Black men from the perspective of Black women, it does not provide a first-hand account of depression from the perspectives of the men themselves. An interesting next step in this research would be to ask the Black female study participants to share the names of the men to whom they were referring during the focus groups. Then, data could be collected from these Black men and cross-referenced with the discussions held by the Black women. Data triangulation approaches such as this should be considered in future studies. Despite these limitations, this study makes valuable contributions to depression work with Black men and members of their social support networks.
Conclusion
Findings from this report of the BWP study data will be used to guide the development of culturally sensitive and gender-specific depression messages (such as how to communicate appeal and language tone) and mediums (communication materials that are most preferred; e.g., flyers, brochures, web-content, videos, radio spots, billboards, workshops, and seminars). The findings will also be helpful to those who want to provide gender and culturally appropriate mental health treatment to Black men and their families. Mental health providers should be aware of the extent to which mental health stigma is still a prominent barrier to care for Black families. Depression is such a difficult topic to discuss; Black women feel the need to raise the issue with their male family members with great sensitivity. For Black men, the presence of depression is not just a health problem that needs to be managed, but rather, it is an issue that raises concerns about their value as men with their own families and communities. According to the participants from this study, Black communities want information to combat the stigma so that from an early age Black men will learn how to talk about their feelings, know that it is okay to talk about their feelings, and trust that others will not hold it against them if they do.
Footnotes
Acknowledgements
We would like to acknowledge Rosalyn Denise Campbell, Antonette King, and Karryll Winborne for their contributions to this project and the study participants who shared their stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by the Sisters Fund for Global Health, awarded to the lead investigator (Watkins) by the Institute for Research on Women and Gender (IRWG) at the University of Michigan.