
Abstract
The purpose of this study was to explore attitudes about condoms that may affect condom use by heterosexual men ages 50 and older who were sexually active and currently using prescribed oral phosphodiesterase type 5 inhibitor medications (Viagra®, Cialis®, or Levitra®) for treatment of erectile dysfunction. The study was part of a larger study that explored the need for safer-sex health promotion and education for these men. Fifty men completed factor subscales of the Condom Attitude Scale. Subscales were scored and analyzed. Positive factors were found with regard to the Interpersonal Impact, Inhibition, Perceived Risk, Perceived Seriousness, and Global Attitudes subscales. Factors with negative or neutral responses included the Effect on Sexual Experience, Relationship Safety, and Promiscuity subscales. Independent t tests revealed no differences between married and nonmarried men for the mean score on any of the subscales, but there was a difference on the Global Attitude Scale, with younger men having a more positive global attitude than older men. Study findings can be used in the development of health promotion educational activities on condom use as a safer-sex practice.
Keywords
Background and Significance
More than 150 million men around the world are estimated to have erectile dysfunction (ED), which results in problems with sexual activities due to the inability to achieve and maintain an erection sufficient to permit satisfactory sexual intercourse (Coward & Carson, 2008). The use of oral phosphodiesterase type 5 (PDE5) inhibitor medications, such as sildenafil (Viagra®), has changed the medical management of ED and allowed men with ED to resume and once again enjoy sexual activity (Dorsey, Keel, Klavens, & Hellstrom, 2010; Karlovsky, Lebed, & Mydlo, 2004).
Viagra received Food and Drug Administration approval in 1998; by 2005, more than 750,000 physicians had prescribed Viagra for more than 23 million men (Jackson, Gilles, & Osterloh, 2005). A study of 899 men who filled first-time prescriptions for Viagra during the initial 24-week period when the drug became available documented that users were between 45 and 74 years of age (Harrold et al., 2000). Use was highest among men ages 55 to 64 years, and more than 60% of Viagra users filled a second prescription within 3 months. A Veterans Administration study of low-income patients showed that clients perceived the benefit of Viagra to outweigh the cost of Viagra. Study participants with a self-reported need for Viagra responded that they were willing to make a higher co-payment ($5.40 for 4 Viagra pills) than the current Veterans Administration maximum co-payment of $2.00, if Viagra was made available (Yu et al., 2001).
However, the use of ED drugs such as Viagra, tadalafil (Cialis®), and vardenafil (Levitra®) has been implicated in the spread of HIV, particularly for men who have sex with men (MSM; Sanchez & Gallagher, 2006; Swearingen & Klausner, 2005). Viagra use by MSM was reported to be associated with unsafe sexual practices, including greater numbers of recent sex partners, higher levels of unprotected anal sex with an HIV-positive partner, and higher rates of sexually transmitted disease (STD; Chu et al., 2003; Ciesielski, 2003; Kim, Kent, & Klausner, 2002). Because of these concerns, the National Institute of Mental Health convened a conference in 2005 to explore the use of ED drugs and associated risk for HIV and other STDs. A conference recommendation was the need for further studies that examined safer-sex practices and sexual risk factors for specific groups, including risk among heterosexual men (Rosen et al., 2006).
Older men may be at risk for sexually acquired HIV or other diseases because they lack factual knowledge of HIV/STD transmission and may not perceive themselves as at risk and/or susceptible to HIV or STDs (Altschuler, Katz, & Tynan, 2004; Falvo & Norman, 2004; Palmer, 2000; Paniagua, 1999). Therefore, older men may not use or understand the need to practice safer sex. Rose (1995) used the health belief model (HBM) as a framework for a study of HIV/AIDS and older adults and reported that participants did not believe themselves to be susceptible to HIV, felt that AIDS was a disease of younger people that did not affect older adults, and did not use condoms. Maes and Louis (2003) reported similar findings in their survey of older adults using questions derived from the HBM. Although respondents recognized the seriousness of AIDS, the respondents did not believe that they were susceptible to the disease, even though 10% indicated sexual activity outside of a long-term relationship. Gott’s (2001) study of men above the age of 50 years documented that many participants reported that they had not received much information on HIV and STDs, and 7% engaged in behaviors that placed them at risk for a STD.
An important component of safer-sex practices is the consistent use of condoms during all sexual encounters, which may not be the practice among heterosexual men. A study of heterosexual men ages 50 to 70 being treated at an STD clinic in Singapore revealed that more than 25% of the sample intermittently used Viagra, did not always use condoms, and felt that condoms affected sexual performance (Tan, Wong, & Chan, 2006). Smith and Christakis (2009) identified an association between diagnosis of an STD and older men who were widowed (but not older women who were widowed). The largest effect was found 6 months to a year after the death of the wife, and the effect for men was larger in the years after the approval of Viagra. The study authors recommended that clinicians need to address sexual health issues for older adults, particularly for older men who were widowers and were using prescribed ED drugs (Smith & Christakis, 2009).
A review of the literature revealed that when men are initially prescribed ED drugs, information is given on dosage, side effects, and when to contact a health care provider for serious adverse effects such as priapism. The mnemonic “EPOCH” was used to describe methods to optimize responses to PDE5 therapy: Ensure realistic expectations of therapy by evaluating and educating; Prescribe an individualized treatment based on the couple’s needs and preferences; Optimize the drug dose/regimen and revisit key educational messages at follow-up visits; Control for comorbidities by strategies such as lifestyle counseling, medications, and/or referrals; and Help patients and their partners to seek other forms of therapy if they have decided not to use a PDE5 inhibitor (Sadovsky et al., 2011; Sadovsky, Brock, Gutkin, & Sorsaburu, 2009). However, only a few studies or articles were found that noted the need to discuss safer-sex practices with heterosexual or older men using prescribed ED drugs to prevent STDs including HIV (Cook et al., 2010; Hellstrom, 2010; Jena, Goldman, Kamdar, Lakdawalla, & Lu, 2010; Paniagua, 1999; Smith & Christakis, 2009). A finding in a study by Altschuler et al. (2004) was that older adults prefer HIV prevention education to be presented by health care providers.
The purpose of this study was to explore attitudes about condoms that may affect condom use by heterosexual men ages 50 and older who were sexually active and currently using prescribed oral PDE5 inhibitor medications (Viagra, Cialis, or Levitra) for treatment of ED. This study was part of a larger investigation that explored the need for safer-sex health promotion and education for this group of men. Concepts from the HBM (Rosenstock, Strecher, & Becker, 1988) served as the conceptual framework for the study. The HBM contends that people are likely to follow health recommendations if they are motivated about their health and if they believe they are susceptible to an ill health condition (perceived susceptibility), that the occurrence of that condition would have serious impact on their lives (perceived seriousness), that following a particular set of health recommendations would be beneficial in reducing either their susceptibility to or the severity of the condition, and that the psychological benefits of following the health recommendation outweighs its cost. Denial in any of these areas results in a lack of health seeking behavior. Specific concepts used from the HBM for this study were cost and benefit, perceived risk/ susceptibility, and perceived seriousness. The study also explored general attitudes and beliefs about condoms and condom use.
Method
Design and Instruments
This was a descriptive exploratory study to examine factors that may affect older men’s use of condoms. The instruments used were subscales from the Condom Attitude Scale (CAS; Sacco, Levine, Reed, & Thompson, 1991). The CAS was developed based on attitudes related to condoms as an AIDS-relevant behavior. Reliability for the CAS was supported by coefficient alpha estimates of .91 and .92 (Sacco et al., 1991). Test–retest reliability was established by administering the CAS to 322 participants and then readministering the CAS 3 to 4 weeks later. The results were r = .86 (Sacco et al., 1991). The CAS was originally developed with a convenience sample of heterosexual college students (Sacco et al., 1991) and was later used in a study of MSM and bisexual men (Sacco & Rickman, 1996).
During the instrument development stages of the CAS, factor analysis of the initial items used for the CAS indicated several attitude factors, which were developed into subscales of the CAS. Items on the subscales are rated on a 7-point scale from 0 (strongly disagree) to 6 (strongly agree). Although a total CAS score can be computed, scoring and analysis of each of the subscales is important because the individual subscale scores reveal more than the total scale score with regard to the relationship between condom attitudes and condom use (W. P. Sacco, personal communication, March 2012). Scoring is done by adding the participant’s response to each subscale item. Some items in each subscale are negatively worded, indicating a negative attitude toward condom use. These items are reverse scored. Higher scores for any of the subscales reflect a more positive attitude toward condoms. Lower scores on a subscale would reflect a negative attitude toward condoms in relation to that factor, which could serve as a deterrent to condom use.
Interpersonal Impact Subscale
The Interpersonal Impact Subscale has 11 items and is rated on a 7-point scale from 0 (strongly disagree) to 6 (strongly agree). The response of neither agree nor disagree is scored as a 3. Possible scores range from 0 to 66. A person who responded in a neutral manner (i.e., neither agreed nor disagreed) to all subscale items would obtain a score of 33. Higher scores (i.e., scores above 33) reflect more positive attitudes toward condom use with partners in relation to interpersonal impact.
Effect on Sexual Experience Subscale
The Effect on Sexual Experience Subscale is composed of 10 items. Since this study specifically explored perceptions of men with ED, Item 8 (“Condoms are clean”) was substituted with an item on loss of erection, “You could lose your erection by putting on a condom.” Possible scores for this subscale range from 0 to 60. Lower scores reflect more concerns about using condoms regarding their perceived negative effects on sexual experience.
Inhibition Subscale
The Inhibition Subscale has four items, and possible scores range from 0 to 24. Lower scores on this subscale would reflect inhibitions about purchasing or carrying condoms.
Perceived Risk Subscale
The Perceived Risk Subscale contains six items, and possible scores range from 0 to 42. Higher scores reflect a higher perception of risk, which may have a positive effect on condom use.
Global Attitude Subscale
The Global Attitude Subscale has nine items. The term global attitudes is related to the original research on gay and bisexual men, which found that unsafe sexual practices were related to the presence of a global negative attitude about condom use (Stall, Coates, & Hoff, 1988). Possible scores range from 0 to 54. Higher scores reflect more positive general attitudes and beliefs toward condoms.
Promiscuity Subscale
The Promiscuity Subscale includes three items, and possible scores range from 0 to 18. Higher scores reflect more positive attitudes toward condoms, whereas lower scores reflect negative perceptions of the association between condoms and promiscuity.
Relationship Safety Subscale
The Relationship Safety Subscale has five items, and possible scores range from 0 to 30. Higher scores indicate a more positive attitude toward using condoms in association with the perception of safety related to the status or potential status of the relationship.
Perceived Seriousness
To assess the concept of perceived seriousness of HIV in older adults, one item was added for this study: “Getting HIV is a very serious health problem if you are an older adult.” Possible scores range from 0 to 6. Higher scores reflect higher concern regarding the seriousness of HIV in older adults, which may have a positive effect on condom use.
Subscales of the CAS were used for this study to measure specific concepts from the HBM. The Interpersonal Impact Subscale, the Effect on Sexual Experience Subscale, and the Inhibition Subscale were used to measure the concepts of perceived costs (i.e., burden, inconvenience, time) and benefits (i.e., personal safety, personal satisfaction, partner safety) related to condoms and condom use. The Perceived Risk Subscale was used to measure the concept of perceived risk and susceptibility, and the one item on perceived seriousness was used to assess the concept of perceived seriousness. The Global Attitude Subscale, the Promiscuity Subscale, and the Relationship Safety Subscale were used to measure general attitudes, knowledge, and beliefs about condoms and condom use (see Figure 1).

Conceptual framework: Heterosexual ED drug users and condom use practices for HIV/STD prevention (adapted from the health belief model).
Sample
After receiving approval from the university institutional review board for the protection of human subjects, sexually active heterosexual men ages 50 and older who had been prescribed ED drugs were recruited for the study. The final sample size was 50 men.
Procedure
A variety of strategies were used to facilitate recruitment of older heterosexual men, including changing the study name from “The Viagra Study” to “The Men’s Health Study” and having male nurse practitioner students serve as study team members in the role of study recruiters and interviewers (Jones, Patsdaughter, & Martinez Cardenas, 2011). Participants were recruited by flyers posted at community venues where men were thought to gather (e.g., parks, clubs, bars, sporting good stores, hardware stores). Community flyers listed a number to call for further information on the study. Several physicians also agreed to assist with the study by telling their eligible clients about the study. Potential participants recruited from the physicians’ offices received a follow-up phone call from study team members. All potential participants who indicated interest in the study were mailed an informed consent form and a packet of study instruments, which included an investigator developed sociodemographic questionnaire and the CAS subscales. Participants were informed that, after sending back the signed consent form and completed study packet, a brief follow-up phone interview of less than 30 minutes would be conducted to complete additional instruments for the larger study. Participants who sent back the study packets and completed the phone interview were then mailed a $25 gift card as a measure of appreciation for their participation.
Data Analysis
Data from the CAS were entered into SPSS version 17.0. Reverse scored items were recoded and exploratory analyses were conducted to search for missing data and outliers. Analysis of sociodemographic data consisted of descriptive statistics (i.e., frequencies, percentages, means, and SDs). Analysis of the subscale data included calculation of a score for each subscale (mean, range, and SD). Descriptive statistics (frequencies, percentages, means, and SDs) were also computed for each item on each subscale. Independent t tests were used to compare the mean subscale scores for married versus nonmarried and for younger (50-59) men versus older (60 and older) men.
Results
Sociodemographic Characteristics
The mean age of the men was 60.56 (N = 50). Although more than half (n = 28; 56%) of the men were aged 50 to 59 years, 14 men (28%) were aged 60 to 69 years and 8 men (16%) were aged 70 to 79 years (see Table 1). A majority of the men self-reported as being White (n = 36; 72%), and a majority (n = 35; 70%) had some college or graduate education. Slightly more than half of the men were currently married (n = 27; 54%); the remainder (n = 23; 46%) included men who were single, engaged, separated, divorced, or widowed. Many of the men (n = 31; 62%) were currently employed. A majority of the men (n = 38; 76%) were taking Viagra, and a majority of the men (n = 40; 80%) had been using prescribed ED drugs for 3 years or longer.
Sociodemographic Characteristics of the Sample (N = 50).
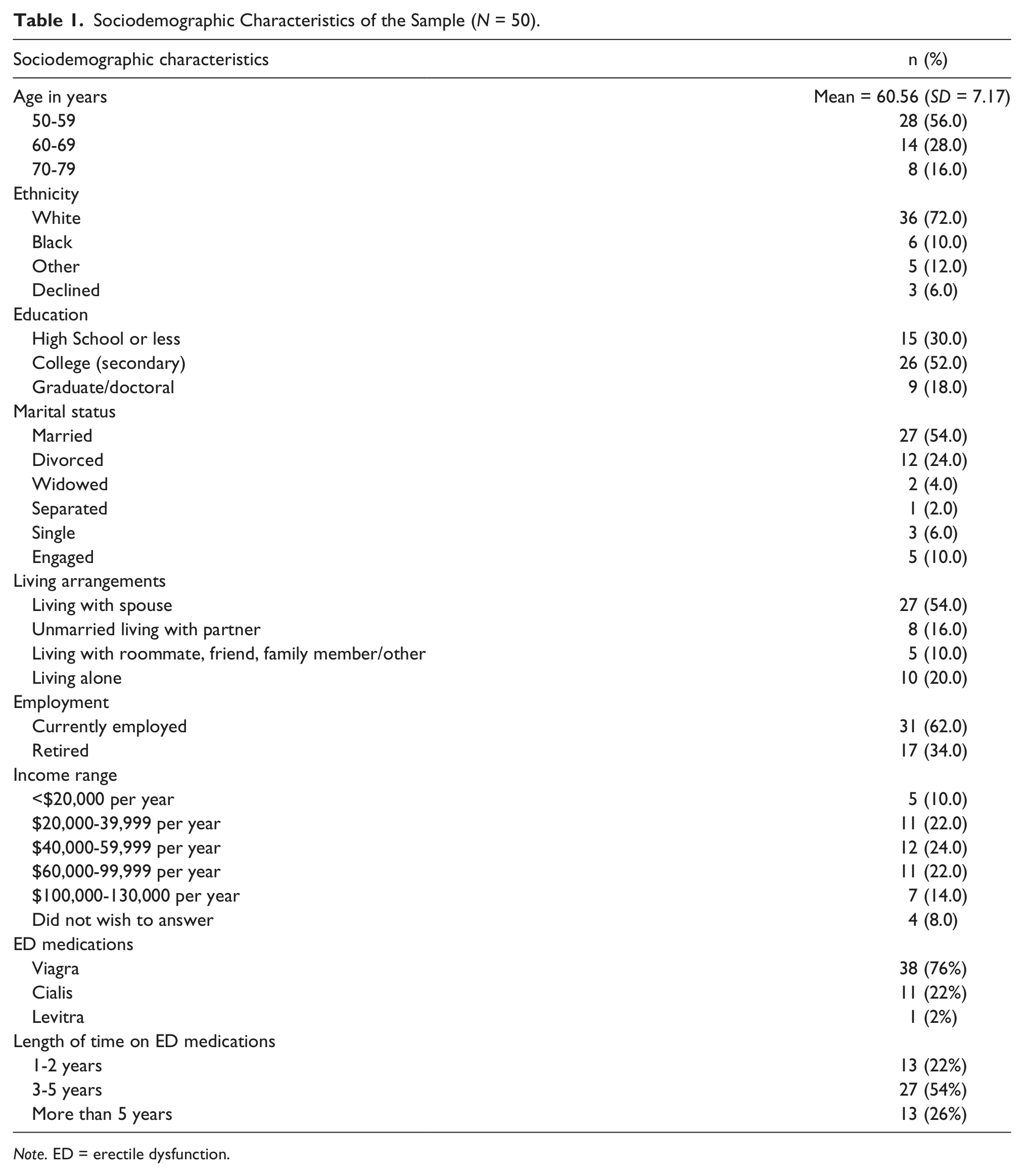
Note. ED = erectile dysfunction.
Subscale Findings
Table 2 is a summary table that displays the number of items per subscale, the range of scores, the mean score, and the standard deviation. Each item on every subscale was then assessed.
Summary Statistics on CAS Subscales (N = 50).

Note. CAS = Condom Attitude Scale.
Interpersonal Impact
The mean score for Interpersonal Impact was 47.90 (SD = 17.18), indicating that for this sample of men, a suggestion by a partner to use a condom was perceived in a very positive way. For example, a majority (n = 40; 80%) of the participants agreed with the statement “If my partner suggested using a condom, I would respect her/him.” Condoms were also perceived as a safety strategy. A majority (n = 35; 70%) agreed with the statement “Condoms create a sense of security.” Participants’ responses for each item are listed in Table 3.
Frequencies and Percentages for Interpersonal Impact Subscale Items (N = 50).

Effect on Sexual Experience
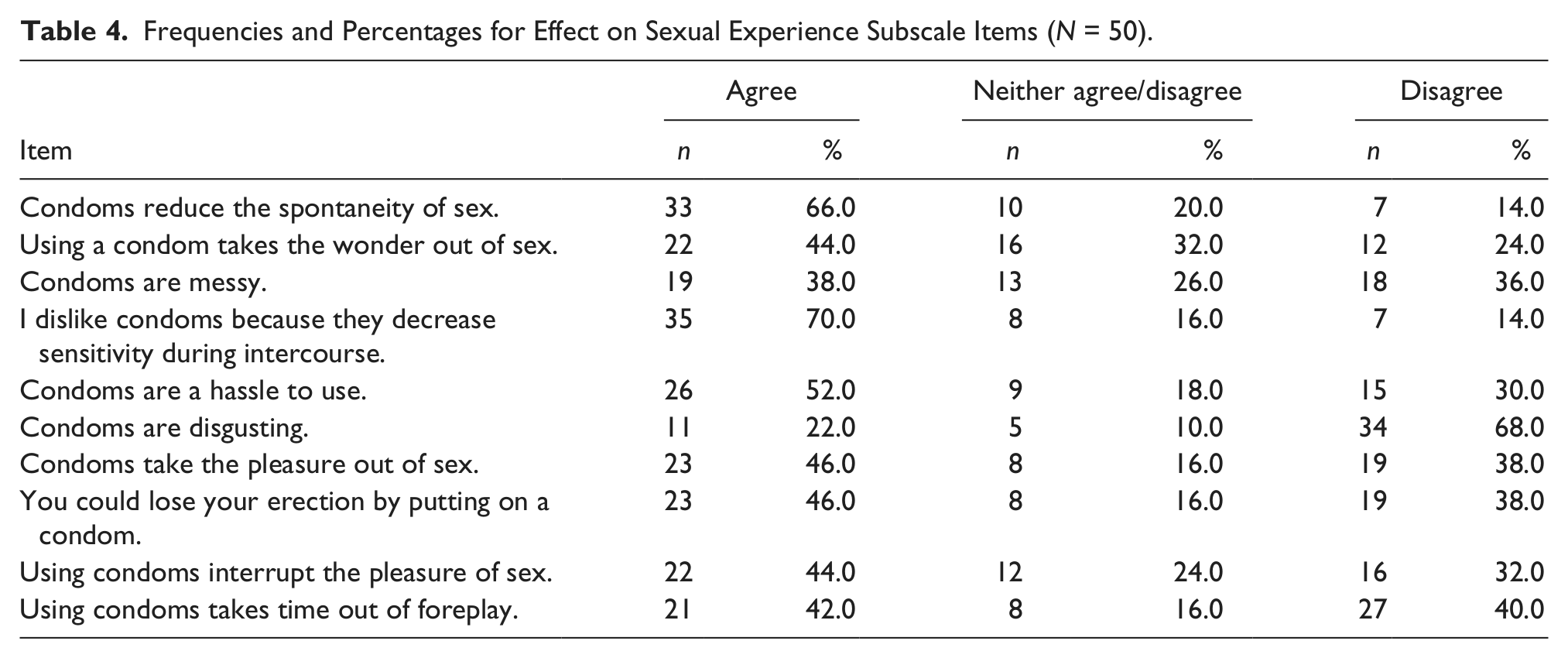
Unlike the interpersonal impact scores, scores on this subscale revealed that participants in this sample had somewhat negative attitudes regarding the effect of condoms on sexual experience (see Table 4). The mean score was 28.08 (SD = 15.86). A majority (n = 35; 70%) of the participants agreed with the statement “I dislike condoms because they decrease sensitivity during intercourse,” whereas two thirds (n = 33; 66%) of the participants agreed with the statement “Condoms reduce the spontaneity of sex.” Almost half (n = 23; 46%) of the participants agreed with the statement “You could lose your erection by putting on a condom.”
Frequencies and Percentages for Effect on Sexual Experience Subscale Items (N = 50).
Inhibition
Participants’ scores ranged from 9 to 24, with a mean score of 19.44 (SD = 4.16), reflecting low inhibition toward condoms. A majority (n = 35; 70%) of participants agreed with the statement “I am not inhibited about buying condoms.” A majority (n = 40; 80%) of participants disagreed with the statement “I’m too old fashioned to buy or carry a condom,” and a majority (n = 41; 82%) also disagreed with the statement “I’d be too embarrassed to buy condoms.” Last, a majority (n = 43; 86%) of participants disagreed with the statement “I wouldn’t keep condoms at home because someone might find out I was having sex.”
Perceived Risk
Participants’ scores ranged from 0 to 36, with a mean score of 26.16 (SD = 10.12), which demonstrated a concern about the risk of contracting HIV and other STDs. A majority (n = 31; 62%) of the participants agreed with the statement “I am concerned about catching HIV/AIDS or some other sexually transmitted disease” (see Table 5).
Frequencies and Percentages for Perceived Risk Subscale Items (N = 50).

Perceived Seriousness
As noted with perceived risk, participants were also concerned with the seriousness of HIV in older adults. Participant scores ranged from 0 to 6, with a mean score of 5.26 (SD = 1.57).
Global Attitude
Participant scores ranged from 12 to 54, with a mean score of 43.76 (SD = 9.52). Participants were generally positive in relation to attitudes and beliefs about condoms. For example, a majority (n = 40; 80%) of the participants disagreed with the statement “People who use condoms are wimps,” and a majority (n = 40; 80%) agreed with the statement “A condom should be used when you have anal sex” (see Table 6).
Frequencies and Percentages for Global Attitude Subscale Items (N = 50).

Promiscuity
Participant scores ranged from 1 to 18, with a mean score of 12.56 (SD = 4.40). This subscale had the highest amount of participants who chose a neutral response (neither agree nor disagree) for all items. For example, while 28 (56%) of the participants disagreed with the statement “People who carry condoms would have sex with anyone,” 15 (30%) of the participants neither agreed nor disagreed. Additionally, while 32 (64%) of the participants disagreed with the statement “People who use condoms sleep around a lot,” 14 (28%) of the participants neither agreed nor disagreed. Last, while 33 (68%) of the participants disagreed with the statement “People who carry condoms are just looking for sex,” 13 (26%) of the participants neither agreed nor disagreed.
Relationship Safety
Participant scores ranged from 0 to 30, with a mean score of 12.35 (SD = 8.01). For more than half of the participants in this study, factors such as monogamy, knowing enough about the person to trust her/his word about their past, and a long-term relationship with the same person negated the need to use a condom. However, intent to marry someone and being pretty sure that a potential partner was STD free was not perceived as negating the need to use a condom (see Table 7).
Frequencies and Percentages for Relationship Safety Subscale Items (N = 50).

A t test was used to compare the subscale mean scores between married and nonmarried men, and no difference was found. A t test was then done to compare the subscale Mean scores between younger (50-59) men and older (60 and older) men. The only difference that was identified was for the Global Attitude Subscale, with younger men having a higher mean score (M = 46.18, SD = 6.49) than older men (M = 40.68, SD = 11.83), t(48) = 2.09, p = .04.
Discussion
The purpose of this study was to explore attitudes about condoms that may affect condom use by heterosexual men ages 50 and older who were sexually active and currently using prescribed oral PDE5 inhibitor medications (Viagra, Cialis, or Levitra®) for treatment of ED. The study revealed both positive findings and findings of concern. Positive attitudes were found with regard to interpersonal impact, inhibition, perceived risk, perceived seriousness, and global attitudes. There were negative and neutral findings for effect on sexual experience, relationship safety, and promiscuity. No differences were found between married and nonmarried men for the mean score on any of the subscales. When a comparison was made between younger (50-59) and older (60 and above) men, the only difference was on the Global Attitude Scale, with younger men having a more positive global attitude than older men. The findings in this study have implications in the promotion of safer sexual practices and the prevention of STDs for older men using prescribed ED drugs.
Interpersonal impact results revealed that this group of men was amenable to a partner’s suggestion of the use of condoms. A majority of men responded in a positive way to the statements “If a partner suggested using a condom, I would feel grateful” and “If a partner suggested using a condom, I would feel relieved.” The finding that older men are not only amenable, but even relieved by their partner’s suggestion to use a condom, has educational implications for both men and women.
The men in this study also responded positively to the statement “Condoms create a sense of security.” This finding could possibly be related to the fact that for this group of older men, condoms are perceived as preventing pregnancy as well as preventing an STD. This finding may be useful as a component of an educational activity focusing on condom use as a way to “stay safe and stay healthy” in relation to prevention of HIV and other STDS. For example, Altschuler et al. (2004) recommended designing HIV/AIDS education programs for older adults as “part of a health series” as opposed to a “stand-alone program.” This finding served as the basis for a successful health care seminar for older adults, called “No One Is Immune,” that was developed to educate older adults about HIV/AIDs, but was framed within a day-long seminar that focused on sexuality, sexual health, and medications (Orel, Stelle, Watson, & Bunner, 2010).
Inhibition can be a potential barrier to condom use by older men, in relation to purchasing or carrying condoms. However, inhibition was not a problem for this group of older men. A majority of the men in the study agreed with the statement “I am not inhibited about buying condoms” and disagreed with the statement “I’m too old fashioned to buy or carry a condom.” This suggests that men are likely to have or be prepared to buy a condom in anticipation of sexual activity, indicating an area for positive behavioral reinforcement of a safe and healthy sexual practice.
In relation to perceived risk, a majority of men in this study were concerned with the possibility of contracting HIV or an STD. This older population of heterosexual men may be very familiar with hearing of the risk of STDs. For example, in the mid to late 20th century in the United States, it was a requirement in many states to have a venereal disease test prior to getting a marriage license. However, not every participant was concerned about contracting either an STD or HIV. This might be attributed to the historical stigma of HIV, which has often been associated with gay men. Heterosexual men may perceive themselves to not be at risk for HIV. Additionally, older men may perceive HIV to be a problem for only young people. These findings reinforce the need to educate men that HIV is a sexually transmitted disease that is not restricted to any one group.
The men in this study, as noted by the responses to the item on perceived seriousness, were also concerned about the seriousness of HIV in older adults. In light of this finding, and in combination with the findings on perceived risk, men in this population may be more open to receiving health promotion education that provides strategies, such as proper condom use to prevent STDs including HIV.
Younger men (ages 50-59) were more positive than older men (60-69) men with regard to global attitudes about condoms. However, for both groups, global attitudes toward condoms were generally positive. For example, four fifths of the men in this study disagreed with the statement that “condoms are for wimps” and an equal number agreed with the statement that “a condom should be used when you have anal sex.” These divergent statements demonstrate condom acceptance from both psychosocial and physical perspectives. The latter finding points to the need to discuss both anal and vaginal intercourse as part of safer sex educational activities with heterosexual men. Although safer anal sex is commonly discussed with MSM, anal sex should be discussed with all sexually active men. Education on how to apply and remove condoms during both vaginal and anal sex may be needed. A study of heterosexual men ages 18 to 66 found that condom use problems were common, and the researchers noted the need for the development of prevention programs for heterosexual men that focused on condom use errors and problems for penile–anal as well as penile–vaginal intercourse (Topping et al., 2011).
The findings from this study also revealed negative attitudes toward condoms. In particular, men in the study were especially negative toward condoms with regard to effects on sexual experiences. A notable number of the men in this study reported that condoms (a) decreased sensitivity during intercourse, (b) reduced the spontaneity of sex, and (c) are a hassle to use. These are important findings. To overcome these negative attitudes, health promotion activities will need to demonstrate that condom use can be pleasurable, fun, romantic, and erotic.
A study on sexual pleasure among heterosexual men during condom-protected vaginal sex found that sexual pleasure increased in conjunction with specific condom-related perceptions, along with specific relational and physiological factors (Hensel, Stupiansky, Herbenick, Dodge, & Reece, 2012). A study by Randolph, Pinkerton, Bogart, Cecil, and Abramson (2007) found that college-age men who believed that condoms reduced pleasure were less likely to use condoms. The study authors noted that their study findings supported previous research findings that pleasure is a more important factor for men in the decision to use or not use condoms than it is for women. The study authors recommended a new form of condom education, promotion, and marketing that highlighted the pleasure benefits of condoms, such as “condoms’ ability to prolong sexual intercourse, thus increasing psychosexual tension, and ultimately sexual pleasure.”
An educational strategy focused on changing negative perceptions about condoms could be to demonstrate to men the newer varieties of condoms available on the market such as flavored, ribbed, and glow-in-the-dark condoms. There are also new latex condoms that are thinner, feel more natural, and have a decreased latex odor. Marketing strategies can also be tailored from condom campaigns developed for younger populations, such as the United Nations Population Fund’s CONDOMIZE! campaign. During the 2012 International AIDS Conference in Washington DC, the CONDOMIZE! campaign used a variety of colorful visuals, lively music, fast-paced dance scenes, and interactive activities such as the “Lube Tasting Bar” to promote condoms as an effective way to prevent HIV (http://www.thecondomizecampaign.org).
Additionally, safer-sex educational activities need to be developed that are geared toward single or widowed older men. This is an important concept since almost half of the men in the study sample were not married or were no longer married and could potentially be actively involved with several new partners. A strategy could be to develop media scenarios depicting an older man and woman discussing the initiation of a sexual encounter and negotiating condoms as a romantic or erotic part of that encounter.
Many men in the study were concerned about losing an erection if they put on a condom. This finding is important because the men in this study had sought out medical care to obtain medication for treatment of ED. Men using prescribed ED drugs may be unwilling to use a condom if they fear it will interfere with their ability to sexually perform. As noted in the HBM, if the benefit does not exceed the cost of behavior modification, behavior will not be changed. For that reason, safer-sex education for men using prescribed ED medications may present more challenges than for men in general. Hensel et al. (2012) found that erection problems decreased sexual pleasure. Health promotion educational activities must address the psychosocial implications of ED as well as the goal of overcoming any potential fears or concerns regarding use of condoms. An additional strategy for these men could be to discuss having their partner use a female condom, if the men were reluctant to use the male condom due to fears of losing an erection.
Concerns were also noted with responses regarding relationship safety. Responses demonstrated that the men in this study perceived factors such as monogamy, knowing enough about the person to trust her/his word about their past, and a long-term relationship with the same person to negate the need to use a condom. Part of a health promotion strategy could be to suggest that in any relationship, although trust is important, partners may not always be candid about their past. Although monogamy was perceived as a situation that negated the need to use a condom, intent to marry someone was not perceived as negating the need to use a condom. This could possibly reflect that intent to marry is not a decisive factor in condom use for older men.
Last, a concern is noted with the neutral responses from participants related to association of condoms with promiscuity, which appeared to be contrary to the findings from the Interpersonal Impact subscale. This finding could reflect a level of ambiguity regarding what constitutes promiscuity. This divergence might also possibly relate to the phenomenon of “the other” whereas the men read the question and answered it in relation to the behavior of others but not in relation to themselves or their partners. A potential way to address this concern could be to focus on condoms as security (“stay safe and stay healthy”), as has been previously noted.
Potential health care policy implications include developing guidelines that address safer-sex practices for all men who are prescribed ED drugs. These guidelines should address the risk for sexually acquired HIV/STDs, current and past partners/relationship status, birth control methods routinely used, and the subject of concurrent partners. Additionally, educational programs need to be developed for men who are prescribed ED drugs and for health care providers that prescribe these drugs. Last, the Centers for Disease Control and Prevention (CDC) has issued revised recommendations for HIV testing for adults (CDC, 2006). The CDC recommends HIV screening in all health care settings for all patients ages 13 to 64. Since some sexually active men in this study were above the age 64 years, it might be pertinent to expand the CDC recommendation to HIV screening for all sexually active persons and not limit this recommendation by specific age groups.
Study Limitations
This study presents new information on attitudes about condom use among older heterosexual men using prescribed medications for treatment of ED. However, a limitation of the study is the small sample size. The convenience sample was drawn from only one location, limiting the generalizability of the findings to the broader population of older heterosexual men. Further research is needed with a larger sample of men from multiple sites to determine if there are differences between and among other subsets of older men in general, such as heterosexual versus MSM and bisexual men, younger versus older men, and men from different minority groups. Studies could also explore condom attitudes and safer-sex practices in relation to birth control methods currently used, commitment to existing relationships, and information about concurrent partners. Additionally, the men in this study were using ED medications that were prescribed for them by health care providers. Further studies might explore for differences between men using prescribed versus nonprescribed (i.e., obtained from friends or other persons, or from online sources) ED drugs.
Conclusion
When men are prescribed ED drugs, information is given on dosage, side effects, and when to contact a health care provider for serious adverse effects such as priapism. However, sexual health information related to HIV and STD transmission and prevention is also needed as part of an individualized, comprehensive safer-sex education program. Findings from this study shed light on the attitudes of older heterosexual men using prescribed ED drugs with regard to condoms and how those attitudes may influence their sexual beliefs and practices. This information can be used by health care providers and other health care professionals (i.e., social workers, counselors, case managers) who work with older men. Findings from this study also provide important insights that could be used to explore the development of safer-sex health promotion educational activities geared specifically toward older heterosexual men who have been prescribed ED drugs for ED.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant #SO6GM08205 from the National Institutes of Health, National Institute of General Medical Sciences, through the Minority Biomedical Research Support (MBRS) Support of Competitive Research (SCORE) program.