
Abstract
Extensive research has focused on understanding family dynamics of men with prostate cancer. However, little qualitative work has examined the role of family ties on men’s prostate cancer decisions across the spectrum of screening, diagnosis, and treatment. Using data from a larger study, we qualitatively explored the influence of family ties on men’s prostate cancer decisions. Semistructured interviews were conducted with men ages ≥50 (N = 64), and data were analyzed using a grounded theory approach and a series of immersion/crystallization cycles. Three major themes of spousal/family member influence were identified: (a) spousal/family member alliance marked by open communication and shared decision making, (b) men who actively opposed spouse/family member pressure and made final decisions themselves, and (c) men who yielded to spouse/family member pressure. Our findings provide insights into men’s relational dynamics that are important to consider for the shared decision-making process across the prostate cancer spectrum.
Family ties play an important role in individuals’ health status and health-seeking behavior (Berkman, 2000; Haines & Hurlbert, 1992; Seeman, 2000; Umberson, 1992; White, Philogene, Fine, & Sinha, 2009). Family ties—typically defined as relations based on blood ties, marriage, or adoption—can provide a conduit of resources to the family member who has a health need or faces a health care decision. Certain resources provided by family members that may affect health outcomes include emotional support, instrumental support (such as financial assistance), or informational support (Berkman, 2000; Seeman & Berkman, 1988). One pathway from family ties to health is through the encouragement of health-promoting behaviors. Here, research has demonstrated that women commonly monitor the health behavior of their family members (Umberson, 1992) and play a key role in ensuring that their family members seek appropriate medical care (Bevan & Pecchioni, 2008; Ferrante, Shaw, & Scott, 2011).
More specifically, the role of family ties is important for understanding the lives of men with prostate cancer. In fact, prostate cancer has been referred to as a “relationship disease” because of the concurrent impact it has on the spouse and other family members as well as the patient (Gray, Fitch, Phillips, Labrecque, & Klotz, 1999). Much of the research in this area has targeted the psychosocial effects on women living with men diagnosed with prostate cancer (Banthia et al., 2003; Cliff & MacDonagh, 2000; Couper et al., 2006; Kershaw et al., 2008; Kornblith, Herr, Ofman, Scher, & Holland, 1994; Manne & Badr, 2008; Manne, Badr, Zaider, Nelson, & Kissane, 2010; Resendes & McCorkle, 2006; Segrin & Badger, 2010). Additional research has sought to understand the impact of prostate cancer on couples’ relationships (Garos, Kluck, & Aronoff, 2007; Harden, Northouse, & Mood, 2006; Illingworth, Forbat, Hubbard, & Kearney, 2010), issues surrounding family members as caregivers (Bevan & Pecchioni, 2008; Given & Sherwood, 2006; Kim & Given, 2008; Pitceathly & Maguire, 2003), and the information needs of partners and family members of cancer patients (Adams, Boulton, & Watson, 2009; Arguelles et al., 2010).
Considering the possible phases of study surrounding prostate cancer–related decision making—from screening, to diagnosis and treatment, to recovery and survivorship—very few studies have addressed the role of family members on men’s prostate cancer screening decisions (Ferrante et al., 2011; Meiser et al., 2007; Volk et al., 1997; Volk et al., 2004; see Figure 1).
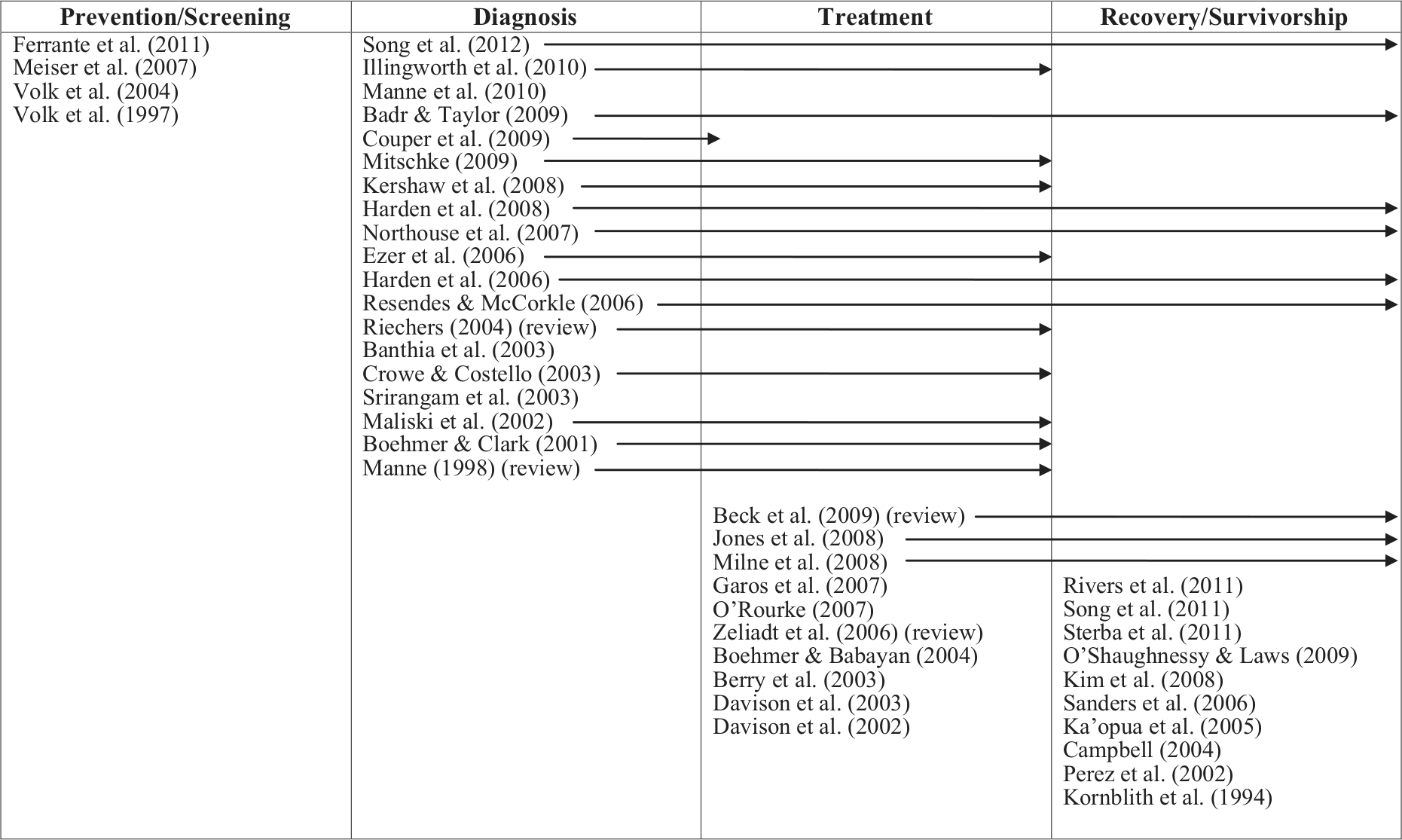
Studies on prostate cancer and family ties by decision-making phase.
Although men often turn to a loved one when they are experiencing symptoms and will seek medical advice when prompted by family members (Bevan & Pecchioni, 2008; Ferrante et al., 2011), there is some evidence that men prefer a no-screening strategy, whereas their wives prefer screening for their husbands (Volk et al., 1997; Volk et al., 2004). Other research has reported that men whose partners were highly involved in men’s screening decisions had a significantly higher uptake of prostate-specific antigen (PSA) testing compared with single men and men whose partners had low involvement (Meiser et al., 2007). Moreover, although quantitative evidence suggests that being married improves the likelihood that a man will be screened for prostate cancer (McFall & Davila, 2008; Merrill, 2001; Ross et al., 2004; Seo & Lee, 2010), significant questions remain regarding these family dynamics. Exploring how spousal/family member ties affect men’s screening behaviors requires qualitative investigations, which are currently limited in the literature.
As Figure 1 reveals, most studies have concentrated on the role of family members during the diagnosis, treatment, and survivorship phases. For example, Boehmer and Clark (2001) reported that, during diagnosis and treatment, the triadic interactions of doctor, patient, and spouse could be categorized into three types: partner excluded, doctor-initiated inclusion of partner, and spousal alliance. The same men who disclosed their health problems to their wives prior to diagnosis involved their wives in treatment decisions, thus suggesting that men’s diagnosis of prostate cancer did not change couples’ communication and decision-making patterns (Boehmer & Clark, 2001). A common finding across studies that focused on diagnosis and/or treatment was that: “no spouses were willing to accept responsibility for the ultimate decision; partners mainly supported patients and helped gather information” (O’Rourke, 2007). Understanding how family members influence men’s prostate cancer treatment decisions remains unclear (Zeliadt et al., 2006).
In this article, we present a qualitative analysis of family member influence on men’s prostate cancer screening, diagnosis, and treatment decisions. In doing so, we provide insights into some of the relational dynamics between men and their family members as men face various prostate cancer decision points. Little work has focused on family ties and prostate screening or qualitatively explored relational dynamics across this spectrum of prostate cancer decision making. Given the uncertainties men often face in making decisions over the course of these phases and the concurrent push for shared decision making, insights from this study may help optimize men’s health care experiences in this area. Moreover, this study may help health care professionals facilitate shared decision making with their patients regarding prostate cancer screening, diagnosis, and treatment by incorporating family members into these discussions.
Method
The data reported here are part of a larger study that was designed to qualitatively explore factors influencing men’s decisions regarding prostate cancer screening and treatment among men who were never screened or those who had an abnormal screening (Ferrante et al., 2011).
Study Sample
For the larger study, a purposive sample of men (N = 64) ages 50 years and older was recruited via community-based organizations and newspaper advertisements in northern New Jersey to participate in an in-depth interview. Our inclusion criteria were men who were never screened for prostate cancer or who had an abnormal screening and, subsequently, had a normal biopsy or cancer diagnosis. Men were excluded if they did not speak or understand English or Spanish. In four cases, we allowed joint husband/wife interviews because the men requested it, feeling that their wives would be helpful in recalling past health care decisions and experiences. All the joint interviews were with men who had abnormal biopsies.
The institutional review boards of University of Medicine and Dentistry of New Jersey, Cancer Institute of New Jersey, and U.S. Army Medical Research and Materiel Command approved the study protocol. All participants provided informed consent prior to the interview and received $30 on completion.
Data Collection
Four trained interviewers conducted semistructured, in-depth interviews with participants in English or Spanish. Questions were designed to elicit (as applicable) participants’ knowledge about prostate cancer and screening; feelings about prostate cancer screening; discussions with doctors about screening, diagnoses, and treatment; experiences with family members or friends regarding prostate cancer and screening; and personal health practices. Probes were tailored to specific interviews in order to elicit more detailed information on these topics. The open-ended interview format gave participants considerable freedom to discuss experiences that were important to them and describe factors they deemed to be important in their decision-making process rather than responding to issues or factors imposed by the researchers. Interviews lasted 30 to 90 minutes and were digitally recorded and transcribed verbatim.
Data Analysis
Transcriptions were imported into Atlas.ti (Scientific Software Development GmbH, Berlin, Germany), a software program that facilitates qualitative analysis. We used a grounded theory approach that involved a series of immersion/crystallization cycles (Borkan, 1999). Immersion/crystallization is an iterative process that is well suited for identifying patterns and connections in qualitative data sets (Borkan, 1999). Core steps in our analytic process included the following: initially, the research team (ES, JS, JF) held a series of meetings in which several interview transcripts were read line-by-line jointly and a set of preliminary emergent codes was developed. Group analysis continued until consensus was reached regarding the coding scheme and code definitions. We then independently analyzed the remaining data, reconvening regular group meetings to discuss interpretations and to refine coding schemes. To ensure reliability, all transcripts were independently read and coded by at least two research team members, and group consensus was used to resolve any differences in coding.
Once the coding process was completed, we used a second immersion/crystallization cycle in which data segments within codes were reread and analyzed to identify themes and patterns among the subjects in the study. At this stage, themes emerged as we focused on understanding the role of family members on men’s decision-making processes. As is common with qualitative analysis, we compared and contrasted each interview with our emergent themes (Strauss & Corbin, 1990). If data from an interview did not fit into an existing theme, this prompted the development of an additional theme. As our themes continued to crystallize by finding additional evidence from participants across the decision-making points, we gained greater insights into thematic commonalities and variations. We also explored (and report here) those instances where there was little or no evidence of a particular theme. Doing so provides a point of comparison across the relational dynamic themes in our data and may be of value for future research. An additional immersion/crystallization cycle incorporated efforts to identify negative or disconfirming evidence for our emerging interpretations by rereading the coded data and exploring potential alternative interpretations of the data. The quotations included here were selected to best illustrate our key findings.
Results
Demographic characteristics of the sample population (N = 64) are reported in Table 1. Most men were between 50 and 69 years of age, White, married, highly educated, and employed. All married men were in heterosexual relationships.
Characteristics of Participants.

Based on the interviews, three major themes were identified regarding spousal/family member interactions with men for prostate cancer screening, diagnosis, or treatment decisions: (a) spousal/family member alliance marked by open communication and shared decision making, (b) men who actively opposed spouse/family member pressure and made final decisions themselves, and (c) men who yielded to spouse/family member pressure. As a secondary analysis, not all participants spoke explicitly about the role of family ties on their prostate cancer decision-making processes. Table 2 reports the distribution of participants across our three themes for each decision point (n = 30). The main findings of our analysis reveal three different family dynamics, as well as variations in how these dynamics shaped men’s screening, diagnosis, and treatment decisions.
Breakdown of Themes by Prostate Cancer Decision Point.

Spousal/Family Member Alliance
Overall, there were relatively few spousal/family member alliances marked by open communication and shared decision making. In fact, there was no evidence of a spousal/family member alliance for men who never received screening. However, we did find such evidence among men with abnormal PSA levels and men diagnosed with prostate cancer. We explored the dynamics of the decision-making process for these alliances, thus providing an important point of comparison with the other themes.
A few men with abnormal PSA results described a spousal alliance regarding further diagnostic procedures. For example, one man (83 years old, Caucasian) indicated that his doctor told him,
It’s up to you what you want to do (regarding having a biopsy). You don’t have to do it because the growth is very slow when you reach a certain age.
At this point, his wife became increasingly important in the decision-making process. As she stated,
I’ve known people that have had it (prostate cancer). I’m up on a lot of medical things because I used to work in the field years ago. But I read everything I can now. I try to learn things.
In the absence of clear direction from the physician, she became an important resource for her husband by finding relevant information and regularly going to his doctor’s appointments with him to help ensure that their questions were answered for making further diagnostic decisions. This particular husband and wife communicated openly about what next steps he should take and jointly decided to continue with the biopsies.
A few men in our sample also described a spousal alliance for prostate cancer treatment decisions. Typically, the spousal alliance carried over from the diagnostic phase. For example, one man attributed his wife’s role as a nurse to be an important element of his health care. She reportedly first received his cancer diagnosis from the doctor and then shared it with him. He described her as being very supportive and an integral part of the diagnosis and treatment decision-making phases. Much like the decision-making process around diagnostic procedures, these men indicated the prominent role of their spouse when there was confusion around treatment options. For example, one man (62 years old, Caucasian) spoke about his experience of facing various treatment options:
Well it was actually enlightening and broadening in a sense that the first thing when I was diagnosed with prostate cancer was my urologist at that time who is a surgeon who does the open type of removal and . . . he recommended that I do surgery right away and not wait longer than 3 months. Um, and so I was thinking that’s what I should do but then I was talking to others and found out there was other options.
He added a rhetorical question:
From checking around, I became aware more and more of lots of different options. So that was good. But then it’s also confusing because there are many options and what is really the best and actually they all make claims of being very good but what has the bad side effects?
During this interview in which his wife was present, they indicated that together they chose watchful waiting for him for about 1½ years based on their knowledge that his cancer would be slow-growing and for fear of negative side effects. They eventually chose to proceed with surgery, articulating in the interview their decision-making process:
Once you treat it (prostate cancer) with the radiation it’s hard to remove the prostate so we ruled out the radiation approach. . . . The surgery approach was always there as the alternate to get rid of the prostate and, you know, absolutely get rid of the prostate cancer. Any of the others (treatment options) had the risk that the cancer could come back and progress to other parts of the body and things like that.
Speaking in this interview just 2 months after his surgery, he shared some distress they have been experiencing with urinary incontinence and negative sexual side effects. He added, “You [can] tell from my wife too that things are getting psychologically not so good.” Later, in the interview, his wife indicated her perceived connection to their treatment decision for him saying, “I feel like I’ve had surgery too.”
Men Who Opposed Family Pressure
Many men in our sample articulated opposition to family pressure for at least one of the decision points—screening, diagnostic procedures, or treatment for prostate cancer. Such opposition was articulated most frequently around treatment decisions.
In the two cases where men opposed family pressure to get screened, they expressed a personal health belief that being asymptomatic meant no action was required. For example, one man stated,
Why should I (get screened) if I feel healthy? My wife says it’s better to know, and I say I don’t agree with that. . . . I think that if I knew, it would bother me, which would create stress . . . and as long as I’m not feeling bad, I don’t do anything. (Age 63 years, Caucasian)
Another man (50 years old, Caucasian) explained that his daughter wanted him to get a PSA test but he told her “it ain’t gonna happen” despite having seen several friends die from prostate cancer. He elaborated that his daughter and mother were pressuring his father to get screened who was reportedly resistant as well. When asked directly “What if your father decided to get screened?” the subject responded “more power to him” and then said he still would not get screened because he did not want to give into family member pressure. Whereas some men who opposed such pressure acknowledged that the family members were doing so out of concern for their health, this particular man gave no such indication and viewed this pressure as an unhelpful annoyance.
Regarding diagnostic procedures, a few men expressed their views as the final decision maker when it came to their personal health care decisions. For example, one man articulated his thoughts about his wife’s role in the decision-making process for his two biopsies:
In both cases, I didn’t do it (get biopsied) without talking to her (his wife). Let me put it this way, they say a good lawyer never asks a question that he or she doesn’t know what the answer’s gonna be before you ask it, and . . . there was no doubt in my mind about what her decision would be, which was consistent with my own decision as well. If my wife had resisted it. . . . I probably would’ve done it anyway. But I just knew when I spoke to her that she would understand and knew that this is something that just had to be done. (Age 65 years, Caucasian)
The majority of men in our sample who articulated opposition to family member pressure did so around treatment decisions. For example, one man stated,
So, after talking it over with my wife . . . I said, “I’m going to attack this thing . . . I don’t see any reason for me to go to the extreme and have robotic surgery” and the doctor said if I elected for the pellet implants, that doesn’t eliminate the possibility that later on it can go further. . . . She (his wife) didn’t want me to do that though. She said, “No . . . have him remove everything.” I said, “I don’t think it’s necessary . . .” So I told (my physician) that I had decided (to have the pellet implants), and I told him my wife didn’t agree—this time it was just he and I, my wife wasn’t with us. (Age 76 years, African American)
Another man revealed how an expert swayed his decision to go against what he and his family had previously decided for treatment:
I really talked a lot about it (treatment options) with my wife and my children because I felt like, you know, this is something they needed to be involved in and I really didn’t know for myself which way I exactly wanted to go. . . . We eventually started leaning towards the radiation . . . until I went to the (cancer coalition) meeting and (a cancer advocate) was talking about the new robotic surgery and how quick the (recovery is). So, you know, based on that I just felt that was the thing I needed to do. (Age 59 years, African American)
Other accounts implicitly revealed spousal/family member support, such as going to doctor’s visits, researching information, and being encouraging, but the husband made the final decision regarding treatment. One man summed up a common mindset among this group of men regarding their treatment decisions stating: “It’s my body and I would have to live with it.”
Men Who Yielded to Family Pressure
Whereas men tended to go against family members on treatment decisions, most men who yielded to family pressure did so for screening. As one man put it, “My decision (to get screened) was that my wife [told] me that I had to go to these doctors to save the marriage. Let’s put it that way [laughing].” In another case, the subject’s wife urged him to seek medical advice and get screened after he told her he was experiencing urination problems. Another man commented,
My wife did have breast cancer. And so she is particularly concerned to make sure that we don’t avoid having tests done that might detect something early enough so the treatment can be affected. (Age 64 years, Caucasian)
In addition to this kind of direct influence from spouses, we also saw examples in which men witnessed close family members’ experiences with prostate cancer that influenced their decisions to get screened. Moreover, two men who were never screened revealed their willingness to get screened if a family member urged them to do so.
A few men articulated a decision-making process in which they eventually yielded to family member pressures regarding diagnostic procedures. Even though these men went against their own initial desires, they generally made positive comments such as:
She (wife) was very supportive and, you know, my daughters pushed me to follow through on all this stuff, too, to make sure I didn’t just let it lapse because with anything it’s very easy just to say, “Ah, it’s alright. It’ll go away.” (Age 66 years, Caucasian)
Last, there was one account of yielding to spousal/family member pressure regarding treatment decisions (82 years old, Caucasian). This was a complex case in which multiple family members and physicians recommended different treatments. During the joint interview with his wife, she commented that her daughter-in-law was a nurse and influenced them to look into proton beam therapy. Shortly thereafter, they spoke to another family member—a surgeon—who emphatically told them not to do radiation. Then, his physician at a cancer center reportedly told them that the proton beam therapy was not a proven treatment and wanted him to have external beam radiation. His wife indicated growing frustration because “there were mixed messages coming from all over the place.” At that point, the subject commented: “That’s why I eventually succumbed to the family’s decision” to get external beam radiation. His wife emphasized, “It was a family decision.”
Discussion
Prostate cancer can affect the spouse and other family members as well as the patient (Gray et al., 1999) and understanding men’s relationships as they face decisions about prostate cancer screening, diagnosis, and treatment is important for identifying optimal health care strategies. This qualitative study revealed three major themes regarding spousal/family member interactions with men for prostate cancer screening, diagnosis, or treatment decisions: (a) spousal/family member alliance marked by open communication and shared decision making, (b) men who actively opposed spouse/family member pressure and made final decisions themselves, and (c) men who yielded to spouse/family member pressure. As our study underscores, men’s relationships with their wives and family members are dynamic and complex. Moreover, how family members influence men’s prostate cancer decisions vary and can change based on the kind of decision at hand (e.g., screening vs. treatment decisions). Our analysis cannot specify a particular family dynamic that is necessarily ideal. However, understanding these variations is valuable for finding optimal strategies to incorporate family members in the decision-making process.
Although our focus was on the role of men’s family ties, not all men provided accounts of family member involvement in their decisions. Most notably, there was no evidence of spousal/family member alliances among men who were never screened. This may be expected given that they either actively refused or passively avoided screening (Ferrante et al., 2011), both of which would likely preclude open communication and shared decision making with a loved one in the decision-making process.
Our findings support and extend the current body of knowledge in this area. Previous research has reported variation in men’s decision-making styles: that men’s traditional social roles make it difficult to relinquish control or ask for help (Tudiver & Talbot, 1999) and, contrariwise, men prefer a passive role in health decision making (Davison, Degner, & Morgan, 1995). From our analysis, a key theme revealed how men can be influenced by their spouse/family members in their decision to get screened. In contrast, when men faced prostate cancer treatment decisions, they emphasized the importance of making the final decision themselves whether it was in agreement with spouse/family members or not. This suggests a mental shift in men’s decision making. That is, men were apt to concede to undergo preventive screening measures “for the sake of others”; however, when men felt that they were making a life-changing decision (i.e., to treat cancer), they tended to want to retain control of that decision.
Screening for prostate cancer remains controversial (Andriole et al., 2009; Esserman, Shieh, & Thompson, 2009; Friedrich, 2011; Hoag & So, 2012; Schroder et al., 2009; Welch & Albertsen, 2009). As such, patients frequently receive mixed messages including from the medical establishment. For example, the U.S. Preventive Services Task Force recommends against prostate cancer screening in asymptomatic men in the general U.S. population, regardless of age (Chou et al., 2011; Moyer, 2012), which stands in contrast to the American Urological Association’s recommendation to screen men starting at age 40 years (Greene et al., 2013). Additionally, the American Cancer Society recommends prostate cancer screening for asymptomatic men at age 50 years and emphasizes an informed decision-making process between the physician and patient (Smith, Cokkinides, & Brawley, 2012). As evidenced in our study and previous research, men and their spouses often feel overwhelmed when faced with multiple options, and are unsure how to deal with conflicting information (Gray et al., 1999). Some men feel that such decisions are best left to the expertise of physicians (Zeliadt et al., 2006). In other cases, as reported here, men may make the final decision on their own or with their family’s input.
Given the extensive research on men with prostate cancer and their spouses/family members at the time of diagnosis, treatment, and during survivorship, interventions have been developed to incorporate spouses/family members of men with prostate cancer to improve communication or manage psychological distress during these phases (Manne, Babb, Pinover, Horwitz, & Ebbert, 2004; Schapira, Meade, & Nattinger, 1997). Our research suggests the value of incorporating spousal/family member involvement in screening decisions as well. Women often effectively monitor the health behavior of their family members (Umberson, 1992) and our analysis supports the notion that spousal/family member influence may facilitate the decision-making process for prostate cancer screening. These findings highlight the need to find strategies for incorporating family members into men’s decision-making process regarding prostate cancer screening.
We recognize several limitations with our study. First, as a secondary analysis, spousal/family member influence was not the central focus of the study and therefore some responses lacked depth and not all participants spoke explicitly about the role of family ties on their decisions. However, the frequency of organic discussions that included references to family members suggests that they were a significant part of men’s decision-making process—even when they opposed the family’s wishes or made the ultimate decisions themselves. Another issue lies with the use of joint husband/wife interviews. The majority of our findings are based solely on the men’s accounts and only four interviews included both husband and wife. Illingworth et al. (2010) provide a useful discussion of the advantages and disadvantages of joint interviewing. We recognize that additional or different kinds of information would likely have been elicited had the research design required joint interviews. Although the spouse’s presence may have altered four of the men’s responses, the husbands indicated that they wanted their wives present to help remember and verify details for events that occurred, in some cases, many years ago. Also, our study was not designed to produce generalizable findings but to probe in depth into participants’ lives in order to create a deeper understanding of particular life stories (Kuzel, 1999). Our findings should not be interpreted as representing men in general. Consequently, additional research is warranted to better understand the role of family ties for larger and more diverse samples of men as they make such health care decisions. Last, we are mindful of potential researcher bias and took steps to minimize these issues through ongoing discussions among the authors to verify our coding scheme, interpretations, and conclusions.
Conclusion
Family ties can have a significant impact on men’s health care decisions and behaviors. Men vary in their interactions with family members when making decisions about prostate cancer screening, diagnoses, or treatment. Until there is greater clarity surrounding these prostate cancer decision points, an emphasis on shared decision making between clinician and patient should continue. However, we cannot assume that family member influences on men’s health decision making is necessarily beneficial. Our research suggests that for men whose spouse/family members do have a positive, influential role in their health decisions, conversations regarding benefits and risks of screening, diagnosis, and treatment should optimally include the family member as well.
Findings from this study can be used by health care professionals to facilitate the shared decision-making process. Providers and other professionals may need to first gauge men’s current family dynamics. If there is evidence of an existing spousal/family member alliance or that a man tends to yield to spousal/family member pressure when it comes to health care decisions, medical professionals may make deliberate efforts to include the spouse/family member in prostate cancer discussions and draw on the benefits of having a loved one who can help find resources, provide support, and help make critical decisions. For men who demonstrate opposition to family members’ suggestions and want to make decisions themselves, conversations solely with the patient may be sufficient, but efforts to open the lines of communication with family members may be encouraged to help ensure that all parties are aware of certain risks and benefits and are comfortable and confident with their screening, diagnostic, or treatment decisions.
Footnotes
Acknowledgements
We sincerely thank the Morris Regional Health Partnership and American Cancer Society for their assistance with the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported through a grant from the Department of Defense as part of the Dean and Betty Gallo Prostate Cancer Center (W81XWH-06-1-0514).