
Abstract
Although there is some evidence that psychological resilience may “buffer” against depression following major stressors, no data have been reported on the nature and variability of this buffering effect among prostate cancer patients during the 5 years following their initial diagnosis. Patients from two sites in Australia and who had received their initial diagnosis within 5 years (n = 255) were surveyed, and the results indicated that there was a significant inverse relationship between resilience and depression in the overall data, but that was mostly accounted for by a single factor of the resilience scale (“Confidence to cope with change”). Variability in that buffering effect was noted over time since diagnosis, with peaks during the first 6 months, at 24 and 60 months. These findings support the argument to develop focused psychiatric interventions at various periods following a diagnosis of prostate cancer.
Introduction
Prostate Cancer
Like most cancer patients, men with prostate cancer (PCa) are more likely to suffer depression than their age-related peers who do not have cancer (Couper et al., 2006; Kronenwetter et al., 2005; Kunkel, Bakker, Myers, Oyesanmi, & Gomella, 2000; Sharpley, Bitsika, & Christie, 2008). In addition to the unpleasant emotional effects of depression itself, these depressed PCa patients also experience more frequent admission to hospital for emergencies, outpatient visits, and death from a range of causes (Van Gastel, Schotte, & Maes, 1997). As may be expected, the depression itself, plus the pessimistic perspective that is reflected in (or caused by) hospital admissions and outpatient visits, are an indicator of the elevated mental health risk associated with PCa itself. That risk is indicated by the fact that, within the first year following diagnosis, PCa patients are almost twice as likely to commit suicide as men of comparable age who do not have PCa (Chorbov et al., 2007). Attempts to understand and prevent these deleterious side effects of PCa therefore remain a priority for translational research.
In terms of understanding how these side effects occur (and hence developing effective preventative interventions), it is noteworthy that only a proportion of PCa patients actually do become depressed (Sharpley et al., 2008). This suggests that at least some of the whole population of PCa patients already have effective coping strategies or characteristics, which help protect them against the development of severe depression following their diagnosis and treatment. For example, patients’ demographic characteristics such as the availability of family and/or partner support (Carli et al., 2011) and educational, social, and financial standing (O’Hara et al., 2012; Schoevers, Beekman, Deeg, Jonker, & Tilburg, 2003; Vergun, 2012) have been reported to help buffer against depression (Slotsky et al., 1991). However, these background factors do not predict as much of the variance in depression scores as some behavioral or attitudinal factors that equip people who hold them to cope effectively with stress (e.g., Bitsika, Sharpley, Aroutzidis, & Smith, 2011; Sharpley, Bitsika, & Christie, 2011a, 2011b; Sharpley, Bitsika, & Christie, 2012; von Ammon Cavanagh, Furlanetto, Creech, & Powell, 2001). One of those behavioral/attitudinal factors that has received a good deal of attention recently in various settings and populations is psychological resilience (Fredrickson, Tugade, Waugh, & Larkin, 2003).
Psychological Resilience
Resilience refers to an individual’s capacity to cope with stressors and to resist the harmful effects of future negative events (Luthar & Cicchetti, 2000). Resilience has been defined as a personal trait or attribute that promotes rebounding from disappointments (Brooks, 2005), positive adjustment in adverse circumstances (Tedeschi & Kilmer, 2005), or successful adaptation to challenging life stressors (Alvord & Grados, 2005). Although once considered to be similar to recovery from trauma, resilience follows a distinct trajectory to recovery after individuals experience a traumatic event (Bonanno, Galea, Bucciarelli, & Vlahoz, 2007). As well as having been reported to intervene between the experience of traumatic events and the individual’s later return to optimism in the face of such occurrences as old age (Jopp & Rott, 2006), chronic pain (Karoly & Reuhlman, 2006), and terrorist attack (Bonanno et al., 2007), resilience assists individuals to overcome the experience of trauma during early childhood and to progress to normal and satisfying lives (Watt, David, Ladd, & Shamos, 1995) and can reduce depression induced by stressful events (Andreescu et al., 2007). Resilience has also been reported to influence physical health, for example, as a protective effect against coronary heart disease in a 10-year study of 1,306 men (Kubzansky, Sparrow, Vokonas, & Kawachi, 2001), chronic illness in adults (Becker & Newsom, 2005) and children (Vinson, 2002), and in helping avoid the onset of illness (Yi, Smith, & Vitaliano, 2005). Initially investigated as a psychological variable, resilience has a biological basis that relies on plasticity of the reward and fear circuits in the brain (Bergstrom, Jayatissa, Thykjaer, & Wiborg, 2007), suggesting that resilience may be learnt and that preventative as well as treatment modalities should be considered (Haglund, Nestadt, Cooper, Southwick, & Charney, 2007). To that end, resilience training has been instituted as a preventative measure against traumatic stress in several major organizations, including the U.S. Army (Vergun, 2012).
In a previous study of resilience and depression in PCa patients (Sharpley, Bitsika, Wootten, & Christie, 2012), factor analysis of one of the most commonly used scales for assessing resilience—the Connor–Davidson Resilience Scale (CDRISC; Connor & Davidson, 2003)—revealed three factors, which were identified as “Confidence to cope with change,” “Being able to take difficult actions,” and “Trusting in a higher power.” Thus, these three factors may be categorized into attributions to “Self/Internal” or “Other/External” sources of control over one’s mental health. However, it is of note that not all of these constructs have been positively associated with mental health. For example, some time ago, Taylor, Helgeson, Reed, and Skokan (1991) showed that male medical patients who attributed control of their illness to external sources (rather than their own actions) had poorer prognoses than those who attributed such control to their own behavior and decisions. Those findings have been replicated with cancer patients (Thompson, Sobolew-Shubin, Galbraith, Schwankovsky, & Cruzen, 1993) and more recently in patients coping with chronic pain (Ramírez-Maestre, Esteve, & López, 2012). Together, these findings suggest that “internal” attributions of control over one’s mental health may exert greater positive effect than “external” attributions of control, within the overall construct of resilience. Therefore, as a means of further understanding the relationship between resilience and depression following a diagnosis of PCa, both the total CDRISC scores and these three factor scores were used in the current study.
However, despite the potential value of resilience in helping PCa patients cope with their stressors arising from diagnosis and treatment, there are no studies that reported on the trajectory of resilience as a buffer against PCa-related depression in the years after diagnosis. Snap-shot studies of resilience and depression at a particular point in time after diagnosis can provide an overall assessment of the power of resilience as a buffer against depression, but data on the presence of any variability in the strength of the buffer effect of resilience against depression over the years following diagnosis and treatment could identify when resilience might be most effective and when alternative coping strategies could be applied.
Study Aims
Therefore, this study investigated the presence and timing of variability in the relationship between depression and resilience during the 5 years postdiagnosis in a sample of PCa patients to “map” that relationship with a view to determining (a) when resilience appeared to have the most powerful buffering effect against depression and (b) when resilience-based or nonresilience-based interventions might be most profitably applied with PCa patients who suffer depression.
Method
Participants
A total of 425 PCa patients from treatment centers in two states of Australia responded to a posted invitation to participate in a study “about how you feel.” This represents a 56.7% response rate, which is commensurate with previous postal surveys carried out with this population (Sharpley, Bitsika, & Christie, 2010; Sharpley, Bitsika, & Christie, 2011a, 2011b). All participants had PCa limited to the primary site and regional draining lymph nodes using conventional staging investigations. Patients were at stages T2 to T4 (UICC Standards), with no involved nodes and no metastases. Treatments included radiotherapy and/or surgery and hormone therapy when required. Other inclusion criteria were the following: (a) the diagnosis of PCa was proven histologically via usual biopsy and related viewing of microscopic indicators of PCa by appropriately qualified pathology staff; (b) all the treatment options were properly considered by patients via discussion with their GP, a radiation oncologist, and a urologist; and (c) patients were included regardless of the type of hormone therapy they had been prescribed. Unwillingness to participate in the study was the only exclusion criterion. From this pool of 425 participants, those 255 who were within 5 years of diagnosis were selected for this study. Five years was chosen as the period for observation because it is a considerable amount of time since diagnosis. To detect variability over time, participants were allocated into ten 6-month cohorts on the basis of the time since their initial diagnosis.
Measures
Background questionnaire items included the following: age (in years), living situation (with wife/partner, widowed, separated/divorced, never married), month and year of first diagnosis, past treatments and current treatments (radiotherapy, surgery, hormone therapy, none), present status of their cancer (cancer still present and undergoing initial treatment, no obvious sign of cancer [in remission], cancer reoccurring after previous treatment).
Depression was assessed via the self-report Patient Health Questionnaire-9 (PHQ9). The PHQ9 was developed from the diagnostic criteria for Major Depressive Disorder from the Diagnostic and Statistical Manual of Mental Disorders, text revision (DSM-IV-TR; American Psychiatric Association, 2000) and possesses excellent validity for patients with severe, moderate and mild depression (Kroenke, Spitzer, & Williams, 2001). Possible scores on the PHQ9 range from 0 to 27.
Resilience was assessed by the CDRISC (Connor & Davidson, 2003). The CDRISC includes 25 items such as “I like a challenge,” “When things look hopeless I don’t give up,” “I bounce back after illness or hardship,” and “I am able to adapt to change” (Connor & Davidson, 2003). Total scores on the CDRISC range from 25 to 100 and are significantly correlated (.83) with total scores on the Kobasa Hardiness Measure and negatively correlated with total scores on the Perceived Stress Scale (−.76), indicating high concurrent validity. The CDRISC has acceptable reliability, ranging from .89 (Cronbach’s α) to .87 (test–retest reliability; Connor & Davidson, 2003).
Procedures
Patients were posted a package including the Participant Information Statement, Background Questionnaire, and copies of the PHQ9 and CDRISC, plus a stamped and addressed envelope for return of the questionnaire package. All procedures were approved by the relevant human research ethics committee. All participants gave written consent to the study.
Results
Sample Results
The background data for the sample of 225 PCa patients are presented in Table 1. There were no significant correlations between PHQ9 scores and any of the demographic variables. The 5% trimmed means for both the PHQ9 and the CDRISC were very similar to the actual means, indicating negligible influence from extreme scores. Reliability (Cronbach α) values for PHQ9 was .876 and for the CDRISC it was .927, supporting further analysis of these data.
Background, Depression, and Resilience Data for Sample (N = 255).

Note. PHQ9 = Patient Health Questionnaire-9; CDRISC = Connor–Davidson Resilience Scale.
Relationship Between Resilience and Depression
The overall correlation for CDRISC total scores and PHQ9 scores from the 255 patients was r = −.521, p < .01, reflecting the inverse relationship between resilience and depression, and CDRISC total score significantly (R2 = .291, F = 165.677, p < .001) predicted PHQ9 total scores in a linear regression equation (Beta = −.539, p < .001). However, the PHQ9 scores were positively skewed (as might be expected in such a sample of nonclinically depressed participants), with a significant Kolmogorov–Smirnov statistic (p < .001) and verified by inspection of the histogram as recommended by Tabachnick and Fidell (2007). As a safeguard against the possible biasing of outcomes from correlational and regression analysis with skewed data, the PHQ9 values were inversely transformed as recommended (Tabachnick & Fidell, 2007). This reduced the degree of skewness to negligible, and the analyses were reperformed on these transformed values to check if transformation influenced the results of the analyses. There was no real difference in the size of the results using the transformed PHQ9 values, although the direction of the obtained correlations and Beta values were changed because of the inverting of the PHQ9 scores (correlation between CDRISC and PHQ9 total scores: r = .533, p < .01; regression of CDRISC on PHQ9 scores: R2 = .284, F = 160.387, p < .001), CDRISC predicted PHQ9 total scores in a linear regression equation (Beta = −.533, p < .001). These results indicate that the statistical analyses were not biased by the original skewness of the PHQ9 scores and hence those initial analyses may be accepted as indicative of the true relationship between CDRISC and PHQ9 in this sample.
As mentioned above, a previous study of resilience and depression in PCa patients (Sharpley, Bitsika, Wootten, et al., 2012) noted three factors for the CDRISC (“Confidence to cope with change,” “Being able to take difficult actions,” and “Trusting in a higher power”). As a means of further understanding the relationship between resilience and depression following a diagnosis of PCa, both the total CDRISC scores and the three factor scores were analyzed separately for their relationship with PHQ9 total scores for the entire sample. Pearson correlations between these three CDRISC factors and PHQ9 total score were −.558, p < .001 (Factor 1), −.333, p < .001 (Factor 2), and −.221, p < .001 (Factor 3), suggesting that all three CDRISC factors were significantly associated with depression, but only Factors 1 and 2 had an inverse relationship with PHQ9 scores. Hierarchical linear regression of the CDRISC factor scores on PHQ total score for the entire sample indicated that only CDRISC Factor 1 significantly predicted PHQ9 total score (R2 = .568, F = 120.738, p < .001), with CDRISC Factor 2 adding only .008 to the R2 (ns) and CDRISC Factor 3 adding only .002 (ns). When directly compared with CDRISC Factor 1 as a predictor of PHQ9 total score, R2 = .568, F(1, 253) = 120.738, p < .001, the total CDRISC score did not significantly add to the prediction of depression (R2 change = .001, ns), suggesting that CDRISC Factor 1 represented the most powerful resilience association with depression in these men.
Time-Since-Diagnosis Cohort Results
In addition to the analysis of data from the entire sample, the presence of different effects according to time since diagnosis was also undertaken. The 6-month cohorts, number of participants in each 6-month cohort, the CDRISC and PHQ9 raw scores, CDRISC factor scores, Pearson correlations between PHQ9 and all four sets of CDRISC scores, and the p value for each correlation are presented in Table 2. Bearing in mind the results from the hierarchical regression of the three CDRISC factor scores on PHQ9 total scores for the entire sample that was described above, it is not unexpected that similar patterns of results appear in the columns reporting correlation coefficients and p values for each of those factors. That is, while Factor 1 was significantly correlated (at the .05 level) with PHQ9 for 9 of the 10 time-since-diagnosis cohorts (shown by underlining), Factor 2 was significantly correlated with depression in 6 of the cohorts and Factor 3 in only 2 of the cohorts; CDRISC total score was significantly correlated with PHQ9 total score in 8 of the 10 cohorts (all underlined). (When the calculation of multiple correlations was accompanied by appropriate Bonferroni corrections to bring the alpha level to .05/10 = .005 for each comparison, the pattern of significant results remained the same: Factor 1 = 6, Factor 2 = 3, Factor 3 = 0, Total CDRISC score = 4.) These results suggested that CDRISC Factor 1 was the most powerful predictor of PHQ9 total scores and therefore this aspect of resilience was the focus of the next analysis.
Six-Month Cohorts, n, PHQ9, CDRISC Total and Factor Scores, Pearson Correlations, and p Values.

Note. PHQ9 = Patient Health Questionnaire-9; CDRISC = Connor–Davidson Resilience Scale.
The standardized scores for PHQ9 and CDRISC Factor 1 across the 10 time-since-diagnosis cohorts are reported in Figure 1 and indicate that, when adjusted for comparison purposes in this way, the two sets of z scores are very similar, a result supported by Pearson correlation of those two sets of z scores (r = .775, p < .01), with CDRISC Factor 1 accounting for more than 60% of the variance in PHQ9 scores over the 10 cohorts. Although z scores do not reflect the inverse relationship between these two variables, that is apparent from Figure 2, which presents the raw correlation coefficients for these two variables. These results confirm those reported above for the entire sample and suggest that CDRISC Factor 1 was the most powerful aspect of resilience that was associated with depression, both overall and within time-since-diagnosis cohorts, and that that relationship reflected the “buffering” nature of CDRISC Factor 1 against PHQ9 scores over time.
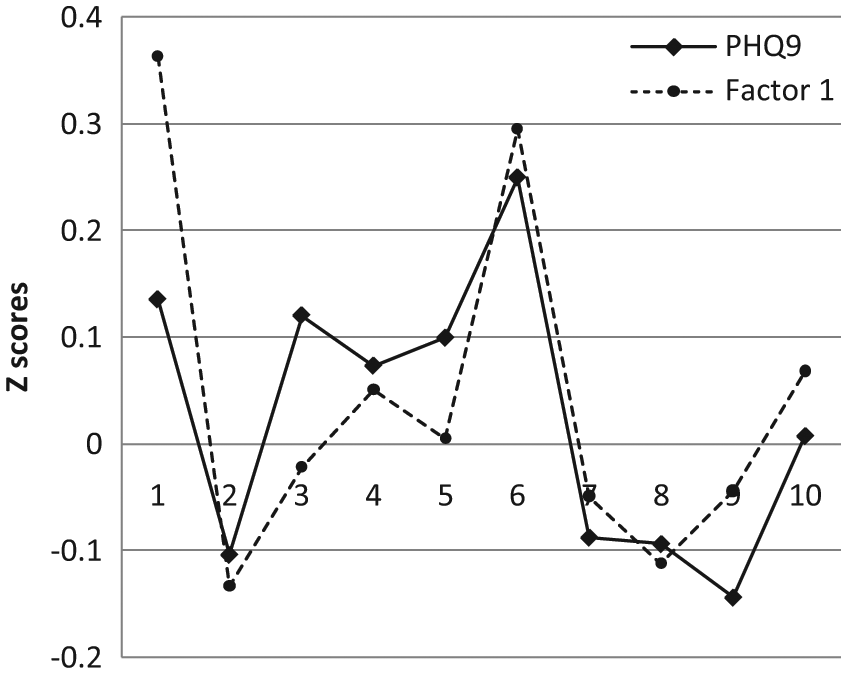
Standardized scores for PHQ9 and CDRISC Factor 1 across 10 time-since-diagnosis cohorts.

Pearson correlations between PHQ9 and CDRISC Factor 1 for 10 time-since-diagnosis cohorts.
However, Table 2 and Figure 2 also indicate the presence of some variability in the buffering effects of CDRISC Factor 1 against depression. That is, as indicated by the fourth-order polynomial trendline, those effects appear to be strong during the first 6 months after diagnosis, then gradually reduce during the next 18 months, rise again at 24 months after diagnosis, drop momentarily at 30 months, and then rise again before a gradual decrease to become nonsignificant at 54 months and rise again at the end of 5 years after diagnosis. Although somewhat generalized, with evidence of intervening variations from that overall pattern, these results suggest that resilience is a powerful buffer at certain times (e.g., at 6, 24, and 30-48 months after diagnosis), it does not buffer against depression as powerfully during the 12- to 18-month period, the 30-month period, and is not significantly related to depression during the 54-month period. There are also treatment variables in play during some of these times that might also influence depression (e.g., patients might receive staging tests, bone and computed tomography scans to check for spread of the cancer beyond the prostate during the first 6 months after diagnosis, and may receive hormone treatment during the period 6 to 12 months, followed by surgery or radiation therapy), plus the presence of recurring cancer versus treatment success after 12 months. However, there were no significant correlations between these treatment of cancer status variables in the sample, suggesting that these factors were relatively less powerful in predicting (or buffering against) depression than CDRISC Factor 1.
Discussion
Summary of Findings
These results confirm the overall buffering effect of psychological resilience on depression in a PCa sample but indicate that most of that effect was because of a single factor in the CDRISC. By breaking the sample into 6-month after-diagnosis cohorts, that result was able to be extended into an analysis of variability in the buffering effects of CDRISC Factor 1 during the first 5 years after diagnosis. It is clear from these data that having the confidence to cope with change was a powerful attribute for dealing effectively with the challenging side-effects of PCa and its treatment for these 255 men, and was the most powerful aspect of resilience, with another aspect of the CDRISC (Trusting in a higher power) actually directly contributing to depression in this sample.
Implications for Clinical Practice
Two major findings from this research have implications for intervention with PCa patients. First, these results suggest that it is only some aspects of resilience (as measured by the CDRISC) that act to protect PCa patients against depression, and some other aspects are either negligibly effective or actually work to increase depression in these men. That is, resilience training for PCa patients might most profitably focus on helping them to build their confidence to cope with change rather than simply leave their mental health to other agencies. Second, the confidence to cope with change may vary in its effectiveness as a buffer against depression over the 5 years following diagnosis.
In terms of the first of these two major findings, having confidence and capacity to cope with change has implications for the therapeutic interventions offered to men who are treated for PCa. An ability to cope with change and confidence in oneself in the context of this change evidently buffers against depressive symptomatology and as such presents an opportunity to enhance these characteristics in the therapeutic setting if required. Confidence in one’s personal capacity to cope with change could be linked to a number of psychological processes that could offer opportune focus for therapy. Strong self-esteem and confidence are most often found in individuals free from negative self-appraisal and who possess a self-determined approach to life. These characteristics could be enhanced through a cognitive behavioral or interpersonal approach to therapeutic interventions aimed at improving the individual’s ability to manage the changing nature of their life. In the context of PCa, masculine self-esteem appears to play a significant role in the individual’s capacity to cope with change. Therefore, therapeutic interventions tailored for men, such as those espoused by Tremblay and L’Heureux (2011), might assist PCa patients cope with the challenges of their disease and its treatment and may also help them (indirectly) enhance their masculine self-esteem, which in turn may build their emotional health.
The second major finding (variability in the buffering effects of resilience over time) indicates that there may be key milestones across the continuum of time after PCa treatment that result in the need to draw on these traits to cope with the physical and emotional challenges related to PCA treatment. It is common for men to lose a sense of control over their side effects at the 12- to 18-month posttreatment milestones when physical symptoms have not resolved to the level they had expected and this is often a time when personal resources and an ability to adapt and cope with this change (or lack of) may come to the fore.
Limitations
There are several limitations to this study. First, although two sites were sampled, data were collected in one nation and may not generalize to others with different cultures. Second, resilience and depression were assessed via self-report, and results may vary if other methods were used. In addition, because the sample was self-selected and data were self-reports, no reliable information could be obtained regarding the presence of other medical and psychiatric conditions, which may have influenced results. Third, although resilience as defined by the CDRISC has been reported to buffer against stressors in this and previous studies of non-PCa patients, the exact nature of this construct may benefit from further examination. For example, the factor structure found with PCa patients differs from that reported by the CDRISC authors, and there may be some uncertainty regarding how resilience manifests itself in different populations. Fourth, further research into the relative effects of resilience for patients undergoing different treatments for their PCa (i.e., surgery, hormone treatment, radiotherapy) could help elucidate the ways in which resilience assists PCA patients deal with the particular challenges presented by the different treatment approaches. Fifth, although accepted as the “gold standard” in diagnosing depression, the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; American Psychiatric Association, 1994) criteria for Major Depressive Disorder or Major Depressive Episode TR (on which the PHQ9 is based) have been criticized for not being relevant to male depression (Cochran & Rabinowitz, 2003; Oliffe & Phillips, 2008). For example, the Gotland Depression Male Depression Scale (Zierau, Bille, Rutz, & Bech, 2002) identified 39% of a male sample of alcoholics to be depressed, whereas the DSM-IV-TR (American Psychiatric Association, 2000) criteria identified only 17% of the same sample as depressed. Measurement of depression in PCa patients has not yet encompassed this “male” perspective, and future research using such a perspective would help determine if there are differences in the way that resilience buffers depression when the latter is assessed via a gender-specific instrument. Finally, although allocating the sample into 6-month cohorts enabled comparisons to be made across those periods, the further collection of prospective data from studies, which repeatedly measure depression and resilience in the same patients over time, would provide an alternative perspective on the issue of how resilience might vary during those periods. However, it should be noted that such research designs that incorporate repeated measurements on the same participants over time are also open to the biasing effects of serial correlation of scores, which has been reported to inflate t or F statistics by as much as 400% (Sharpley & Alovosius, 1988), thus making the kind of cross-sectional study used here a valid alternative.
Notwithstanding these limitations, these results confirm the buffering effects of resilience over the first 5 years following a diagnosis of PCa but show that there is some variability in that relationship over that period. Implications for provision of resilience-building indicate that men with PCa who do not show a capacity to cope with change, or who rely on external factors (such as a higher power) in an attempt to cope with change, may benefit from psychotherapeutic interventions aimed to strengthen confidence and self-esteem at specific periods after diagnosis.
Conclusions
These results are congruent with those previously reported for the effects of resilience as a buffer against depression in patients undergoing other physical health stressors and which were described in the Introduction. However, the findings from this study also extend that previous research by identifying the active component (i.e., CDRISC Factor 1) in the resilience measure that was used here. Furthermore, although no previous studies have examined the trajectory of the influence of resilience on depression in PCa patients, allowing for specialized conclusions regarding this patient group to be drawn. Although those conclusions may not necessarily generalize to other patient populations, the previous literature regarding the relative effectiveness of “Internal” versus “External” sources of perceived control over one’s health is verified within the PCa population by this study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the contribution made by the Collaborative Research Network on Mental Health and Well-being in Rural Communities, supported by the Department of Industry, Innovation, Science, Research and Tertiary Education, Commonwealth Government of Australia.