
Abstract
Although there is an abundance of evidence regarding clinical efficacy and safety of benign prostatic hyperplasia (BPH) treatment, real-world evidence is lacking for pharmacotherapy utilization and trends. It is unclear how evidence demonstrating the efficacy of combination 5-alpha reductase inhibitors and alpha blockers for improving symptoms and reducing risk of disease progression translates into real-world practice for the treatment of BPH. A retrospective study of a database was conducted to describe pharmacotherapy utilization/trends in the treatment of BPH among patients in the managed care setting. After inclusion and exclusion criteria were applied, the final sample size was 107,038. The proportion of patients with BPH receiving 5-alpha reductase inhibitors therapy increased (21.1% in 2003 to 30.5% in 2007), as did the proportion receiving combination therapy (10.7% and 16.1%, respectively). We observed an almost 50% increase in 5-alpha reductase inhibitors use over 5 years and a 60% increase in the use of combination 5-alpha reductase inhibitors/alpha blockers therapy.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a chronic progressive urologic disorder commonly associated with bothersome lower urinary tract symptoms (LUTS). The prevalence of BPH and resultant economic burden is high, ranking as the fourth-most-commonly diagnosed disorder in men older than 50 years, with an estimated $1.1 billion in total direct medical costs each year (Issa, Fenter, Black, Grogg, & Kruep, 2006; Fenter, Naslund, Shah, Eaddy, & Black, 2006; Wei, Calhoun, & Jacobsen, 2005). Approximately, one in four men will require medical care for BPH by the age of 80 years, and more than 90% will have histological evidence of BPH by the age of 85 years (American Urological Association, 2010; McConnell, Barry, & Bruskewitz, 1994; Roehrborn et al., 2003). As BPH progresses, men may develop acute urinary retention (AUR) and other serious complications that may require surgical intervention (Emberton et al., 2003). Beyond the direct clinical manifestations and economic burden, BPH is associated with diminished quality of life, with increasing severity of symptoms associated with lower general health perception, physical condition, and role limitations, as well as impaired sexual functioning (Roberts et al., 1997; Rosen et al., 2003).
Historically, therapy for BPH has focused on surgical intervention and symptom management. However, over the past several years, there has been a shift toward pharmacotherapy for first-line treatment of LUTS (Sarma et al., 2005). The complex nature of BPH involves the prostate, bladder, and central nervous system, thus, allowing for several therapeutic targets (Desgrandchamps, 2004). Current medical treatment guidelines recommend combination therapy incorporating alpha blockers (ABs) and 5-alpha reductase inhibitors (5ARIs) for patients experiencing LUTS associated with demonstrable prostatic enlargement (American Urological Association, 2010; Desgrandchamps, 2004). Although AB therapy provides rapid relief of symptoms (within 1 week of initial administration) by decreasing smooth muscle tone in the prostate, urethra, and bladder (Dunn, Matheson, & Faulds, 2002), ABs have no effect on prostate volume and therefore do not affect the risk of disease progression. Conversely, although symptom improvement takes longer (3-6 months) for 5ARI therapy, it also decreases risk of disease progression by inhibiting the conversion of testosterone to dihydrotestosterone, a hormone that stimulates prostate growth (American Urological Association, 2010; Rigatti et al., 2003). 5ARI therapy has demonstrated a 57% reduced relative risk of AUR and a 48% reduced relative risk of surgical intervention compared with placebo at 2 years (both p < .001 vs. placebo; Roehrborn, Boyle, Nickel, Hoefner, & Andriole, 2002), and these reductions were maintained to 4 years during open-label phases of the studies (Debruyne et al., 2004). Therefore, combination 5ARI + AB therapy not only provides short- and long-term relief of symptoms but also decreases the risk of disease progression and associated surgical intervention and complications.
A growing body of evidence supports the use of combination 5ARI + AB therapy. The European PREDICT trial (Kirby et al., 2003) reported that patients receiving combination doxazosin + finasteride had significant improvement in American Urological Association symptom scores (p < .01 vs. finasteride alone) and peak flow rate (p < .01 vs. finasteride alone) compared with patients receiving finasteride monotherapy or placebo. The European Medical Therapy of Prostatic Symptoms study (McConnell et al., 2003) reported that combination 5ARI + AB was associated with significantly lower risk of clinical progression (risk reduction of 66% for the comparison with placebo, p < .001; p < .001 for each pairwise comparison of combination therapy with monotherapy) and improved symptom scores compared with either agent alone (p < .001 for the 5ARI + AB combination therapy group vs. the 5ARI monotherapy group; p = .006 for the 5ARI + AB combination therapy group vs. the AB monotherapy group). Risk of urinary retention and the need for invasive therapy was reported to be reduced in patients receiving either combination 5ARI + AB therapy (p < .001) or 5ARI monotherapy (p < .001) but not in patients receiving AB monotherapy. More recently, the CombAT study (Roehrborn et al., 2009; Roehrborn et al., 2010) reported similar results. Spanning 4 years, this study demonstrated that combination therapy was associated with reduced risk of clinical progression (p < .001 for both comparisons) and greater improvement in symptoms (p < .01 for both comparisons) compared with either AB or 5ARI monotherapy, as well as reduced risk of AUR or BPH-related surgery compared with AB monotherapy (reduction in relative risk of 65.8%; Roehrborn et al., 2010). Results from observational studies have paralleled the conclusions of the pivotal clinical trials. Naslund and colleagues identified that 5ARI therapy was associated with lower rates of AUR compared with patients receiving AB monotherapy (Naslund, Issa, Grogg, Eaddy, & Black, 2006), and more recently demonstrated that delayed initiation of 5ARI therapy among patients receiving combination 5ARI + AB therapy was associated with increased risk of clinical progression (Naslund, Eaddy, Hogue, Kruep, & Shah, 2009).
Given the accumulating evidence from clinical trials demonstrating the benefit of combination 5ARI + AB therapy in terms of symptom improvement and disease progression, one would expect that this therapeutic combination would be used to an increasing degree. Although there is an abundance of evidence regarding clinical efficacy and safety of BPH treatment, real-world evidence is lacking for pharmacotherapy utilization and trends. To the authors’ knowledge, there have not been any retrospective database analyses to characterize the real-world use of these medications published to date. As such, the purpose of this study was to describe pharmacotherapy utilization and trends in the treatment of BPH among patients in the managed-care setting over a 4-year period of time.
Materials and Methods
This was a retrospective cohort study using data on BPH patients from the MarketScan Database. This database contains commercial and Medicare medical and pharmacy claims data that is sourced directly from health plans and employers, representing approximately 18 to 20 million individuals annually from multiple states. The time period for this study spanned 5½ years, from January 1, 2003 to June 30, 2008. Men aged 50 years and older who were treated with an AB or 5ARI alone or in combination between July 1, 2003 and June 30, 2007 were eligible for study inclusion. This enrollment period allowed for treatment patterns to be evaluated 12 months after the index date, defined as the first fill for a BPH-related prescription. A 6-month period preceding the index date allowed for an evaluation of baseline characteristics of patients. Documentation of a BPH diagnosis among patients was evaluated in the 6-month preperiod and 1-year postindex assessment period. The study design employed for identifying eligible patients and for evaluating treatment patterns is illustrated in Figure 1. Exclusion criteria were patients who had prostate cancer (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9] codes 185, 198.82, 233.4, 236.5, 239.5, V10.46) or bladder cancer (ICD-9 codes 188, 198.1, 223.3, 233.7, 239.4, V10.51) during the study period; had prostate-related surgery (Current Procedural Terminology [CPT] codes 52601, 52612, 52614, 52620, 52640, 52647, 52648, 55801, 55821, 55831, 52850, 52852, 52852, 52853) prior to or within 1 month of the index date; received finasteride dose indicative of male pattern baldness; were not continuously eligible for 6 months pre- and 12 months postinitial prescription; or did not have a documented BPH diagnosis.

Study design.
Patients were assigned to treatment groups based on the presence and timing of fills for classes of BPH-related medications. The following five groups were defined:
AB monotherapy;
5ARI monotherapy;
Early combination, AB + 5ARI combination therapy (within 30 days);
Delayed combination, AB + 5ARI combination therapy (with 5ARI starting more than 30 days after AB but within 1 year);
5ARI before AB.
Changes in these treatment groups were evaluated across the years of data. Accordingly, all analyses were descriptive in nature and were conducted using SAS version 9.2.
Results
The application of study exclusion criteria and resultant attrition of the potential pool of study patients are illustrated in Figure 2. A total of 585,932 patients were initially identified, who were treated with AB and/or 5ARI therapy during the study enrollment period. Reasons for exclusion and resultant patient attrition are illustrated in Figure 2. After applying all inclusion and exclusion criteria, a total of 107,038 evaluable patients (18% of initially identified patients) remained for analysis.

Patient selection algorithm.
The distribution of patients across treatment groups are presented in Table 1. The majority of patients (n = 78,324; 73.2%) received AB monotherapy during the study time period, whereas 8.6% (n = 9,225) received 5ARI monotherapy. A total of 15,379 patients (14.3%) received combination 5ARI + AB therapy: 6.5% of patients (n = 7,001) received early 5ARI therapy (within 30 days of AB therapy), whereas 7.8% of patients (n = 8,378) received delayed 5ARI therapy. Finally, 3.8% (n = 4,110) received 5ARI therapy followed by AB therapy.
Numbers of Patients by Treatment Group.

Note. 5ARI = 5-alpha reductase inhibitor; AB = alpha blocker.
Trends in treatment patterns over time among patients treated for BPH are depicted in Figure 3. The proportion of patients with AB monotherapy decreased from 78.9% in 2003 to 69.5% in 2007. Or, conversely, the proportion of BPH patients receiving 5ARI therapy increased from 21.1% in 2003 to 30.5% in 2007. The proportion of patients receiving combination therapy (early and delayed 5ARI therapy) over the years was as follows: 10.7% in 2003, 11.7% in 2004, 15.2% in 2005, 16.5% in 2006, and 16.1% in 2007.
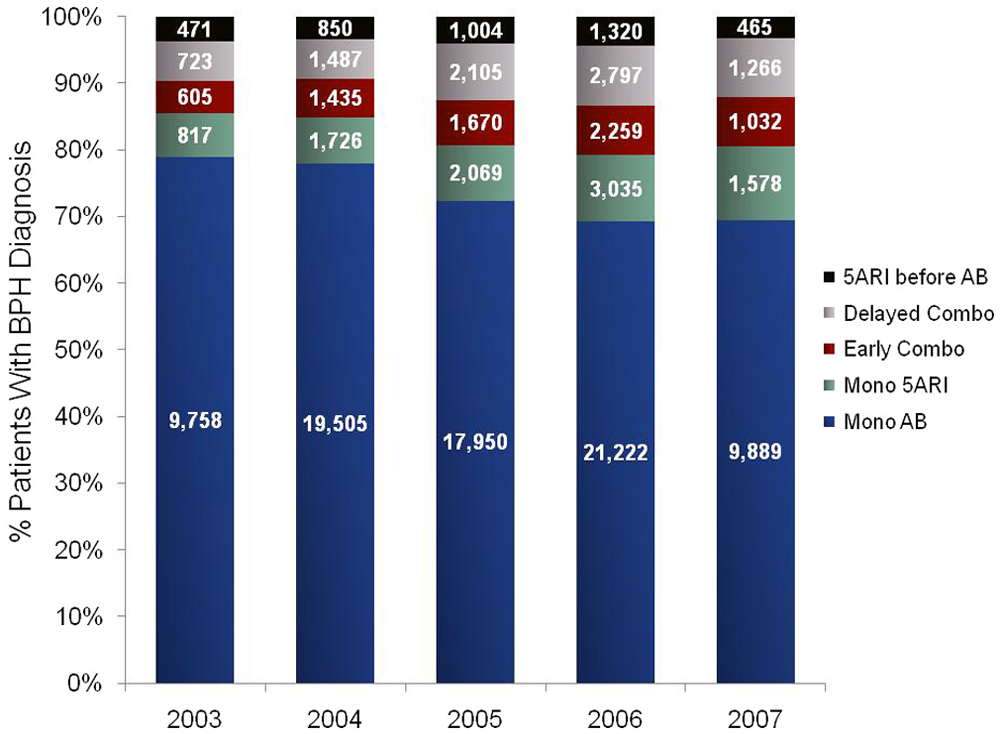
Treatment patterns over time.
Discussion
Despite the demonstrated clinical efficacy of 5ARI therapy, results of this retrospective study suggest that a large proportion (73%) of BPH patents continue to receive only AB therapy. Furthermore, combination 5ARI + AB therapy was used in only 14% of patients treated from 2003 to 2007. However, there was a noted 50% increase in 5ARI use over the study period and a 60% increase in combination use.
Prior to the time frame of this study, pharmacotherapy for BPH focused primarily on symptom management. However, results from several pivotal trials, including the Medical Therapy of Prostatic Symptoms study (McConnell et al., 2003), and the PREDICT trial (Kirby et al., 2003) released in 2003 highlighted the potential benefit of a more comprehensive strategy of combined symptom management and disease modification. The complementary mechanisms of action of AB therapy, which provides rapid symptom improvement, and 5ARI therapy, which improves symptoms, reduces prostate size, and reduces the risk of disease progression over time, make them a valuable and potentially superior alternative to monotherapy. With the accumulation of evidence and increased awareness of the clinical benefit of combination 5ARI + AB therapy, one might expect a resultant change in treatment patterns from an emphasis on symptom management (i.e., AB monotherapy) to combination therapy. In our current study, we did observe moderate shifts in real-world treatment patterns over the time frame of the study. Although AB monotherapy remained the predominant choice of therapy, utilization of 5ARI therapy overall (alone or in combination) increased from approximately 20% to 30% from 2003 to 2007. There was an observed trend in increasing utilization of combination 5ARI + AB therapy as well. Over the 5-year time frame of the study, we saw that utilization of combination therapy increased by approximately 50%, from 10.7% in 2003 to 16.1% in 2007.
More recent research suggests that early initiation of 5ARI therapy in combination with AB therapy may be associated with lower risk of disease progression compared with patients with delayed initiation of 5ARI therapy (Naslund et al., 2009). In this current study, we found that among patients receiving combination therapy (N = 15,387), 45.5% of those (n = 7,001) were early initiators of 5ARI therapy. This proportion did not change significantly over time: 45.6% of patients receiving combination therapy in 2003 were early 5ARI initiators versus 44.9% among combination therapy patients in 2007.
Although this study highlights changes in treatment trends over recent years, there are inherent limitations that should be mentioned. Because of the deficiency of clinical data available in this claim-based analysis, diagnosis of BPH was dependent on a diagnostic code and lacked the clinical context that would be provided with clinical data (e.g., prostate size, American Urological Association symptom score, etc.). Given the nature of claims data, a substantial number of patients were excluded because of an insufficient enrollment period, which may affect the generalizability of results. Furthermore, a large number of patients receiving BPH-related therapy did not have a documented diagnosis of BPH and were not included in the current assessment of therapy utilization. Although this may introduce constraints on how these data are interpreted, it also highlights an important point that the true burden of BPH may be underestimated because of incomplete documentation of this disease. Finally, although the data used for this study included multiple payer types (commercial and Medicare) and should be considered a strength, our results may not reflect treatment patterns among indigent and underserved populations.
In conclusion, this study sheds light on the recent treatment patterns of patients with BPH receiving pharmacotherapy in a managed care setting. Although there has been a slight shift in therapy utilization from AB monotherapy to combination 5ARI + AB therapy over time, the latest data suggest that there remains a large proportion of the patient population who may be receiving suboptimal therapy. Future studies should attempt to further characterize this subgroup in an effort to identify high-risk patients who might benefit from combination therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BBG is an employee of GlaxoSmithKline. EJK and SC are employees of Xcenda, a consulting company that received payment from GlaxoSmithKline to assist with this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by GlaxoSmithKline.