
Abstract
Prostate cancer and its outcomes are a real threat for health and well-being for men living in the Western world. The number of men with a diagnosis of prostate cancer, before the age of 65 years, has increased in recent decades. The aim of this study was to explore how some of these Swedish men experienced and talked about their sexuality. Four focus group discussions were performed in the context of associations for prostate cancer. Using qualitative content analysis, it was identified how the diagnosis was a threat to their male identity; the men’s vulnerability as a group in society was made explicit. Their sexuality was diminished by their illness experiences. These experiences were difficult to share and talk about with others and therefore connected with silence and sorrow. As a result of this, the informants often played a passive role when or if they discussed issues related to sexuality with someone in the health care organizations. The possibility of voluntarily joining a cancer association was probably highly beneficial for these men. During the sessions, several men expressed the opinion that “it is always great to talk.”
Urological cancers encompass about one third of all cancers diagnosed in men worldwide, and prostate cancer is the most common urological cancer (Boyle & Levin, 2008). Unfortunately, individual prognostic approaches are poorly developed, and for most men, prostate-specific antigen (PSA) testing is the only way to track the progress of the illness (Cady, 2009; National Cancer Institute, 2007). Furthermore, barely 20% of all men have already reached a chronic stage when they are diagnosed with prostate cancer, and when one modality fails the patient, another is used. As such, for these men, living with prostate cancer means living with uncertainty and negative side effects of treatments (Haas & Yenser Wood, 2009; National Cancer Institute, 2007).
Prostate cancer appears predominantly among older men. The median age at diagnosis is 72 years (National Cancer Institute, 2007). However, diagnoses in the younger population, that is, those 65 years or younger at the time of diagnosis, have increased in recent decades. This is plausibly because of amplified awareness in this population, which has led to more frequent use of PSA testing, despite scientific controversy over its value (Hogle, 2009; Krantz, 2008). In Sweden, it is possible for all men to get a PSA test if they have worries about prostate cancer or ambiguous symptoms. One consequence of this is that it diagnoses apparently healthy individuals (Hogle, 2009; Krantz, 2008; Swedish Urological Association, n.d.).
The negative effects of treatment on sexuality for men diagnosed with prostate cancer are quite well explored. Surgery as well as radiotherapy and brachytherapy can damage the nerves and blood vessels that are needed for an erection. Hormonal therapy reduces the levels of testosterone essential for sexual desire and erection (Galbraith & Chrighton, 2008; Moore, 2009; National Cancer Institute, 2007). Many of the sexual consequences can have significant negative effects on the quality of life in cancer survivors (Galbraith & Chrighton, 2008; Hughes, 2000; Tierney, 2008). However, even if sexual dysfunction and its negative effect are well explored, a more holistic view of men’s sexuality is rare. Some studies indicate that men are poorly prepared to symptoms typically associated with being a woman such as gynecomastia and hot flushes (Galbraith & Chrighton, 2008; Gray et al., 2005). In this article, the definition of sexuality from the World Health Organization (WHO) is used, where sexuality is seen as a central part of human needs throughout life. It is practiced and articulated in who we are, what we feel, what we think, and what we do. Sexuality emerges in a dynamic mix of biological, psychological, socioeconomic, cultural, ethical, and religious/spiritual factors (World Health Organization, Pan American Health Organization, & World Association for Sexology, 2000).
Sweden, where this study takes place, is known as a liberal country in terms of sexual freedom and observance of equality between the sexes. Sexual education as a topic in comprehensive schools was introduced in the 1960s, and men have been allowed to go on parental leave since 1974. Sweden was also the first country to initiate legislation criminalizing the pay for, but not the sale, of sexual service in 1999 (Swedish Government Official Reports, S.O.U., 2010). Nevertheless the culture still seems to be built on strong ideals of hegemonic masculinity and sexuality (Centerwall, 2003; Holter, 2005; Plummer, 2005). The theory of hegemonic masculinity proposes that there are different types of masculinities, which are hierarchically organized and part of legitimizing patriarchal structures in society. The ideal hegemonic masculinity is built on heterosexuality and specific performances of masculinity related to virility, power, and the ability to act (Connell, 2003). Even if hegemonic masculinity is perceived as a quality of those in power, it is a model that individuals tend to strive for and a model that every man will be compared with (Connell, 2003). Hegemonic masculinity stresses sexuality more as instrumental and performance related rather than emotional and connective, which limits men from expressing their sexuality in various ways (Brubaker & Johnson, 2008). As a result of this, it is common that men in modern society separate sexual function and urinary incontinence from sexuality (Plummer, 2005).
The relationship between prostate cancer and masculinities is most complex and not well explored (Broom, 2009; Oliffe, 2009). Research has identified that men who are unable to be flexible in their masculinity are particularly at risk of negative psychological and/or psychosocial effects when they are diagnosed with prostate cancer and thus their masculinity is put under pressure of change (Maliski, Rivera, Connor, & Lopez, 2008; Stansbury, Mathewson-Chapman, & Grant, 2003; Wall & Kristjanson, 2005). Men in contrast to women are less likely to seek help in different group activities (Burns & Mahalik, 2007; Dunn, Steginga, Occhipinti, McCaffrey, & Collins, 1999). For couples, where the men are suffering from prostate cancer, studies have proven that women also are in need for emotional support. Men and women seem to think and respond differently about sexuality in this context. They express a mutual need for individual information about how to improve their sexual life depending on the situation (Heyman & Tarler Rosner, 1996; Sanders, Pedro, O’Carroll Bantum, & Galbraith, 2006). The reason for this is probably complex. In a previous quantitative study, both prostate cancer patients and their partners experienced a high degree of sexual dysfunction. This study confirmed that the communication patterns that the couples used affected their sexual relations. Constructive communication was associated with less marital adjustment in spite of the participants’ own levels of sexual gratification (Badr & Taylor, 2009). In Daker-White and Donovan’s (2002) focus group study, about sexual satisfaction in hospital patients’ accounts of their (hetero) sexual relationships, sexual intercourse could be understood as a transaction for the exchange of emotion and intimacy (Daker-White & Donovan, 2002). Another study in this population showed that having a sexually active partner was important for men’s ability to continue a satisfactory love life after prostate cancer diagnosis (Schover et al., 2002). The theory of hegemonic masculinity described by Connell is criticized for its one-sided stress on power (Seidler, 2004). Even if the issue of power is essential in gender studies, consideration also has to be paid to men’s emotions, fears, and other individual experiences (Seidler, 2004). It can be useful to understand hegemonic masculinity as working on different levels in the society, where individual men adopt or distance themselves from the hegemonic model depending on the situation (Connell, 2005). The modern Western societies are highly complex and for the modern man there are an amount of different strategies to use when they cannot any longer live up to the ideals in the societies (Cushman, Phillips, & Wassersug, 2010; Nielsen, Brixen, & Huniche, 2011).
Friendship between men has been proven to be more instrumental than that in women; that is, through sharing of activities with other men, they feel close to each other. In friendship between women, self-disclosure is more common than it is between men (Brubaker & Johnson, 2008). Charmaz’s (1995) research on men living with a chronic disease indicated that the male’s hierarchical position often changes in these situations. Since women are usually subordinated to men, the changes in relationships between men and women are less than those among healthy men. According to the ideal of hegemonic masculinity, men in general depend on women for their well-being and, in this perspective, sexual health (Charmaz, 1995; Oliffe, 2009).
The aim of this study was to explore how men diagnosed with prostate cancer before the age of 65 years, in all stages, experienced and talked about changes in their sexuality due to cancer as a subgroup in the society.
Method
Four focus groups, intended to capture the meaning of sexuality, were used for this qualitative and inductive study. The benefits of the focus group design are that group processes can help the participants to explore and elucidate their own views by relating to each other. This interpersonal communication can highlight (sub)cultural values and/or group norms (Krueger & Casey, 2009). This is particularly important in studies of sensitive topics (Robinson, 1999). A focus group interview generally consists of 4 to 12 subjects and is synchronized by a moderator (Krueger & Casey, 2009). Given the sensitive nature of the topic of this study and the high levels of involvement from the cancer association’s members, the size of each focus group was limited to six males. This facilitates more open sharing of views and also gives everybody the possibility to make their voices heard (Krueger & Casey, 2009). This method can also be an opportunity for people to come together and share their experiences, a sort of intervention.
Sample
The 19 informants were recruited in different ways. First, an announcement about the study and an invitation to join it was placed in a magazine for members of prostate cancer associations. As a result, a handful of men signed up for some of the groups. Some of these men were chairpersons of a group and offered themselves to take care of the arrangements. This was the case in Focus Groups 1, 3, and 4. In those cases, the chairperson sent out an invitation to the members that suited the criteria, and the men who were interested to join addressed this back to the chairperson. In Focus Group 2, two men were recruited after help from one urological unit at a university hospital in Sweden. In this case, the men were selected by a nurse and received information about the study in a letter. In the letter, they were informed of the aim of the study and assured of confidentiality and the voluntarily nature of their involvement throughout the process. The letter also explained that one of the researchers (KK) would call them by phone a week later. It was not until this point that they could decide if they wanted to join or not. Altogether, the letter was sent to 10 men. The other three men in Focus Group 2 were recruited by the announcement in the magazine for members of prostate cancer associations. The research plan was approved by the Regional Ethics Committee in Linköping. In accordance with the Helsinki Declaration, the men were assured of confidentiality and of the voluntary nature of their participation during the whole process (World Medical Association, 2008). Before the group discussions took part they all had signed an informed consent form. The criteria for participation were as follows: prostate cancer at any stage and (a) age approximately 65 years or younger at the time of diagnosis, (b) 6 months or longer having passed since the diagnosis, and (c) Swedish-speaking. The study was performed with members of different prostate cancer associations. Cancer associations differ from support groups in that way that there are never professionals involved in associations. People who participate in voluntary organizations often have a higher socioeconomic status than average citizens. They also have certain abilities, for example, speaking in public and socializing with people (Söderholm Werkö, 2008). Voluntary organizations offer the members with a collective identity related to the members’ sense of who they are and to mutual definition. This also contributes to the ability of the members to accomplish empowerment (Söderholm Werkö, 2008). Characteristics of the focus group informants are demonstrated in Table 1. They all belonged to different cancer associations for prostate cancer. Most of these men were passive members. Six persons were involved in the board where half of them operated as supervisors in some of the groups.
Characteristics of the Focus Groups Informants
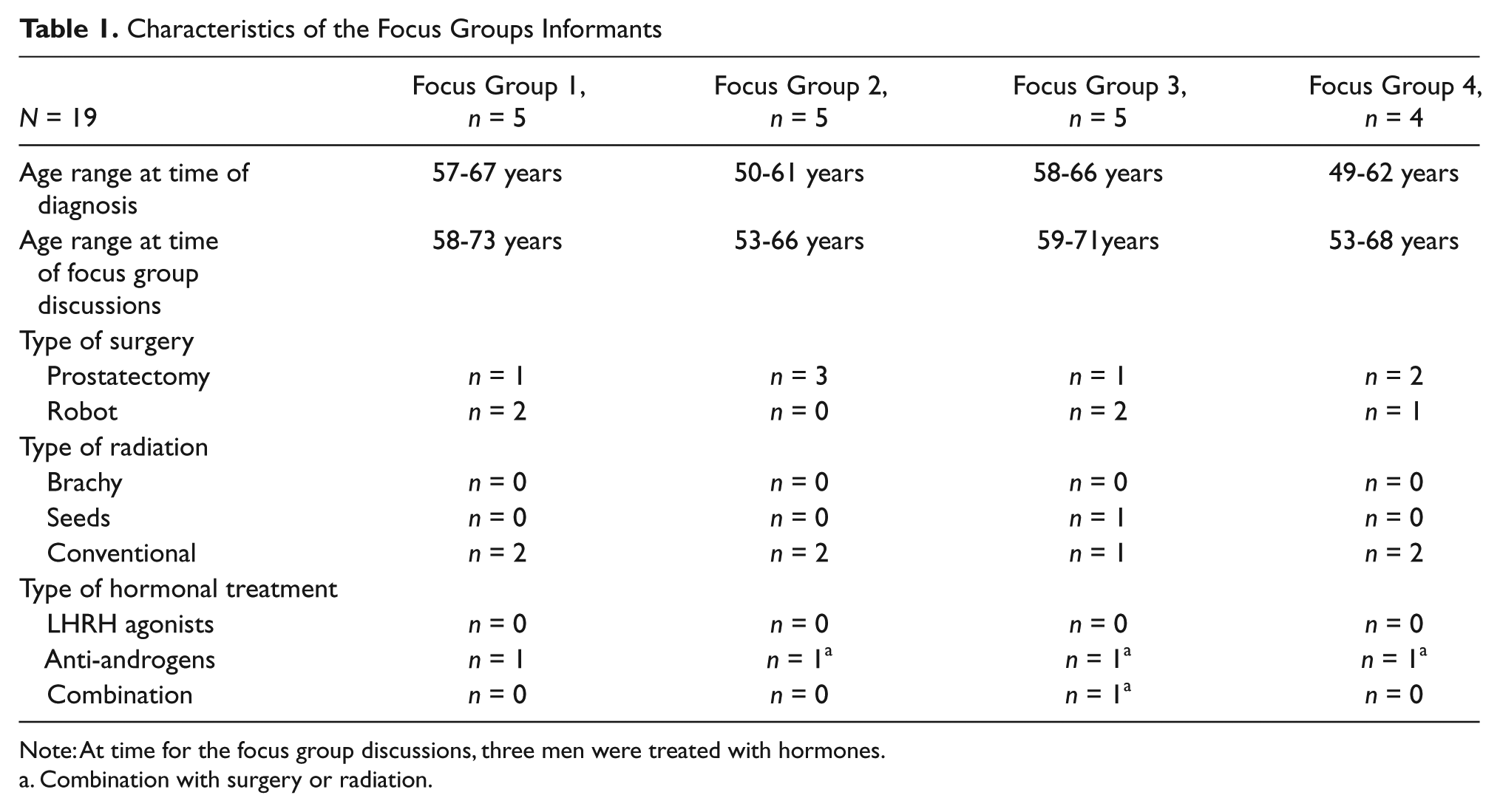
Note: At time for the focus group discussions, three men were treated with hormones.
Combination with surgery or radiation.
Procedures
The focus group sessions were carried out at the same place as where the associations had their regular meetings, with the exception of one group (Focus Group 2), where the focus group discussion was carried out in one of the oncological centers in Sweden. Before the sessions started, the moderator (KK) explained the purpose and the topic for the session, and everybody had to sign an informed consent form. First, there was some small talk in order to bring the informants together and to help them to get to know each other. As a trigger for the discussions, the film Through Sorrow and Joy—A Film about Cancer and Sexuality was shown. This 45-minute-long film was produced for people living with cancer or having a close relationship with someone who is, but it is also intended to provide insight into issues of sexuality for health care professionals (Korst, 2004). The group dynamics differed in each of the four groups. The moderator steered the focus of the group discussions and ensured that dialogue occurred among the group members rather than between them and the moderator. The moderator of the focus groups was a trained oncology nurse well acquainted with and responsive to the topics being discussed. In two of the four groups, an assistant researcher was present. The groups were rather small so no use for speakers log was evaluated to be necessary. The sessions lasted approximately 3 hours, and the discussions after seeing the film were audio-taped and lasted 100 to 120 minutes.
Analysis
The analytic process was inductive, and both manifest and latent qualitative content analyses without any hypotheses were used (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005). In the first phase, the ambition was to grasp the substance in each of the four focus groups and obtain a sense of whole. When this phase was completed, the organization of qualitative data began. This phase included open coding and the creation of categories. During this phase, the written manuscripts were read through again and as many headings as necessary were written down in the margins to illustrate all aspects of the phenomenon under study. This was a creative phase and the first author went back and forth through the text to discover patterns. After this, all of the texts were compared with each other to understand the underlying meaning, which is the latent phase. During this phase, the first author discussed and critically checked the importance of outliers with the other authors. We also discussed surprises and negative evidences in the data. During this stage we reviewed the illustrated sketches and referred back to the original text several times. By sorting the different categories to clusters with collective meanings, it was possible to abstract and label different subthemes and themes. Subthemes and themes overlap each other and were used instead of categories (Graneheim & Lundman, 2004). This demanding and serious work generated 14 subthemes and 4 themes (Table 2). After completion of the analysis, the findings were translated into English, and a native-born Englishman working with language revision had discussions with the researchers with the goal of finding and using words that correctly conveyed the nuances of the original speakers.
Presenting Subthemes Building and Included in the Themes Illustrating Prostate Cancer’s Effect

Results
Prostate cancer’s effect on the informants’ sexuality was captured in the 14 subthemes. These subthemes were included in the four themes that represented the abstraction of the statements in the four groups: a different kind of love, prostate cancer’s effect on masculinity, sex with technical aids and pills, and to lead the way and have the courage to talk. All the informants’ names have been changed in the text.
A Different Kind of Love
In this study, the majority of men were married or lived in long-term cohabiting relationships with females. The different sexual patterns that the couples had developed during these years were suddenly gone and a mutual acceptance of silence between the couples appeared. Sexual needs were suppressed when the ability of the informants to perform was the main stressor.
In the focus groups, the men stated that their partners showed great understanding for their situation and sexually they did not seem to dictate any own needs. To be satisfied in their love life after diagnosis, it was essential to be able to have a dialog, to really talk to each other about sexuality. This seemed to be difficult, and those few informants who had succeeded in this goal had been helped by a social worker, psychologist, and/or sex therapist. The turning point for Teddy and his wife, for example, came in connection with a visit by one of their mutual male friends to their country house. This man had also been treated for prostate cancer in the same way as Teddy and had successfully introduced technical aids into his life, about which he told them. When Teddy’s wife heard this, she started to cry. Then Teddy realized how much their sex life meant to his wife; this insight enabled him to consider his wife’s needs in a new way. After this episode, Teddy and his wife went to conversational therapy. Nowadays, Teddy can relax and accept that he does not have to perform. Even for those men, who claimed that they had a dialogue with their partner, a silent agreement appeared about the changed sex life prevailed.
One can fulfill each other in other ways for sure, but it is not so often. Intimacy and such things it will be in such cases. But it feels like, I don’t know, like a sort of silent agreement. [laughing] (One informant in Focus Group 4)
Many informants testified that they nowadays thought about sex as a duty, something they did more for her sake than for themselves. “One does it because; well, because of the wife’s needs. I don’t feel a need any longer; it’s dead I’m afraid” (One informant in Focus Group 2).
Fear, anger, and frustration were feelings that ran as a red thread throughout the four group discussions. This fear was above all associated with the feeling of not being a real man any longer but also the fear of death. From the narratives and statements from the discussions, it could be interpreted that the men perceived that they had suffered a huge loss. Something was gone and some men expressed that it felt like they had died a little bit and that they substantially missed their sexuality as it was before. On the other hand, there was also a lot of pleasure and joy for those informants who recovered their sexual function. To be able to get an erection in spite of everything, or sometimes learning to make love in different ways that still provided some pleasure, all this made the men feel much satisfaction. Tom in Focus Group 1 stated that he had tried every technical aid that was provided but suddenly he got an erection by himself. This was something that made him so happy that he cried the first time. This statement made Georg jealous:
Because as I said I live with a new woman whom I like very much but I can’t say that I have this immediate physical response, which turns it [the desire] on so to say. And which is also important for her to feel. This is not about words; it is about smell, about feelings. . . . But then I have to heat it up anyway and then I have to do some planning and [pause] yes I must say that I’m very jealous of you.
Although the men shared the same experiences, they interpreted them in many different ways, some of them contradictory. Mood changes, for example, were for some men an effect of disease, but during the discussions, the opposite meaning was also expressed. The informants expressed in words that they felt different from before and it seemed that they were all very sure that this was something psychological going on in their head. This was a huge frustration, especially for one informant, who believed that if he became okay in his head he would get his erection back.
In the different group discussions, it was noticeable that, during the sickness process, some men reevaluated their sexual life and a new definition of “the self” emerged. This process was strongly connected to their life situation overall. Sex was no longer so important; they were older and their partners were not so interested in it any longer. For those of the informants who had lived with the same partner for decades, some felt that sex was something of a routine anyway. Instead, the couples enjoyed traveling and appreciated fine food and drinks. Children and grandchildren became more important and some subjects reevaluated the importance of work, which for some meant continuing to work despite reaching retirement age, whereas for others it meant retiring. Working as an active member of a cancer association group gave approximately half of the informants a possibility to maintain a positive self-conception.
One can find new ways?
Yes that is what one has to do.
Mm.
And then it is as said, it was like I said: it is all about the family. I rejoice just as much when I get the grandchildren home on a visit.
Yes.
It is very pleasant.
Mm.
To hold them and hug but there is absolutely not a sexual thought.
No, but you can feel that your need is satisfied?
Yes, sure, the intimacy and tenderness like that [pause].
Prostate Cancer’s Effect on Masculinity
This theme symbolizes the informants’ self-identity during the illness transition. Virility, desire, and being able to have an erection were central and essential for how they expressed their potency. This potency was something different from other sorts of human experiences, but it seemed to be difficult for the men to explain why. It was not possible to compare it with the concept of sexuality on the whole or to compare it with women’s lust and desire. These experiences were most individual and how they dealt with them varied substantially. The feeling of being bereaved for their masculinity was collective in these experiences. Sexuality was experienced as self-evident before the diagnosis, but during the process of self-reflection, which occurred in the different sessions, the informants obtained new knowledge, which they generously shared with each other. The majority of the informants in all four groups had changed their habits related to sexual intimacy and intercourse with their partners. This was something that affected the informants deeply, but in different ways. It seemed as though they were convinced that this affected them more than their partners. For some of them, these changes also affected their self-esteem.
Before it is, and I think that it is worse for us males. I can only speak for myself anyway.
Yes of course.
It is probably worse for me than for my wife.
Mm.
She seems to have taken it rather well. She does not care so much about it.
She does not seem to miss it?
No.
No.
No, it is probably about our self-esteem as well.
Probably.
It does absolutely.
We cannot perform, and then we think that we are bad.
One man in one of the focus groups explained that he was afraid of intimacy with his wife after the operation because he was frightened of getting aroused, something which made him suffer from performance anxiety. Next day he called on the telephone and wanted to explain further what he meant. He said that during his rehabilitation period he got himself a dog. One day he met a younger woman who also had a dog. During a period they met several times. He felt that he was in love with this woman and that the feeling was reciprocated. Out of consideration to his wife but also due to the fact that his potency was unreliable their relationship only developed platonically. This was his first relationship with a woman that was not built on erotic feelings, and after this episode he could more easily accept that he no longer could live up to the hegemonic ideals in the society.
Another aspect that affected self-identity was related to the bodily changes that developed as a result of the different treatment regimes. The treatments that involved hormones were clearly described as having additional effects. However, even those men who underwent an operation as their only treatment also experienced bodily changes. There was, for example, an intense discussion about the size of the penis in Group 1, where the men were not aware of the risk of shortening of the penis, even though this is common after prostatectomy and/or treatment of hormones. The decreased virility and desire was for a majority the biggest change after treatment. One of the informants was treated with hormones before radiotherapy. For a year, he felt no desire toward his wife, and he remembered exactly the day when the hormones came back and desire was again present in relation to his partner.
The aftermath of cancer treatment could also affect men’s social interactions in a wider context. The possibility to have a mistress or to flirt with women in bars was not conceivable any longer. This was not a problem for the majority of the informants but, even for the more reserved men, the interaction with women had changed. Earlier these men were not unfaithful for moral reasons. Nowadays, the limitation was the fact that they were not potent any longer. Attraction to the opposite sex seemed to be an important dimension for their quality of life, which the quote below is demonstrating.
Sure, I don’t know if it is unique but . . . when men see a beautiful woman, we really think—wow that was a beautiful woman.
Mm.
But now it is no use for me to be interested. Not that I’m out chasing beautiful women.
No.
But anyway, you can still see—wow that was a beautiful woman.
The bodily changes due to treatments did change the men’s interaction with females in intimate as well as social contexts. This brought a new unfamiliar dimension into their lives and affected their overall quality of life and well-being.
Sex With Technical Aids and Pills
When attraction to the opposite sex had changed and virility and desire were diminished, sexuality was no longer something natural in the men’s lifeworld. Technical aids seemed to be very difficult to use successfully. Their use took away the spontaneity between the couples and led to sensations of pain in the genitals. For a majority, it took away all the joy connected with erotic pleasures. If oral medication alone was sufficient, it had the greatest potential to be accepted. In the four different groups, there was an abundance of experiences and knowledge about different technical aids and how to use them, which they eagerly shared with each other. In Focus Group 2, the men were more relaxed to talk about this than in the other groups. Jonny had first tried Viagra and other tablets with no effect. After this, he tried an injection, but this was also a disappointment for him and his wife. It was not until he bought some sex toys that he and his wife became satisfied. Now they can reach mutual orgasms without penetration, which they both appreciate. Something that is most frustrating for Jonny is the fact that these things are called toys. For him and his wife, these things are technical aids equal to other equipment that is used in the case of handicap.
There are other things . . . if you read the paper and in the shops, they sell sex toys. But I go crazy when they say sex toys—they are sex aids. They are aids. I mean if you got a walking frame or a pair of crutches, they aren’t toys.
The different group sessions made it possible for the informants to share their experiences with each other, and for the men, these sessions filled an unsupplied need. This part of sexuality, the more mechanical or technical dimension, seemed to be an area where health care organizations had arranged some support for the men. The routines for this support differed ever since they had been prescribed some PDE5 inhibitors without any follow-up, or visiting a nursing reception with more substantial advice. Nevertheless, there was severe criticism both verbally expressed and also implicit in the informants’ narratives. In Focus Group 3, there were three men who were also cancer association’s leaders and trained in supporting new members. These three men were convinced that the rehabilitation after treatment has to change and that issues about sexuality in particular have to be taken care of in a more supportive way. Harald’s prostate cancer was chronic and he was treated with hormones, which caused his libido to disappear. “And it must work in a better way [communication about sexuality in health care] because otherwise people will be tremendously disappointed about things. And this thing also shapes [pause] [sigh] bad relationships in the next phase.”
Urinary incontinence, which was a common effect in conjunction with operation and radiotherapy, seemed to be the most detrimental effect in terms of attractiveness and an acceptable love life. For the informants in this study, this was a substantial obstacle during the first period after treatment. In spite of this, the discussions indicated that the informants did not link urinary incontinence and its aftermath to sexuality as a whole. If the men lived in a trusting and caring relationship and with the help of pelvic floor exercises, it was possible to overcome this obstacle over time for most but not all of the men. Melker was diagnosed with prostate cancer 5 years previously at the age of approximately 50 years. Ever since his prostatectomy, he had been suffering from severe urinary incontinence. In time for the focus group discussion, his libido was nonexistent owing to hormone treatments, and injection with Caverject was the only way to have an erection. Unfortunately, urinary incontinence was an obstacle for this.
Later on I got a kind of injection. Like a diabetic injection that I got to try there [at the hospital] on the toilet. And this injection had some effect, it really had, but at the same time it doesn’t feel so great when one pees in one’s pants. There is also the problem that you don’t want to pee in your woman, so to say.
Sex was transformed to something artificial and some experienced that they were no longer able to show their partner love and passion. Technical aids and/or pills were something essential for any possibility of being intimate and reaching mutual satisfaction. Unfortunately, the men did not feel that they received the right support from doctors and nurses to give them enough skill to be able to incorporate the aids and pills into their sex lives. At the same time, they blamed themselves for being passive and perhaps giving priority to other issues, when they had an appointment with a health care professional. During the sessions, the complexity of sexuality was elucidated and some good examples of support from health care workers that were beneficial for the men were described. In the discussions, no informants mentioned a wish to discuss this topic only with male doctors or male nurses. Instead, there were wishes to meet health care workers who were mature in their own sexuality and had a great interest in the topic.
To Lead the Way and Have the Courage to Talk
Most of the men did not have any problem identifying themselves as a member of a cancer association. As a matter of fact, they tried to benefit from their situation in recruiting new members. Some of these men became engaged with the issue in the media and wrote debate contributions concerning prostate cancer for publication; they also undertook some promotional activities to attract new members. On the other hand, the discussions during the different sessions indicated that these men were a special group owing to their openness about sexuality. As a role model, the former Swedish Minister of Finance, Kjell-Olof Feldt, played an important role for the informants regarding the ability to change their understanding of cancer and give them courage to talk about their own situation with people in all sorts of situations. The informants received solace and confidence from his book about the experience of suffering from prostate cancer. To lead the way and to have the courage to talk about such sensitive topics as prostate cancer and its influence on the genitals and sexuality was in this study very important for the self-understanding of these men.
Being associated with a group of elderly men smelling of urine seemed to be something that the informants wished to avoid.
When I sat in the waiting room, there was another man who was elderly. We talked a little and he had his wife with him. Then he said: “I don’t care about this thing about sex as long as I don’t go around smelling of urine.” Well this is not kind of funny. Yes, it is noticeable if one goes to visit relatives. I have had my parents in an old people’s home, and when it smells of urine it’s not funny. It feels bad.
During the group sessions, it was evident that issues of sexuality were difficult to share and to talk openly about. In Focus Group 1, there were two men who were their complete opposites. Tom, who could talk about everything concerning his diagnosis, including sexuality, was also involved with seminars together with his urologist with the goal of bringing light to the topic.
Everybody in the world of sports knows me and I tell them: What the hell, I’m an old prostate cancer geezer. If you have any questions, I’ll get up and talk about it. And the sport clubs, lots of them, they say come and talk about it. What the hell, they are shocked. You don’t look sick. No I’m not sick but I’m a cancer patient.
Conny, on the other hand, was joining the support group for the first time and he could only talk with his family about his situation. He worked as a businessman and was convinced that his image could be hurt if he was associated with prostate cancer.
I would think that it was bloody unpleasant if I was to appear in a newspaper. If I’m out in the field and meet a lot of people, I’m a salesperson and traveling around in Sweden, meeting pretty girls who are purchasing managers. So you have prostate cancer they say, we read it in the newspaper.
During the four group discussions, the symbolism of the phallus in society was discussed both explicitly and implicitly. This seemed to have a dual meaning for the informants. Dual in that sense that they were convinced that getting an erection was a man’s right in a way. On the other hand, they should be grateful for their treatment and happy to be alive. The discussions in the different four focus groups made it evident that men living with a diagnosis of prostate cancer experienced a gap between their self-perception and their social identity. It seems as hegemonic masculinity is hidden in social norms and ideals. This, in turn, obstructs people’s abilities to cope and renegotiate their identity which in the long run effect sexual health and well-being in these populations.
But what it is, is that we never do it [talk about sexual feelings]. We have never done that. There isn’t any teenage boy who runs around telling his buddies that he thinks that he has problems with girls, and so it will continuing during the whole life. We are shaped that way. We don’t sit down and cry and talk. Instead we go home and feel very bad [the others in the group agree]. I remember once in my teenage when I felt bad, what did I do, I drank my father’s Genever [everybody laughs].
Discussion
The findings, from these four focus group sessions, elucidate men’s vulnerability as a group in the society when prostate cancer affects their ability to perform sexually. Even though these experiences are most individual, the ideal of hegemonic masculinity influence men’s ways to cope and interact, which is illustrated to special themes in this study: a different kind of love, prostate cancer’s effect on masculinity, sex with technical aids and pills, and to lead the way and have the courage to talk.
From a biomedical perspective, prostate cancer is not a disease with a high mortality rate. However, individual prognostic approaches are poorly developed and around one fifth of affected men have already progressed to a chronic stage by the time of diagnosis. As in Brooms (2009) study, men have to balance the possibilities for cure in contrast to potency continuously through their illness trajectory, which influenced how they talked in the different sessions. This we already know can have a huge impact on how men view themselves concerning their masculinity (Burns & Mahalik, 2007; Connell, 2005; Gray, Fitch, Fergus, Mykhalovskiy, & Church, 2002). In this study, the different group sessions made it possible for the informants to share their experiences with each other, and for these men the sessions filled an unsupplied need. In these groups, the men were able to discuss sensitive issues without losing face, for example, how their bodies failed and changes in their close relationships, which were illustrated under the theme, a different kind of love. The friendship between the men in the different groups was obvious and probably highly beneficial for their well-being and efforts to cope with their sexuality. The informant’s motivation as well as ability to communicate with their partners was a prerequisite for achieving a satisfactory love life. In current study, the majority of the informants lived with females of the same age as themselves, where sexual intercourse was something of a routine. The motivation above all to maintain this routine seems to be less, for the women related to the discussions in the focus groups. This is rather contradictive since earlier studies suggest that having a sexual active partner has been most beneficial in this context (Schover et al., 2002). The reason for this is probably complex. As reported in the background section, communication patterns between couple do affect sexual health and well-being and that individual gender perspective influence the need of information and support in this area (Badr & Taylor, 2009; Heyman & Tarler Rosner, 1996; Sanders et al., 2006). Another study in this population showed that, in addition, the fact that the interaction with females in general and partners in particular changed indicates that the experiences of living with a prostate cancer diagnosis are both existential and biological in nature. This is something that has been observed in other qualitative studies in the same Swedish population, in the United Kingdom, as well as in Australian studies (Gray et al., 2002; Kelly, 2009; Lindqvist, Widmark, & Rasmussen, 2006; Oliffe, 2005). According to the ideal of hegemonic masculinity, men in general depend on women for their well-being and, in this perspective, sexual health. Men who have the courage and acceptance to be able to talk about the issues dealt with in this study could probably have other advantages in terms of the quality of their close relationships and intimacy, which was in fact indicated herein. The men’s feeling of an unspoken agreement not to discuss the changes in their sex lives with their partners indicates that these issues are difficult to talk about. Daker-White and Donovan’s (2002) study was intended to shed light on what disturbances meant to sexual function for heterosexual couples. In this previous study and in the present study, sexual intimacy was transferred by the erect penis and thus it was not easy to discuss the problem of impotence when it occurred (Daker-White & Donovan, 2002).
The history and cultural attitudes in our modern societies is visible in the theme prostate cancer’s effect on masculinity. These men’s invisibility is articulated, according to the norm that a modern man is expected to be sexual active and virile for as long as he lives. This includes urine incontinence, something difficult for the men to adapt to, and so are all experiences that are embodied. Shame more than anything else is connected to these experiences. This can probably be explained by domination of the phallocentric model of sex in modern society, which in turn affects hegemonic masculinity (Plummer, 2005). Therefore, it is not strange that, in biomedical discourses, impotence is presented only as a physiological event. Consequently, it is nearly impossible to meet the men in a way that promote personal development. Even health care professionals separate urinary incontinence from sexuality, and the target for the health care service is to educate the men in pelvic floor exercises and supply men with diapers. However, this is perhaps not what the average man needs. He needs a holistic view that includes both physiological and psychological approaches. He has to learn to cope with the insecurity of experiencing urinary leakage, and perhaps most important, he has to cope with the insight of not being able to match the masculine ideals but rather find new ways to be masculine. To our knowledge, this is a rather unexplored experience, which only has been discussed in the group of men with advanced prostate cancer and their castration (Cushman et al., 2010; Gray et al., 2002; Oliffe, 2006). Another interesting finding was the informants’ difficulties in accepting and adapting to the use of technical aids in their sexual life, which was demonstrated in the theme sex with technical aids and pills. Their use took away all the joy connected with erotic pleasures and reduced the informants’ motivation. As in Arrington’s (2003) study, there was an unwillingness to become an “artificial man.” This is perhaps not surprising as that the informants in our study further testified that such aids are connected with pain and discomfort in the genitals. Additionally, both the joy as well as spontaneity connected with love and lovemaking was lacking. This is in line with two other qualitative studies in the same context (Arrington, 2003; Fergus, Gray, & Fitch, 2002). Primarily, the men who were able to reevaluate the value of penile-vaginal penetration had the best chances to redefine their sexual identity, which, in some cases, meant incorporating technical aids into their sex life. The fact that it has been possible to buy sex aids at pharmacies in Sweden for a couple of years now has probably been helpful for this group of persons.
The theme to lead the way and have the courage to talk is probably a product of the context that this study emanates from. Men with prostate cancer are, as a group, more vulnerable than other men suffering from illness according to its affects on the sexual organs and ability to perform intercourse. Therefore, role models and cancer associations have a positive influence in this population, which the discussions and dialogues in these four group sessions indicated. These role models and cancer associations can at best help men to develop a new and broadminded confidence and self. The current study demonstrated that men are able to talk and respond on a more individual and sensitive way under the right conditions, as already had been observed in Seidler’s (2004) critics of Connells theory. The outcomes for health and well-being in male populations are often not predictable and stereotyped, even if the hegemonic ideals can be recognized (Nielsen et al., 2011).
In the context of prostate cancer associations, the intimacy produced in these groups is an important part of male friendships. This male friendship built on the experience of “being in the same boat” supplies men with collective reciprocity of not being alone. This can be most beneficial for the transformation of feelings connected to the crisis that cancer often brings (Adamsen, Midgaard Rasmussen, & Sonderby Pedersen, 2001; Oliffe, Gerbrandt, Bottorff, & Gregory Hislop, 2010).
Trustworthiness
In this study, exploring a sensitive and in many ways difficult topic, it was rather complicated to recruit quite enough informants. Therefore, different approaches were used to recruit informants and this is perhaps the reason for the homogenous nature of the groups. All the informants were heterosexual and most of them were living in long-term relationships with females. Also, the fact that some of the informants were deeply engaged in prostate cancer associations made them not representative for the majority in this population.
Something that could influence the findings was the sex of the researchers and the translation to English. The sensitive topic and the qualitative inductive approach can obstruct the clarification of the findings. However, the researchers were aware of this and made arrangements for the men to feel trust and reliance as long as possible. The researchers represented two different scientific traditions (nursing and sociology), which can be an advantage during the analyzing process (Perry, Thurston, & Green, 2004). To preserve the genuine tone and meaning in various statements, special arrangements were done. A skilled and experienced proofreader was used and the coauthors are well qualified in the English language. Some of the same findings were made in similar studies in comparable populations, which strengthen their validity. Qualitative studies such as these are not intended to produce findings that are generalizable to the whole population; however, the findings of this study could be transferable to similar groups of men elsewhere.
Conclusions and Implications
In the future, patients, as well as their partners, have to be invited to talk and reflect before, during, and after their treatments about their life situation, with a focus on masculinity and sexuality. Similar to this study, the use of men’s groups ought to be a beneficial alternative during the rehabilitation phase. This can probably be established on a wide scale if health care services and cancer association members cooperate, something is not routine at present. Psychosocial oncology, including sexuality, should be of higher priority in the health care organizations. The professionals have to be mature and safe in their own sexuality to manage this priority. By letting regular preceptorship and other tutorials play an important part in the health care organizations, the professional skills will develop.
The erotic part of sexuality and support with medical and technical advice could be usefully captured with regular questionnaires. It should be evident from the medical records if the patients wish to fill in such questionnaires, and if they do, follow-ups are important. Educating resources including booklets, websites, and other informative materials increase the opportunities for the patient to obtain knowledge about his body and the sexual consequences of the disease. It should be natural to offer regular patient education sessions, which will complement the care. Then the patient alone can decide when and whether or not to learn about cancer and its outcomes.
More of interdisciplinary research is desirable in the future in these male populations. The relationship between couples is one important and undeveloped area. Ethnicity and homosexuality are topics that deserve more efforts in future research.
Footnotes
Acknowledgements
The authors are grateful to all those men who participated in the study and shared their experiences with us.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful to The Skaraborg Institute for Research and Development, The Research and Development Unit at Skaraborg’s Primary Health Care, and The Faculty of Health Sciences, Linköping University, for financial support.