
Abstract
Research examining psychosocial functioning in African American prostate cancer survivors has been limited, in spite of documented higher mortality from prostate cancer and worse long-term physical and emotional outcomes from prostate cancer treatment reported by this group of survivors. In addition, the role of masculinity in psychosocial adjustment among prostate cancer survivors is not well understood. In this study, 59 African American prostate cancer survivors completed a questionnaire assessing masculinity beliefs related to self-reliance, emotional control, and dominance, as well as measures of psychosocial functioning (i.e., symptom distress, negative mood, and functional and social well-being). Results of regression analyses indicated that masculinity beliefs predicted negative mood, functional well-being, and social well-being, controlling for age, income, and medical comorbidities. The findings reported here, although preliminary, suggest that masculinity beliefs could be important therapeutic targets for improving the efficacy of cognitive-behavioral interventions for men adjusting to prostate cancer survivorship.
Introduction
Prostate cancer disparities have been well documented for African American men, including a 60% higher incidence rate, later stage at diagnosis, and a mortality rate that is more than twice that of Caucasian men (American Cancer Society, 2011). To address these disparities, medical research has focused increasingly on early diagnosis and treatment of prostate cancer among African American men, resulting in increased survival rates (American Cancer Society, 2011). However, little attention has been paid to posttreatment survivorship issues where disparities have been documented. African American men report slower recovery from prostate cancer treatment, more dissatisfaction, and regret following prostatectomy (Schroeck et al., 2008); more persistent problems with sexual, urinary, and bowel symptoms (Lubeck et al., 2001; National Cancer Institute, 2004); and greater emotional distress in response to having cancer compared with Caucasian men (Campbell et al., 2004; Rodrigue, 1997). In spite of the evidence that African American men experience worse long-term physical and emotional outcomes from prostate cancer, research examining psychosocial functioning in African American prostate cancer survivors has been limited (Weber & Sherwill-Navarro, 2005).
One variable that is potentially quite important, but that has not been addressed in prior work with African American prostate cancer survivors, is conformity to majority culture norms on masculinity (often termed traditional masculinity). Such norms include emotional control, self-reliance, and social dominance (Mahalik, 1999; Mahalik et al., 2003; Lazur & Majors, 1995). Men who have been treated for prostate cancer often experience physical symptoms (e.g., sexual or urinary dysfunction; Litwin et al., 1995; Potosky et al., 2000) and can experience related emotional difficulties (e.g., depression, heightened emotionality; Weber & Sherwill-Navarro, 2005) and social changes (e.g., social isolation, concerns about losing intimate relationships) that conflict with these common beliefs about masculinity. As a result, survivors may perceive a diminished sense of manhood, which could have a negative impact on their psychosocial functioning.
Previous research suggests that men who conform to more traditional views of masculinity report increased emotional distress, including higher depression and anxiety (Good et al., 1995; Courneyer & Mahalik, 1995). African American prostate cancer survivors may be particularly vulnerable in the face of a threatened sense of manhood since they are caught in a bind between maintaining a strong masculine image consistent with the majority culture as a buffer against racism, powerlessness, and socioeconomic disadvantage on the one hand (Mahalik, Pierre, & Wan, 2007) and accommodating the realities of their illness on the other. However, researchers are only just beginning to explore how masculinity beliefs affect prostate cancer survivorship.
An earlier study by Burns and Mahalik (2006) reported that, in a sample of 230 men treated for prostate cancer, men with poor physical health who held more strongly to traditional masculinity views about self-reliance and emotional control reported much worse mental health. In contrast, men with poor physical health who believed less strongly in traditional masculine norms related to self-reliance and emotional control reported much better mental health. However, in this study there were only six African American men in the sample (3%), which limits the extent to which these findings can be generalized to African American prostate cancer survivors.
Another study of masculine conformity and psychological functioning by Mahalik et al. (2007) employed a larger sample of African American men (aged 18-25 years). The results of this study indicated that greater conformity to traditional masculine norms was associated with lower self-esteem and higher psychological distress (Mahalik et al., 2007). However, because the participants in this study were young men who were not prostate cancer survivors, the findings may have limited generalizability to middle-aged and older men coping with the physical, emotional, and social challenges of prostate cancer survivorship.
This study addresses the gaps in the research literature noted above by examining conformity to traditional masculinity norms related to self-reliance, emotional control, and social dominance in a sample of middle-aged and older African American prostate cancer survivors. Specifically, this study examines how variations in masculinity beliefs are related to important indices of psychosocial functioning (symptom distress, self-efficacy for symptom control, negative mood, functional well-being, and social well-being).
Method
The study was approved by the Institutional Review Board of Duke University Medical Center. All participants underwent the informed consent process and gave written consent prior to participating in this study.
Participants and Eligibility
Participants were African American prostate cancer survivors who received active treatment (i.e., surgery, radiation, hormone therapy) for localized prostate cancer within the previous 2 years. Eligibility was confirmed by each participant’s physician.
Recruitment
An important recruitment aim of this study was to reach an economically diverse population of African American men, including the economically disadvantaged and the medically underserved. To achieve this aim, recruitment was carried out in both clinical settings and through community outreach. Clinic-based recruitment was coordinated through the Duke University Medical Center Prostate Center. Community recruitment involved comprehensive outreach using newspaper and web-based advertising and community-based prostate cancer advocates serving African American communities. As a result, 37% of participants were self-referred in response to our outreach efforts. Sixty-three percent of participants were clinic-referred.
Measures
Demographic information
Demographic data collected included participant age, education, income, prostate cancer treatment modality (e.g., surgery or radiation), and comorbid medical or psychiatric conditions.
Masculine conformity
Masculine Conformity was assessed using three subscales (21 items) of the Conformity to Masculine Norms Inventory (CMNI; Mahalik et al., 2003), which assess the extent to which an individual desires to conform to masculinity norms related to emotional control, self-reliance, and pursuit of power/dominance. The CMNI has demonstrated validity and reliability (Mahalik et al., 2003). Reliability coefficients (Cronbach’s αs) for CMNI subscales for the current study were .82 for the emotional control subscale, .72 for the self-reliance subscale, and .56 for the dominance subscale. Alpha coefficients are reported similarly for all other study measures described below.
Measures of Psychosocial Functioning
Symptom distress was assessed using the Expanded Prostate Cancer Index Composite (EPIC; Wei, Dunn, Litwin, Sandler, & Sanda, 2000). The EPIC is a 50-item scale that assesses symptom severity and symptom distress in sexual, urinary, and bowel symptom domains related to prostate cancer treatment. Sexual Bother, Urinary Bother, and Bowel Bother subscales of the EPIC were used to assess Symptom Distress. Higher scores on these scales reflect less symptom distress. Each of these subscales has demonstrated good internal consistency in African American prostate cancer survivors (Campbell et al., 2004). In the current study, Cronbach α coefficients were .78 for the urinary bother subscale, .75 for the bowel bother subscale, and .72 for the sexual bother subscale.
Self-efficacy for symptom control was assessed using a modified version of a standard self-efficacy scale (Lorig, Chastain, Ung, Shoor, & Holman, 1989). This 22-item self-efficacy scale has shown good reliability in previous research with African American prostate cancer survivors (Campbell et al., 2004) and includes three subscales: symptom management self-efficacy (i.e., confidence in managing cancer-related symptoms), coping-self-efficacy (i.e., confidence in coping with emotional aspects of cancer), and functional self-efficacy (i.e., confidence in one’s ability to function in spite of symptoms). In the current study, all three self-efficacy subscales demonstrated excellent reliability. The coefficient αs were .92 for symptom management self-efficacy, .96 for coping self-efficacy, and .95 for functional self-efficacy.
Negative mood was assessed using the depression and tension (i.e., anxiety) subscales of the Profile of Mood States-SF (POMS; Lorr & McNair, 1982). Higher scores on these POMS-SF subscales indicate more distress. The POMS has been used previously in prostate cancer research (Clarke & Talcott, 2001; Ulrich, Carson, Lutgendorf, & Williams, 2003) and demonstrated good reliability in the current study sample, with α coefficients of .82 (Depression subscale) and .74 (Tension subscale).
Functional well-being was measured using the Functional Well-being subscale of the Functional Assessment of Cancer Therapy–General (Cella et al., 1993). This subscale includes seven items that assess survivors’ ability to carry out life activities that can be negatively affected by cancer treatment (e.g., work, leisure activities). Evidence supports the reliability of this subscale (Cella et al., 1993). In the current study, the functional well-being subscale demonstrated good internal consistency with a coefficient α of .86.
Social well-being was measured using the seven-item Social/Family Well-being subscale of the Functional Assessment of Cancer Therapy–General (Cella et al., 1993). This subscale assesses survivors’ perceived support from family and friends. In the current study, the α coefficient for the social well-being subscale was .71.
Statistical Analyses
Descriptive statistics were calculated including means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Correlational analyses were conducted to identify associations between demographic variables and key study variables and among key study variables. Hierarchical multiple regression analyses were then conducted to evaluate how well masculine conformity predicted symptom distress, self-efficacy for symptom control, negative mood, and physical and social functioning, over and above demographic factors. For each regression model, demographic variables found to be significantly correlated with measures of masculine conformity and psychosocial functioning were entered into the model first, followed by masculine conformity indices.
Results
Descriptive Statistics
A total of 59 participants completed a baseline questionnaire battery as part of a pilot randomized controlled trial comparing two supportive care interventions. The mean age of participants was 61.2 years (SD = 8.3). Most participants were married or partnered (85%) and received prostate surgery as their primary form of treatment (64%). Forty-three percent of participants were college graduates, 44% were working full-time or part-time, and 80% of participants reported middle-income levels or higher. Descriptive statistics for demographic variables are summarized in Table 1 and Figures 1 and 2. Means, ranges, and standard deviations for masculinity subscales and other psychosocial measures are provided in Table 2.
Demographic Characteristics (N = 59)
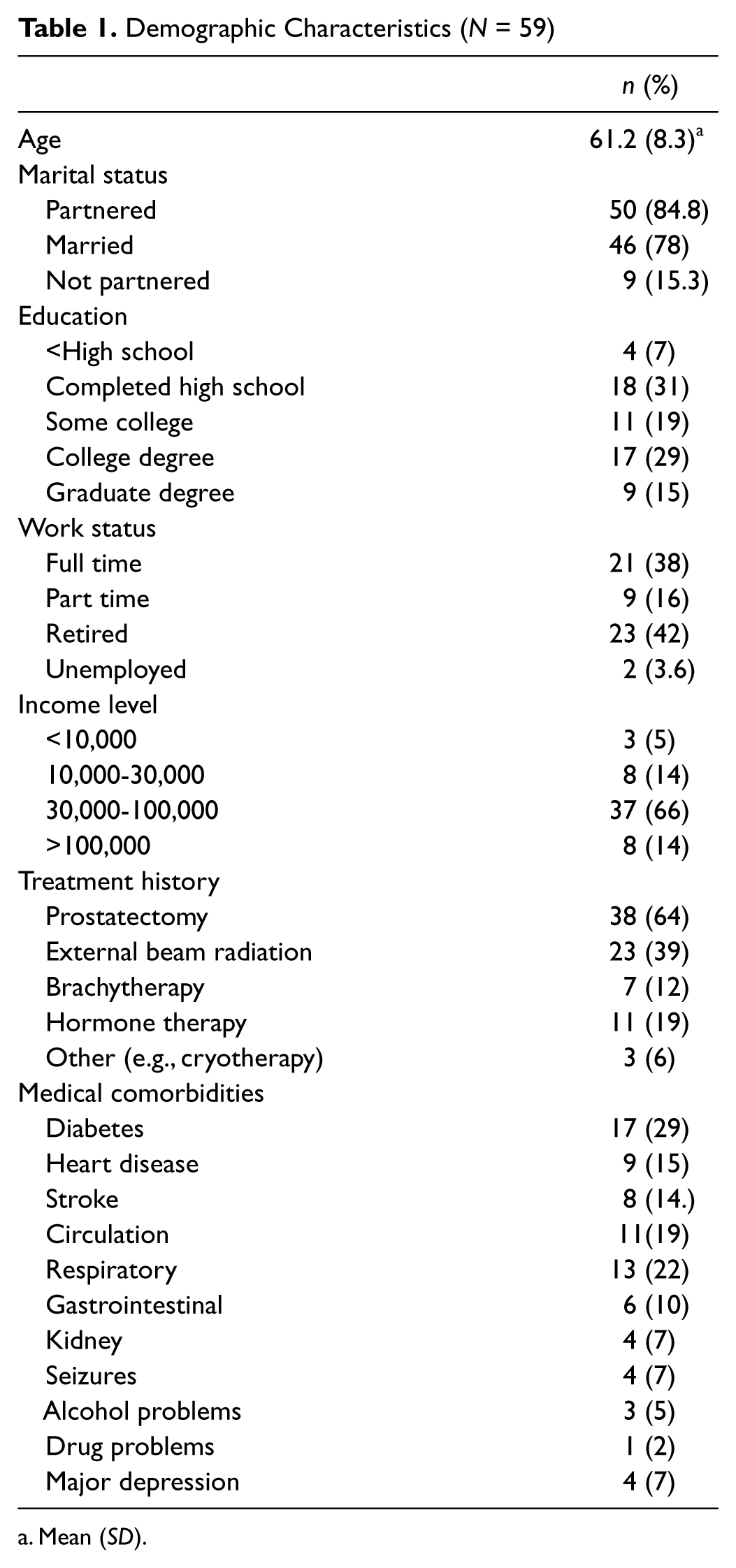
Mean (SD).

Demographic characteristics

Treatment history and medical comorbidities
Means and Standard Deviations for Self-Efficacy, Masculine Conformity, and QOL Variables

Note. EPIC = Expanded Prostate Cancer Index Composite; POMS-SF = Profile of Mood States-SF; FACT-G = Functional Assessment of Cancer Therapy–General.
Correlational Analyses
Demographic variables and key study variables
Several significant correlations were observed between demographic and key study variables; however, none of the correlations should be interpreted as implying causality.
First, older participants reported stronger masculinity beliefs about emotional control and less urinary symptom distress. Second, participants reporting a higher income level also reported higher functional self-efficacy (r = .52, p < .001) and functional well-being (r = .42, p < .01) and lower levels of depression (r = −.36, p < .01). Third, patients with a greater number of medical comorbidities also reported lower symptom management self-efficacy, coping self-efficacy, and functional self-efficacy (r = −.36, −.34, and −.43, respectively; all p values < .01), functional well-being (r = −.294, p < .001), and more depressed mood (r = .29, p < .05). In sum, of the demographic variables examined, age, income, and medical comorbidities were each related to one or more measures of masculine conformity and psychosocial functioning.
Correlations between masculine conformity and psychosocial variables
Unadjusted correlations between masculine conformity subscales and psychosocial variables indicated that self-reliance was significantly positively correlated with tension/anxiety scores, r(58) = .32, p < .05, and significantly negatively correlated with social well-being, r(59) = −.37, p < .01. Analyses also indicated that dominance was significantly positively correlated with depression scores, r(59) = .39, p < .01, and significantly negatively correlated with coping self-efficacy, r(59) = −.33, p < .05, functional self-efficacy, r(59) = −.30, p < .05, functional well-being, r(59) = −.43, p < .01, and social well-being, r(59) = −.49, p < .001. These correlations are presented in Table 3.
Masculine Conformity Subscale Correlations With Symptom Distress, Self-Efficacy, Negative Mood, Physical Functioning, and Social Functioning Subscales

Note. POMS-SF = Profile of Mood States-SF; FACT-G = Functional Assessment of Cancer Therapy–General.
p < .05. **p < .01. ***p < .001.
The low alpha coefficient for the Dominance subscale (.56) identified in this study suggests that, in this sample, this subscale may not be reliably capturing the traditional masculinity norm related to dominance. To explore this further, each of the four items in this subscale was correlated with the psychosocial variables. An adjusted α of .005 was used to test for significance (.05/10 subscales). The item “In general, I must get my way” was significantly negatively correlated with physical functioning, r(58) = −.37, p < .005. The item “I should be in charge” was significantly negatively correlated with physical functioning, r(58) = −.41, p < .005, and social well-being, r(58) = −.41, p < .005. The item “I make sure people do as I say” was significantly negatively correlated with the functional self-efficacy, r(58) = −.38, p < .005, physical functioning, r(58) = −.37, p < .005, and social well-being, r(58) = −.41, p < .005. The item “I’m comfortable trying to get my own way” did not correlate with psychosocial variables when using the adjusted alpha level. To promote comparability across other studies using this subscale, we did retain the full Dominance subscale in the analyses but associations between this scale and other study variables are interpreted with caution.
Regression Analyses
Hierarchical multiple regression analyses were conducted to examine the unique contribution of masculine conformity beliefs to symptom distress, self-efficacy for symptom control, negative mood, functional well-being, and social well-being, controlling for age, income, and medical comorbidities (see Table 4).
Regression Results Predicting Negative Mood, Functional Well-Being, and Social Well-Being

p < .05. **p < .01.
Symptom distress and self-efficacy for symptom control
The results of the regression analyses indicated that, after controlling for age, masculine conformity was not a significant predictor of symptom distress. Similarly, after controlling for age, income, and number of comorbid medical conditions, masculine conformity also did not account for a significant proportion of the variance in self-efficacy for symptom control.
Negative mood
Masculine conformity accounted for 18% of the variance in POMS depression scores R2 change = .18, F(3, 48) = 5.1, p < .01, controlling for age, income, and medical comorbidities. Self-reliance and dominance were significant positive predictors of depressed mood, indicating that men who more strongly endorsed traditional masculinity beliefs related to self-reliance and dominance also reported more depressed mood. In contrast, emotional control was a significant negative predictor of depressed mood, indicating that men who more strongly endorsed traditional masculinity beliefs related to emotional control also reported less depressed mood.
Masculine conformity also accounted for 17% of the variance in POMS tension scores R2 change = .17, F(3, 54) = 3.70, p < .05, after controlling for age. Of the masculine conformity indices, self-reliance was a significant positive predictor of tension, such that men reporting a greater need for self-reliance also reported higher levels of tension.
Functional well-being
Masculine conformity accounted for 16% of the variance in functional well-being after controlling for age, income, and medical comorbidities, R2 change = .16, F(3, 48) = 4.43, p < .01. In this model, self-reliance and dominance were significant negative predictors of functional well-being, indicating that men who more strongly endorsed traditional masculinity beliefs related to self-reliance and dominance also reported lower functional well-being. In contrast, emotional control was a significant positive predictor of functional well-being, indicating that men who more strongly endorsed traditional masculinity beliefs related to emotional control also reported better functional well-being.
Social well-being
Masculinity beliefs also accounted for 27% of the variance in social functioning, R2 change = .27, F(3, 53) = 5.25, p < .01, after controlling for age. Of the masculine conformity indices, dominance was a statistically significant negative predictor of social well-being, indicating that men endorsing more traditional views of dominance also reported lower quality of life related to social relationships.
Discussion
This study is among the first to examine masculine conformity variables as predictors of psychosocial functioning in a sample of African American prostate cancer survivors. When findings of the current study are compared with the previous examination of masculine conformity in a predominantly Caucasian sample of prostate cancer survivors (Burns & Mahalik, 2006), both similarities and differences are observed. Like the previous study, the current study found that men who believed more strongly in traditional masculine views about self-reliance reported less favorable mental health (i.e., depressed mood and tension). However, unlike the previous study, stronger traditional views about emotional control were associated with less depressed mood and better functional well-being. One explanation for these seemingly different findings could be related to cultural and generational differences in how emotional control is expressed. For example, in middle-aged and older African American men, desire for emotional control could lead to denial of sad feelings when asked about such feelings on a self-report measure. Another explanation might be that desire for emotional control stimulates active coping in African American men, leading them to “do” more to distract or distance themselves from the emotional impact of their disease. Staying active may ultimately convey benefits in the form of maintaining functional well-being. However, the extent to which the current study findings reflect cultural differences in enactment of traditional masculinity remains to be examined in future research. Both qualitative and quantitative research with sufficient representation of both African American and Caucasian men are needed to increase our understanding of how socialization and culture influence emotional adjustment and other aspects of quality of life in prostate cancer survivors.
There are study limitations that should be noted. Although the sample size of 59 African American prostate cancer survivors outnumbers African American representation in most prostate cancer research, the sample is still relatively small. Although care was taken to maximize the diversity of the sample with regard to demographic characteristics, a sample of this size may not be representative of the larger population of African American men. Indeed, it should be noted that the educational attainment of the sample (43% college graduates) is greater than the 2010 estimates of educational attainment among African American men aged 25 or older (17.9% college graduates; Current Population Survey; U.S. Census Bureau, 2010). Also, the sample size may not have been sufficient to achieve sufficient power for all analyses. Another limitation was the low internal reliability of the dominance subscale. Although this variable was found to predict psychosocial functioning and three of four items in the subscale were correlated with psychosocial variables in exploratory analyses, the relatively weaker internal reliability of the dominance subscale suggests the need to interpret findings related to this predictor variable with caution.
Despite the limitations noted above, the findings reported here could have important implications for development of effective supportive care interventions for African American prostate cancer survivors. Importantly, only a subset of interventions to improve quality of life in prostate cancer survivors has demonstrated substantial benefit (Chambers, Pinnock, Lepore, Hughes, & O’Connell, 2011). Furthermore, intervention studies have not included significant numbers of African American men or focused on masculinity issues beyond sexual functioning (Chambers et al., 2011; Molton et al., 2008; Penedo et al., 2007). Therefore, there is little in the psychosocial intervention literature that addresses cultural factors that may shape how masculinity beliefs are enacted by African American prostate cancer survivors and what therapeutic strategies could be effective for promoting adjustment.
The findings reported here, although preliminary, suggest that masculinity beliefs related to self-reliance could be an important therapeutic target for cognitive-behavioral interventions. To the extent that perceived dependence on others is interpreted as diminished masculinity, survivors may avoid asking for needed help and be left alone to deal with the gap between life demands and current capacity to meet those demands. Such men could be at increased risk for anxiety as our findings linking self-reliance and tension/anxiety suggest. Similarly, when dominance or power figure heavily into one’s concept of masculinity, the prostate cancer experience can present challenges (e.g., cutting back or early retirement from a job that allows demonstration of mastery). Perceived loss of power in public arenas could lead to efforts to preserve ones sense of masculinity by exerting more control within the private arena of the home or within close social networks (Charmaz, 1995). Based on clinical observations, the result of such efforts at exerting control is often diminished social relationships and greater psychological distress, which is also consistent with our study findings linking dominance beliefs to social functioning and depressed mood.
Masculinity theorists are calling increasingly for psychosocial interventions that address masculinity issues (Good et al., 2005; Mahalik, Talmadge, Locke, & Scott, 2005) not with the goal of pathologizing manhood but to help men improve their lives in those areas that they value most (Fischer & Good, 1997). In future studies, cognitive-behavioral techniques may be useful for helping African American prostate cancer survivors and men from other cultural groups to identify important masculinity beliefs and enact these beliefs in ways that are culturally congruent and promote psychosocial adjustment to cancer survivorship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research and manuscript preparation supported by DOD Grant W81XWH-07-1-0991 (Campbell/Keefe) and NCI Grant CA122704 (Campbell).