
Abstract
Few researchers have examined where African American men obtain, process, and use health information. A thematic analysis of data from eighteen exploratory focus groups conducted with 154 urban African American men aged 32 years and older revealed that men received health information from a variety of sources, including health professionals, media, and members of their social networks. At times, information raised their awareness of health issues, but trust in the source of the information influenced how this information was perceived. Medical professionals were the most common source of health information, but family members were the most trusted source of health information. Health problems and social support increased men’s motivation to use health information in order to improve their health and healthy behaviors. These findings illustrate that it is critical to identify factors that influence what information men choose to believe and follow or decide to ignore.
Keywords
Health knowledge is a critical aspect of health education and health promotion theories and a fundamental, necessary, and modifiable aspect of initiating and sustaining healthy behavior (Glanz, Rimer, & Viswanath, 2008). According to a recent Institute of Medicine report, almost 90% of U.S. adults have difficulty using everyday health information that is available in health care facilities, retail outlets, communities, and the media (Institute of Medicine, 2011; Office of Disease Prevention and Health Promotion [ODPHP], 2010). Obtaining, processing, and understanding basic health information are critical aspects of health literacy, or one’s capacity to make appropriate decisions about health (Institute of Medicine, 2011; ODPHP, 2010). Medical professionals have been some of the common sources of health information, but a number of studies have investigated how trust in formal health care settings affects utilization of health information and health behavior (Boulware, Cooper, Ratner, LaVeist, & Powe, 2003; Gamble, 1997). Although it is important to examine factors associated with information acquired through health care facilities, individuals are likely to encounter health knowledge much more frequently from sources outside of the health care setting (Cotten & Gupta, 2004). According to the Centers for Disease Control and Prevention (2009), over the course of 1 year, the average American spends only 1 hour in a health care setting and makes many health decisions based on health information received in other contexts such as at home or in their communities.
Increased health literacy has been associated with greater health knowledge, more health behavior changes, better disease management skills, and improved overall health outcomes (Volandes et al., 2008; Williams, Baker, Parker, & Nurss, 1998). One of the critical aspects of health literacy and being an effective consumer of health information is recognizing what sources of health information are trustworthy and which are not (ODPHP, 2010). Health literacy and health knowledge are dependent on a combination of formal education, access to and quality of health services, and social and cultural factors (Nielsen-Bohlman, Panzer, & Kindig, 2004). Differences in health literacy, health knowledge, and motivation to adopt and maintain health-promoting behaviors may contribute to racial (Bennett et al., 1998; Paasche-Orlow, Parker, Gazmararian, Nielsen-Bohlman, & Rudd, 2005) and gender–health disparities (Payne, 2006).
African American men are disproportionately affected by numerous chronic diseases that can be prevented or ameliorated by behavioral and lifestyle changes such as increasing and maintaining healthy eating and physical activity (Warner & Hayward, 2006). Having information on changes that could benefit their health and how to incorporate these changes into their daily lives, and receiving that information in a way as to motivate change, could play a critical role in reducing many of the leading causes of morbidity and mortality for African American men (ODPHP, 2010). While some African American men have considerable knowledge about nutrition (Ravenell, Johnson, & Whitaker, 2006; Watters, Satia, & Galanko, 2007), others may benefit from information on basic nutrition, serving sizes, or understanding food labels (James, 2004). Increased knowledge of nutrition guidelines (Wolf et al., 2008) and belief in the importance of a diet high in fruits and vegetables (Watters et al., 2007) have been positively associated with fruit and vegetable consumption. In addition, some African American men may be aware that they need to improve their diet in certain areas (i.e., more fruits and fiber), but may not understand the quality of their current diet in relation to federal recommendations (James, 2009; Watters et al., 2007; Wolf et al., 2008). Approximately half of African American men report no leisure time physical activity (Ward et al., 2004). African American men may be more likely, however, to engage in physical activity if they receive positive messages about doing so from a trusted and reliable source (Friedman, Hooker, Wilcox, Burroughs, & Rheaume, in press; Hooker, Wilcox, Rheaume, Burroughs, & Friedman, 2011). Thus, African American men’s responses to health information and their motivation and ability to act on it may be influenced by numerous factors interacting at different levels that warrant further examination. The purpose of this article is to explore how middle aged and older African American men felt about different sources of health information and how they made use of the health information they received.
Method
Study Design
The data analyzed were collected as part of the Men 4 Health (M4H) study (Griffith, Gunter, & Allen, in press). The goal of M4H is to systematically develop a culturally, contextually, and gender-sensitive intervention that addresses the individual and social barriers to healthy eating and physical activity among middle aged and older, urban African American men. Exploratory focus groups were conducted in southeast Michigan with African American men in this population of interest to inform the development of the M4H intervention.
The focus groups lasted approximately 2 hours and included a meal, the completion of consent and demographic forms, and a guided, semistructured discussion. Half the focus groups primarily focused on determinants of healthy eating, whereas the other half focused on determinants of physical activity. Two interview guides were used, one for each behavior, composed of four broad questions: Why do you think African American men do not eat more fresh fruits and vegetables/aren’t more physically active? What influences what you and other African American men aged 35 years and older eat/how much physical activity you get? For you or other African American men aged 35 years and older, what makes it easier or harder to eat healthy/be physically active? How does stress affect eating/physical activity for African American men in your age group? The facilitators, also African American men from the geographic areas of interest, engaged in extensive probing to elicit detailed discussion. The facilitators also documented group dynamics and tracked comments of individual speakers. Unique identifiers were assigned to each participant to ensure anonymity. The University of Michigan Institutional Review Board reviewed and authorized the overall study and materials.
Recruitment and Study Participants
The African American male focus group facilitators recruited study participants through snowball sampling via word-of-mouth, flyers, presentations at appropriate venues, and social network connections of the facilitators and partner organizations. Each participant received an incentive worth $20, with a choice of receiving either a gift card to local business or a countertop electric grill. In all, 154 African American men participated in 18 exploratory focus groups held in southeastern Michigan between July 2008 and March 2010 (see Table 1 for selected participant characteristics).
Selected Demographic and Health Characteristics of Study Participants

Data Analysis
Each focus group was audio-taped, transcribed verbatim, and entered into the qualitative data software package, ATLAS.ti.5.2 (Scientific Software Development, Berlin, Germany, 1998). The unique identifiers and observers’ notes were used to link a participant’s demographic data to his discussion comments. The data organization process was similar to the methods used by Allen, Griffith, and Gaines (2011) and Griffith and colleagues (Griffith et al., 2007, Griffith et al., 2008; Griffith, Allen, & Gunter, 2011; Griffith, Gunter, & Allen, 2011). Each transcript was “chunked” into segments of text that represented distinct “meaning units” that conveyed their original meaning apart from the complete transcripts. Each unit was linked to the unique identifier of the speaker, the date of the focus group, the overall question, and any other stimuli that appeared to influence the individual’s statement. Selected transcripts were reviewed in order to identify recurring patterns and topics that emerged from the transcripts. This yielded a codebook of phenomenological concepts, or “codes,” that were chosen to enhance the ease and reliability of the assignment of codes to the text segments. A team of university-based researchers trained to employ the codes in a consistent manner then assigned codes to the meaning units within each focus group transcript.
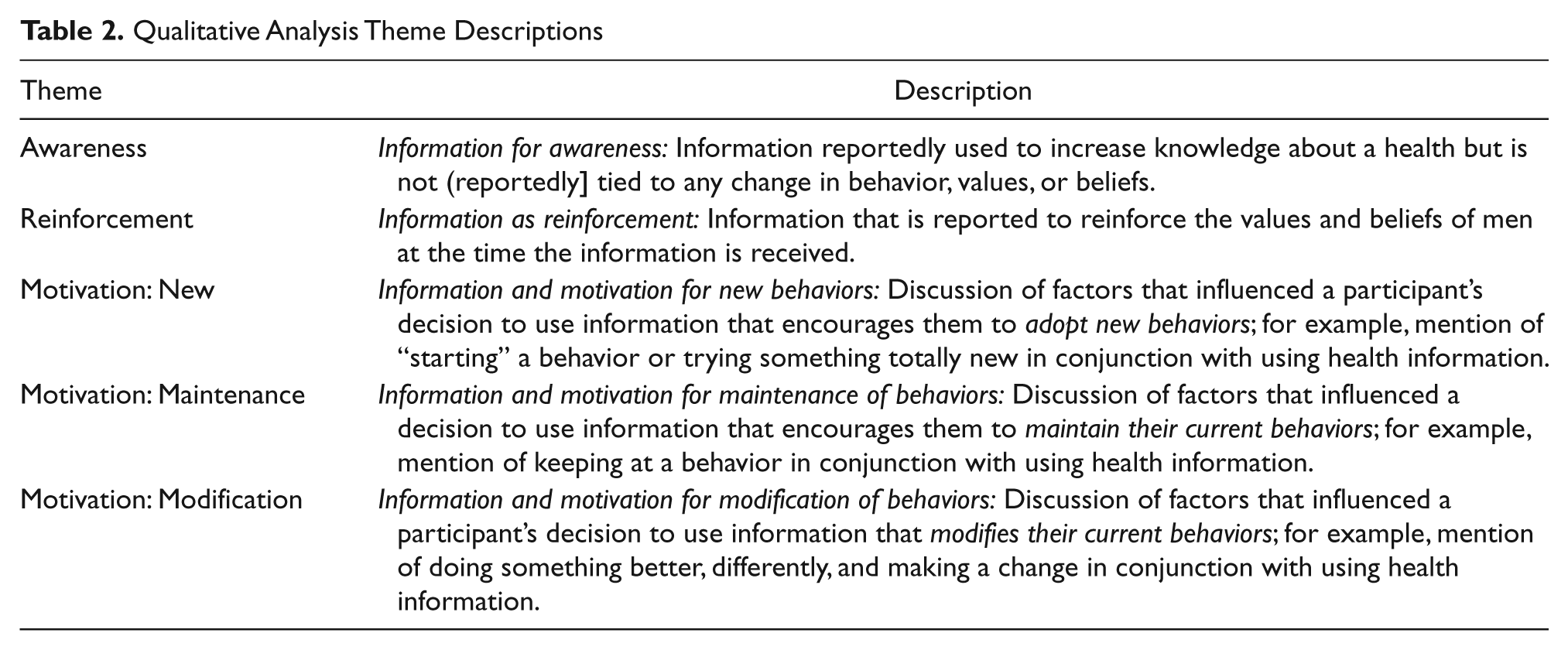
The data for this article are derived from the Sources of Health Information (SoHI) code. The meaning units summarized under this code includes text in which individual African American men report seeking or having found health information, strategies men use to find health information, where participants expected to find and yet are not getting health information, and where participants think they should be able to get health information. The Data captured with this code was comprehensive; thus examining the meaning units assigned to this code was appropriate and adequate for a thorough analysis of how men discussed issues associated with health information sources. An analysis of the number of focus groups and individual men who discussed the topic demonstrated broad representation. Examination of the SoHI text segments using a combination of short restatements of the data and direct quotes in the margins led to the identification of themes. Next, documentation of underlying themes, potential questions, and suggestions for further analysis occurred. Comparison margin analysis was used to ensure consistent interpretation of the statements. These notes and the corresponding quotes were summarized into a larger document organized according to five distinct themes that emerged during this analytic process. The small number of quotes that discussed men’s provision of health information to others but did not directly address how men obtained and used information were excluded from this analysis. Review and revision of this document occurred until consensus was reached on the detailed descriptions of the themes (Table 2) and the quotes attributed to each theme. Representative quotes were selected to reflect common themes and convey the voices of the men sharing their experiences and perceptions.
Qualitative Analysis Theme Descriptions
Results
The first section of the results briefly summarizes key sources of health information that the focus group participants discussed. The second section explores in detail how information the men received influenced them and their health behavior.
Sources of Health Information
Men discussed sources of information from four main categories: media, medical professionals, social network, and community resources. Medical professionals were the most common source of health information. Television was the most frequently mentioned form of media, followed by videos, radio, books, newspapers, magazines, and the Internet. Friends, family, peers, and people at church were people in men’s social network who were described as sources of information. Community resources, which were discussed least often, included food labels and the workplace.
Purpose of Health Information: Raising Awareness
Many men reported that information increased their awareness of health-related issues. Several of the men described gaining increased awareness of health issues from the media. Television helped some men learn more about diabetes prevention and the health of African American men in general. One man explained that television challenged his perception of cultural norms about older men’s engagement in physical activity. He stated,
. . . I’ve seen guys—especially on TV—[in their] 80s and 90s . . . exercising . . . I think it’s been . . . a cultural thing that as men we think as we get older that we’re supposed to slow down . . .
Several of the men also reported receiving information from their doctors that increased their awareness. A few men discussed an expectation that their doctor would provide health information, and a couple of men discussed visiting their doctor in order to receive health information.
The theme of trust emerged in discussions of receiving health information for awareness. Though media was the most frequently reported source of health information for awareness, it was not always trusted. For example, one man reported that newspaper statistics about the health of African American men compared with White American men were misleading. Family members were most often cited as trusted sources of information. Some men, but not all, found doctors to be trustworthy.
Purpose of Health Information: Reinforcing Knowledge
Some of the men received information from a doctor which reaffirmed knowledge that men already possessed. For example, a participant stated,
. . . It’s beneficial and rewarding, but . . . a lot of times, I dread [exercising]. But I still do it anyway because of the benefits. My doctor told me once that when you get on the treadmill or move for a while, it releases a natural euphoria. And a lot of times [after I finish exercising] I feel so good . . .
Another participant noted,
. . . Stress will make you or cause you to . . . react in a variety of ways . . . [my doctor said] stress will take you out if you don’t address it . . .
This information strengthened some of the men’s commitment to physical activity as part of their overall lifestyles and as a way to cope with stress.
Purpose of Health Information: Increasing Motivation
Men discussed examples in which health information increased their motivation to improve their health according to three subthemes. For men who adopted new behaviors, a number of factors contributed to their decision to use health information they received about the behaviors. Second, men described factors that motivated them to use information that supported behavior maintenance. Finally, other men mentioned factors that motivated them to use information that would require modification of certain behaviors.
New behaviors
A couple of men reported that they were motivated to engage in new behaviors after receiving information that doing so could prevent health problems. The majority of the men who discussed engaging in new behaviors, however, did so in response to an existing health problem. More specifically, several men reported that after being diagnosed with a health problem, they were more likely to adopt a new behavior when their doctor informed them that doing so would be beneficial to their health. Thus, their motivation—to alleviate a health problem—was directly tied to information provided by a medical professional about engagement in a health behavior. For example, one focus group participant stated,
I recently went to the doctor because I’ve been experiencing stomach issues and my doctor told me, I need you to eat no meat for two weeks. Fruits and vegetables all you want, but no meat . . . I didn’t think I could do it, but, when it came down to my health, I said—I better do this, at least try. So I ended up losing 13 pounds in 10 days—I know in my mind it’s possible, and healthy, to consider what I eat . . .
Another man reported that if a doctor “mandates” following information about exercise engagement to treat a health problem, men have an easier time following the mandate. Although most of the examples provided in which men changed their behaviors in response to health information were about adopting positive behaviors, this was not always the case. As one participant explained,
It’s hard to get up early and go work out. I did it when I had a scare. When the doctor scared me, I did it. But as soon as that scare’s over, I stayed in the bed . . .
Maintenance of behaviors
A few men continued their engagement in certain behaviors because they wanted to avoid health problems, complications from current conditions, or remain healthy for their families. These men reported seeking out and receiving health information that encouraged and enabled them to maintain certain healthy behaviors such as exercise and dietary quality. For example, one participant described,
. . . I have diabetes . . . And when you go in for testing, they always tell you that you need to work out . . . if I don’t take care of myself, I can have an amputation, kidney failure . . . So, that alone pushed me into exercising and making that a part of my life . . .
Nutrition labels also were reported to be sources of information that supported the maintenance of healthy behaviors. One man reported that his practice of reading nutritional information from food labels helps him to maintain a healthy diet.
Modification of behaviors
Several of the men reported modifying certain behaviors after receiving health information. In these instances, the motivation for using the health information was not as explicit, though there was a general theme of becoming healthier. What was clearer was the role that social support played in helping men modify their behavior. Sources of information that provided support for modification of existing behaviors included family, people in the church, and fruit and vegetable vendors.
For several men, wives provided the support they needed to modify behavior after receiving information about healthy eating. For one of these men, it was his wife’s detailed discussion of healthy eating and the specific health benefits of certain foods that led him to modify his behavior. For another man, information from a doctor helped him to be more cooperative with actions his wife had been taking to improve the quality of their diets. Less frequently, men discussed modifying their eating habits after reading about healthy eating.
Discussion
This study shares the perspectives of African American men on key sources of health information and factors that influenced how they incorporated health information into their lives. Doctors and medical professionals were the most common source of health information, and television was the most frequently mentioned media source. Members of men’s social networks, such as friends, family, peers, and church, also were key sources of health information. Family members seemed to be the most trusted information source, while trust levels with physicians and media sources varied. Many men reported accessing and obtaining health information, but factors such as trust shaped how much that information influenced them or their behavior. These data are inconsistent with previous research that suggests that overcoming concerns about trust is an important factor in African Americans’ interactions with medical professionals and health resources and facilities (Boulware et al., 2003).
Some of the information men received, such as the benefits of exercise and the consequences of stress, affirmed their current beliefs and values. Thus, information that supported men’s healthy beliefs and values helped to increase their motivation to adopt, modify, or maintain healthy behavior (Bandura, 2004; Rubak, 2005). Men often, however, receive information from a variety of sources, and these sources may include dissonant information or recommendations. It is important, therefore to ask explicitly if men have received discrepant information from trusted sources.
Health information that is from a trusted, accessible, and useful source is an essential component of motivation to engage in healthy behavior (Fisher & Fisher, 2002; Ryan & Deci, 2000). Consistent with previous research about African American men (Allen et al., 2011; Griffith, Allen, et al., 2011; Griffith et al., 2007), men in the current study reported that receiving social support from spouses and faith community members helped them to use health information and increased their willingness to follow recommendations from medical professionals to improve healthy behaviors. For people who are managing a disease, Paasche-Orlow and Wolf (2007) note that self-management requires knowledge, capacity, and the will to engage in recommended health behaviors. Existing health problems were a common motivating factor for men who adopted new behaviors. Most often, their doctor provided them with information about the behaviors they needed to engage in to manage or alleviate the health problem (Griffith, Allen, et al., 2011). Men also reported being motivated to adopt new behaviors after learning that the behaviors could prevent health problems.
Social support is a critical aspect of helping African American men maintain their overall health (Ravenell et al., 2006) and healthy behaviors (Griffin, Wilson, Wilcox, Buck, & Ainsworth, 2008), such as physical activity (Hooker et al., 2011). These findings reinforce the notion that it is critical to help men secure resources and skills that will help men both initiate behavior change and create lifestyle change. Kumanyika et al. (2000) argue that it is useful to obtain very specific information from men about the behavior change that occurs so that important issues related to the long-term adoption of behaviors can be highlighted and addressed. Information that supported behavior maintenance was helpful for men who were already engaging in healthy behaviors. It is critical to help men to access and maintain social relationships that support their use of health information to engage in healthy behaviors.
While it is important to help individuals access and comprehend information about healthy behaviors, emerging research on African American men and health behavior highlights the need to help men more effectively negotiate the social and environmental context of the behaviors. For example, research by Griffith and colleagues (Griffith et al., in press; Griffith, Gunter, et al., 2011; Griffith, Wooley, & Allen, 2011) and Hooker and colleagues (Friedman et al., in press; Hooker et al., 2011) found that many of the barriers African American men faced in trying to increase and sustain regular physical activity and healthy eating, for example, were related to their ability to negotiate job and family priorities that competed for their time and energy and decreased their motivation to prioritize health and engage in physical activity and healthy eating.
Limitations
There was not a specific question in the interview protocol in which men were asked about health information; these data were derived from systematically probing the focus group data on physical activity and healthy eating. Had the focus been more specifically on health information, men’s responses may have been different. Given the frequency and the consistency of responses across the 18 focus groups and the fact that the men offered opinions and examples of the role of health information in their lives with minimal prompting on the topic, the findings in this article offer useful insight on where African American men access health information and how they use it in support of healthy behavior.
Implications for Practice
Health researchers and professionals who work with African American men should consider the factors that influence not only their access to health information but also their utilization of health knowledge. While barriers to utilization of health knowledge—both individual and contextual—are likely to persist, there also are many available opportunities to support men’s health behaviors. Overall, these data provide evidence that men may have different information needs if they are adopting, maintaining, or modifying behavior. African American men have been skeptical of health promotion materials and messages that are perceived to be too general and lacking cultural relevance for African Americans generally and African American men specifically (James, 2004, 2009). Tailoring information to their specific health and information needs may increase their adoption and maintenance of healthy behaviors. As demonstrated in these focus groups, many men possess health information that can be used to improve their health. Thus, it is important to focus not only on providing men with health information but also on helping them acquire the skills and resources needed to use health information.
Footnotes
The contents of this article are solely the responsibility of the authors and do not necessarily represent the views of the funders or the University of Michigan.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported in part by grants from the American Cancer Society (MRSGT-07-167-01-CPPB), the Michigan Center for Urban African American Aging Research, and the Cancer Research Fund of the University of Michigan Comprehensive Cancer Center, and by the University of Michigan Center on Men’s Health Disparities.