
Abstract
Men have higher cancer mortality rates for all sites combined compared with women. Cancer screening (CS) participation is important for the early detection of cancer. This study explores gender differences in CS beliefs, behaviors, and willingness to participate. The data were collected from a stratified, random-digit dial survey of adults living in New York, Maryland, and Puerto Rico. Chi-square tests and logistic regressions were computed to analyze gender associations among CS beliefs, behaviors, and willingness variables. Men and women believed that CSs were effective, though a higher percentage of men had never had a past CS. Men were less willing to participate in a CS at the present time and in a skin cancer exam; however, when given descriptions of screening conditions, men indicated more willingness to participate. These gender differences highlight the need for health professionals to examine their efforts in providing enhanced CS promotion and education among men.
Introduction
Men have consistently underutilized preventive health care services compared with women (Bertakis, Azari, Helms, Callahan, & Robbins, 2000; Green & Pope, 1999). In 2007, about 21% of adult men did not make health care visits to a doctor’s office, emergency department, or use home visits compared with only 12% of women (National Center for Health Statistics, 2010). In addition, about 24% of males reported having no usual source of care between the years 2006 and 2007 compared with 13% of females (National Center for Health Statistics, 2010).
Men’s underutilization of health services places them at a disadvantage and may be partially caused by the role of masculinity and social norms, which has frequently been documented as contributing to men not using services (Addis & Mahalik, 2003; Courtenay, 2000). On the other hand, women have more frequent contact with health care professionals in relation to pregnancy, childcare, and hormone replacement therapy (Evans, Brotherstone, Miles, & Wardle, 2005). Also, women report more interest in health (Green & Pope, 1999).
Cancer screening (CS) is one way of using preventive health services, and it is important for the early detection of cancer. When cancer is detected in later stages and/or has spread into other areas of the body, it causes treatment to be difficult (National Cancer Institute, 2010b). Cancer mortality rates for all cancer sites combined are currently higher among men than among women (Jemal, Siegel, Xu, & Ward, 2010; Pinkhasov et al., 2010). It is estimated that between 3% and 35% of cancer deaths could have been prevented by early CSs (National Cancer Institute, 2010b). Fortunately, CS rates improved slightly from the years 2005 to 2008 regarding breast cancer (mammography), colorectal cancer, and prostate cancer, but rates are still lower than optimal (Smith et al., 2011). Current studies examining gender differences in CS mainly analyze colorectal CS participation, given that it is the only comparable CS between men and women. Results from studies using national datasets indicate that higher prevalence of colorectal CS participation was reported among men compared with women (Meissner, Breen, Klabunde, & Vernon, 2006; Stock, Haug, & Brenner, 2010).
Rather than only analyzing a specific cancer, this study explores gender differences in CS beliefs, behaviors, and willingness to participate in a general sense. Thorough knowledge about gender differences as it relates to these CS variables is lacking in the literature, and it is critical to understand how men and women differ regarding several aspects of CSs in order to improve health promotion strategies. Discovering effective strategies to get more men involved in preventive health services may potentially reduce cancer mortality rates. This knowledge has implications for health promotion practices for health professionals, physicians, and community-based organizations.
Method
The data were collected from a disproportionally allocated, stratified, random-digit dial telephone survey of noninstitutionalized adults (≥18 years old) living in New York City, New York; Baltimore, Maryland; and San Juan, Puerto Rico. The survey, the Cancer Screening Questionnaire (CSQ), was developed by a multidisciplinary, multiuniversity research team within the New York University Oral Cancer RAAHP (Research on Adolescent and Adult Health Promotion) Center, an NIDCR/NIH (National Institute of Dental and Craniofacial Research/ National Institutes of Health) Oral Health Disparities Center and was conducted in 2003. The CSQ was adapted from a previously validated questionnaire, the Tuskegee Legacy Project Questionnaire, which was designed to assess willingness to participate in biomedical research (R. V. Katz et al., 2006). English and Spanish versions of the questionnaire were administered per participant preference. The English version of the questionnaire was pilot-tested among persons residing in the U.S. recruitment cites (Baltimore and New York). The Spanish version of the questionnaire was validated through pilot tests in San Juan, Puerto Rico. The CSQ addresses a range of issues related to the beliefs and willingness to participate in CS examinations in an ethnically diverse sample.
Each of the three cities was sampled independently and with specific race/ethnic group targets within each city: 300 African Americans (150 in New York City, 150 in Baltimore); 300 Puerto Rican Hispanics (150 in San Juan, 150 in New York City); and 300 Whites (150 in New York City, 150 in Baltimore). Baltimore, New York, and San Juan were selected as recruitment cities to ensure a wide geographic and racial/ethnic representation. The initial sample allocation across strata (within city) was based on expected yields computed using exchange incidence data. Sampling weights were produced because of the complex design of the CSQ Study. A more detailed explanation of the study design, and justifications of methodological decisions, is described elsewhere (R. V. Katz et al., 2008; Kressin et al., 2010). A total of 1,148 participants completed the telephone survey. The original targeted enrollment goal of 300 for each racial/ethnic group was met or exceeded within each city: 355 African Americans, 311 Puerto Rican Hispanics, and 482 non-Hispanic Whites. Response rates (the percentage of completions of residential households dialed) for San Juan, Baltimore, and New York were 58%, 51%, and 45%, respectively with an overall completion rate (percentage of completed interviews once contact was made with the targeted household subject) of 82.6%, which is based on the Council of American Survey Research Organizations rates (CASRO, 1982). The study was approved by the University of Puerto Rico and New York University Institutional Review Boards.
Measures
The variables examined in this study are listed in Table 1. Participants’ CS belief was assessed using the variable of how effective CSs are in detecting cancer (all/most of the time detect cancer, some of the time detect cancer, occasionally/rarely detect cancer). Participants’ CS behavior was assessed using the variable of whether they ever had a CS in the past. If they answered “No,” a follow-up question was asked at the end of the survey that specifically asked females if they ever had a mammogram or Pap smear, asked males if they ever had a prostate exam, and asked everyone if they ever had a cancer exam of the mouth. Those who answered “No” to the first question and then answered “Yes” to a specific screening were classified as having had a CS in the past. Willingness to participate in a CS was assessed through several questions asking willingness to participate in a regular CS at the present time, willingness to participate in a screening depending on who conducts the screening, willingness to participate in a screening depending on what one is asked to do during the screening, and willingness to participate if the CS was for a particular type of cancer. The willingness to participate variables were dichotomized into “Likely” (very likely and somewhat likely) and “Unlikely” (not quite sure, somewhat unlikely, and very unlikely). Not quite sure was categorized under “Unlikely” based on previous research, which is described elsewhere (R. V. Katz et al., 2006).
Variables Used to Assess Cancer Screening Beliefs, Behaviors, and Intentions

Statistical Analysis
Weighted frequency distributions of sociodemographic variables (race/ethnicity, age, education, income, and city) were computed to show the characteristic distribution of the sample by gender. The Rao–Scott chi-square test, a design-adjusted version of the Pearson chi-square, was employed to calculate bivariate differences between gender and CS beliefs and behavior. Since CS participation is highly based on age, gender differences within each age group were also assessed for past CS behaviors using the Rao–Scott chi-square tests. Separate logistic regression models were computed to predict the relationship between gender and willingness to participate in CSs. Each willingness variable was the dependent variable and gender was the independent variable, adjusting for race/ethnicity, age, education, income, and city. Response choices of Don’t Know or Refused for all variables were classified as missing. Statistical significance was determined at a p value of <.05. SAS version 9.2 (SAS Institute, Inc., Cary, NC) was used for all data analyses.
Results
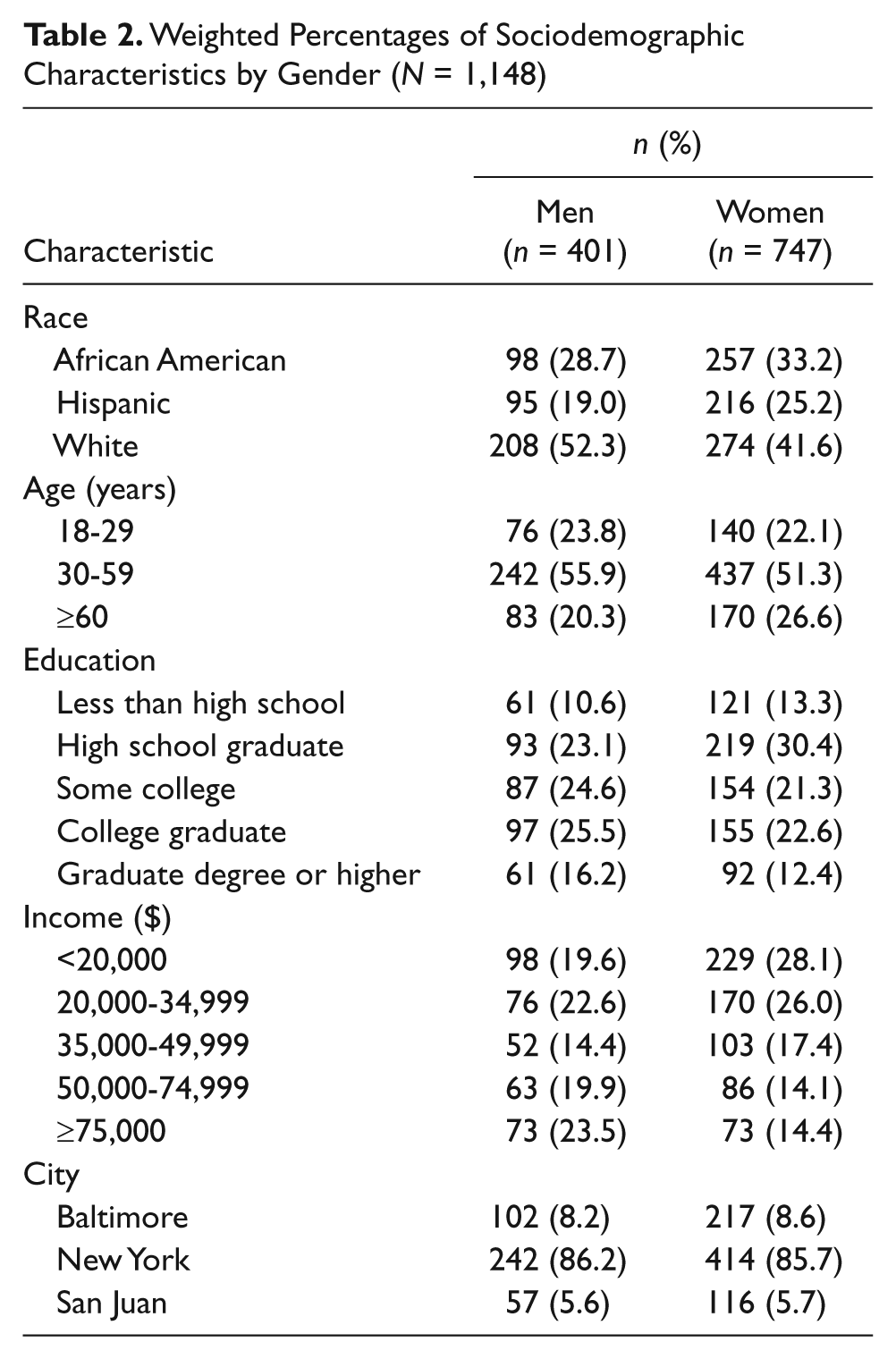
The sociodemographic characteristics by gender are reported in Table 2. Men constituted about 35% of the sample and about half of them were White. There were slightly more White women, closely followed by African American women, then Hispanic women. A majority of both men and women were 30 to 59 years old. Men had higher levels of education and income than women.
Weighted Percentages of Sociodemographic Characteristics by Gender (N = 1,148)
Gender associations with CS beliefs and past CS participation are presented in Table 3. Participants’ beliefs about CS effectiveness was not statistically significant (χ2 = 4.90; p = .09). Approximately the same percentage of men and women believed CSs detected cancer all/most of the time (67% vs. 66%, respectively). Rao–Scott chi-square tests resulted in significant associations (χ2 = 118.3; p < .0001) between gender and past CS participation. Overall, about 41% of men had never had a CS in the past compared with only 5% of women who had never had a screening. Within the age groups of 18- to 29-year olds and 30- to 59-year olds, statistically significant results included a higher percentage of men who had never had a CS compared with women (shown in Table 3). However, there were no statistically significant differences among men and women 60 years and older for ever having had a CS.
Weighted Rao–Scott Chi-Square Results by Gender

The odds ratios (ORs) and 95% confidence intervals (CIs) of the statistically significant gender associations among the variables measuring CS willingness are reported in Table 4. Men were less willing to participate (OR = 0.50; 95% CI = 0.32-0.77) when asked a general question about participating in a CS at the present time compared with women. The statistically significant variables assessing willingness to participate in a CS when given specific details (i.e., when told what one has to do during a screening and when told who conducts the screening), all showed men being slightly more willing to participate than women. For example, as shown in Table 4, men were 1.51 (95% CI = 1.02-2.23) times more willing to participate in a CS when told the exam would be given by the government compared with women. The variables assessing specific details about what one has to do during the screening revealed being interviewed about smoking habits as the only statistically significant variable (OR = 1.56; 95% CI = 1.00-2.43). Being screened for skin cancer was the only specific type of cancer that was found to be significant between genders, with men being less willing to participate in a screening for skin cancer (OR = 0.59; 95% CI = 0.39-0.90).
Logistic Regression Results a for Statistically Significant Willingness to Participate in Cancer Screening Variables

Results are modeled for men, with women being the reference category and adjusting for race, age, income, education, and city.
Discussion
This study examined gender associations in beliefs, behaviors, and willingness to participate in CSs to gain insight for improving existing cancer health promotion practices. The findings particularly emphasize the need for better health and CS promotion among men. Despite a majority of men and women believing that CSs are effective in detecting cancer, a significant proportion of men had never had a CS. This finding may be explained by the fact that women have more “ongoing, routine” opportunities to be screened when visiting their primary care doctor (e.g., menstrual problems, pregnancies), whereas men lack these kinds of health events. In addition, men have to deal with the uncertainties of CS benefits and making an informed decision to participate in their most common CS, screening for prostate cancer (Centers for Disease Control and Prevention, 2010). It has been found that men who have already undergone a screening for prostate cancer are more likely to participate in a screening for colorectal cancer (Carlos, Underwood, Fendrick, & Bernstein, 2005; Wong & Coups, 2011). So, the frustration, fears, and feeling overwhelmed with making a decision about being screened for prostate cancer may hinder participation in other screenings.
However, the media may be another contributor to the finding that women participate more in CSs. There is a great deal of cancer awareness for women’s cancers and far less coverage on men’s cancers in the media (George & Fleming, 2004; M. L. Katz et al., 2004). In a study exploring newspaper cancer stories, it was found that mammography was mentioned significantly higher than prostate-specific antigen or colorectal screenings in mainstream and in ethnic newspapers (Stryker, Emmons, & Viswanath, 2007). Many fundraisers, commercials, and community awareness events about women’s cancer issues already exist (i.e., the National Football League routinely shows players wearing pink gear to support breast cancer screening during October for National Breast Cancer Awareness Month), but men’s health promotion lacks parallel events of this magnitude and visibility. The Prostate Cancer Foundation is only now petitioning the National Football League to allow their players to wear blue during September, the National Prostate Cancer Awareness Month (Prostate Cancer Foundation, n.d.).
Lack of men’s health promotion is evident even within national government agencies. The National Institutes for Health currently has the Office of Research on Women’s Health and the Department of Health and Human Services has the Office on Women’s Health (National Institute of Health, n.d.; U.S. Department of Health and Human Services, 2010). Unfortunately, neither agency has a counterpart men’s health office. Though, there is now a proposed legislative bill to finally create the Office of Men’s Health within the Department of Health and Human Services (Men’s Health Policy Center, 2010). This bill comes nearly 20 years after the Office of Women’s Health was first created. In addition, the National Cancer Institute estimated in 2009 that funding for breast cancer research was nearly twice as high as funding for prostate cancer research (National Cancer Institute, 2010a). These examples provide clear evidence, at the national agency level, of the degree to which men’s health promotion lags behind women’s health promotion.
Another main finding of our study was that men were less willing than women to participate when asked a general question about participating in a CS at the present time, but when given various descriptions of screening conditions (i.e., who conducts the screening and what one has to do during the screening), they were slightly more willing to participate than women. In other words, when told more specific details about the CS, men seemed to be more willing to participate compared with being asked about getting a CS at the present time with no specific details. Even though each of the screening-specific variables in and of themselves may not hold any implications, the very fact that men were slightly more willing to participate in these specific screening events strongly suggests that men are susceptible to participate in a variety of CS events when given more information about the screening. In light of this opportunity to promote CS in men, health educators, physicians, and community-based organizations should make a concerted effort to educate men on the exact screening procedures, how cancer is detected, and what to expect during the screening. Men seem to be eager for sufficient explanations about health exams in order to have a good experience during the exam and to learn more about making a decision for participating (Dubé, Fuller, Rosen, Fagan, & O’Donnell, 2005). This has the potential to result in increasing men’s self-efficacy in participating in CSs, partly because they will have increased knowledge due to these campaigns and partly because they have given evidence of their willingness to participate in CSs.
Men were identified as less likely to want to participate in a screening for skin cancer than women. This finding is consistent with previous findings (Janda et al., 2004; Weinstock et al., 1999). One way to detect skin cancer is self-examination; however, men are less likely to self-examine than women (Evans et al., 2005). Therefore, this provides another opportunity to educate men about the detection of skin cancer and what certain signs/symptoms they should be looking for on their skin. Some evidence shows that a screening service may be effective in conjunction with educational campaigns in facilitating early detection of skin cancers (Koh et al., 1996). This is very important because the patient has more intimate knowledge of his or her skin and has more frequent opportunities to inspect his or her skin. Also, it has been found that having the assistance of a partner or spouse is a predictor for skin self-examination (Weinstock et al., 2004). Increasing knowledge about skin self-examination could lead to men detecting signs of cancer earlier, and it could amplify the voice of the women in their lives as they will also get educated about the self-examination benefits for their men and will help to urge them to practice it.
Limitations of this study include some typical methodological limitations associated with the chosen study design. Individuals were excluded if they did not have a telephone land line and the data were self-reported, which may have introduced recall and reporting error. Other variables that could affect CS participation that were not collected are health insurance status and family history of cancer. Another limitation is that the data used are nearly 9 years old; however, these results can inform CS promotion, which is still a relevant issue today. Finally, no questions were asked about testicular cancer screening. Including testicular cancer exams as a follow-up question for past CS behaviors might have more accurately reflected young men’s CS past behaviors, especially since testicular cancer affects younger men more than older men (Altekruse et al., 2009).
Future efforts in CS promotion need to be redirected and specifically targeted toward the appropriate populations. In addition, future research should explore how health education on specific CS tests and procedures increases self-efficacy and control. This increase in self-efficacy may increase CS participation rates among men. Another recommendation for future research is to replicate this study with other large urban samples regarding willingness to participate in CSs. This study highlights the need to increase awareness and promotion of men’s health, especially with regards to CS and cancer prevention. More precisely, the results indicate that men appear to be both susceptible and ready to respond to CS promotional efforts, creating an opportunity for health professionals to have an impact on cancer survival in men if they proceed to provide men with more explanations and education about CSs.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grant U54 DE 14257 from the National Institute of Dental and Craniofacial Research/National Institutes of Health (NIDCR/NIH), the New York University Oral Cancer Research on Adolescent and Adult Health Promotion Center (an Oral Health Disparities Research Center).