
Abstract

Introduction
Optimal antiplatelet management in the perioperative and outpatient settings of coronary artery bypass grafting (CABG) remains a critical determinant of perioperative bleeding risk, graft patency, and long‑term cardiovascular outcomes. Although evidence‑based guidelines exist, clinical practice is often complicated by urgent surgical timelines, choice of conduit, operative strategy, and patient‑specific factors. Aspirin (ASA) has been well established as a safe antiplatelet agent in the preoperative and postoperative phases of CABG with low rates of complications or side effects; however, its use as part of a dual-antiplatelet therapy (DAPT) strategy is where recommendations differ. P2Y12 inhibitors (P2Y12i) are well established in cardiology for secondary prevention in acute coronary syndrome (ACS) and percutaneous coronary intervention (PCI) but continue to present a variable balance of risks and benefits when it comes to surgical revascularization. Furthermore, the choice of P2Y12i agent to use alongside ASA continues to be a topic of debate, with numerous clinical trials having compared short-term and long-term outcomes. DAPT recommendations continue to evolve as clinical trials explore their use in more specific surgical settings, such as off-pump CABG (OPCAB), total-arterial grafting, and minimally invasive cardiac surgery (MICS) CABG, especially as these surgical approaches grow in popularity.
The following 10 commandments synthesize current evidence and expert opinion to provide a practical framework for antiplatelet therapy decision‑making across a range of common clinical CABG scenarios.
1. Stop DAPT Prior to Semi-Urgent or Elective CABG
In the nonurgent setting, when surgical revascularization can be timed with flexibility, the evidence pertaining to antiplatelet therapy has been well described. Despite recommendations calling for the discontinuation of ASA as much as 10 days prior to noncardiac surgery, ASA has a protective effect in cardiac surgery patients by stabilizing plaque, reducing perioperative myocardial infarction (MI) and other thrombotic events, as well as improving graft patency. 1 For these reasons, the benefits of continuing ASA until surgery outweigh its relatively low risk of bleeding. Compared with ASA, P2Y12i are more potent antiplatelets and are associated with higher risks of bleeding, particularly in the cardiac surgery population. Although ASA causes irreversible, broad inhibition of thromboxane A2 production, P2Y12i (e.g., clopidogrel, ticagrelor) specifically target the adenosine diphosphate receptor on platelets to inhibit the final, critical step of aggregation. 2 Continuing either clopidogrel or ticagrelor for at least 48 h prior to surgery significantly increases the risk of massive transfusion and major bleeding complications.3,4 In the elective and stable inpatient setting, P2Y12i should be held 3 to 5 days for ticagrelor, ≥5 days for clopidogrel, and ≥7 days for prasugrel (Fig. 1). 5 By keeping ASA onboard and holding P2Y12i preoperatively in nonurgent patients, one generally maintains the benefits of the lower risk antiplatelet and reduces the risks of bleeding.
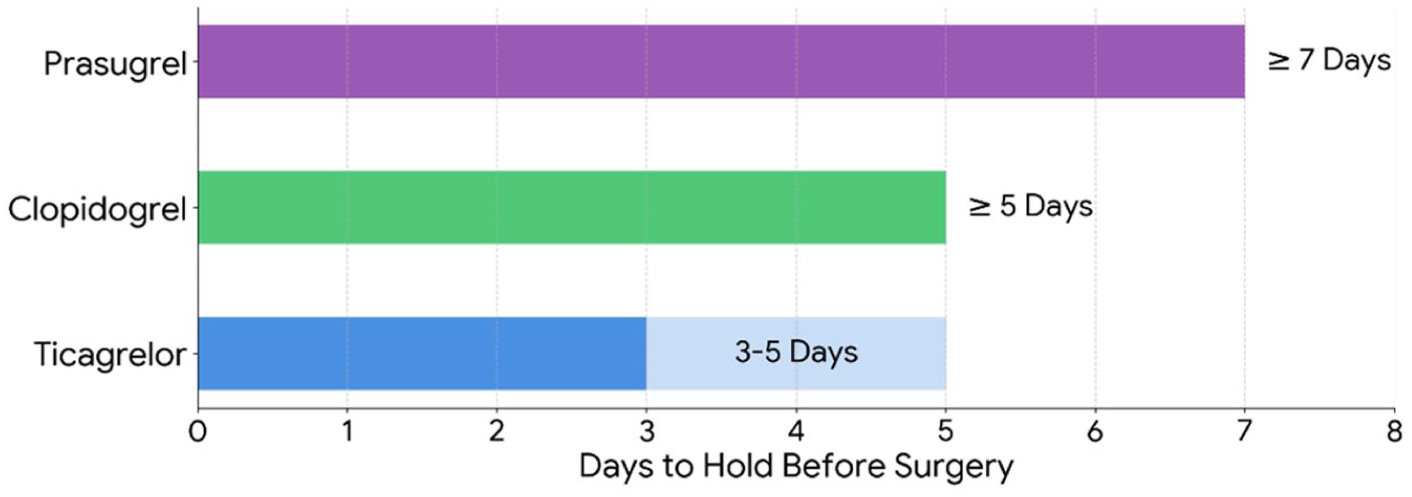
Recommended length in days of withholding oral antiplatelets prior to coronary artery bypass grafting.
2. ASA Should Be Restarted 6 Hours After CABG
ASA is well known for its benefits in patients undergoing CABG; however, the timing of restarting and the dose of ASA after surgery are more controversial. The early initiation of ASA postoperatively has been associated with a reduced risk of death, decreased ischemic complications, and reduced early graft occlusion in CABG patients.1,4,6 A low dose (50 to 100 mg) to medium dose (300 to 325 mg) of ASA should be initiated within 24 h after CABG in order for patients to benefit from these protective effects. A systematic review by Musleh et al. found that the most optimal timing of ASA initiation to maximize cardioprotective effects was within 6 h after CABG, with no benefit seen if started >48 h postoperatively and an increase in reoperation for tamponade if started as early as 1 h postoperatively. 7 When comparing low-dose to medium-dose ASA, major outcomes such as death were similar; however, the medium dose led to increased rates of gastrointestinal bleeding. On the other hand, high doses of ASA are recommended by the American Heart Association and American College of Cardiology as they significantly reduce serum thromboxane B2, a factor common in vein graft failure, and may be beneficial in combating high residual platelet reactivity (HRPR). 8 Indeed, HRPR, or ASA/clopidogrel resistance, is a relatively common clinical phenomenon after CABG that restricts the ability of antiplatelet therapies to inhibit platelet activity. Occurring in as many as 50% of cases and being a major risk factor for vein graft occlusion, early graft failure, and adverse cardiovascular events, higher doses of ASA in the postoperative period have been recommended to combat this effect. Clinical trials such as CASCADE also demonstrated that medium-dose ASA is similar to DAPT with clopidogrel, with no significant difference in vein graft intimal hyperplasia, patency, major bleeding, or major adverse cardiac and cerebrovascular events (MACCE). 9
In summary, to maximize benefit, low-dose ASA given at 6 h postoperatively appears safest; however, regardless of dose, ASA should be initiated within 24 h. After the immediate postoperative period, ASA is recommended to be continued lifelong, with consideration given to using medium-dose ASA (our preferred approach when not using DAPT). With minimal bleeding risk and established graft protection, ASA continues to be of benefit long after the index surgery.
3. OPCAB Can Be a Life Saver in Emergency Surgery for Patients on DAPT
For patients on DAPT who require emergent CABG, OPCAB is a viable, and often preferable, strategy to minimize perioperative bleeding. By avoiding higher activated clotting time targets needed for the bypass circuit, the need for cannulation and extra sites of bleeding, and the secondary platelet dysfunction associated with the use of cardiopulmonary bypass, OPCAB decreases the risk of major bleeding, transfusion requirements, and reopening for tamponade compared with conventional CABG. 10 Also, by minimizing aortic manipulation, OPCAB has been shown to decrease the incidence of stroke, especially in high-risk patients such as those presenting with ACS on DAPT.11,12 In combination, if surgery occurs within the first 2 days of an ACS, OPCAB has shown significantly lower mortality compared with on-pump CABG and should be considered in high-volume centers with surgeons who are experts in off-pump techniques.13,14
4. DAPT May Be Given After CABG in Patients Presenting With ACS
The benefit of DAPT in patients who present with ACS has been well described in those undergoing PCI; however, for patients who proceed to surgical revascularisation, the decision regarding postoperative DAPT is less clear. Recommendations and data continue to shift between favoring and challenging the notion of postoperative DAPT, balancing the risk of bleeding with the benefits of inhibiting platelet aggregation. In post hoc evaluations of randomized controlled trials (RCTs) investigating ACS patients who underwent CABG, mainly CURE and PLATO, DAPT provided significantly lower rates of ischemic events, episodes of MACCE, and all-cause mortality when compared with ASA alone (Fig. 2).15–17 However, these data suffer from selection bias in which the decision for CABG occurred after randomization and thus after potential serious complications, such as major bleeding, may have occurred that would have excluded DAPT patients from the surgery group. 18 This could have artificially favored the DAPT group because only patients who did well on DAPT preoperatively ended up proceeding to surgery in the trial. Moreover, in the CURE trial, most of the prevented events associated with DAPT in surgical patients were observed in the preoperative phase, between the initiation of DAPT and the time of surgery. The TACSI trial, which studied ACS patients receiving CABG, reported no difference in the composite of death, MI, stroke, or repeat revascularization at 1 year between DAPT (ticagrelor + ASA) and ASA alone. 19 However, more than 10% of patients in TACSI were also on oral anticoagulants, and one-third of the patients assigned to ticagrelor did not complete their 1-year treatment, mitigating the overall conclusions. Overall, the data are inconclusive on a clear choice for ACS CABG patients and suggest that DAPT postoperatively in the short-term may be beneficial. In the absence of clear evidence in high-risk populations, the risk of graft occlusion from inadequate platelet inhibition may outweigh the risk of major bleeding, and thus DAPT should be considered according to individual characteristics (e.g., ACS, OPCAB, diffuse coronary artery disease [CAD], prothrombotic phenotype).
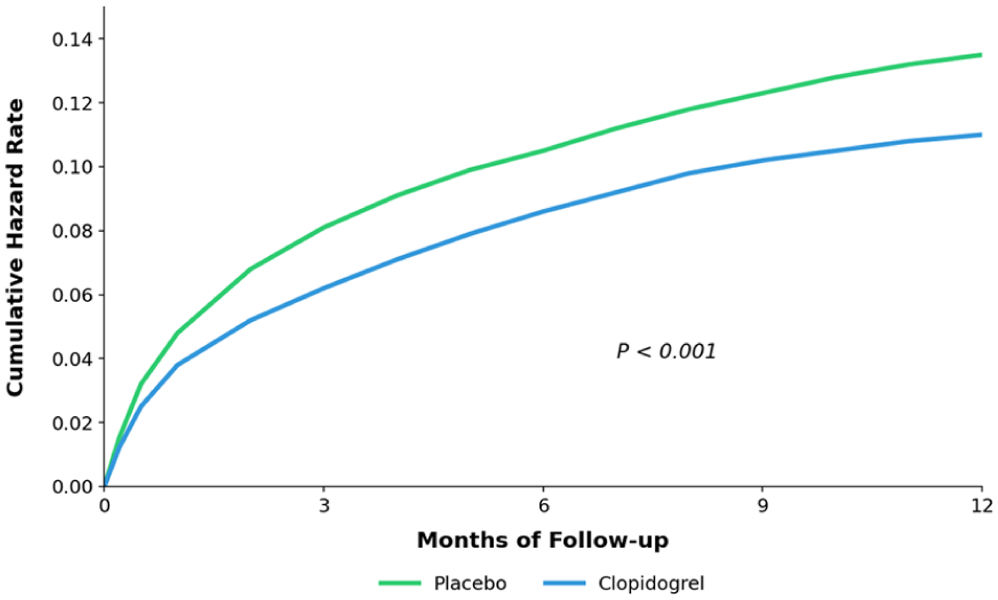
Cumulative hazard rates for the composite of death from cardiovascular causes, nonfatal myocardial infarction, and stroke comparing clopidogrel to placebo over a 12-month period in acute coronary syndrome patients who received coronary artery bypass grafting. Graph adapted and redrawn from data presented by Yusuf et al. in the CURE trial. 17
5. DAPT Should Be Used After OPCAB
Antiplatelet therapies may be of particular importance in OPCAB compared with conventional CABG due to the heightened prothrombotic state of OPCAB. Compared with on-pump procedures, OPCAB stimulates increased platelet activity due to the lower heparin doses and lack of platelet inhibition from the avoidance of cardiopulmonary bypass. To counteract this effect, emphasis is placed on early and continued DAPT therapy in OPCAB, regardless of surgical urgency or ACS presentation. In a systematic review of 4,424 patients, Peksa et al. found DAPT administration after OPCAB increased graft patency and decreased MI and thromboembolism events postoperatively when compared with ASA alone. 20 In the short-term, 3 months of DAPT administration was also not associated with increased incidences of major or minor bleeding, proving it a safe and preferred option for OPCAB patients. Our practice has been to restart DAPT on day 0 after OPCAB when chest drain output is ≤50 mL/h for 2 h. This has been the routine at our institution for more than 2 decades, with a safe risk profile over several thousand patients.21,22
6. Ticagrelor Is More Potent Than Clopidogrel After CABG but Harmful Before CABG
Ticagrelor provides clear early advantages but carries important long-term and perioperative risks that limit its overall favorability before and after CABG. Ticagrelor has a rapid onset and increased overall percentage of platelet inhibition compared with clopidogrel, offering meaningful and quicker initial postoperative protection (Fig. 3a). 23 However, these properties create problems beyond the acute phase when patients recover beyond the initial prothrombotic state of surgery. The initial benefit of almost 90% platelet inhibition may no longer be necessary to provide adequate cardioprotective effect because clopidogrel provides the same long-term benefits in graft patency without an increased risk of major bleeding. In addition to bleeding risk, a lesser recognized side effect of ticagrelor is dyspnea. Ticagrelor increases intravascular adenosine levels as a downstream effect of inhibiting adenosine uptake into platelets, resulting in dyspnea affecting 10% to 20% of patients. In postoperative cardiac surgery patients who commonly have atelectasis, fluid shifts, pleural inflammation, or pulmonary edema, experiencing dyspnea can slow recovery and potentially increase the risk of respiratory complications. In the long-term, even if dyspnea does not cause complications, it can greatly affect adherence to therapy, with studies finding dyspnea-related discontinuation rates significantly higher with ticagrelor than with clopidogrel (Fig. 4). 24
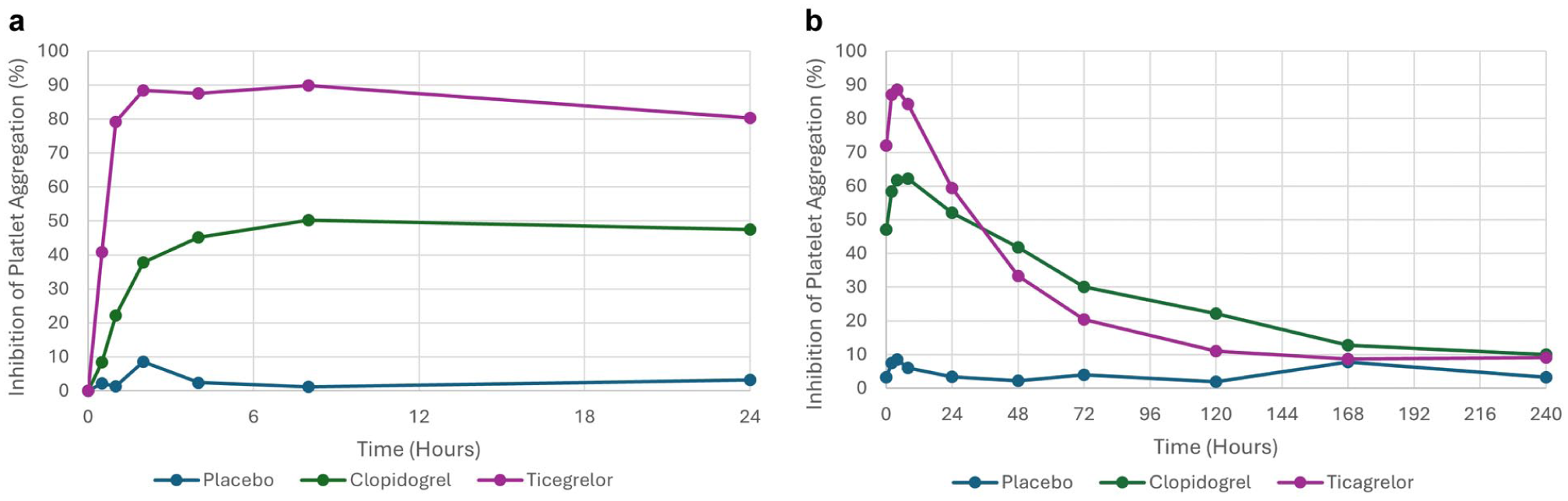
(a) Percentage of platelet aggregation inhibition for patients receiving clopidogrel, ticagrelor, or placebo from time of initial dose to 24 h later. (b) Percentage of platelet aggregation inhibition for patients receiving clopidogrel, ticagrelor, or placebo from time of medication discontinuation until 10 days later. Graph adapted and redrawn from data presented by Gurbel et al. in the ONSET/OFFSET Study. 23
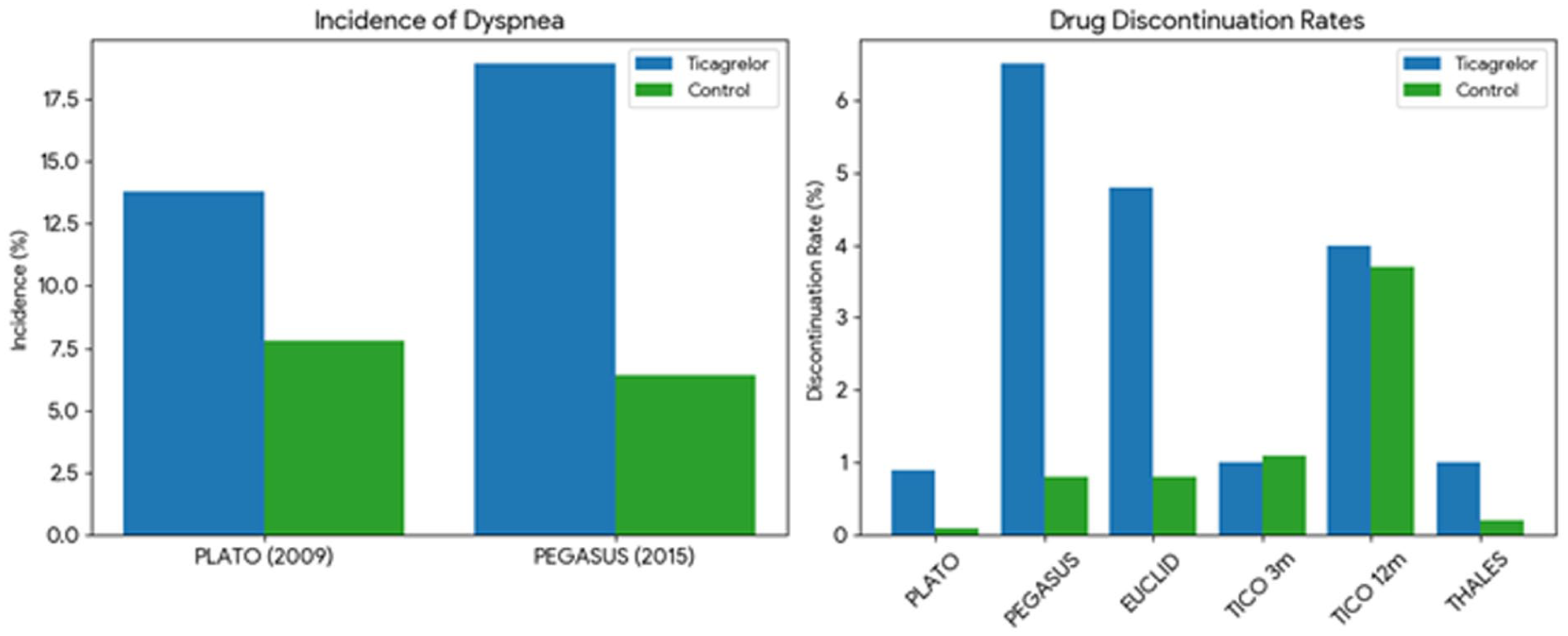
Dyspnea incidence and rate of dyspnea-related discontinuation rates across various randomized controlled trails comparing clopidogrel with ticagrelor. Graph adapted and redrawn from data presented by Kim et al. 24
In the preoperative phase, ticagrelor has been demonstrated to have a faster offset, surpassing clopidogrel after 48 h (Fig. 3b); however, prior to this time it still has significantly higher levels of platelet inhibition with a higher risk for perioperative bleeding if urgent procedures are required. 23 Its reversibility also becomes a disadvantage in the intraoperative setting with the remaining ticagrelor continuing to inhibit newly transfused platelets. This makes platelet transfusion far less effective in patients undergoing CABG while still on ticagrelor, which is not uncommon due to coagulopathies, severe perioperative bleeding, or prolonged cardiopulmonary bypass. In contrast, the irreversible binding of clopidogrel allows for transfused platelets to function normally, which is more optimal in patients requiring CABG while on DAPT. Overall, clopidogrel is the preferred agent for ACS patients without prior PCI when CABG is anticipated, whereas ticagrelor is more advantageous postoperatively in the short-term when the benefits of possible enhanced graft patency and mitigation of early prothrombotic risk outweigh its higher bleeding liability.
7. DAPT Is Not Required Postoperatively in Chronic Stable CAD
For patients undergoing elective CABG for stable CAD, there is little clinical evidence of postoperative DAPT having clinical benefit over ASA alone. An individual patient data meta-analysis of 871 RCT patients demonstrated improved 1-year vein graft patency rates for patients receiving DAPT with ticagrelor versus ASA alone (11.2% vs 20%, P < 0.001); however, it also demonstrated a significantly increased rate of major bleeding. 25 Despite showing a 50% reduction in vein graft failure, there was no change in mortality, ischemic events, or embolic events, suggesting that there was overall more clinical harm than benefit to giving DAPT in patients with chronic stable CAD. Given the lack of current evidence demonstrating clear mortality benefit, DAPT is not traditionally recommended for patients after elective CABG for stable CAD. However, current trials and investigations are starting to show that DAPT with clopidogrel may increase graft patency without significantly increasing bleeding risk, promoting organizations such as the Canadian Cardiovascular Society to recommend the use of DAPT in elective CABG. 26 The international ODIN RCT is currently ascertaining, in 700 patients, whether the use of DAPT with ticagrelor for 1 month after CABG will minimize bleeding complications while maximizing the benefits on all-cause death, stroke, MI, revascularization, and graft failure at 1 year. 27 As this evidence comes out, DAPT use in elective CABG may become more popular and have stronger recommendations.
8. Delay CABG 4 to 6 Weeks After PCI to Prevent In-Stent Thrombosis
Performing CABG in post-PCI patients creates a challenge of timing and bleeding risk mitigation. After PCI, stents have exposed metal in the coronary system that is thrombogenic until the body can “neutralize” it via endothelialization. This process typically takes 4 to 6 weeks, and withholding DAPT during this period increases the risk of stent thrombosis and acute occlusion. When it comes to stable, staged CABG for residual multivessel CAD after PCI, surgery should be delayed for 6 months post-PCI, after which withholding DAPT is safe. If the surgery is urgent and cannot be safely delayed, the risks of severe bleeding while operating on DAPT must be weighted against the risk of stent thrombosis if DAPT is held prior to surgery. Even then, stent thrombosis, with severe consequences, may occur because of surgical manipulations, perioperative inflammation, and a prothrombotic state. A minimum of 6 to 12 weeks is ideal before withholding DAPT in recent PCI patients, 8 and if the patient requires CABG prior to the 6-week minimum, it is recommended to continue DAPT without interruption perioperatively. The use of OPCAB and MICS CABG in this setting has been found beneficial in our practice. If DAPT must be absolutely discontinued in this early period, for instance in a practice that does not include expertise in complex OPCAB, bridging with intravenous cangrelor should be considered prior to holding DAPT completely.
9. Patients With Arterial Grafts May Need Less Antiplatelet Therapy
Among the many benefits of arterial grafting in CABG, internal mammary arteries and radial arteries may not require the added protection of DAPT compared with vein grafts. Arterial grafts do not undergo venous arterialization stress, making them less likely to stimulate the coagulation cascade and enable the platelet adhesion, intimal hyperplasia, and clot formation that DAPT aims to prevent. Arterial grafts have the added benefit of being “living grafts” that respond and adapt to changes in pressure and produce higher levels of nitric oxide and prostacyclin, preventing platelets from adhering to the graft wall. In studies such as the meta-analysis by Nocerino et al. of RCT data including 958 CABG patients, DAPT improved vein graft patency but had no effect on arterial graft patency (Fig. 5). 28 This further promotes multiarterial grafting as a strategy to avoid the bleeding risks associated with DAPT, particularly with total arterial grafting.
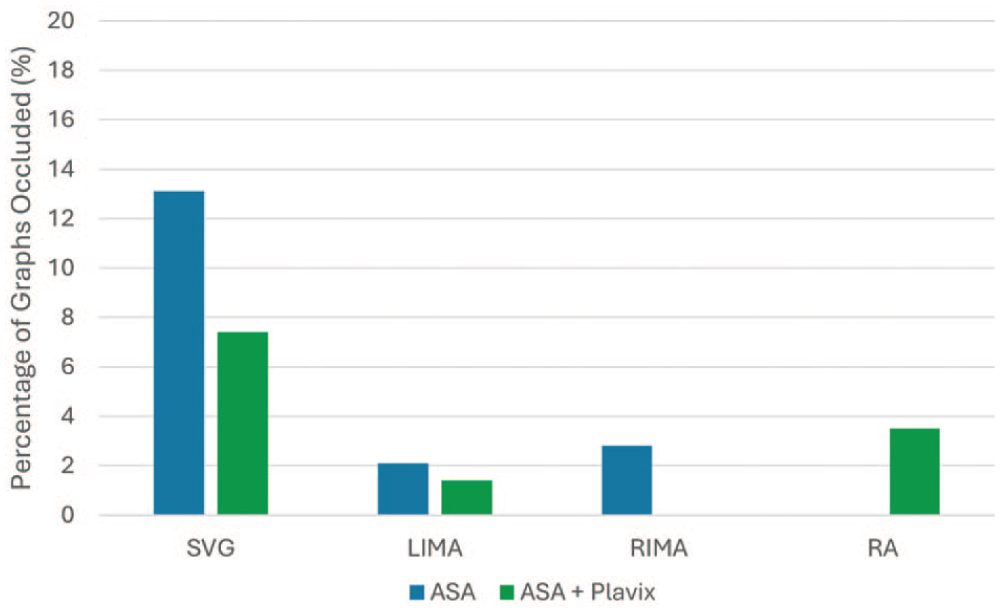
Percentage of graft occlusion events for patients receiving ASA + clopidogrel versus ASA alone compared across graft type. Graph adapted and redrawn from data presented by Mannacio et al. in the CRYSSA Study. ASA, aspirin; LIMA, left internal mammary artery; RA, radial artery; RIMA, right internal mammary artery; SVG, saphenous vein graft.
10. Clopidogrel Monotherapy Is Acceptable in CABG Patients With ASA Allergy
In stable preoperative CABG patients with ASA allergy, rapid inpatient ASA desensitization is preferred when surgical timing and clinical stability allow, as it can safely restore ASA tolerance in most cases. In patients with a history of life-threatening anaphylaxis, severe systemic hypersensitivity, or when urgent antiplatelet therapy is required, clopidogrel monotherapy is an appropriate and evidence-supported first-line alternative.17,29 In the stable CAD post-CABG context, clopidogrel provides adequate long-term platelet inhibition with a lower bleeding risk than a more potent P2Y12i such as ticagrelor. Therefore, clopidogrel offers a favorable balance between maintaining graft patency and minimizing postoperative hemorrhagic complications. Consequently, lifelong clopidogrel monotherapy is considered an acceptable strategy for ASA-allergic patients who are unable to complete desensitization.
Conclusions
This article summarizes the best evidence and current clinical opinion on antiplatelet management before and after CABG (Fig. 6). These 10 commandments underscore the need for individualized, evidence‑driven antiplatelet strategies in patients undergoing CABG with a focus on balancing the benefits of ischemic protection with the risks of bleeding and its long-term consequences. Most notably, surgeons and physicians who care for CABG patients need to recognize when DAPT is essential compared with when monotherapy is sufficient and adapt antiplatelet therapy to graft type, surgical urgency, and patient‑specific indications. We hope that these principles will help guide and clarify antiplatelet therapy in CABG patients so that clinicians can optimize perioperative safety, preserve graft function, and improve long‑term cardiovascular outcomes across the wide spectrum of CABG populations.

Summary figure of the 10 commandments of DAPT in CABG. ACS, acute coronary syndrome; ASA, aspirin; CABG, coronary artery bypass grafting; CAD, coronary artery disease; DAPT, dual-antiplatelet therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.