
Abstract

Introduction
The evolution of cardiac surgery has been marked by continuous efforts to reduce surgical trauma while maintaining or improving procedural efficacy.1,2 Over the past few decades, pioneering work by surgeons such as Alain Carpentier, widely regarded as the father of modern mitral valve (MV) repair; 3 Friedrich Mohr, a great pioneer in minimally invasive cardiac surgery (MICS); 4 Hugo Vanermen, one of the early adopters of MICS and especially totally endoscopic MICS; 5 and Randolph Chitwood, one of the first to systematically use the robot and telemanipulation in MV surgery, 6 laid the groundwork for the transition from traditional median sternotomy to more refined approaches. Early innovations, including the development of Carpentier’s ring annuloplasty for MV repair, helped establish new standards of valve durability and functional outcomes. 7 Meanwhile, Vanermen’s and Chitwood’s successful demonstration of totally endoscopic/robotic procedures in the late 1990s showcased the viability and safety of MICS. 8
These advancements paved the way for a new era in MV and tricuspid valve (TV) surgery, shifting from direct vision approaches to video-assisted and finally totally endoscopic techniques. This transition promises numerous benefits, including reduced postoperative pain, shorter hospital stays, faster recovery times, and improved cosmetic outcomes. 9 However, the journey from traditional open surgery to totally endoscopic techniques is not without challenges. It requires careful patient selection, specialized training, and a structured learning curve for the whole surgical team.10,11
To ensure a safe and effective shift from direct vision to endoscopic MV and TV surgery, it is crucial to adhere to basic principles that guide surgical practice, team dynamics, patient safety, and continuous professional development. The following “10 Commandments” should serve as essential guidelines for cardiac surgeons embarking on this transformative journey. They emphasize the importance of mastering fundamental skills, building a cohesive multidisciplinary team, embracing simulation and continuous learning, and ultimately prioritizing patient outcomes above all.
1. Thou Shalt Master the Fundamentals
Establishing a robust basis in MV and TV surgery under direct vision is an indispensable prerequisite before moving into the totally endoscopic MICS techniques. This includes a comprehensive understanding of cardiac anatomy, valve morphology, pathophysiology, and the principles underlying successful valve repair and replacement. It is critical to become adept at traditional open surgical approaches, as they provide tactile feedback and visual cues that form the basis for advanced procedures. Whenever possible, seek hands-on experience in MICS, endoscopic, or robotic surgery to familiarize yourself with the nuances of these approaches. Mastery of the fundamentals ensures not only technical proficiency but also the confidence to handle intraoperative challenges with precision and control.
2. Thou Shalt Build a Multidisciplinary Team
Assemble a dedicated, well-trained multidisciplinary team comprising anesthesiologists, perfusionists, scrub nurses, and echocardiographers experienced in MICS procedures. Each team member plays a critical role in ensuring the success and safety of the operation. Anesthesiologists must be proficient in managing patients undergoing single-lung ventilation and capable of advanced hemodynamic monitoring. Perfusionists should be skilled in managing peripheral cannulation and minimally invasive cardiopulmonary bypass circuits. Scrub nurses need specialized training in handling long-shafted endoscopic instruments and anticipating the surgeon’s needs. Echocardiographers, both preoperatively and intraoperatively, provide essential real-time imaging to guide surgical decisions.
Effective communication and collaboration within this team are not just beneficial but essential for procedural success. Regular team briefings, debriefings, and simulation drills help build a culture of trust and responsibility. Establishing clear protocols for intraoperative decision-making, including predefined criteria for conversion to open surgery, enhances team efficiency and patient safety. A cohesive team that understands the nuances of MICS can anticipate challenges, adapt to unexpected situations, and contribute significantly to optimal surgical outcomes.
3. Thou Shalt Invest in Training and Simulation and Respect the Learning Curve
Mastery in totally endoscopic MV and TV surgery is achieved through continuous and structured training. Before performing procedures on patients, surgeons must engage in rigorous simulation-based training designed to replicate real-life surgical conditions. This includes hands-on practice with endoscopic (long-shafted) instruments to develop precision, navigating complex camera angles, and mastering ergonomics unique to MICS.12,13 In the meantime, 3-dimensional (3D) printing technologies with promising educational and training opportunities broadened the training and simulation opportunities for MICS and endoscopic cardiac surgery. 14
Acknowledging the learning curve is critical; achieving proficiency requires dedication, time, and a methodological approach. 15 Continuous self-assessment through video reviews of past surgeries allows for the identification of technical gaps and refinement of skills. Regular feedback from experienced mentors—whether through direct observation or remote—enhances learning efficiency. 16
Training should be seen not as a finite process but as an ongoing journey. Cultivating a mindset focused on incremental improvement boosts resilience and patience, which are essential attributes in endoscopic surgery. The ability to remain composed during complex cases and to adapt techniques based on reflective practice distinguishes the proficient surgeon from the novice. Endoscopic surgery is, indeed, the ultimate school of patience, demanding both technical excellence and a lifelong commitment to learning.
4. Thou Shalt Do Preoperative Preparation and Planning
Comprehensive preoperative preparation and planning is the cornerstone of successful fully endoscopic MV and TV surgery. This involves more than routine diagnostics; it requires a systematic approach to evaluating the patient’s overall condition and surgical suitability. Detailed imaging, including high-resolution multislice angiography computed tomography (CT) scans (Fig. 1), including both the thoracic part and the peripheral vessels, transesophageal echocardiography, and, when necessary, cardiac magnetic resonance imaging, provides critical insights into anatomical variations, vascular access routes, and potential procedural challenges.
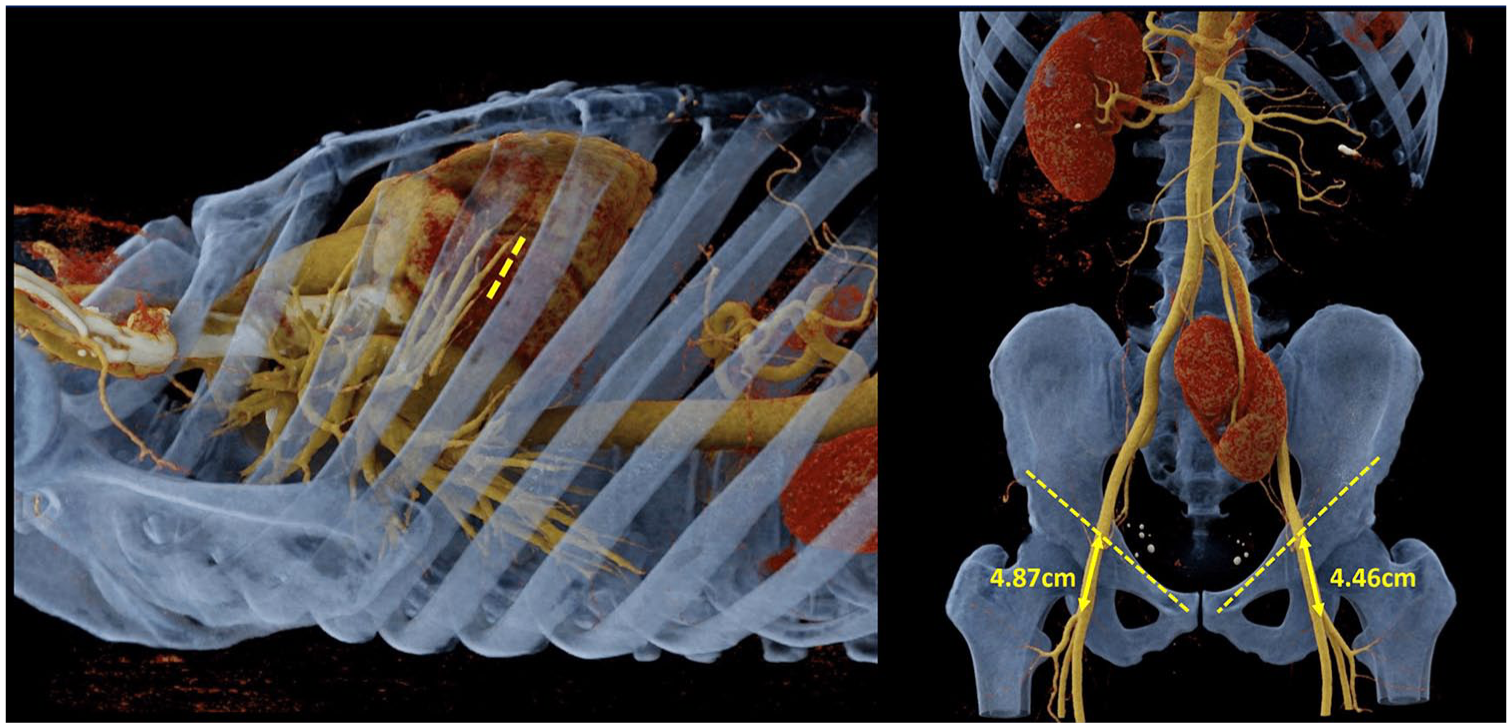
Preoperative computed tomography 3-dimensional scans using cinematic volume rendering technology with postprocessing syngo.via software (Siemens Healthineers AG, Erlangen, Germany) for optimal of access and cannulation strategy.
Meticulous planning should also encompass the assessment of comorbidities, coagulation status, and previous surgical history, which may influence intraoperative decisions. Developing a well-structured surgical strategy includes outlining primary and contingency plans, anticipating possible complications, and ensuring the availability of all necessary instruments and equipment.
Preoperative discussions with the multidisciplinary team are essential to align surgical objectives, clarify roles, and optimize intraoperative coordination. By fostering a culture of thorough preparation, surgeons can enhance procedural efficiency, reduce intraoperative stress, and improve patient outcomes. Remember, a well-prepared surgeon is not only technically ready but also mentally and strategically equipped to manage unexpected situations.
5. Thou Shalt Start With Simple Cases
The journey into totally endoscopic MV and TV surgery should begin with cases that present minimal anatomical and pathological complexity. Focus on patients with isolated MV prolapse, particularly involving the posterior leaflet, as these cases often provide clearer exposure and more predictable repair techniques. Similarly, uncomplicated TV repairs without leaflet pathology offer an ideal starting point.
These simpler cases serve as a practical platform to refine the technical aspects of endoscopic surgery, such as handling long-shafted instruments, mastering endoscopic suturing, and optimizing camera navigation. They also allow the surgical team to adapt to new workflows, improve coordination, and fine-tune intraoperative communication in a controlled environment. Gradually increasing the complexity of cases, once foundational skills are firmly established, helps build the surgeon’s confidence while minimizing patient risk. This stepwise approach is essential for developing the proficiency needed to manage more challenging pathologies safely and effectively in the future.
6. Thou Shalt Always Prepare the Operative Setting Thoroughly
The basis of a successful totally endoscopic MV and TV surgery lies in the meticulous preparation of the operative setting. This extends beyond standard surgical protocols to encompass every detail that influences intraoperative efficiency and patient safety. Optimal cannulation is of paramount importance, with careful consideration given to peripheral access routes to ensure stable and effective circulatory support. This includes precise placement of arterial and venous cannulas to minimize the risk of vascular complications and facilitate adequate perfusion. 17 One critical aspect is venous drainage, which traditionally relies on dual cannulation—using a superior vena cava cannula and an inferior vena cava cannula—to ensure effective venous return. However, this approach can be technically demanding in a fully endoscopic setting due to limited access and visualization. Besides specially designed long venous cannulas, which are being placed mainly through the right femoral vein, a promising innovation in this field is the venous virtually wall-less cannula (smartcanula, SmartCanula sárl, Lausanne, Switzerland; Fig. 2), a self-expandable stent cannula using the principles of high surface tension. 18 Van Praet et al. showed that the venous smartcanula allows optimal venous drainage at low negative drainage pressures, facilitating sufficient perfusion. 19
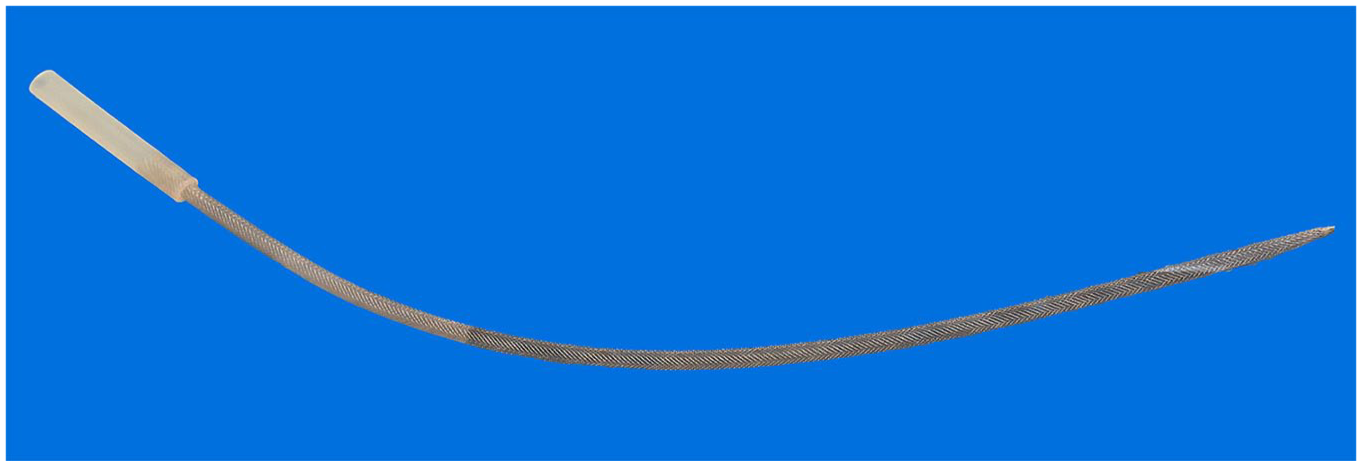
Venous virtually wall-less self-expandable smartcanula (SmartCanula sárl, Lausanne, Switzerland).
Equally critical is the management of this peripheral perfusion setting. Establish robust monitoring protocols to detect any signs of limb ischemia early and ensure perfusion lines are securely positioned to avoid kinking or dislodgement.
Effective cardioplegia administration is essential for myocardial protection; select the appropriate cardioplegia solution and delivery method based on the patient’s cardiac anatomy and procedure specifics. Continuous monitoring of myocardial temperature and perfusion ensures that the heart remains well protected throughout the whole surgery.
In addition, the arrangement of surgical instruments, endoscopic equipment, and perfusion devices should promote a seamless workflow (Fig. 3). Position monitors and cameras to provide the surgeon with an unobstructed, high-definition view of the operative field. Regularly check and calibrate all equipment before the procedure to prevent technical issues. By dedicating time and attention to these preparatory steps, the surgical team can create an environment that maximizes efficiency, minimizes risks, and supports the delivery of optimal patient care.
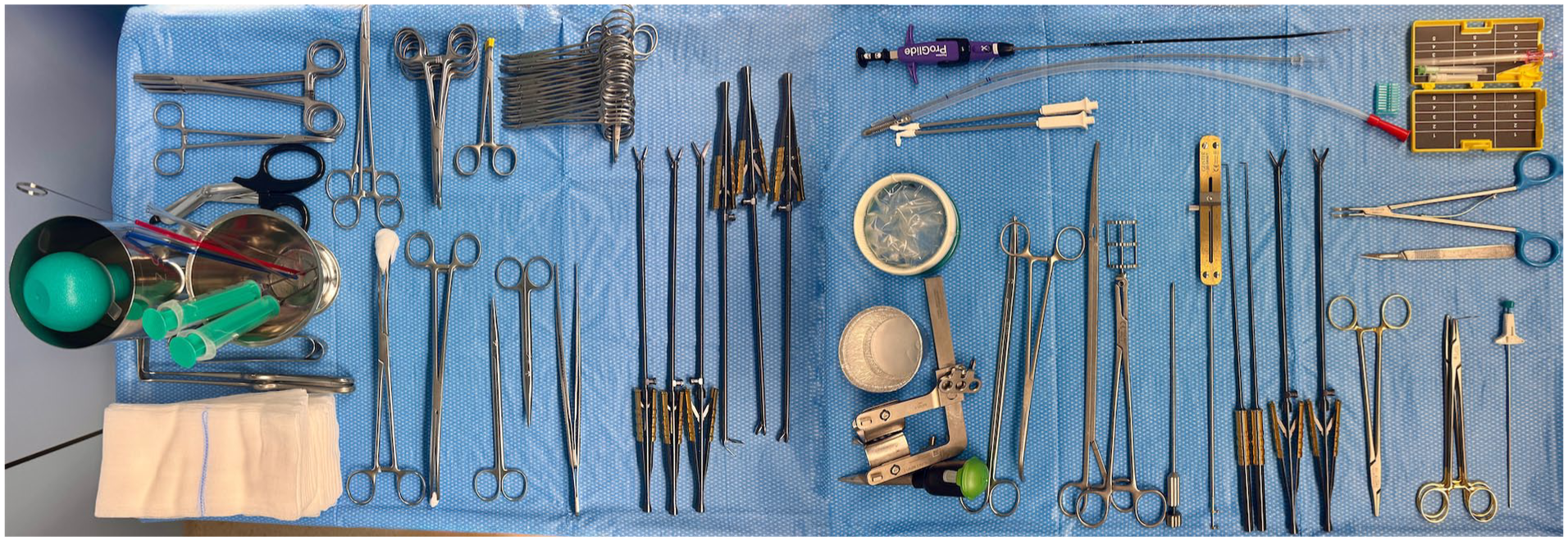
Typical set of instruments, including long-shafted instruments, Chitwood clamp, soft-tissue retractor, for minimally invasive and totally endoscopic mitral and tricuspid valve surgery.
In conclusion, successful surgery begins with meticulous preparation of the operative environment; therefore, perform optimal cannulation and effective cardioplegia to ensure myocardial protection throughout the procedure.
7. Thou Shalt Maintain Optimal Visualization
Achieving and maintaining optimal visualization is the basis of successful totally endoscopic MV and TV surgery. Superior exposure begins with strategic patient positioning and careful placement of the endoscopic ports to provide the best possible access to the operative field (Fig. 4). Adjust lighting meticulously to reduce glare and enhance depth perception, ensuring that anatomical structures are clearly visible at all times. Commandment 4 will help you with this point. For example, use 3D CT postprocessing software, such as syngo.via software (Siemens Healthineers AG, Erlangen, Germany) or 3mensio Structural Heart software (3mensio Medical Imaging BV, Utrecht, The Netherlands), to prepare and plan for the patient in your head.
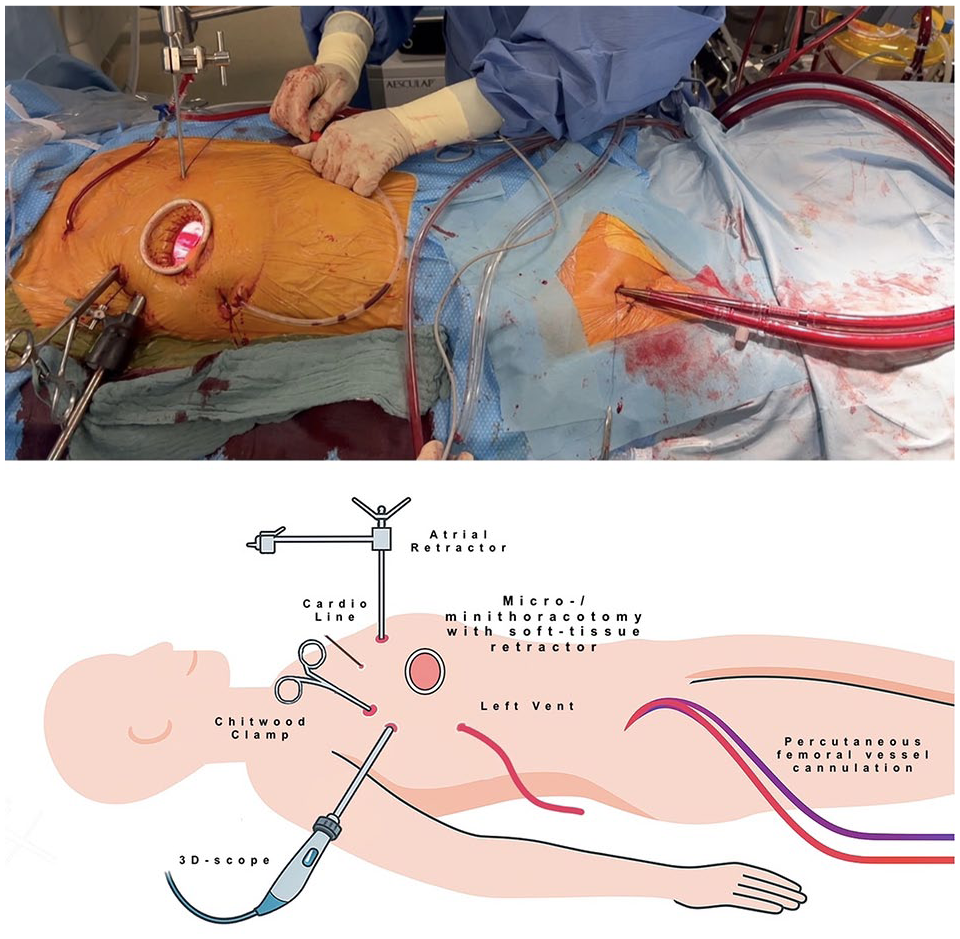
Intraoperative setting for minimally invasive and totally endoscopic mitral and tricuspid valve surgery. 3D, 3-dimensional.
Optimize camera angles to avoid distorted perspectives using high-definition or 3D imaging systems (Fig. 5) when available to improve spatial orientation. Position instruments thoughtfully to minimize visual obstruction and reduce instrument collisions, allowing for smooth, coordinated movements. In complex procedures, such as endoscopic aortic valve replacement and/or combined procedures, precise control over the camera and instruments is of paramount importance. Identifying and maintaining the correct angle for endoscopic instruments facilitates better visualization of valve structures, enhances suturing accuracy, and improves the surgeon’s overall efficiency. Regularly reassess visualization throughout the procedure, adjusting as needed to accommodate shifts in anatomy or surgical technique. Incorporate real-time feedback from the surgical team to ensure a consistently clear and unobstructed view, thereby reducing the risk of technical errors and enhancing procedural safety.

EinsteinVision® 3-dimensional endoscopic video tower system (AESCULAP, B. Braun, Melsungen, Germany).
8. Thou Shalt Avoid Complacency With Safety Protocols
Unwavering adherence to safety protocols is the foundation of successful totally endoscopic MV and TV surgery. This begins with meticulous patient selection, ensuring that only candidates with favorable anatomical and clinical profiles are chosen for minimally invasive and especially totally endoscopic approaches. A thorough preoperative evaluation should identify any potential risk factors that could complicate the procedure.
Intraoperatively, comprehensive transesophageal echocardiographic assessment is essential. It provides real-time visualization of valve function, ventricular performance, and the positioning of cannulas and surgical instruments. Surgeons and anesthesiologists must collaborate closely to interpret these findings and adjust the surgical strategy as needed.
In addition, always maintain readiness for an immediate conversion to open surgery via sternotomy, if complications arise. This requires having the necessary instruments, equipment, and trained personnel available throughout the procedure. Establishing clear protocols for rapid conversion and conducting regular team drills can improve response times and outcomes during critical situations.
Finally, respect for surgical indications and contraindications must remain paramount. Avoid extending the scope of minimally invasive techniques beyond their proven efficacy, especially in complex or high-risk cases. Prioritizing patient safety over procedural ambition ensures consistent, high-quality outcomes.
9. Thou Shalt Embrace Technological Advancements Wisely
The integration of technology into endoscopic MV and TV surgery has significantly expanded the boundaries of what is surgically possible. Leverage cutting-edge technologies such as 3D endoscopy, which enhances depth perception and spatial orientation, providing a more immersive view of the operative field. Advanced imaging modalities, including high-definition cameras and intraoperative 3D echocardiography, offer detailed anatomical visualization, aiding in precise surgical navigation.
Robotic assistance can further refine surgical precision, allowing for greater dexterity and control in complex procedures. 20 However, the adoption of these advanced tools must be grounded on a solid basis of fundamental totally endoscopic techniques. Surgeons should probably first achieve proficiency with basic MICS approaches to ensure they fully understand the underlying principles and limitations of endoscopic surgery.
Modern devices can enhance procedural efficiency, such as an automated dual curved needle annular suturing device (RAM® Device, LSI SOLUTIONS, Victor, NY, USA) and/or a suture fastening and trimming COR-KNOT® device (LSI SOLUTIONS; Fig. 6), designed to expedite secure suturing and suture fastening. Nevertheless, these technologies should be used thoughtfully, with a clear understanding of their functioning and potential pitfalls. Continuous evaluation of new technologies, balanced with clinical judgment and evidence-based practice, ensures that technological advancements enhance surgical outcomes without compromising patient safety.
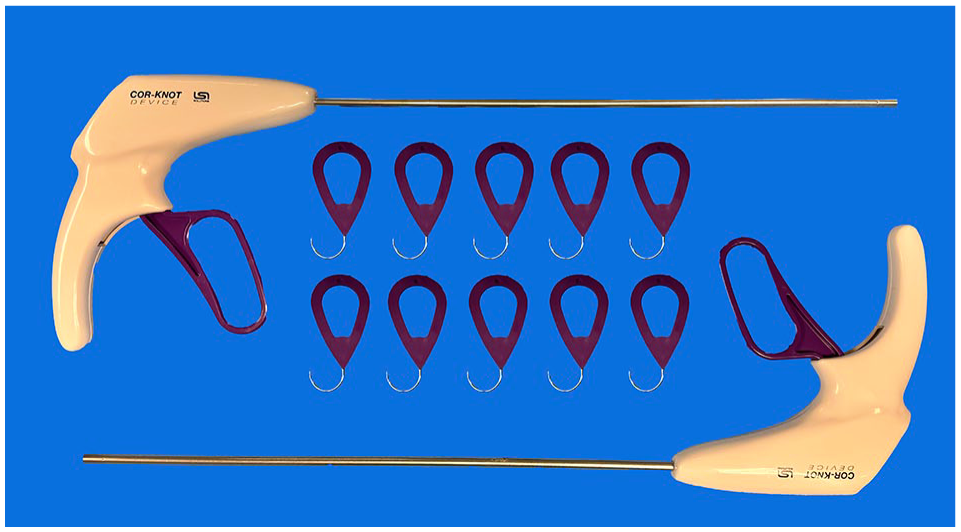
Suture fastening and trimming COR-KNOT® device (LSI SOLUTIONS, Victor, NY, USA).
10. Thou Shalt Prioritize Patient Outcomes Above All
The primary goal of totally endoscopic MV and TV surgery is to ensure patient safety and achieve optimal surgical outcomes. This requires precision, thoroughness, and adherence to the principle of “do not harm,” especially during the early learning phase when technical risks are higher. Surgical excellence is defined by durable valve repairs, minimal complications, and rapid recovery—not by speed.
Beyond the operating room, patient-centered care involves transparent communication about risks, benefits, and expected outcomes. Continuous learning and self-assessment, guided by postoperative results and patient feedback, are essential for ongoing improvement. Ultimately, a steadfast commitment to patient outcomes fosters trust, enhances surgical success, and upholds the highest standards of cardiac care.
Conclusions
The transition from traditional direct vision techniques to totally endoscopic MV and TV surgery represents a transformative journey in cardiac surgery. This evolution is marked by the need for comprehensive training, meticulous preparation, technological integration, and unwavering commitment to patient safety.
In addition, we would like to introduce an 11th Commandment: Thou Shalt Always Stay in Contact With Enthusiastic Endoscopic Cardiac Surgeons. This Commandment provides a framework for navigating this complex landscape, emphasizing the importance of foundational knowledge, teamwork, continuous learning, and the pursuit of surgical excellence.
Although technical skills and procedural knowledge are critical, the center point of successful endoscopic surgery lies in a surgeon’s dedication to patient outcomes and professional growth. By adhering to these principles and boosting strong connections within the surgical community, cardiac surgeons can ensure that their practice remains dynamic, innovative, important, and consistently aligned with the highest standards of care.
Footnotes
Acknowledgements
The authors acknowledge the use of ChatGPT (OpenAI, GPT-4) exclusively for language refinement, including grammar correction and improvements in clarity and style. No scientific content, data interpretation, analyses, or conclusions were generated using artificial intelligence. All outputs from the tool were critically reviewed and revised by the authors, who retain full responsibility for the integrity and accuracy of the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.