
Abstract
Objective:
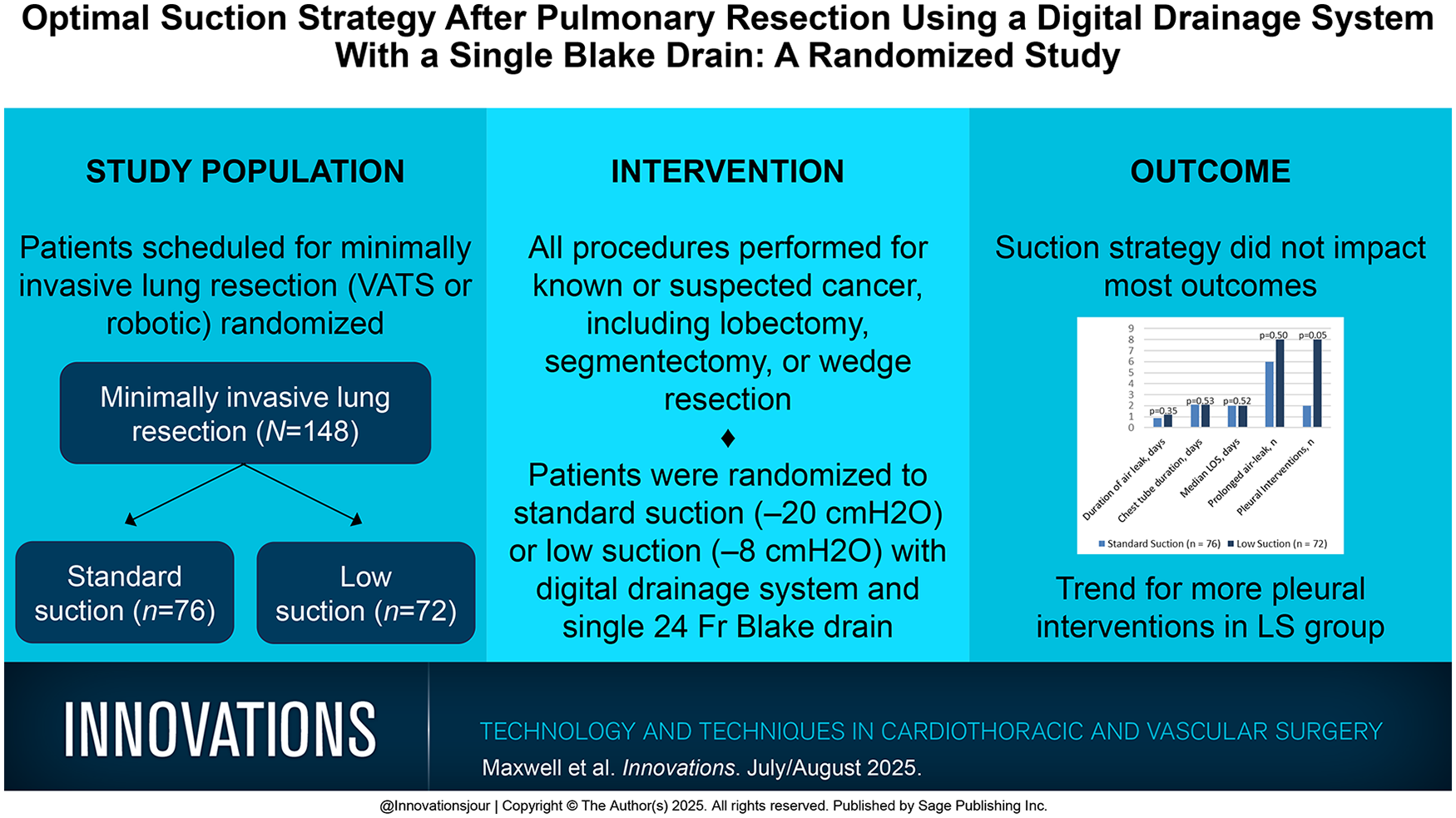
Chest tube management after pulmonary resection is not standardized. Surgeons vary regarding the use of suction versus water seal, single versus multiple drains, drain type, and drainage threshold before removal. A randomized study was undertaken comparing standard suction (SS) of −20 cmH2O to low suction (LS) of −8 cmH2O using digital drainage systems. The primary aim was to demonstrate a shorter duration of air leak with LS. Secondary aims included chest tube duration, length of stay between arms, and the effectiveness of using a single 24 Fr Blake (channel) drain.
Methods:
Patients scheduled for minimally invasive lung resection were eligible. The threshold for tube removal was a drainage volume of ≤450 mL/24 h and air leak of ≤20 mL/min over 6 h.
Results:
A total of 148 patients were eligible (76 SS and 72 LS). There were no differences in baseline characteristics. The duration of air leak (0.9 vs 1.2 days), chest tube duration (2.1 vs 2.1 days), hospital stay (2 vs 2 days), and prolonged air leak incidence (8% vs 11%) were not significantly different. In LS patients, there were more pleural interventions required (11% vs 3%, P = 0.05) and a trend for more subcutaneous emphysema (14% vs 4%) on chest x-ray before chest tube removal.
Conclusions:
The routine use of a 24 Fr Blake drain and a drainage threshold of 450 cc/24 h for chest tube removal was safe and effective. We found no advantage of LS. However, more pleural interventions were required and a trend for increased subcutaneous emphysema with LS was found, suggesting SS may be preferred when an air leak is present.
Get full access to this article
View all access options for this article.