
Abstract
Objective:
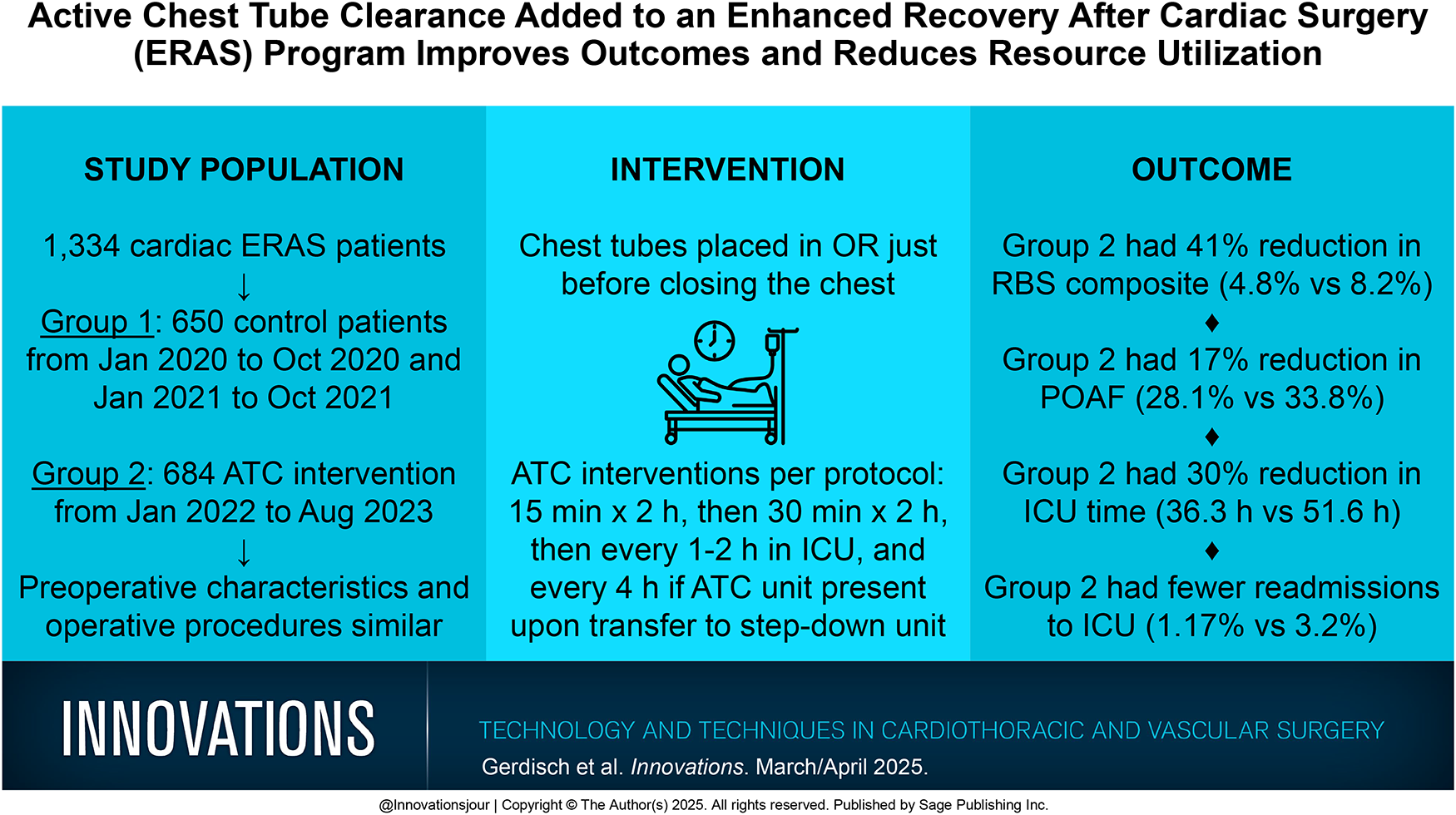
We initiated a cardiac enhanced recovery after cardiac surgery (ERAS) program in early 2019, protocolized it and applied it to all patients in 2020, and added the use of active chest tube clearance (ATC) in 2022. Prospective data collection of ATC patients was compared with historical controls to determine the impact of the device on outcomes.
Methods:
The study comprised 1,334 patients with 650 in the control group (group 1) and 684 in the ATC intervention group (group 2). Group 1 (historical control) consisted of 650 patients from January 1, 2020, to October 31, 2020, and January 1, 2021, to October 31, 2021. From October 31, 2021, to December 31, 2021, we introduced ATC use per protocol. Group 2 (ATC) consisted of 684 patients treated consecutively from January 1, 2022, to August 31, 2023, with ATC. The preoperative characteristics and operative procedures between groups were similar.
Results:
Patients in the ATC intervention (group 2) experienced a 41% reduction in the composite of retained blood syndrome (8.2% in group 1 vs 4.8% in group 2, P = 0.014). Postoperative atrial fibrillation was 17% reduced for group 2 (178 [33.8%] in group 1 vs 158 [28.1%] in group 2, P = 0.049). Group 2 had a 30% reduction in median intensive care unit (ICU) hours (51.6 [30.1 to 76.9] h in group 1 vs 36.3 [20.7 to 687] h in group 2, P < 0.001). Twenty-one patients (3.2%) were readmitted to the ICU after initial discharge to the step-down unit in group 1 and only 8 (1.17%) in group 2 (P = 0.013).
Conclusions:
The addition of the ATC intervention to an established ERAS program in a high-volume private practice setting decreased complications, improved outcomes, and decreased resource utilization.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.