
Abstract
Objective:
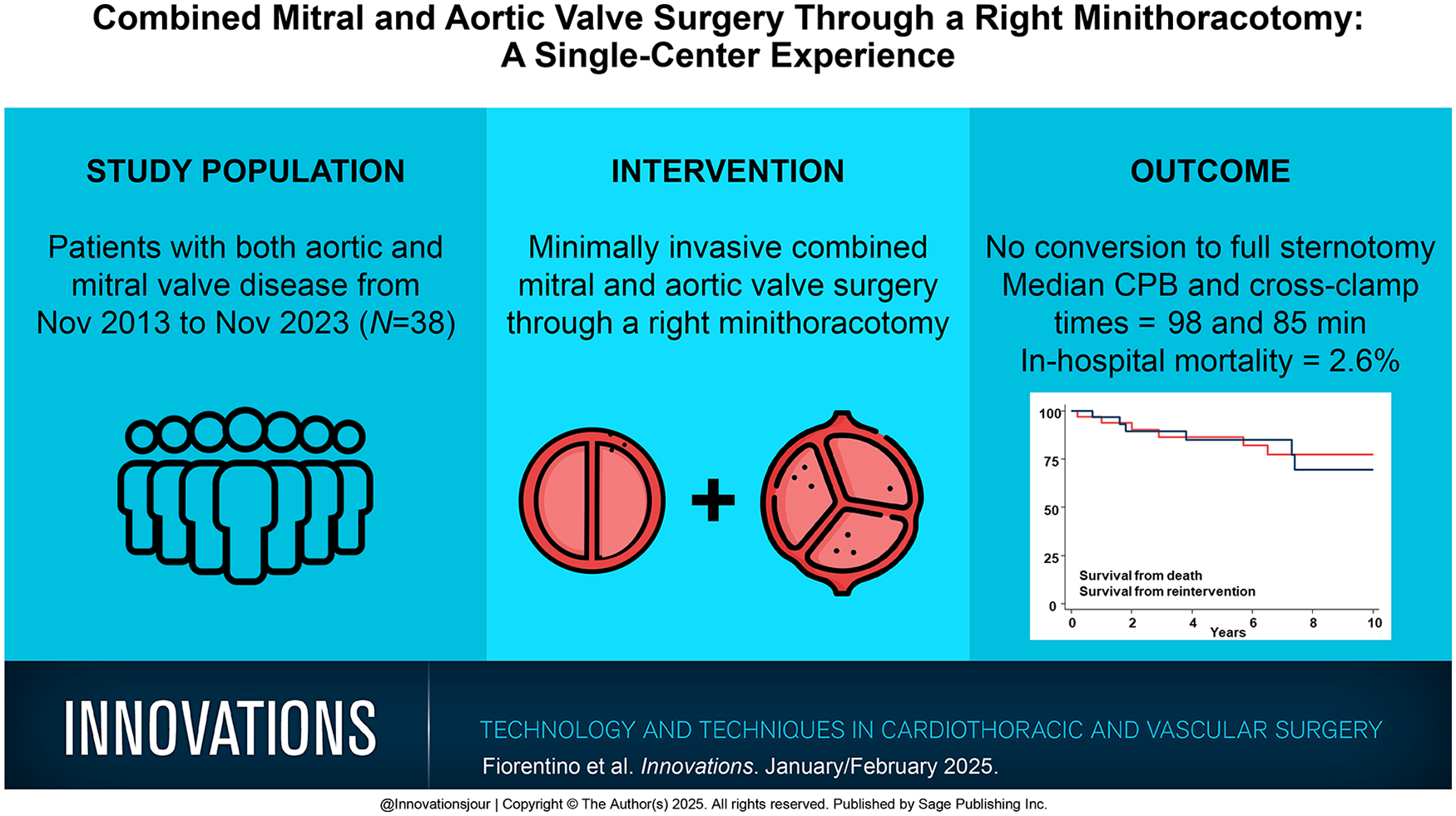
Minimally invasive combined mitral and aortic valve surgery is still uncommon. We report our experience performing multiple valve procedures through a right-sided minithoracotomy.
Methods:
We present an observational case series with a retrospective analysis of 38 patients who underwent double valve surgery through right anterior thoracotomy from November 2013 to November 2023.
Results:
The median age of our population was 72 years, and 61% were female patients. The median EuroSCORE II was 2.27. Three patients (7.9%) had redo operations. The median cardiopulmonary bypass (CPB) and cross-clamp times were 98 and 85 min, respectively. No conversion to full sternotomy was necessary. In-hospital mortality was 2.6% (1 patient); the patient died of septic shock and consequent multiorgan failure. Of the patients, 53% required transfusions with packed blood cells. Postoperative atrial fibrillation was observed in 12 patients (32%), and 2 patients (5.2%) required pacemaker implantation due to third-degree atrioventricular block. Also, 1 stroke (2.6%) and 1 rethoracotomy for bleeding were observed. The median ventilation time was 10 h. The median intensive care unit and postoperative length of stay were 2 days and 7.5 days, respectively. Survival at 1, 3, 5, and 10 years was 93.8%, 86.3%, 86.3%, and 77.2%, respectively, with a median follow-up time of 6.5 years. Freedom from reintervention at 1, 3, 5, and 10 years was 96.8%, 89.5%, 85.0%, and 69.5%, respectively, with a median follow-up time of 5.7 years.
Conclusions:
In our experience, a minimally invasive approach for combined aortic and mitral valve surgery is safe and feasible, with acceptable CPB and cross-clamp times and good outcomes. Therefore, it can be an attractive option for patients with double valve diseases.
Get full access to this article
View all access options for this article.