
Abstract

Introduction
The aorta is a complex organ, and the treatment of aortic disease has become increasingly complex. This is reflected in the most recent guidelines on the treatment of aortic disease published by the American College of Cardiology and American Heart Association in 2022 (“American” guidelines) and the European Association for Cardio-Thoracic Surgery and Society of Thoracic Surgeons in 2024 (“European” guidelines), which span 148 and 99 pages, respectively.1,2 As aortic disease is largely asymptomatic until the development of catastrophic complications, its care is underpinned by imaging. The following 10 commandments focus on the imaging and treatment of stable aortic disease in the proximal thoracic aorta.
On a most basic level, the goal of caring for patients with aortic disease, most commonly aneurysmal disease, is the avoidance of 2 devastating complications, namely, dissection and rupture (i.e., adverse aortic events [AAEs]). From a biomechanical perspective, dissection occurs when the aortic wall stress exceeds the aortic wall strength.3,4 Unfortunately, neither aortic wall stress nor strength can be measured in vivo, but wall stress can be determined with computational modeling (Fig. 1). Thus, the holy grail of aortic imaging is a modality that provides in vivo surrogates of aortic wall stress and strength over time. Until such a development, we must rely on current imaging modalities that largely use aortic size as a proxy for wall stress and subsequent risk for AAE. Below are 10 commandments that we follow when using current imaging in the care of aortic patients.
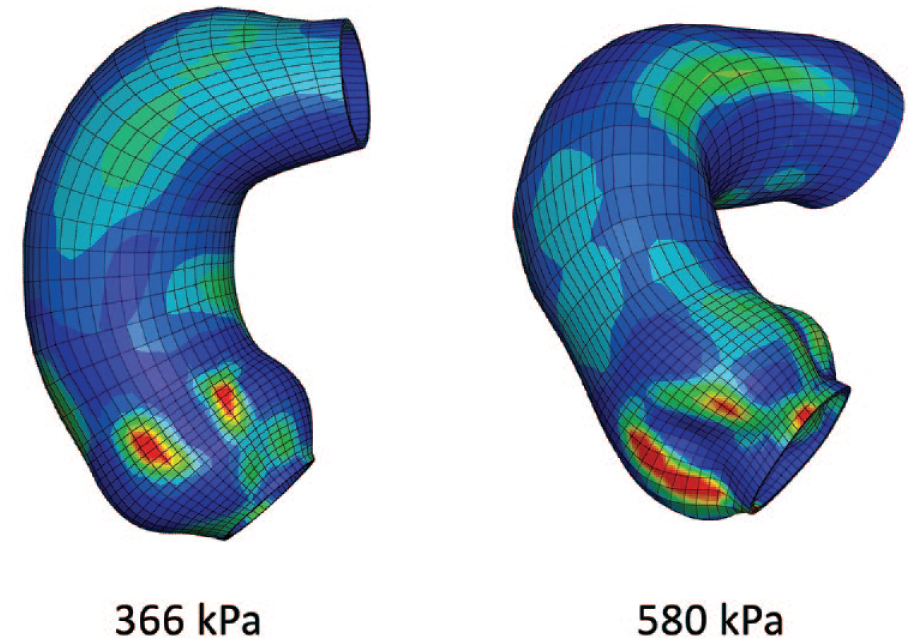
Peak longitudinal stresses of root and ascending aortic aneurysms derived from computational modeling of electrocardiogram-gated computed tomography angiography scans.
1. Understand the Imaging Modality
The most common aortic imaging modalities today are transthoracic (and transesophageal) echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI). It is critically important to understand the details of each, technical variations, limitations, and how the different modalities relate to each other.
Echocardiography (typically transthoracic) is frequently used as a screening tool for aortic root and ascending aortic aneurysms.5,6 It is easy and quick to obtain, does not require contrast, and allows for assessment of heart and valve function. 7 Importantly, it distinguishes between tricuspid and bicuspid aortic valves, which has relevance in aortic disease. As such, it is an excellent screening tool. However, it has several limitations that preclude it from providing accurate aortic measurements. It is significantly dependent on the person performing the exam. A “true” aortic measurement requires 3-dimensional (3D) centerline analysis to provide imaging at an orthogonal plane (see next commandment), and this can be difficult to achieve with echocardiography. Furthermore, the most common reporting standard for aortic measurements with transthoracic echocardiography (TTE) is the leading-edge to leading-edge technique, which does not have a physiologic correlate, and is in contrast to CT and MRI measurements that are most commonly reported as inner-edge to inner-edge or outer-edge to outer-edge measurements.8,9 More recently, inner-edge to inner-edge measurement on TTE has been shown to have excellent agreement with CT and MRI. 10
CT is the most accurate imaging modality that is commonly used for surgical decision making and planning. The latest dual-source, photon-counting CT scanners allow image acquisition with a spatial resolution of 0.2 mm. 11 However, significant differences in aortic dimensions can result from the use of contrast, gating with electrocardiogram (ECG), as well as phase of gating. Iodinated intravenous (IV) contrast is needed to opacify the aortic lumen and delineate the inner wall of the aorta. Noncontrasted studies produce measurements that are 2 to 4 mm greater than inner-edge to inner-edge measurements on IV contrast studies, as the aortic wall is often between 1 to 2 mm in thickness (Fig. 2).

Iodinated intravenous contrast opacifies the aortic lumen and allows for easier size measurements. (a) Coronal view of a noncontrast CT scan of the chest. (b) Orthogonal reconstruction of the ascending aorta from a noncontrast CT scan. (c) Scan from panel (a) after intravenous contrast. (d) Orthogonal reconstruction of the ascending aorta from a scan with intravenous contrast. CT, computed tomography.
In the past, it was argued that measurements should be made from inner edge to inner edge, unless significant vessel wall abnormalities exist, which are more common in the descending thoracic and abdominal aorta. However, such abnormalities can occur in the ascending aorta, notably calcification. Currently, the American and European guidelines disagree on this point, with the European guidelines arguing for outer-edge to outer-edge measurements when the vessel wall is visible (Fig. 3).
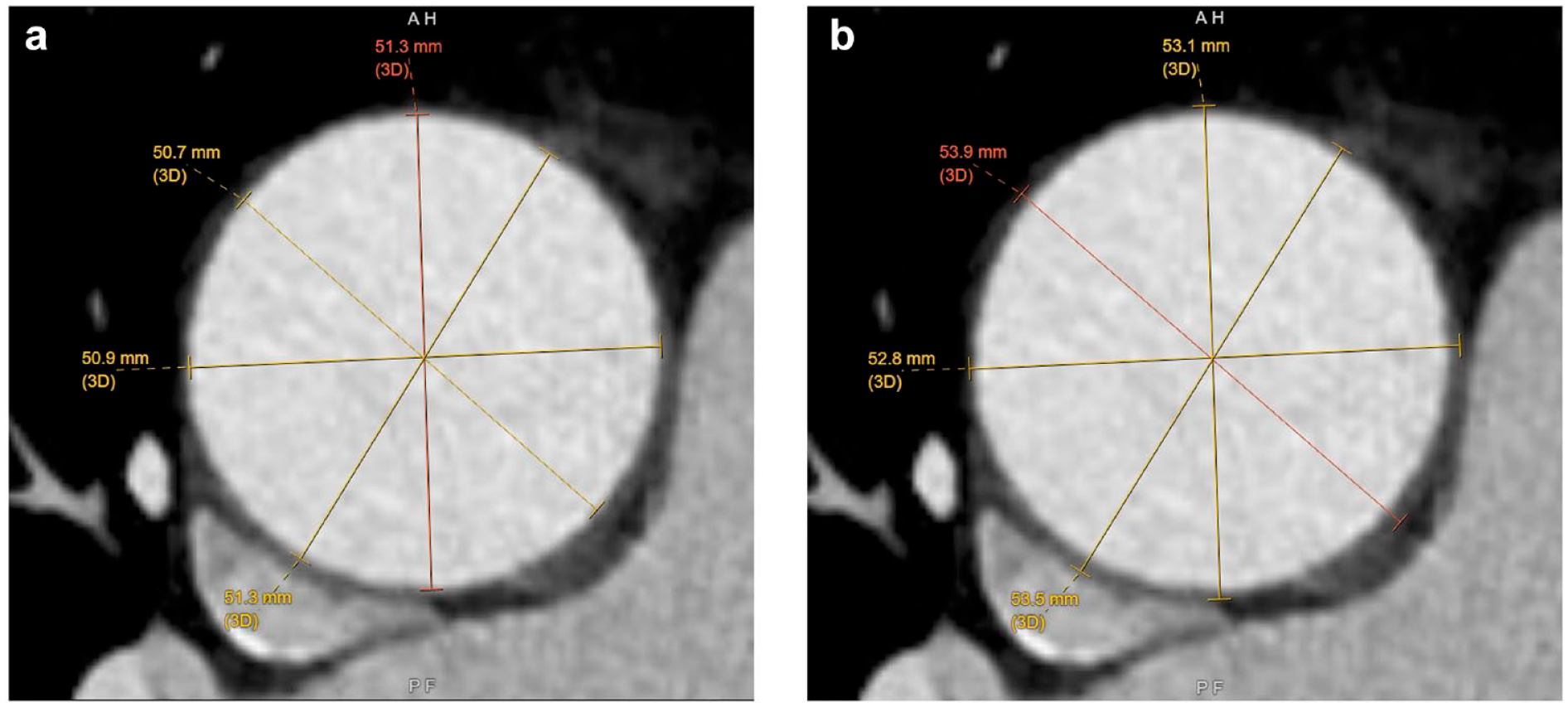
(a) Inner-edge to inner-edge versus (b) outer-edge to outer-edge measurements of an ascending aortic aneurysm.
Due to the motion of the heart throughout the cardiac cycle, CT images can suffer from motion artifact, especially close to the aortic root. ECG gating can significantly reduce such issues and is necessary for accurate measurement of the aortic root and ascending aorta (Fig. 4).12,13 The exact phase at which the images are acquired also significantly affects measurements, with differences between systole and diastole of several millimeters. 14 Systolic measurements, which lead to higher diameters, most closely reflect the physiologic state when aortic dissection or rupture occurs, namely, when wall stress exceeds wall strength. Notably, radiology standards report aortic measurements in the 70% diastolic phase and ECG-gated CT angiography (CTA) for aneurysms may not include 30% systolic gating unless specifically requested by the physician. Transcatheter aortic valve replacement (TAVR) has required annular measurements at 30% systolic phase in addition to 70% diastolic phase, to prevent incorrect valve sizing and valve embolization. Thus, our preference is to use TAVR ECG-gated protocols for aneurysms to obtain the maximum diameter of the aneurysm.
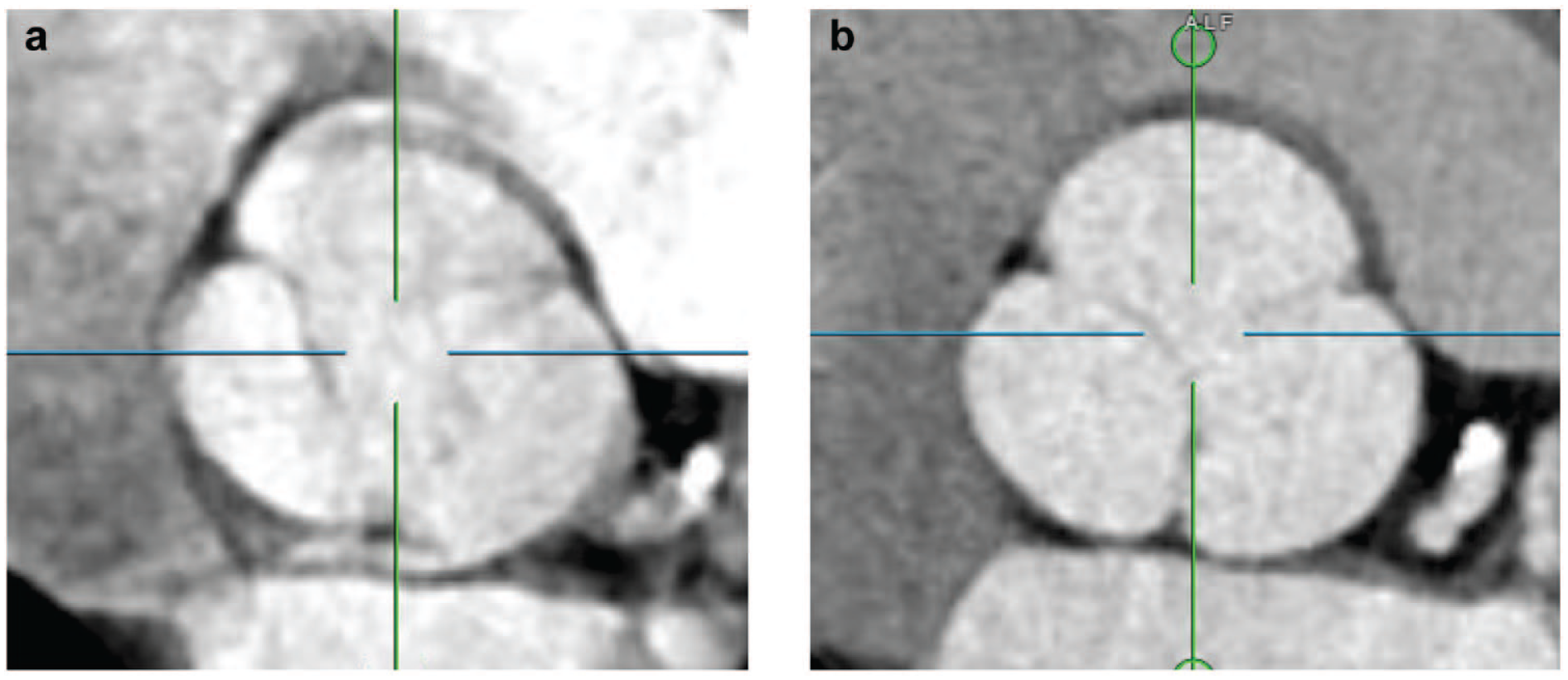
Orthogonal reconstruction of the aortic root (a) without and (b) with electrocardiogram-gating.
MRI provides 3D images similar to CT with sufficient temporal and spatial resolution to make aortic measurements without the need for radiation. Acquisition times are longer, and the resolution is inferior to that of CT. However, it provides better soft-tissue contrast that allows for visualization of the aortic wall and is thus the preferred imaging modality to characterize the aortic wall when inflammation is present. Similar to CT, ECG gating should be used for evaluation of the aortic root. Furthermore, MRI has the benefit of providing functional assessment of the ventricles and valves. Young patients with aortas below the surgical threshold benefit from MRI surveillance as they are anticipated to require a large number of surveillance scans in the future. Once surgical range is reached, we switch back to CT for accurate measurements and consistency. Disadvantages of MRI include significant noise and potential claustrophobia that patients experience, which, coupled with longer scan times and the list of MRI contraindications, often make it challenging to use for routine surveillance. However, from a research perspective, MRI has notable advantages. Cine MRI provides evaluation of wall thickness that is not clinically feasible at present with CT. DENSE-MRI provides aortic distensibility, which may be important for predicting dissection. Four-dimensional flow MRI provides 3D visualization of flow, including flow eccentricities, velocity profiles, vorticity, and helicity, as well as kinetic energy loss and wall shear stresses. Although not ready for primetime clinical applications, these modalities may provide valuable insight into the development and growth of aneurysms.
2. Make Orthogonal Measurements
Both echocardiographic images and cross-sectional images from CT and MRI are likely not orthogonal to the centerline axis of the aorta. Orthogonal images are required for accurate measurement of aortic diameter (Fig. 5).15–17
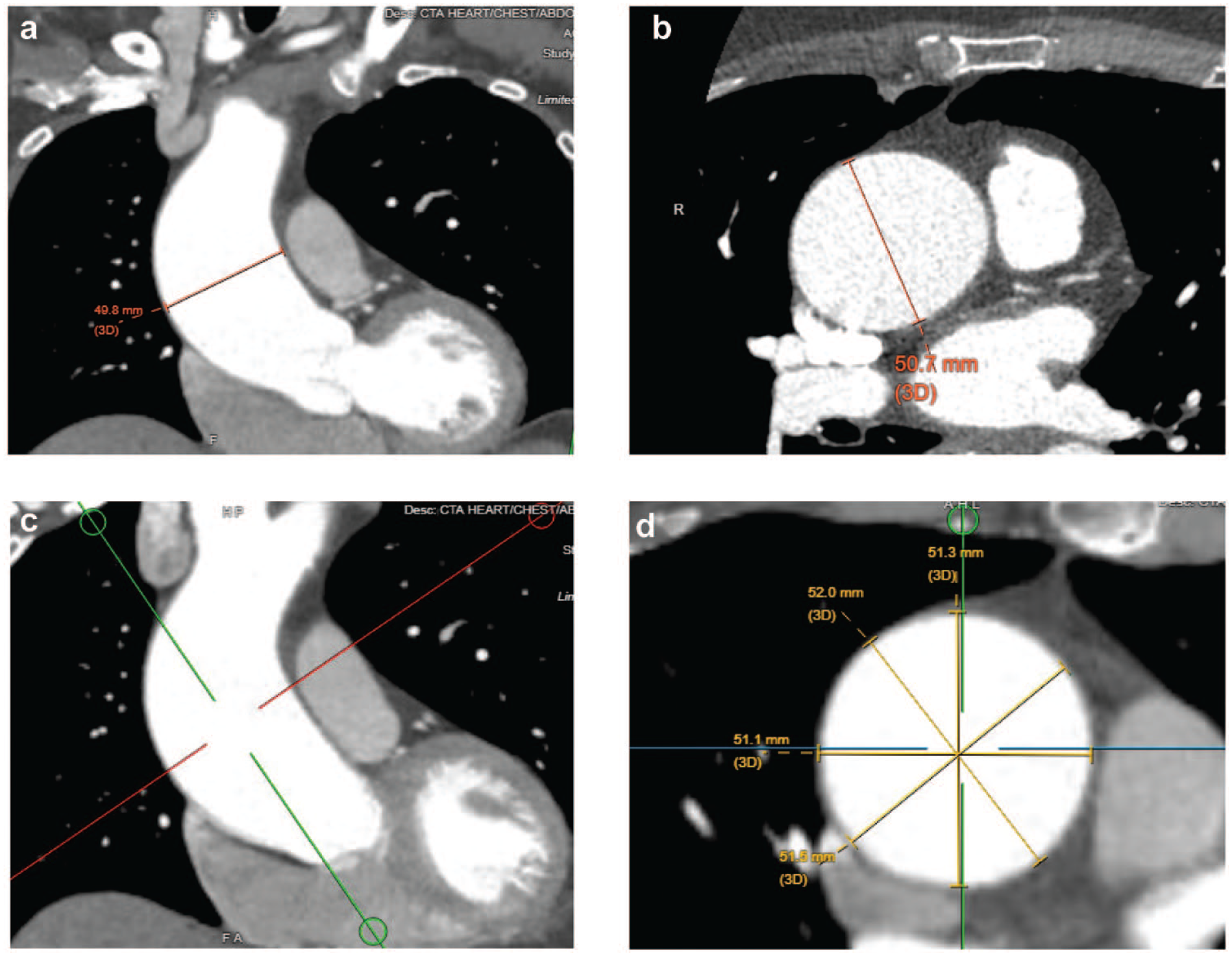
Orthogonal reconstructions allow for accurate measurement of aortic diameter. (a) Standard coronal, (b) axial, and sagittal views often lead to inaccurate aortic measurements. (c) The red line indicates the plane of orthogonal reconstruction. (d) Orthogonal reconstruction of the scan from panel (c).
Echocardiography is user dependent. In long-axis views, views off of the true mid-axis underestimate the size of the aorta, whereas in short-axis views, oblique projections make the aorta oblong and overestimate its diameter.
Similar issues exist in standard axial, coronal, and sagittal views in cross-sectional imaging. There are numerous software packages that allow for 3D centerline reconstruction and creation of orthogonal views of every segment of the aorta. These are critical for accurate measurement of size and consistency in measurements over time. Ideally, screenshots of such measurements should be included in the patient’s chart. These are extremely useful for future reference and comparisons. The aorta is rarely perfectly cylindrical, and multiple measurements should be made to determine the maximum and minimum diameter. A note should be made if inner-edge to inner-edge or outer-edge to outer-edge measurements are made, and a similar technique should be consistently applied over time to allow for consistent comparisons.
3. Make Guideline-Based Aortic Root Measurements
Measurement of the aortic root remains a challenge due to the fact that the root is not a tube but rather a cloverleaf structure (in tricuspid valves). Bicuspid aortic roots have further variability in shape that ranges from slight asymmetry of the cloverleaf shape, to pear-like shapes, to perfect ovals in true Sievers type 0 bicuspid valves. 18 How is one to measure the size of these shapes?
Historically, radiology reports have reported sinus-to-commissure measurements, which are still quite useful for TAVR. 19 However, such measurements do not have a clear biomechanical correlate and are oftentimes impossible to make in bicuspid valves. As such, the latest American and European guidelines recommend maximal sinus-to-sinus measurements, which have good correlation with TTE and MRI as well as lower interobserver and intraobserver variability.1,2 The difference between sinus-to-commissure and sinus-to-sinus measurements can be significant, upwards of 5 mm (Fig. 6).10,19,20
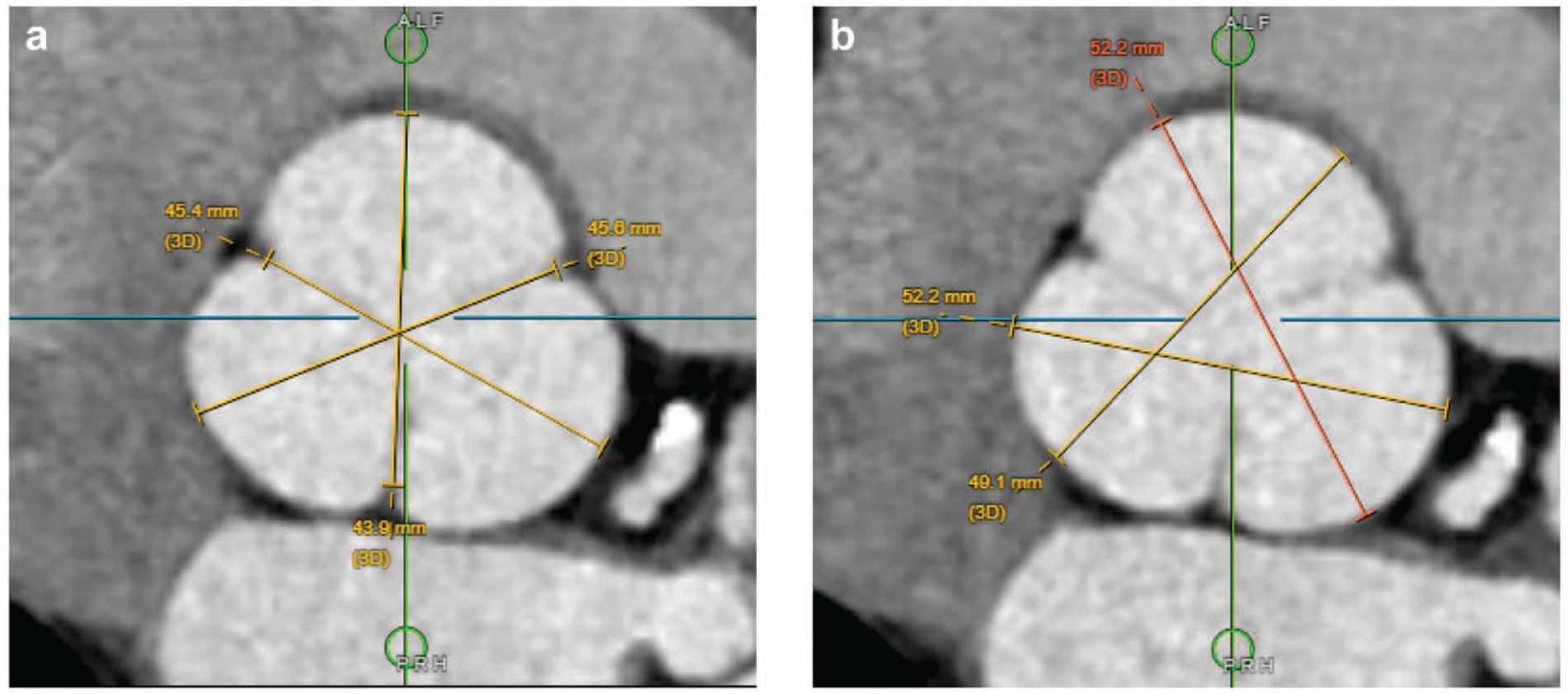
(a) Sinus-to-commissure and (b) sinus-to-sinus aortic root measurements.
4. Determine the Morphology of the Aortic Valve: Bicuspid Versus Tricuspid
Aortic disease in the context of a bicuspid aortic valve (BAV) behaves differently than tricuspid aortic valve (TAV) disease. Determination of aortic valve morphology can typically be accomplished with TTE, although extensive calcification and poor image quality remain a challenge, and misclassification is common. 21 In cases in which TTE is indeterminate, appropriate classification can be accomplished with transesophageal echocardiography, high-resolution ECG-gated CTA, or MRI, which are more sensitive for detecting BAV morphology. 22
BAV aortopathy is frequently considered in relation to valvular disease because aortic insufficiency occurs more frequently in younger patients with root aortopathy compared with older patients who more frequently have aortic stenosis. Aneurysm management can be complicated by the corresponding valvular disease because patients under surgical threshold may be offered surgery early when BAV repair can be offered for insufficiency at specialized aortic centers. Young patients with BAV aneurysm can have an undiagnosed genetic aortopathy such as Loeys-Dietz and others, which also alters the size thresholds for aneurysm management. On the other hand, older patients with aortic stenosis and concomitant aneurysms <5.5 cm face challenging decisions in which aortic guidelines suggest surgical aneurysm repair is reasonable at lower size thresholds, whereas valvular guidelines provide transcatheter options as part of shared decision making. In those settings, BAV versus TAV determination may play a pivotal role in patient management.
Historically, BAV aortopathy was thought to portend a worse prognosis, and there are still robust data that show “root” phenotype BAV aortopathy has a higher risk of AAEs.23–26 However, earlier intervention in this group has altered its natural history, and as a result, it has become more difficult to discern differences between BAV and TAV aortopathy. 27 Biomechanically, bicuspid aortas are not weaker than tricuspid ones.28,29 Furthermore, recent population-based data suggest that bicuspid aortas are less likely to dissect than tricuspid ones, but this is confounded by a higher proportion of patients with BAV aortopathy having undergone prophylactic surgery. 27
5. Determine the Full Extent of Aneurysm Proximally and Distally
The guidelines recommend measuring the aorta at standardized locations including the root, sinotubular junction, midascending aorta, zone 0 just proximal to the innominate artery, zone 1, and zone 3 just distal to the left subclavian.1,13 In addition, the location of maximum diameter should be reported if it is different from the above. A systematic approach to the measurement of the aorta allows for systematic surveillance of the aorta.
Once surgical treatment is recommended, accurate assessment of the extent of the aneurysm dictates the extent of the operation. The American guidelines suggest that it is reasonable to extend ascending aortic repair with a hemiarch replacement if the aneurysmal disease extends into the proximal aortic arch. However, the size criteria are deliberately vague. In practice, centers with aortic expertise may remove distal aortic segments >4.5 cm in BAV or TAV patients depending on patient factors and tissue quality. One might accept leaving behind a 4.6 or 4.7 cm distal ascending aneurysm in an elderly patient who may not tolerate circulatory arrest for a hemiarch. Similar considerations come into play in the aortic root, where surgeon experience with aortic valve preservation and/or repair should be considered. If a surgeon is lacking in such experience, a young patient may be better served with a residual <5.0 cm root aneurysm with a functioning native aortic valve, as opposed to a Bentall root replacement with an aortic valve prosthesis in place. Alternatively, referral to high-volume surgeons and centers should be considered in such cases.
6. Size Is Not Everything
Biomechanically, aortic dissection and/or rupture can occur when wall stress exceeds wall strength. Aortic diameter is the most commonly used proxy for the risk of AAEs, but it is far from perfect. Most dissections occur at diameters below thresholds for preventive surgery.30,31 Beyond diameter, there are a number of other measurements that have been associated with the risk of dissection and/or rupture and should be measured/calculated. 1 These include cross-sectional aortic area/height, aortic size index, aortic height index, growth rate, and aortic length.32–36 The first 3 are measures of aortic size indexed to patient size and are particularly important in patients of small stature, in whom a relatively small aorta may nevertheless be significantly aneurysmal for a given body size.
Growth rate has long been recognized as a risk factor for AAEs, with growth of ≥0.5 cm/year (or 0.3 cm/year for 2 years) being an indication for intervention in the American guidelines and ≥0.3 cm/year in the European guidelines in patients with a TAV. In BAVs, both guidelines recommend intervention if growth ≥0.3 cm/year is observed.1,2
Aneurysmal degeneration of the aorta occurs not only in the circumferential but also in the longitudinal direction. As such, aortic length has emerged as an important risk predictor for AAEs. Like orthogonal measurements, aortic length is measured using software that can analyze 3D datasets and fit a centerline in the aorta that is in the center of the true lumen and parallel to the potential flow of blood. Aortic length is defined as the centerline length from the aortic annulus to the origin of the innominate artery. Aortic length >11 cm is predictive of AAEs and has increased sensitivity compared with aortic diameter, which is specific but not sensitive. 36
7. Understand the Past and Outline the Future
With the ubiquitous use of cross-sectional imaging in modern medicine, many patients have had a number of scans by the time they come for evaluation of their aortic disease. Obtaining all relevant past scans can be time-consuming, but the effort is well worth it. Aortic aneurysms are a chronic disease and longitudinal understanding of a patient’s aorta is much more powerful than a cross-sectional one at a single time point.
It is obvious that growth rate can be better ascertained with analysis of multiple scans. Furthermore, as mentioned in the first commandment, scans can have varying quality. Sometimes the most recent scan may not be the highest quality one, and older, higher quality scans can provide valuable information. Knowledge of prior aneurysm behavior can allow for more appropriately timed surveillance, typically with reduction in the number of exams and radiation.37,38
Neither guideline document specifies precise surveillance regimens; this is a reflection of the incredible complexity of aortic disease as well as lack of sufficient evidence to allow for codifying exact surveillance schedules. Surveillance recommendations will require better growth rate and AAE data that are stratified by aneurysm morphometrics. Such data will have to be generated across multiple institutions globally with diverse demographics. As a general rule, if there are no prior scans available for a significant aneurysm, an initial short-interval follow-up scan (often 6 months) is warranted to ascertain aneurysm growth. If the aneurysm is stable, further surveillance scans can be extended to longer intervals.
8. Know the Patient
The previous 7 commandments focus heavily on understanding a patient’s aorta in detail. However, aortic care is woefully incomplete without a thorough and complete understanding of the patient as a whole.
A detailed discussion on aortic patient evaluation is beyond the scope of this article, but some factors to consider include patient age, history of hypertension, blood pressure control, other comorbidities, prior chest surgery, medications, smoking, stimulant drug use, and patient priorities. Only once these details are known can the patient’s aortic disease be placed in the correct context and an appropriate treatment plan formulated.
9. Know the Guidelines
Thorough understanding of the latest American and European guidelines on the treatment of aortic disease is a critical and minimum requirement for any clinician treating aortic patients (Fig. 7, Fig. 8).1,2 This article summarizes some of the key concepts and recommendations, but a significant portion has been left out. Beyond the guidelines, knowledge of the primary literature is very helpful in decision making, as there are many nuances that are too subtle to be captured in a guideline document. Furthermore, the field is rapidly evolving, and the guidelines are becoming more outdated with every new publication.
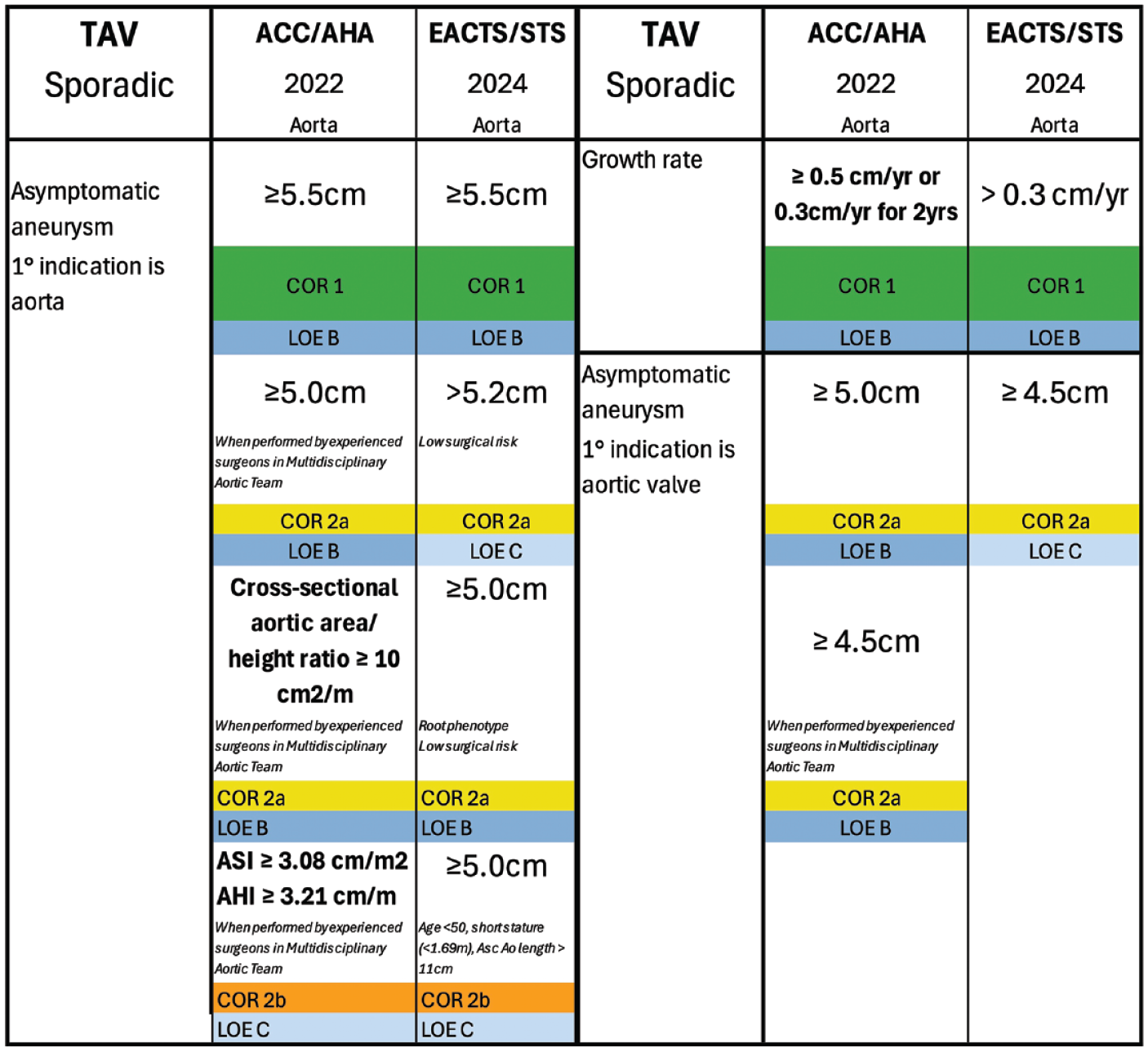
Summary of intervention recommendations for sporadic TAV root and ascending aortic aneurysms from the 2022 ACC/AHA and 2024 EACTS/STS guidelines. ACC, American College of Cardiology; AHA, American Heart Association; AHI, aortic height index; ASI, aortic size index; COR, Class of Recommendation; EACTS, European Association for Cardio-Thoracic Surgery; LOE, level of evidence; STS, Society of Thoracic Surgeons; TAV, tricuspid aortic valve.

Summary of intervention recommendations for BAV root and ascending aortic aneurysms from the 2022 ACC/AHA and 2024 EACTS/STS guidelines. ACC, American College of Cardiology; AD, aortic dissection; AHA, American Heart Association; BAV, bicuspid aortic valve; COR, Class of Recommendation; EACTS, European Association for Cardio-Thoracic Surgery; LOE, level of evidence; STS, Society of Thoracic Surgeons.
10. Know the System You Practice in and How That Affects Intervention Thresholds
Key concepts that permeate both guidelines are high-volume centers, experienced surgeons, and multidisciplinary aortic teams. Underlying these concepts is the fact that there is a robust volume to outcome relationship in aortic surgery, with an annual institutional volume of 30 to 40 cases needed to achieve an observed to expected mortality less than 1.39–41 Superimposed on this is the fact that in 2016 there were only 24 centers in the United States that performed more than 50 proximal thoracic aortic operations for aortic aneurysms annually.
A basic tenet of aortic aneurysm surgery is to intervene when the risk of surgery is lower than the risk of AAEs. Individual surgeons and centers must track and know their operative volumes and outcomes. Surgeons need to critically ascertain their skill set, especially as it pertains to root surgery, aortic valve–sparing surgery and repair, and aortic arch surgery.
Beyond the individual surgeon, the aorta is a complex organ that intersects with a number of specialties including vascular surgery, cardiology, radiology, and others, thereby necessitating multidisciplinary aortic teams for optimal care. It is critical for surgeons to understand the system within which they practice.
Conclusions
Imaging of the thoracic aorta continues to improve dramatically. As a first step, the aortic surgeon must understand the nuances of the available imaging modalities to accurately measure aortic size. Once the size and morphology of the aorta is understood, he or she can place the aorta within the context of the individual patient with their associated risk factors. Only then can a determination of both aortic and operative risk be estimated to the guide the decision of whether prophylactic surgery or surveillance has a lower risk. With the staggering advances in artificial intelligence, the great majority of steps described in the above commandments will be automated, significantly easing the workflow of the aortic surgeon and likely increasing measurement accuracy and consistency. Nevertheless, even when imaging processes become automated, it will be important to understand the underlying commandments outlined above.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.T.B. is a consultant for Edwards Lifesciences. E.E.T. is SFVA site-principal investigator for NEWTON-CABG (Amgen, Inc) and UCSF/SFVA site-PI for TITAN (Ottawa Heart Institute).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E.E.T. is supported by the Veterans Affairs Merit Award I01CX002365-01A1.