
Abstract
By sparing the sternum, the right anterior minithoracotomy (RAMT) approach may facilitate a quicker functional recovery when compared with conventional aortic valve replacement (AVR). In the following review, outcomes after RAMT AVR are compared with full sternotomy AVR. The RAMT approach is described, including suggestions for patient selection. The application of the RAMT approach for other cardiac procedures is also discussed.
Keywords
Central Message
RAMT AVR is a safe and appealing option for appropriately selected patients, with a growing number of studies demonstrating its potential advantages.
Introduction
Aortic stenosis is the most common valvular heart lesion requiring surgical management. 1 Full sternotomy (FS) is the conventional approach for aortic valve replacement (AVR) as it offers optimal exposure with low rates of morbidity and mortality. 2 However, many patients referred for AVR have a high-risk profile, and as transcatheter AVR (TAVR) continues to evolve, treatment options for these patients have expanded. 3 However, not all patients are candidates for TAVR due to anatomical constraints such as annulus size or prohibitive calcification. 4 Some of these patients may benefit from minimally invasive AVR (MIAVR). MIAVR may also be a good option for healthy patients with low surgical risk who prefer to avoid sternotomy, offering advantages over both FS AVR and TAVR. 5
Since the first report of MIAVR done by Cosgrove and Sabik in 1996 through a parasternal approach, MIAVR has been slow to gain traction.3,6 Although evidence is limited, MIAVR has been associated with less bleeding and transfusion, fewer arrhythmias, better cosmesis, shorter hospital stay, and less postoperative pain when compared with FS.6–23 Although the most common MIAVR approach is ministernotomy or upper hemisternotomy, right anterior minithoracotomy (RAMT) may be more beneficial by avoiding sternotomy altogether.6,10,14,24 Studies have also found RAMT to be a more cost-effective approach to AVR compared with sternum-based strategies.25,26
Despite evidence of safety and improved outcomes, groups have suggested that RAMT AVR is more technically challenging and is associated with a steeper learning curve.13,27 Herein, we provide a comprehensive overview of RAMT AVR. In doing so, we outline preoperative and operative considerations, including patient selection factors and appropriate investigations. We also summarize the clinical outcomes for RAMT AVR, compared with FS AVR and ministernotomy AVR. Although not the purpose of this manuscript, future clinical studies should compare MIAVR (including RAMT) and TAVR. Once a substantial body of data has been generated, systematic reviews and meta-analyses should be conducted as well on this subject matter. Given the relative paucity of data, for the purpose of this review, we will not compare RAMT AVR with TAVR.
Preoperative Imaging
Anatomical suitability for RAMT should be determined with preoperative imaging, specifically computed tomography (CT) scanning. Favorable anatomy includes an ascending aorta that is rightward or centrally positioned—a distance of less than 10 cm between the ascending aorta and the chest wall at the right second intercostal space (Fig. 1).28–32 Relative contraindications for RAMT include left-sided aorta position and aneurysm or calcification of the ascending aorta.30,31 Previous right internal mammary artery harvest (RIMA) with an in situ patent RIMA graft may also preclude RAMT AVR. Significant right pleural adhesions from previous surgery, infection, trauma, chest wall deformities, or a deep chest can also be challenging anatomy that must be carefully evaluated. 3 CT scans are also helpful to measure the aortic annulus and its distance from the skin. 33 There is also evidence suggesting that preoperative imaging can reduce the likelihood of rib fracture and dislocation, thereby decreasing the rate of postoperative bleeding and pain control. 34 Preoperative CT scans can also identify small aortic roots or other anatomical concerns that can prolong operative times and guide the modification of the MIAVR approach. 35 Although some groups suggest that preoperative imaging is not necessary for RAMT,9,13,36,37 most advocate for a preoperative CT scan that includes the peripheral vessels when peripheral cannulation is indicated. Figure 2 summarizes the key criteria we use at our center for RAMT AVR patient selection. It should be noted that these factors are only suggested and should not be considered as absolute indications or contraindications.
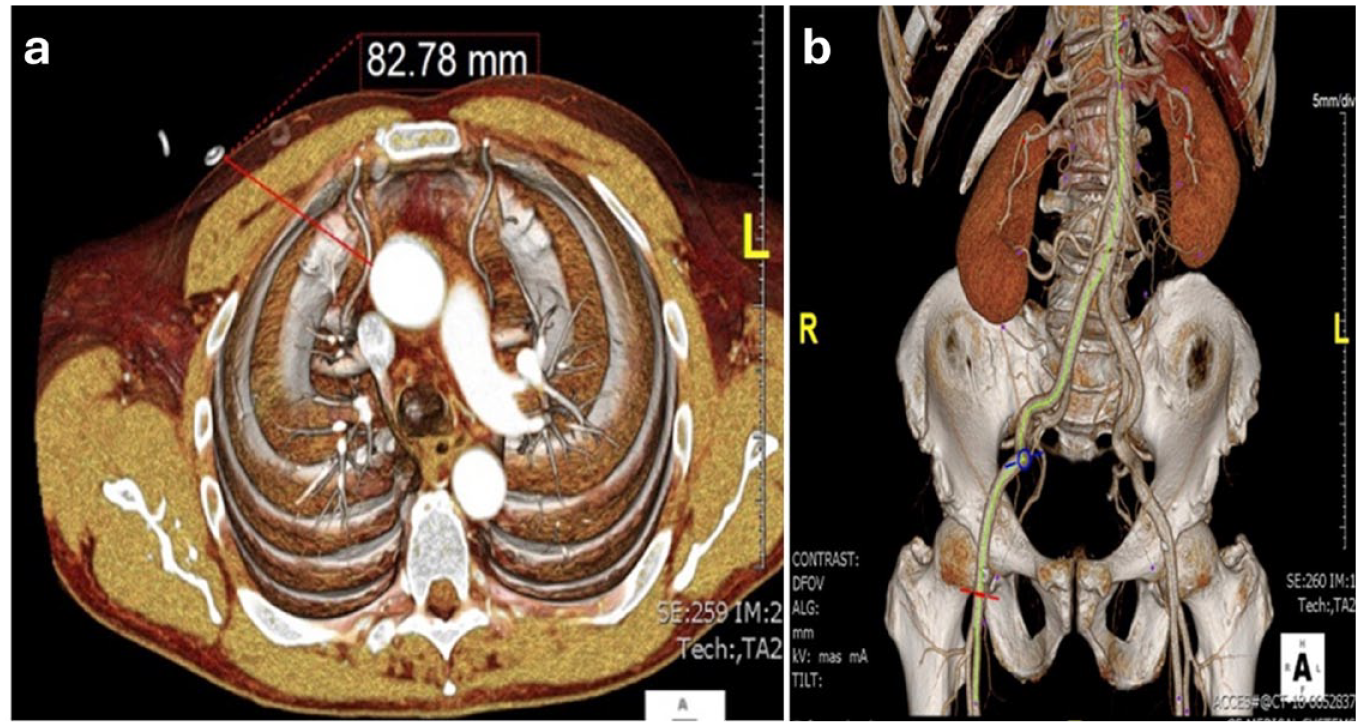
Preoperative CT scans showing anatomical features favorable for RAMT AVR. (a) Preoperative CT scan is essential for RAMT. The ascending aorta should not be displaced leftward. On axial imaging at the level of the pulmonary artery bifurcation, at least half of the aorta should be to the right of the ipsilateral sternal border. At the pulmonary artery bifurcation, the aorta should be <10 cm deep to the chest wall at the midclavicular line. (b) Cannulation is most commonly performed femorally via percutaneous puncture or a small cutdown; thus, CT images should confirm adequate size and absence of severe calcification of the femoral vessels. AVR, aortic valve replacement; CT, computed tomography; RAMT, right anterior minithoracotomy.
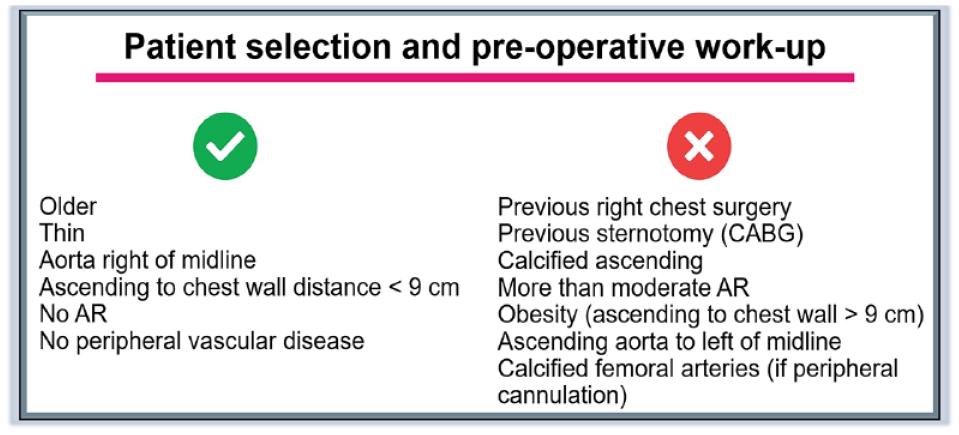
Suggested patient and anatomical factors for selecting patients for RAMT AVR. Lack of these criteria is not a contraindication to RAMT AVR but will make the approach more challenging, and familiarity with the procedure should be considered. AR, aortic regurgitation; AVR, aortic valve replacement; CABG, coronary artery bypass grafting; RAMT, right anterior minithoracotomy.
RAMT Surgical Approach
The operative approach for RAMT AVR has been previously described.3,29,31,34,36–42 Briefly, a 5 to 7 cm incision is made in the right second (generally better if direct aortic cannulation is used) or third (for a longer ascending aorta, providing better access to the aortic annulus) intercostal space. The pericardium is then opened, and traction sutures are brought through a lateral stab incision.35,36 This pulls the ascending aorta rightward and closer to the incision for improved exposure of the valve.36,37 Some surgeons place a silk suture around the tip of the right atrial appendage then out the chest wall for exposure of the proximal aorta. 43 In our view, a multi–side-port femoral venous cannula with optimal vacuum-assisted drainage achieves full decompression of the right atrium and excellent exposure for aortotomy. Some groups suggest dividing the third rib at the costochondral junction is required, with clipping of the right internal thoracic vessels.29,44,45 In our view, this is rarely needed for optimal exposure.
Cardiopulmonary bypass (CPB) is instituted through either peripheral cannulation via the femoral artery and vein with a femoral cutdown or percutaneous technique, or by central cannulation directly into the ascending aorta and right atrium. Peripheral cannulation with a cutdown is associated with risk of groin infection and lymphocele, which can be mitigated by a percutaneous or central cannulation technique. 6 The left heart can be vented through the right superior pulmonary vein or directly through the aortic valve using a small sump sucker. The ascending aorta is clamped, and antegrade cardioplegia is administered. An aortotomy is performed, and the native aortic valve is excised and replaced with a mechanical or bioprosthetic valve. Sutureless or rapid deployment valves can be used, or automated knot fasteners can help to facilitate a shorter cross-clamp. Once the aorta is sutured closed, the cross-clamp is removed, and the patient is weaned from CPB. A list of the specialized instruments that can be used to perform a RAMT AVR is provided in Figure 3.
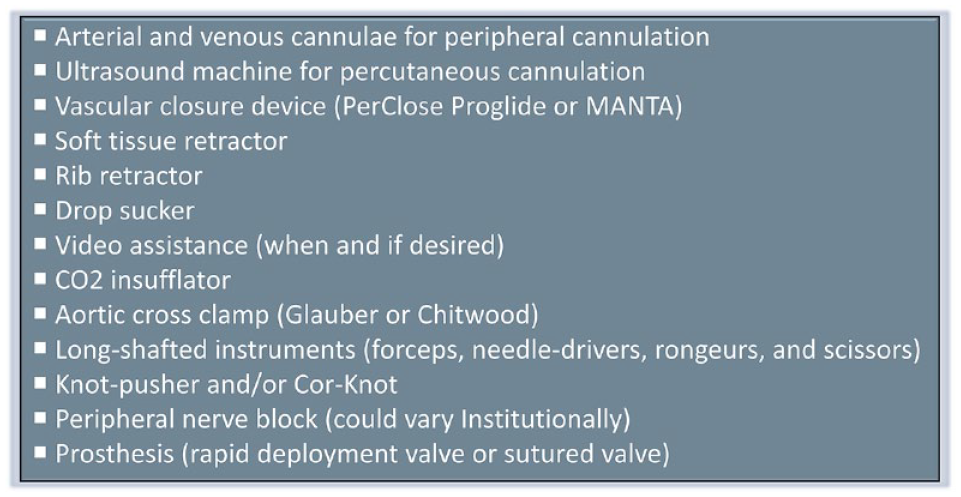
Instruments that can be used to perform a right anterior minithoracotomy aortic valve replacement.
The addition of video assistance can improve surgical vision for valve positioning and reduce the size of the thoracic incision. 40 Bakhtiary and colleagues suggest total endoscopic guidance allows a RAMT to be done in all patients, even those with suboptimal chest wall anatomy. 46 The use of 3-dimensional visualization may further facilitate this approach through enabling total endoscopic surgery, avoid the use of a rib retractor, fully visualize the aorta during cross-clamp, and allow the surgeon to more precisely perform valve replacement. On the other hand, Totsugawa et al. have shown that RAMT AVR can be safely performed in octogenarians without the use of video assistance. 47 The Supplemental Video shows a RAMT AVR done at our center.
Clinical Outcomes
It is important to critically appraise the outcomes of RAMT across different centers and throughout time. This should include metrics such as mortality, stroke, operative times, kidney failure, reoperation, bleeding, transfusions, conductive block requiring permanent pacemaker (PPM), paravalvular leak (PVL), transvalvular pressure gradient, postoperative atrial fibrillation, postsurgical infection, vascular complications, length of stay (LOS) in the intensive care unit (ICU), and length of hospital stay. It is also essential to compare the clinical outcomes of RAMT versus FS and other minimally invasive (MI) approaches for AVR. In addition to encouraging a higher rate of adoption, these assessments help determine which patients benefit most from a RAMT approach. It is imperative to interpret findings in the context of certain factors, including type of prosthesis and case volume, as they can greatly affect outcomes. It is also important to acknowledge the impact that appropriate patient selection could potentially have on clinical outcomes. Although not explicitly stated in many studies, given the relative novelty of RAMT, it is highly likely that surgeons selected patients who would be “ideal” candidates for RAMT, especially during the early stages of this operation. Their selection criteria would probably include patients with a lower comorbidity profile and patients undergoing first-time and isolated operations. It is also worth noting that a RAMT approach may have been rejected for a patient with atrial fibrillation who would benefit from a full Cox maze IV surgery. In the following section, we will first summarize the clinical outcomes of isolated RAMT. Then, we present the findings of studies that compared the outcomes of RAMT with FS AVR, followed by studies that compared RAMT with other MI approaches for AVR.
Outcomes of RAMT AVR
A growing number of studies have reported the clinical outcomes of RAMT AVR, which are summarized in Table 1.3,29,33,36,40,42,46,48–74 These studies range from single center to multicenter, include a varying number of patients, and have used different prostheses for the AVR. The studies assessed well-established clinical outcomes, including death, stroke, operative times, rate of PVL, incidence of conversion to sternotomy, emergent reopening due to bleeding, transfusion of blood products, rate of PPM implantation after RAMT AVR, and length of ICU/hospital stay. The 30-day mortality ranged from 0% to 5%, and most studies reported a mortality rate less than 1% for RAMT AVR. Regarding the study that reported 5% mortality after RAMT AVR by Fortunato Júnior et al., their group used a small sample size (N = 40), is one of the earlier studies reporting the outcomes of RAMT AVR (published in 2012), and a 5% mortality rate was also observed in their FS AVR group. 75 With respect to stroke, rates ranged from 0% to 2%, further highlighting the safety of RAMT.36,42,53,54,59,60,63,68,73 Conversion to sternotomy and early reoperation for bleeding or prosthesis failure are important metrics in MI cardiac surgery. In the studies summarized in Table 1, the conversion rate to sternotomy ranged from 0% to 5%,36,46,50,56,64,69,71,74 and the most common reasons for converting to sternotomy included inaccessibility of the aorta and bleeding. The rate of reoperation for bleeding ranged from 0% to 4%.36,49,53,56,62,64 The percentage of patients requiring transfusion of blood products postoperatively was also assessed; the rate of transfusion of blood products was generally low in those undergoing RAMT AVR, ranging from 4% to 19%. 33
Clinical Outcomes of RAMT AVR.
Abbreviations: ACC, aortic cross-clamp; AS, aortic stenosis; AVR, aortic valve replacement, BAV, bicuspid aortic valve; CPB, cardiopulmonary bypass; EF, ejection fraction; ICU, intensive care unit; IQR, interquartile range; MIAVR, minimally invasive aortic valve replacement; N/A, not applicable; PPM, permanent pacemaker; PVL, paravalvular leak; RAMT, right anterior minithoracotomy; RIMA, right internal mammary artery.
Value is reported as a median.
These studies also evaluated the need for a PPM in patients undergoing RAMT AVR. Rates of implantation of a PPM within 30 days after surgery ranged from 0% to 5.9%.46,48,51,63,64,68,73 One study reported a PPM rate of 7.6%; 61 however, this value represents 1 of only 13 patients included in the study. The degree of postoperative PVL was also assessed in some of these studies, where outcomes were reported as either PVL requiring reintervention or grade of PVL. Most of the studies highlighted in Table 1 found no significant amount of PVL.46,55,58,61,63,69,71 A few studies also determined the postoperative transvalvular pressure gradient in patients undergoing RAMT AVR, which ranged from 8.5 to 14.6 mm Hg.55,58,61,63,69,71 When interpreting findings with respect to PPM, PVL, pressure gradients, and patient-prosthesis mismatch, it is important to query whether the type and size of prosthetic used affected outcomes more or less than the RAMT surgical approach. RAMT AVR was also associated with shorter hospital LOS ranging from 5 to 7 days.36,48,53,57,63,72 In 2011, Sansone et al. reported a mean LOS of 11.6 days, but they attribute this to their selected cohort of older patients with more comorbidities. 67 Finally, the use of vascular closure devices may reduce the risk of vascular complications after peripheral decannulation in RAMT AVR. 50 Overall, these studies demonstrate that RAMT is a safe and reproducible approach to AVR with good clinical outcomes with no evidence to suggest a higher rate of postoperative complications.
RAMT AVR Versus FS AVR
Several studies have compared RAMT to conventional FS AVR and are summarized in Supplemental Table 1.6,8,11–13,15,19,21,75–92 These studies articulate the comparable safety and efficacy of the RAMT approach compared with FS, with largely equivalent perioperative and postoperative outcomes. In-hospital and 30-day mortality did not differ significantly and ranged from 0% to 4% for RAMT and from 1.4% to 5.7% for FS. In some studies, RAMT trended toward better long-term survival.21,80 There was no difference in the incidence of postoperative stroke between RAMT and FS in all studies, and femoral cannulation for RAMT was not associated with increased risk of stroke. 83 Several studies compared propensity score–matched patient pairs undergoing RAMT or FS AVR and reported no significant differences in 30-day mortality, postoperative stroke, kidney failure, or 1-year survival.6,8,11–13,15,76,79,80,82,84,86,90 Some propensity-matched studies also demonstrated that RAMT offers the added benefits of lower postoperative chest tube drainage, lower rate of blood transfusions, and shorter ventilation time, ICU stay, and hospital LOS.6,8,11,12,15,79,80,84,87,91 RAMT was also associated with 5% to 19.9% lower rates of postoperative new-onset atrial fibrillation compared with FS.6,12,15,80,87 In contrast, some studies found no difference in rates of atrial fibrillation,11,84 and 1 study by Seitz et al. reported a trend towards higher postoperative atrial fibrillation, additionally finding a longer ICU and hospital LOS after RAMT. 82 However, these trends were nonsignificant and potentially limited by power in their study of 53 propensity score–matched patient pairs. Although the RAMT approach with a groin incision carries the risk of groin complications, including infection and lymphatic fistula formation, RAMT avoids the risks of sternal wound infection and prolonged wound healing associated with FS. The groin complication risks can be mitigated using percutaneous techniques. RAMT also carries the benefit of improved postoperative rehabilitation with no need for sternal precautions.
Outcomes of RAMT compared with FS were also examined in specific populations. A study of elderly patients aged 80 years or older undergoing AVR discovered that while RAMT carries the risk of requiring conversion to FS, overall, RAMT was associated with lower rates of postoperative stroke, earlier extubation, and shorter hospital stay. 11 The study of patients with preserved ejection fraction (40% or greater) reported shorter ICU and hospital LOS and a trend toward lower 30-day mortality after RAMT. The same study examined patients with left ventricular dysfunction (ejection fraction lower than 40%) and demonstrated that outcomes including mortality and hospital LOS were largely equivalent in RAMT compared with FS. 80 In the study by Nguyen et al., operative times were not different between RAMT and FS AVR, and the authors attributed this finding to the generally higher-risk profile of the study patients. However, this finding may be limited by the low power of the study that included only 35 patient pairs and thus may have masked the true benefit of a RAMT approach in this population. The efficacy of RAMT was also demonstrated in pediatric patients with a bicuspid aortic valve requiring AVR, with no differences in ventilation times, ICU or hospital LOS, or reoperation at 5 years after RAMT compared with FS. 85 Together, these data indicate that RAMT reduces the invasiveness of AVR and provides the added benefits of shorter recovery and likely lower morbidity, while still maintaining the same efficacy and safety as FS AVR.
RAMT AVR Versus Ministernotomy AVR
As the popularity of RAMT increases, groups have sought to compare RAMT to another established MIAVR approach, the ministernotomy or hemisternotomy AVR.10,14,24,27,76,86,93–96 These findings are summarized in Supplemental Table 2. Most groups found no difference in perioperative, in-hospital, and 1-year mortality between RAMT and ministernotomy. There was also no difference in postoperative stroke, atrial fibrillation, or surgical site infection.14,24,76,86,95,96 Many of these were propensity score–matched studies that reported no significant differences in mortality after AVR.10,14,24,76,86,95 Despite the majority of these studies reporting comparable outcomes between the 2 MIAVR approaches, the study by Bonacchi et al. reported that RAMT resulted in higher noncardiac 30-day mortality, longer length of ICU and hospital stay, and worse 20-year survival than ministernotomy AVR (35.4% in RAMT compared with 42.4% in ministernotomy). 10 Some studies reported more frequent conversion to FS in RAMT compared with ministernotomy,10,96 and 1 study reported more frequent reoperation for bleeding. 96 Overall, the outcomes were otherwise comparable, and other studies demonstrated that RAMT was associated with the added benefits of lower postoperative drainage, shorter ventilation times, and lower incidence of PPM implantation and revision surgery compared with ministernotomy.14,96
Anterolateral minithoracotomy is a similar MIAVR approach to RAMT that was also compared with ministernotomy. The studies by Semsroth et al. found that anterolateral minithoracotomy had higher conversion to sternotomy, higher requirements for a second clamp time, longer operative times, and more groin complications compared with ministernotomy.86,96 These data suggest that the anterolateral approach is inferior to RAMT. In summary, outcomes after RAMT AVR are largely comparable to ministernotomy AVR, and overall, these MIAVR techniques provide a less invasive approach to AVR. Compared with ministernotomy, RAMT is associated with similar rates of mortality, stroke, atrial fibrillation, and infection. Some studies note that RAMT carries the risk of potentially higher rates of conversion to FS and reoperations for bleeding compared with ministernotomy. There remains conflicting evidence regarding adverse outcomes after AVR through the right anterolateral approach, and careful patient selection must be undertaken in these cases.
Operative Times
As noted above, operative times have often been cited as a reason for the low adoption rate of a RAMT approach for AVR. Indeed, earlier studies, as shown in meta-analyses and systematic reviews, insinuated that a major drawback to RAMT is the longer operative times due to more challenging surgical exposure.18,20,97 This is relevant and important, as longer CPB and aortic cross-clamp (ACC) times are known to be risk factors for adverse outcomes.19,27,37,57,61,76,82,93 However, more recent studies have shown that operative times can be shorter in RAMT when compared with ministernotomy.21,76 Generally, more time is spent implanting the valve with a RAMT approach, but less time is required to close the chest and obtain hemostasis compared with FS AVR. 98 Del Giglio et al. found that RAMT CPB and ACC times were shorter compared with conventional FS AVR but had overall longer operative times due to preparation of the operative field. 13 Moreover, the advent and increased popularity of rapid deployment and sutureless valves have greatly reduced operative times in MIAVR and RAMT.27,33,37,40,41,52,57–60,99–101 One report suggests that rapid deployment valves can reduce ACC time by 26 min. 52 The use of Perceval (LivaNova, London, UK) sutureless valves in a RAMT approach can reduce ACC and CPB times by 38% and 40%, respectively, when compared with other biologic stented valves. 27 Glauber et al. also found a mean reduction of 33 and 35 min in ACC and CPB times, respectively, with the Perceval valve in a 10-year experience review of RAMT AVR. 57 Other rapid deployment valves including the Edwards Intuity valve (Edwards Lifesciences, Irvine, CA, USA) have been used in the RAMT approach. 63 As presented in a recent meta-analysis and systematic review, more studies have demonstrated the impact that rapid deployment and sutureless valves have had in reducing operative times. 19 Moreover, there is evidence that RAMT operative times may be further reduced with the use of video assistance,40,46,64 or automated knotting systems, such as COR-KNOT (LSI SOLUTIONS, Victor, NY, USA). 29 Collectively, these studies provide encouraging evidence supporting the incorporation of innovative technology into RAMT to reduce operative times and deliver favorable outcomes.
Learning Curve
Given that RAMT AVR is a relatively new surgical approach, it is important to determine whether it is associated with a significant learning curve, given that this will affect its adoption and the generalizability of the results. A few studies have specifically examined how increased expertise with RAMT affects intraoperative and postoperative outcomes.53,56,82,102–105 Although it is difficult to use multicenter or registry data to accurately determine the learning curve associated with RAMT AVR, single-center studies can be used as a reasonable surrogate. In a 13-year experience study, Bethencourt and colleagues noted an improvement in intraoperative and postoperative outcomes, including significantly reduced operative times, earlier extubation, fewer blood transfusions, shorter LOS, fewer strokes, and a lower number of reoperations after the first 65 RAMT cases at their institution. 53 Stolinski et al. similarly noticed improvements over time, in which the perioperative complications rate diminished from 44.9% of the patients in the first year of adopting RAMT for AVR, to 15.6% of patients in the fourth year. 56 Seitz and colleagues found that the first 10 RAMT cases of surgeons had longer operative times, longer ICU and overall hospital LOS, and higher postoperative atrial fibrillation rates. 82 Studies done by Taylor et al. and Masuda et al. found that after 40 patients, surgeons become more comfortable with RAMT AVR, as evidenced by shorter operative times.102,103 In contrast, Murzi and colleagues did not find evidence of a learning curve in a surgeon’s initial experience with RAMT in a propensity score–matched study. Specifically, they report that a single surgeon’s first 100 RAMT AVRs were not associated with increased short-term or long-term mortality. Furthermore, they instead demonstrated superior outcomes after RAMT compared with ministernotomy in which RAMT patients had shorter ventilation times, lower rates of transfusion and postoperative atrial fibrillation, and shorter ICU and total length of hospital stay. 105
Finally, in another study, Murzi and colleagues performed an analysis of the first 300 consecutive patients who underwent sutureless valve implantation via RAMT between 2011 and 2015. 104 In that study, the learning curve was analyzed by dividing the study population into tertiles of 100 consecutive patients each. Importantly, the authors did not find any significant differences with respect to mortality, operative times, or complications between the tertiles. While their study failed to identify a trend suggesting a learning curve, some of the surgeons in the study experienced a small initial learning curve at the beginning of the experience. Specifically, 6 patients had poor alignment of the sutureless valve necessitating revision, with 1 patient requiring a sutured prosthesis. This prompted modification of the patient selection process to identify high-risk candidates prior to surgery and determine the optimal method of treatment: FS AVR, RAMT AVR, or TAVR. The authors also developed a standardized RAMT approach that includes extensive annulus decalcification and precise valve sizing and placement, leading to more consistent outcomes after RAMT AVR. 104 Overall, this study underscores the importance of continually assessing outcomes and adjusting protocols when appropriate and necessary.
In our experience, to best mitigate the challenges of a learning curve, a surgeon should be more selective when presented with candidates for RAMT AVR and avoid operating on patients with factors or anatomy that may preclude a straightforward RAMT procedure. Other considerations that may facilitate a surgeon’s initial experience with RAMT are video assistance, use of sutureless or rapid deployment valves, use of automatic knotting systems such as COR-KNOT, and percutaneous closure systems such as the Perclose ProGlide (Abbott, Chicago, IL, USA) and MANTA (Teleflex, Wayne, PA, USA) vascular closure device. Once the surgeon gains more experience and comfort with RAMT AVR, they may elect to operate on higher-risk patients or those with more challenging anatomy. Peer-to-peer teaching has been invaluable in transferring knowledge from expert to novice surgeons, while high-fidelity simulation apparatuses have been instrumental in teaching the basic concepts of RAMT. Furthermore, prior experience in conventional AVR is likely a necessity before surgeons adopt RAMT. In fact, a natural progression from standard median sternotomy would be a partial sternotomy (or hemisternotomy) AVR before attempting RAMT AVR. Although multicenter data are lacking, we believe 20 to 30 cases of RAMT AVR are needed to overcome the major technical nuances of RAMT, whereas an annual surgical volume of 50 RAMT AVR cases should be sufficient for upholding skills. At our center, residents are exposed to RAMT AVR at an early stage, usually as soon as they start. Initially, they are taught the steps for peripheral cannulation and performing a thoracotomy. Trainees have an opportunity to become familiar with MI instruments using simulation models. Once they are facile, they are entrusted with placing sutures for cardioplegia and performing the aortotomy. During their later years of training, residents have an opportunity to excise the native valve, debride the annulus from calcium, and place guiding sutures for placing rapid deployment or sutureless valves. In select cases, a trainee may have an opportunity to implant a sutured valve through a RAMT incision.
RAMT Approach for Other and Concomitant Procedures
While RAMT provides adequate exposure for AVR, surgeons have adopted this approach to safely and effectively perform other cardiac operations.106–115 These studies found that double or triple valve replacements may be done through a RAMT approach, with no increased risk of paravalvular leakage, postoperative valve migration, or valve-related death when compared with median sternotomy. However, RAMT was associated with increased procedure-related costs and operative times.106,107 Operations on the aorta with and without an AVR have also been done through a RAMT approach.108,109 In a single-center study, 10 patients underwent an elective RAMT for replacement of the ascending aorta with or without AVR, in which 2 patients required rethoracotomy for bleeding and 2 patients needed a subxiphoid pericardial drain to remove pericardial effusions. 108 In a recent study, Ji and colleagues demonstrated that RAMT can be adopted to perform a Bentall procedure. 109 This was also a single-center study that reported the outcomes of 15 patients, among whom there were no deaths perioperatively or at 6-month follow-up. The authors did emphasize that a Bentall procedure via RAMT should be considered as an option only in carefully selected patients, namely, patients with normal heart function who require no other cardiac procedures and aortic arch pathology requiring no more than a hemiarch replacement. These suggestions are in addition to the general patient selection criteria for a RAMT approach. 109 In another study, Robinson et al. demonstrated that the RAMT approach can also be used to perform annular enlargement concomitant to AVR. 111
A RAMT incision has also been used in concomitant valve and coronary artery bypass graft (CABG) surgeries. 110 Hasde and colleagues reported the outcomes of 28 consecutive patients who underwent single or combined valve surgery concomitantly with CABG of the right coronary artery (RCA). One patient underwent reoperation for bleeding. There were no instances of postoperative stroke, myocardial infarction, renal failure, or wound infection. The authors concluded that the presence of an RCA lesion is not a contraindication for the MI approach to single or combined valve surgery, and these cases can be safely and feasibly performed through a RAMT incision. RAMT can also be used to treat atrial septal defects, in which both patch closure112–114 and device deployment 115 are possible. At this time, an isolated RAMT approach is likely not feasible for performing a Cox maze IV operation. More limited iterations or versions of atrial fibrillation surgery may be conceived of for patients, but those will also likely need multiple MI incisions.
Conclusions
There is a growing number of studies showing the safety and efficacy of a RAMT approach for treating various types of cardiac diseases. Appropriate patient selection early on will mitigate the learning curve that is associated with RAMT. Moreover, there is a need for more randomized studies examining the outcomes of RAMT in comparison with ministernotomy, FS, and transcatheter approaches. Increased literature outlining the positive outcomes and experience with various approaches with preoperative and perioperative techniques can contribute to the utilization of MI techniques in cardiac surgery.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845241276876 – Supplemental material for Right Anterior Minithoracotomy Approach for Aortic Valve Replacement
Supplemental material, sj-pdf-1-inv-10.1177_15569845241276876 for Right Anterior Minithoracotomy Approach for Aortic Valve Replacement by Ali Fatehi Hassanabad, Melissa A. King, Wojtek Karolak, Aleksander Dokollari, Aizel Castejon, Dominique de Waard, Holly N. Smith, Daniel D. Holloway, Corey Adams and William D. T. Kent in Innovations
Supplemental Material
sj-pdf-2-inv-10.1177_15569845241276876 – Supplemental material for Right Anterior Minithoracotomy Approach for Aortic Valve Replacement
Supplemental material, sj-pdf-2-inv-10.1177_15569845241276876 for Right Anterior Minithoracotomy Approach for Aortic Valve Replacement by Ali Fatehi Hassanabad, Melissa A. King, Wojtek Karolak, Aleksander Dokollari, Aizel Castejon, Dominique de Waard, Holly N. Smith, Daniel D. Holloway, Corey Adams and William D. T. Kent in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.