
Abstract
Objective:
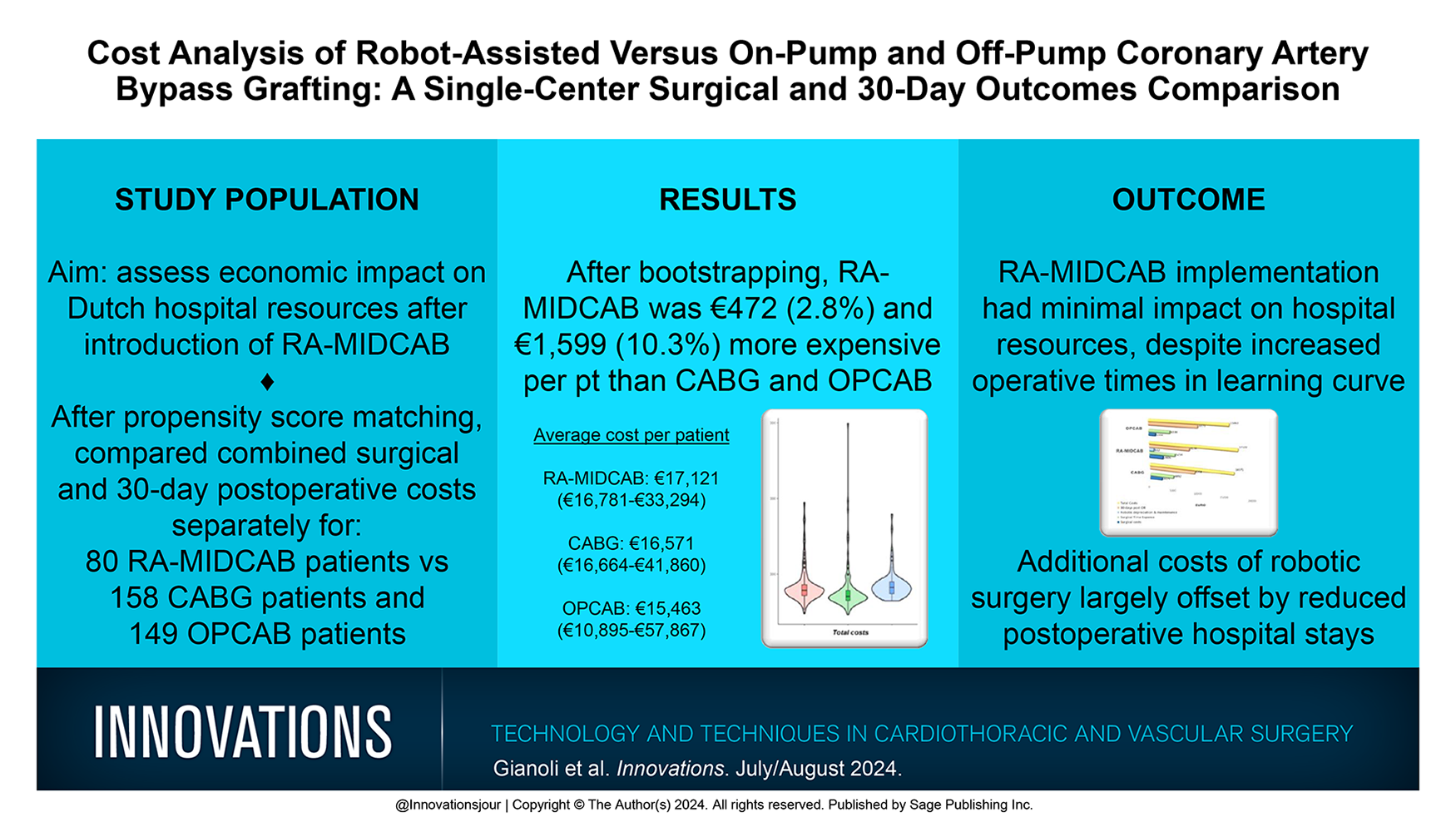
Throughout Europe, the interest in implementing robot-assisted minimally invasive direct coronary artery bypass (RA-MIDCAB) has been growing. However, concerns about additional costs have emerged concurrently. In this analysis, we aim to provide a comparison of the cumulative perioperative costs of RA-MIDCAB, on-pump coronary artery bypass grafting (CABG), and off-pump CABG (OPCAB).
Methods:
We conducted a propensity score–matched analysis comparing patients undergoing RA-MIDCAB with those undergoing CABG or OPCAB at our institution from January 2016 to December 2021. After matching, we analyzed the combined intraoperative surgical costs and 30-day postoperative costs. We first compared RA-MIDCAB costs to CABG and then to OPCAB separately. Violin plots illustrated the cost distribution among individual patients. Total cost uncertainty was estimated using 1,000 bootstrapping iterations.
Results:
Seventy-nine RA-MIDCAB patients were matched to 158 CABG patients, and 80 RA-MIDCAB patients were matched to 149 OPCAB patients. Considering both surgical and clinical outcomes, RA-MIDCAB yielded an average cost of €17,121 per patient (€16,781 to €33,294), CABG was €16,571 per patient (€16,664 to €41,860), and OPCAB was €15,463 per patient (€10,895 to €57,867). After bootstrap iterations, RA-MIDCAB was found to be €472 (2.8%) and €1,599 (10.3%) more expensive per patient than CABG and OPCAB, respectively.
Conclusions:
In The Netherlands, the adoption of RA-MIDCAB did not show a significant economic impact on hospital resources. The additional robotic costs for the surgery were almost entirely offset by the cost savings during the postoperative hospital stay. However, these comparisons may differ when considering hybrid coronary revascularization with its additional percutaneous coronary intervention costs.
Central Message
Although RA-MIDCAB incurred higher surgical expenses than open chest CABG did, it yielded 30-day postoperative economic advantages. The potential benefits for patients highlight the crucial role of improving surgical techniques, emphasizing positive outcomes despite the economic impact of the learning curve.
Introduction
Coronary artery bypass grafting (CABG) is the most effective revascularization treatment in patients with severe coronary artery disease (CAD). In Europe alone, 188,000 CABG procedures are performed on a yearly basis, which results in an estimated >2 billion in direct health care costs.1,2 In addition to having a large economic impact, CABG is associated with considerable morbidity due to the invasive character of the procedure. 2 To reduce surgical trauma, several centers in Europe have pioneered a minimally invasive program: robot-assisted minimally invasive direct coronary artery bypass surgery (RA-MIDCAB). 3 Early findings indicate that RA-MIDCAB is both safe and efficacious. 4 Nevertheless, as with all advancements, there are reservations primarily surrounding its economic feasibility in a health care landscape that emphasizes cost containment. Adopting the RA-MIDCAB procedure not only requires a dedicated surgical team but also demands substantial upfront capital investment for the robotic infrastructure and recurrent maintenance expenses. However, benefits of RA-MIDCAB, such as an earlier discharge, shorter intensive care unit (ICU) stay, and a decrease in complications, might well counterbalance its initial costs when compared with CABG and off-pump coronary artery bypass (OPCAB).5–8 By avoiding complications, RA-MIDCAB could offset the costs of robotic implementation. In Europe, no comprehensive analyses are available on the costs and the economic impact of the introduction of RA-MIDCAB. The aim of the current study is to provide a perioperative cost comparison between RA-MIDAB, CABG, and OPCAB.
Methods
Patient Population
We performed a propensity score (PS) analysis of prospectively collected data comparing consecutive patients undergoing RA-MIDCAB (n = 80) with patients undergoing CABG (n = =684) or OPCAB (n = 350) at the University Medical Center Utrecht between January 2016 and December 2021. All RA-MIDCAB and OPCAB procedures were performed by 1 surgeon, whereas CABG was performed by 8 different consultant surgeons. All patients were categorized into groups, namely, RA-MIDCAB, CABG, or OPCAB, and analyzed based on an intention-to-treat study design. Inclusion criteria for patients receiving RA-MIDCAB have been described in detail by de Jong et al. in 2023. 9 The inclusion criterion for CABG patients was a maximum of 3 distal anastomoses. CABG and OPCAB graft type choices included the left internal thoracic artery with the saphenous vein as well as total arterial revascularization. Exclusion criteria for all 3 revascularization strategies were preoperative dependency on mechanical circulatory support or ventilation or the need for concomitant procedures.
This study was approved by the ethical committee of the University Medical Center Utrecht, The Netherlands (METC protocol No. 21/623). Informed consent was waived for the retrospective use of data from patients who underwent CABG and OPCAB. Patients who underwent RA-MIDCAB prospectively provided written consent for the use of their anonymized data.
Data Collection
All financial data were extracted from the hospital’s financial registration of each individual patient, including the surgical procedural costs and further costs resulting from clinical outcomes within the first 30 days postoperatively and were collected in a database and manually verified.
Surgical Costs Related to RA-MIDCAB, CABG, and OPCAB
The cost of a surgical procedure was estimated by multiplying the cost of €22 per min for the duration of the operation based on reference prices of the Dutch guidelines on cost research in health care. 10 This rate includes the use of the operation room, anesthesiologist and surgical team, and also the sterilization costs of the surgical instruments. The specific additional surgical costs for RA-MIDCAB, CABG, and OPCAB were calculated by summing the prices of the different devices, disposables, instruments, and operative facilities used during the selected type of revascularization strategy. These costs were calculated using actual purchase prices. Surgical techniques are briefly described in Supplemental Appendix 1. The instruments and devices considered as additional costs, as well as the surgical techniques implemented, are provided in Supplemental Appendix 2.
Costs of the Clinical Course Within the First 30 Postoperative Days
The costs of the following postoperative clinical course events were included: ward and ICU admissions, reinterventions, blood transfusions, consultations, medication, imaging, laboratory tests, other diagnostics, and other costs. At our academic hospital, the ICU billing system permits a claim for a 2-day stay when a patient is discharged to the ward department after noon on the first postoperative day. The calculation of hospital stay remains consistent in this regard, meaning that discharging the patient to home or to referral hospitals after noon is considered as an additional day of stay in the claims to the health insurance companies.
Those costs were based on the Dutch guidelines on cost research in health care and the Dutch Healthcare Authority.10,11 Reimbursement prices issued by the Dutch Healthcare Authority and national reference prices of the Dutch guideline on cost research in health care were used, as outlined in the current Dutch pharmaco-economic guidance. 12
Outcomes
The primary study endpoint was the difference in total costs between RA-MIDCAB and CABG and between RA-MIDCAB and OPCAB in our hospital. These total costs were further broken down into surgical expenses and costs associated with clinical outcomes observed within 30 days postoperatively.
Statistical Analysis
We performed a PS-matched analysis to address variations among the RA-MIDCAB, CABG, and OPCAB groups. A 1:2 matching analysis was performed using a logistic regression model, incorporating 9 variables: age, sex, body mass index (BMI), diabetes mellitus, New York Heart Association class (I or II vs III or IV), preoperative acute myocardial infarction, left ventricular dysfunction (grade 1 or 2 vs 3 or 4) and multivessel disease (single vs multivessel). The PSs were constructed with logistic regression for each comparison separately with 1:1 matching of the PSs for each RA-MIDCAB patient with its closest match. We included restrictive cubic splines with 3 knots for both age and BMI to correct for any nonlinear effects. We subsequently matched the logit of predicted probabilities of the models with a nearest neighbor match procedure with a caliper of 0.2 in a random order. We aimed to match approximately 2 controls for each intervention patient. 13 The total costs and costs of subcategories of the CABG group were first compared with patients receiving RA-MIDCAB, and in a separate comparison, the OPCAB group was compared with patients receiving RA-MIDCAB. Matched samples were compared using conditional logistic regression analysis for categorical variables and conditional linear regression analysis for continuous variables. The resulting P values are reported, with a significance threshold set at P < 0.05. Violin plots were drawn to visualize the distribution of costs over individual patients. To estimate the uncertainty of the total costs, bootstrapping was performed with 1,000 iterations. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R statistical computing version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
After PS matching, we identified 158 CABG patients to serve as the comparison control group for 79 RA-MIDCAB patients. Similarly, 149 OPCAB patients were selected to compare against the 80 RA-MIDCAB patients. Table 1 provides the baseline characteristics after PS matching. Postoperative 30-day length of stay and complications are shown in Table 2.
Baseline Characteristics and Intraoperative Data of Patients Undergoing CABG Versus RA-MIDCAB, and OPCAB Versus RA-MIDCAB, After Propensity Score Matching.
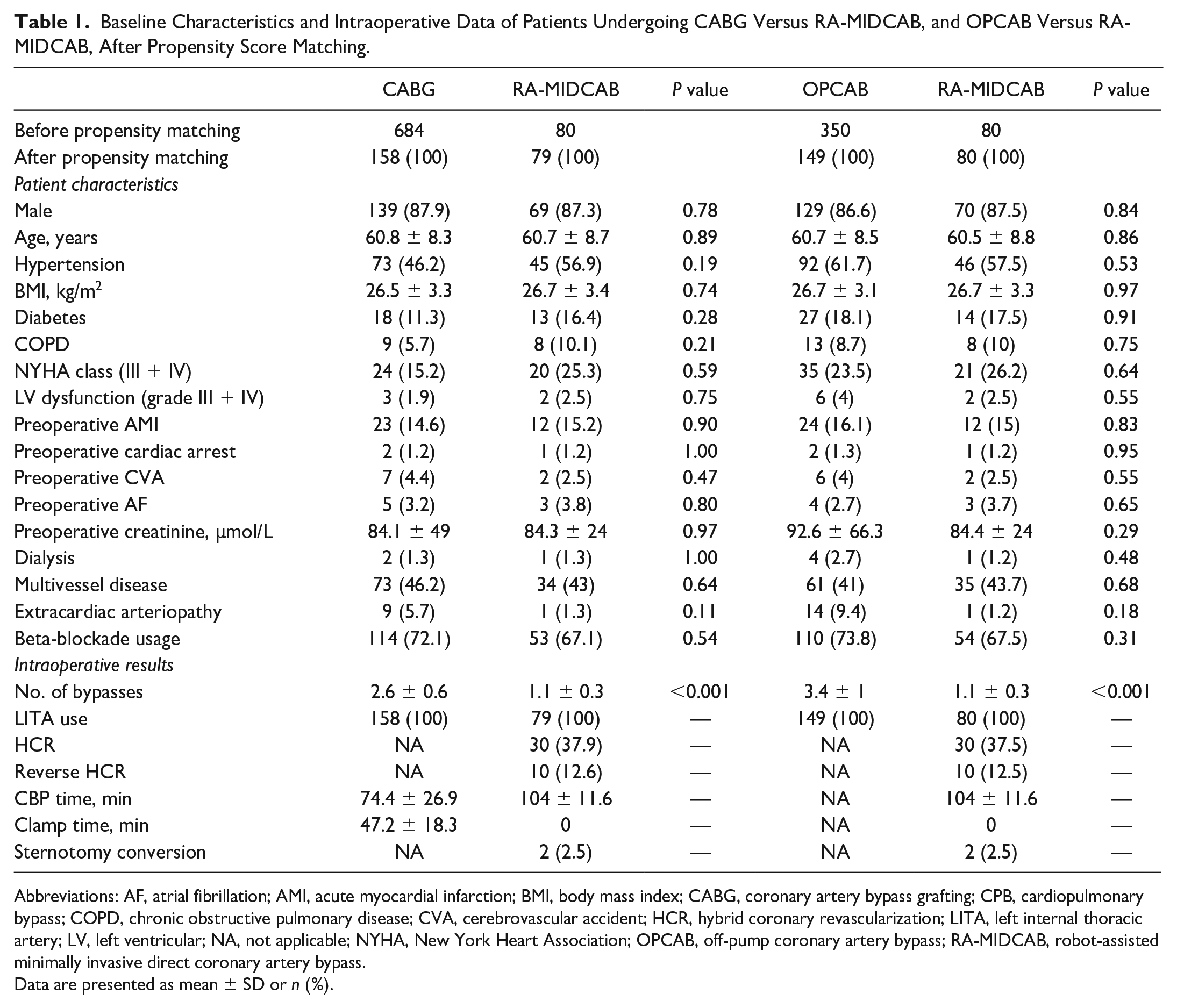
Abbreviations: AF, atrial fibrillation; AMI, acute myocardial infarction; BMI, body mass index; CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; HCR, hybrid coronary revascularization; LITA, left internal thoracic artery; LV, left ventricular; NA, not applicable; NYHA, New York Heart Association; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
Data are presented as mean ± SD or n (%).
Postoperative 30-Day Hospital Stay and Complications Among Patients Undergoing CABG Versus RA-MIDCAB and OPCAB Versus RA-MIDCAB, After Propensity Score Matching.
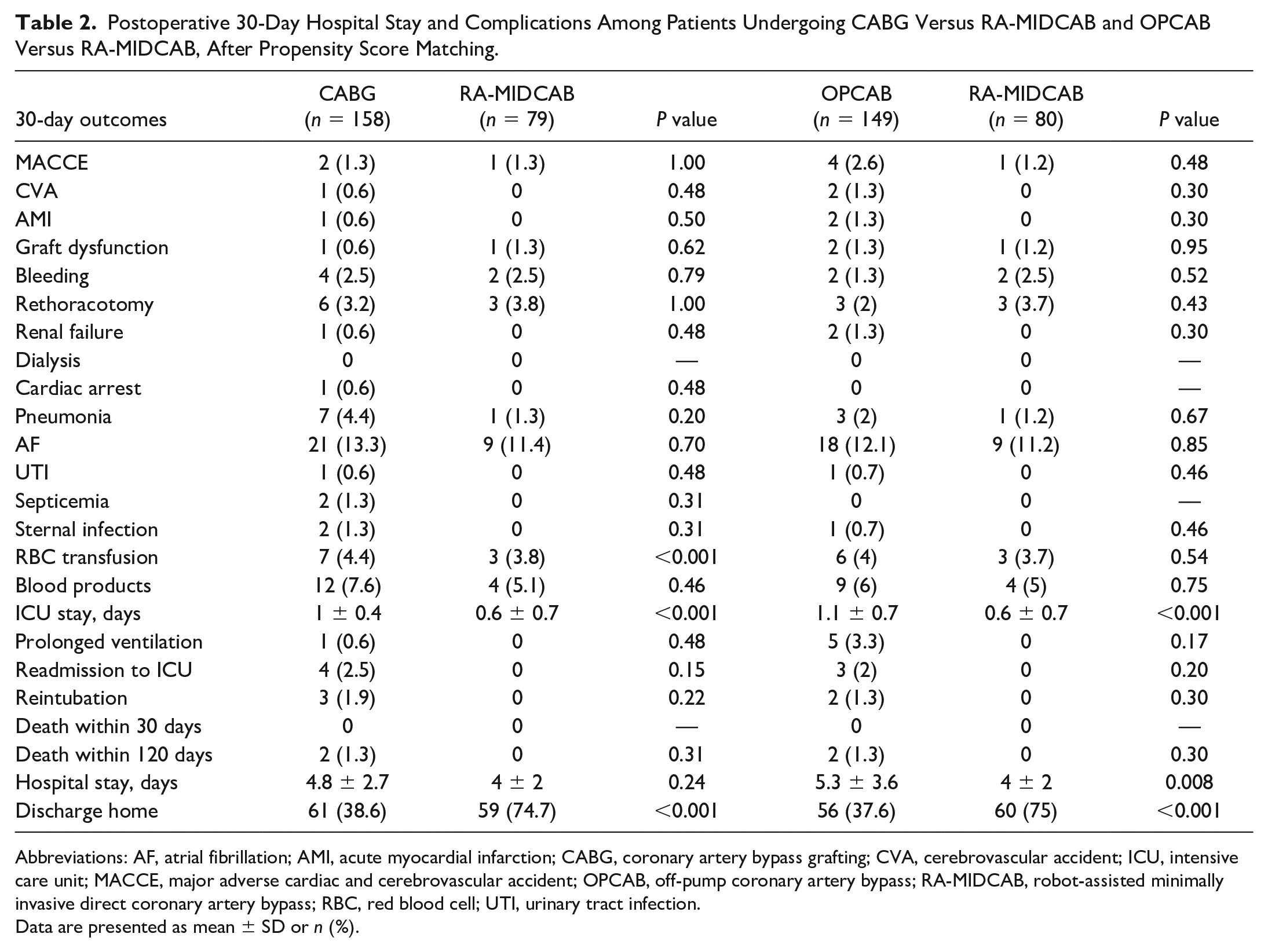
Abbreviations: AF, atrial fibrillation; AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; CVA, cerebrovascular accident; ICU, intensive care unit; MACCE, major adverse cardiac and cerebrovascular accident; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass; RBC, red blood cell; UTI, urinary tract infection.
Data are presented as mean ± SD or n (%).
Primary Outcome
In the RA-MIDCAB group, combining the costs of the surgery (accounting for operative time and robotic implementation) and the 30-day postoperative outcomes yielded an average cost of €17,121 per patient, with a range from €16,781 to €33,294. For patients undergoing CABG, the costs of the surgery (operative time) and postoperative outcomes were €16,571 per patient, ranging from €16,664 to €41,860. Through bootstrapping iterations, RA-MIDCAB displayed a mean cost increase of €472 compared with CABG, accounting for 2.8% of the total costs. After bootstrapping, 71.4% of iterations supported the cost increase in favor of CABG.
In comparison between RA-MIDCAB and OPCAB, the RA-MIDCAB group averaged a cost of €17,097 per patient (considering surgical time and robotic application combined with 30-day postoperative outcomes), with a range from €16,757 to €33,270. For OPCAB patients, the combined costs of surgery (operative time) and postoperative outcomes averaged at €15,463 per patient, with a range from €10,895 to €57,867. The bootstrapping iterations revealed that RA-MIDCAB average costs were €1,599 higher compared with OPCAB, representing a 10.3% of the total costs. After bootstrapping, 99.3% of iterations supported this increase of costs favoring OPCAB.
The total costs are presented in Figure 1, and the distribution of the cost differences after bootstrap iterations is shown in Figure 2. Surgery costs are presented in Figure 3. Detailed information on the surgical costs can be found in Supplemental Appendix 3 (Supplemental Table 1, Supplemental Table 2, Supplemental Table 3). The duration of the surgical procedure had an impact on costs, accounting for more than half of the total expenses on average. Regarding the RA-MIDCAB, our analysis encompasses the program’s inception, a phase during which our team was still within the learning curve. Consequently, this period contributed to an increase in surgical costs. However, our examination of the operative time trendline revealed a decreasing trend in procedural duration with an increasing number of procedures performed, especially after 50 procedures (Supplemental Table 4, Supplemental Fig. 1).
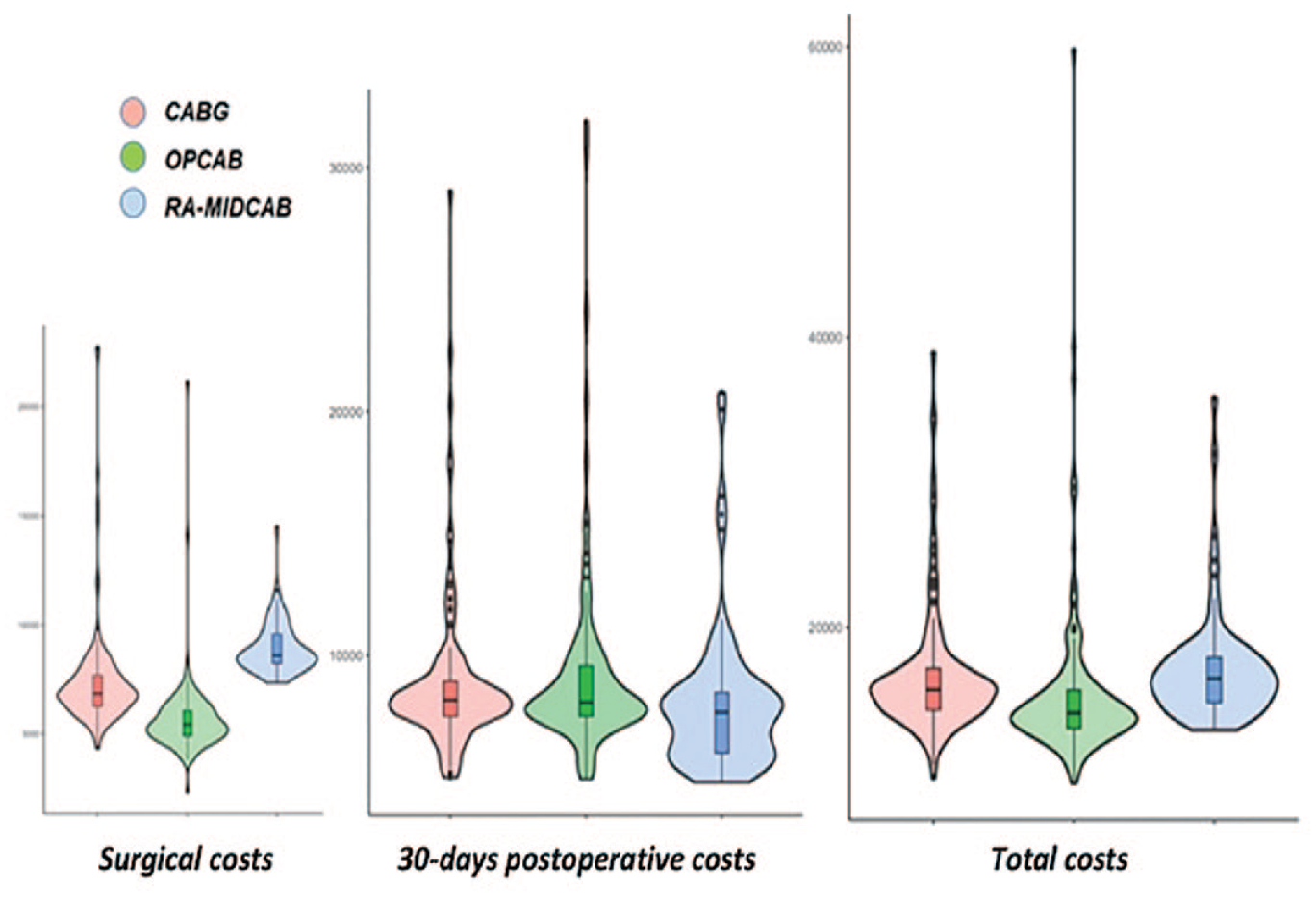
Violin plots showing the distribution of total costs for the patients who underwent RA-MIDCAB, CABG, and OPCAB with the costs on the y-axis and the width of the violin representing the number of patients at each cost level. €, Euro; CABG, coronary artery bypass grafting; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
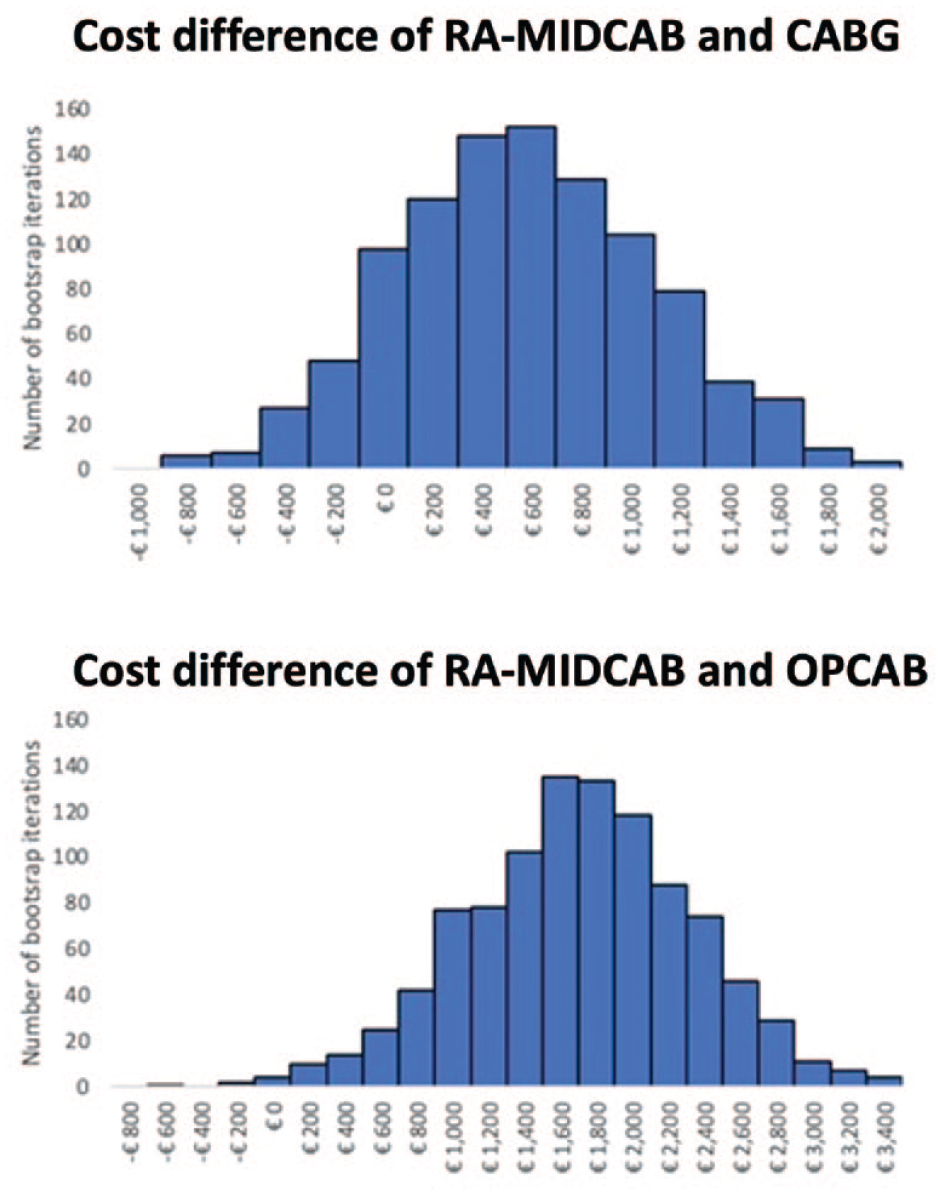
The number of bootstrapped iterations into categories of total cost difference between RA-MIDCAB and CABG and OPCAB. €, Euro; CABG, coronary artery bypass grafting; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
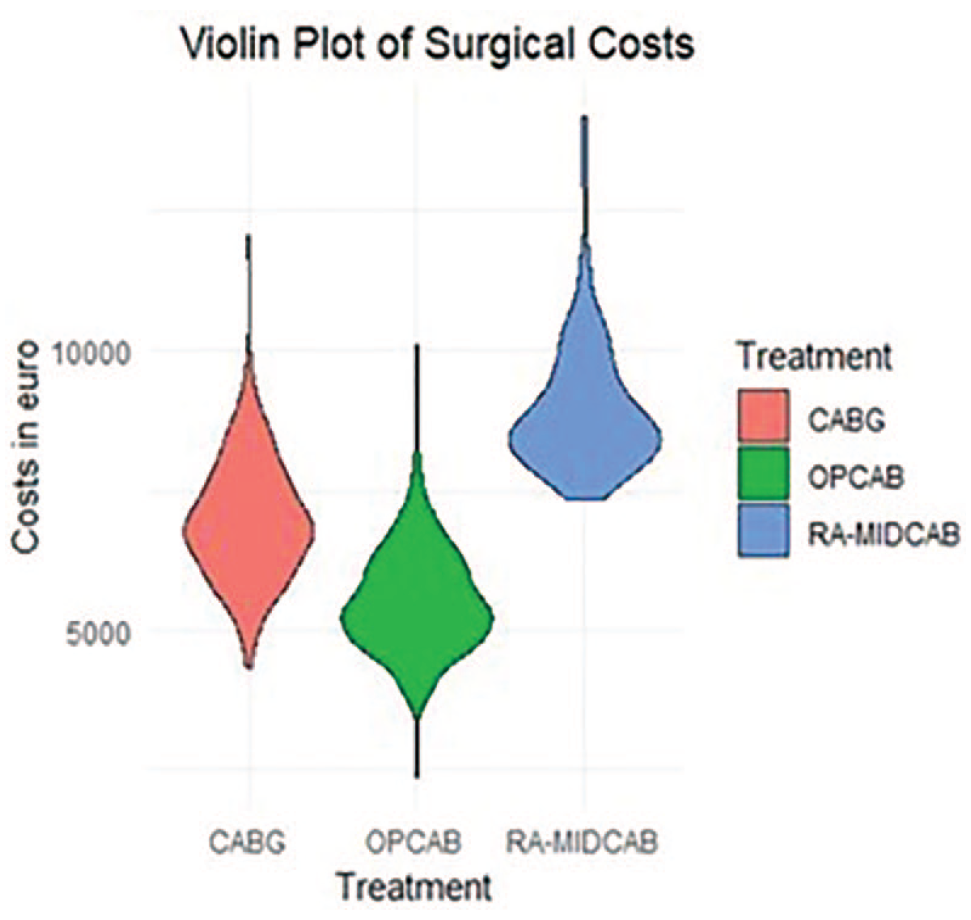
Violin plots showing the distribution of surgical costs for the patients who underwent RA-MIDCAB, CABG, and OPCAB with the costs on the y-axis and the width of the violin representing the number of patients at each cost level. Robotic depreciation and maintenance costs are excluded in this figure. €, Euro; CABG, coronary artery bypass grafting; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
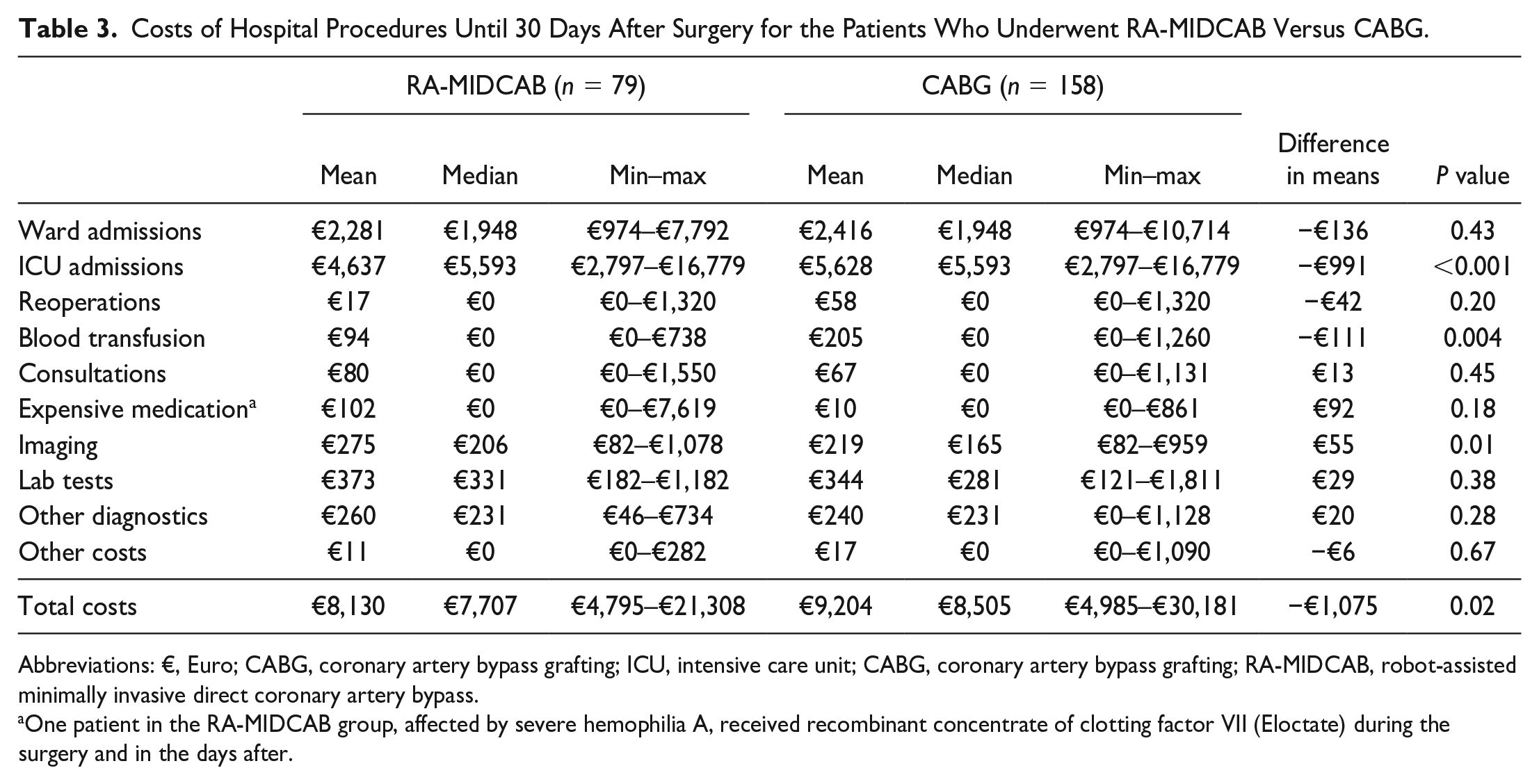
When compared with CABG, the costs of the clinical outcomes within 30 days after RA-MIDCAB were on average €1,075 cheaper per patient. Clinical outcomes and costs of the ICU admissions, reoperations, blood transfusion, and other in-hospital procedures directly related to the original procedure until 30 days after surgery are shown in Table 3. The lower postoperative costs after RA-MIDCAB were mostly the result of shorter admission time to the ICU. After RA-MIDCAB, 40.5% of patients were admitted to the ICU for only 1 day, in comparison with only 10.8% after CABG.
Costs of Hospital Procedures Until 30 Days After Surgery for the Patients Who Underwent RA-MIDCAB Versus CABG.
Abbreviations: €, Euro; CABG, coronary artery bypass grafting; ICU, intensive care unit; CABG, coronary artery bypass grafting; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
One patient in the RA-MIDCAB group, affected by severe hemophilia A, received recombinant concentrate of clotting factor VII (Eloctate) during the surgery and in the days after.
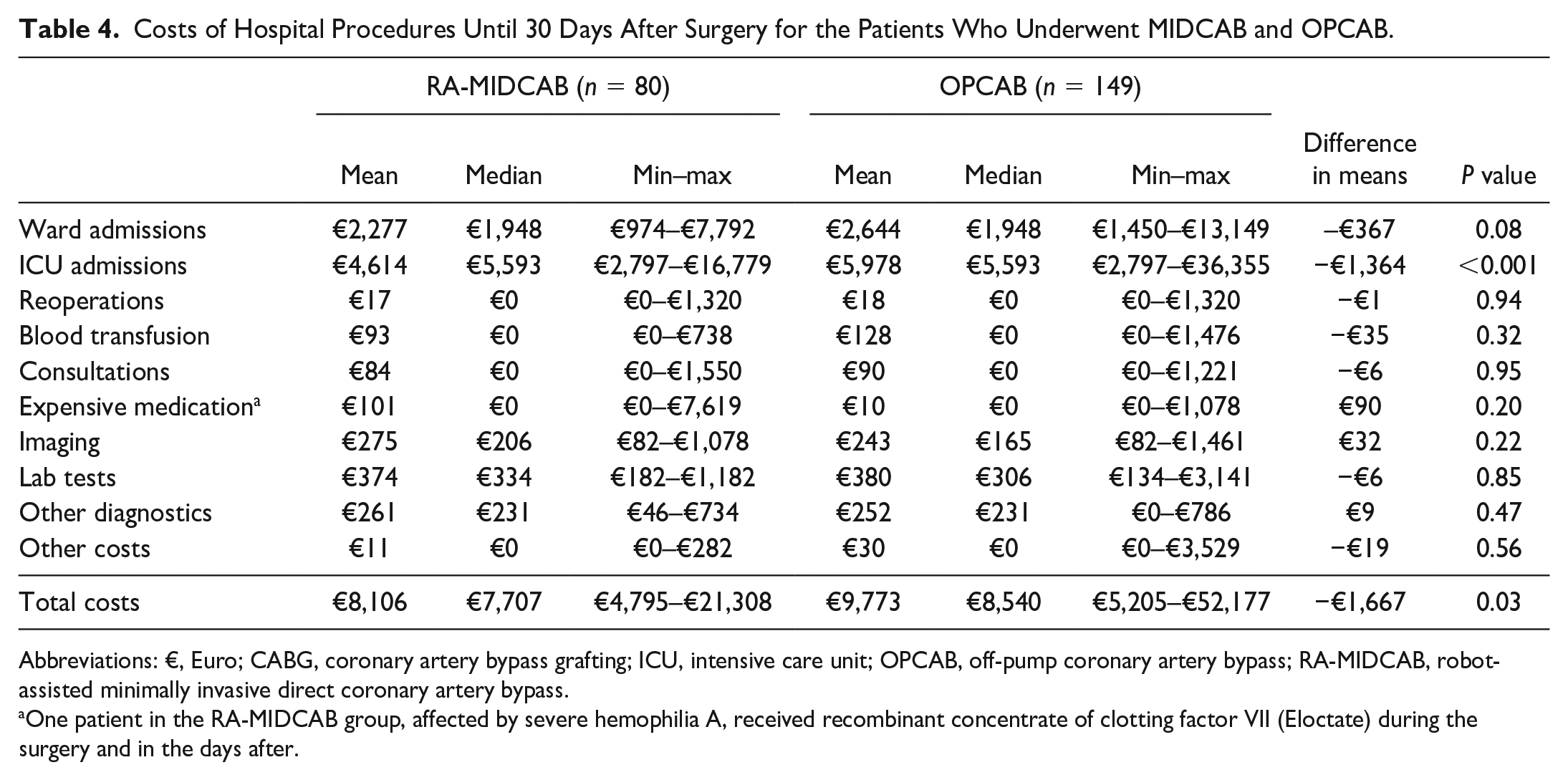
When compared with OPCAB, the costs of the clinical outcomes within 30 days after RA-MIDCAB were on average €1,667 cheaper per patient (Table 4). ICU costs were on average €1,364 cheaper after RA-MIDCAB compared with OPCAB. After RA-MIDCAB, 41.3% of the patients had 1 day ICU admission, in comparison with only 8.1% after OPCAB (Supplemental Table 5).
Costs of Hospital Procedures Until 30 Days After Surgery for the Patients Who Underwent MIDCAB and OPCAB.
Abbreviations: €, Euro; CABG, coronary artery bypass grafting; ICU, intensive care unit; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
One patient in the RA-MIDCAB group, affected by severe hemophilia A, received recombinant concentrate of clotting factor VII (Eloctate) during the surgery and in the days after.
Violin plots were used to visualize the 30-day postoperative costs (Fig. 4). RA-MIDCAB showed a larger proportion of patients with lower postoperative costs and also a smaller proportion of outliers with higher costs than patients receiving CABG or OPCAB. Furthermore, the violin plots showed less heterogeneity in the RA-MIDCAB distribution of 30-day postoperative costs when compared with CABG and OPCAB.
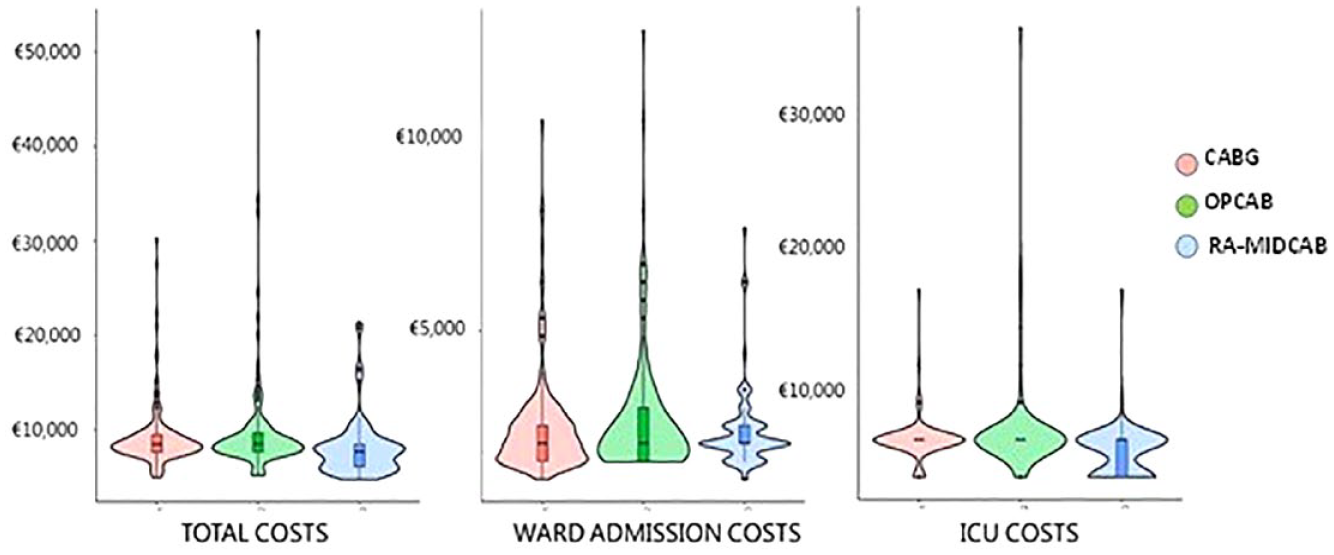
Violin plots showing the distribution of total costs, ward admission costs, and ICU costs until 30 days after surgery for the patients who underwent RA-MIDCAB, CABG, and OPCAB with the costs on the y-axis and the width of the violin representing the number of patients at each cost level. €, Euro; CABG, coronary artery bypass grafting; ICU, intensive care unit; OPCAB, off-pump coronary artery bypass; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass.
Subgroup Analysis
A subgroup analysis specifically on the hybrid coronary revascularization (HCR) group, incorporating the costs of the complementary percutaneous coronary intervention (PCI) into the postoperative outcomes cost evaluation, is provided in Supplemental Appendix 4 and Supplemental Figure 2. This analysis encompasses all PCI procedures, regardless of whether they were conducted at our institution or elsewhere. Notably, by factoring in the estimated costs of complementary PCIs, the total cost of RA-MIDCAB would have increased by €1,472 (8.9% higher) compared with CABG and by €2,599 (16.8% higher) compared with OPCAB.
Discussion
In a comparison of the surgical costs of RA-MIDCAB with CABG and OPCAB, RA-MIDCAB emerged as more expensive. However, when evaluating the postoperative costs within the initial 30 days, RA-MIDCAB proved to be more cost-effective, saving an average of €1,075 and €1,667 per patient against CABG and OPCAB, respectively. But when aggregating both surgical and clinical outcomes costs, RA-MIDCAB turned out to be more costly, €472 (2.8% higher) than CABG and €1,599 (10.3% higher) than OPCAB, as determined by bootstrap iterations.
In our assessment, the integration of robotic technology had a relatively modest impact on overall hospital expenses. In our evaluation, the incorporation of robotic technology only marginally influenced the overall hospital expenses. However, the subgroup analysis indicated a notable financial escalation for RA-MIDCAB when accounting for supplementary estimated PCI costs associated with HCR. However, it is worth noting that for HCR, both surgical revascularization and PCI are reimbursed separately by health insurance. As a result, HCR not only increases hospital procedural costs by combining 2 different treatments but also increases hospital reimbursement. This leads, as already shown by Halkos et al., to a higher net profit for hospitals in the case of HCR compared with CABG, despite the additional cost burden on the health system. 14
The findings of this study confirm that the implementation costs of robotic technology in surgery are high, and RA-MIDCAB emerges as the most expensive revascularization strategy compared with CABG and OPCAB. The significant difference in surgical costs between RA-MIDCAB and sternal spreading revascularization techniques primarily stems from the longer operation time. As with any new technology, there is a learning curve associated with its use, and a recent study reported that an average of 100 RA-MIDCAB cases is required to master the procedure. It is important to note that the population analyzed in our study was still within that learning curve. 15 However, we demonstrated a persistent decrease in surgical time as our team accumulated more experience. Ultimately, our goal is to attain outcomes comparable to those achieved by experienced centers, targeting an anticipated operation time of 3.3 h, in contrast to the average of 4 h reported in our study. 16 Such improvements would not only enhance efficiency but also lead to a significant reduction in the surgical costs associated with this technology. In our case, it would result in RA-MIDCAB becoming more cost-competitive with standard CABG or eventually offsetting the additional costs associated with HCR. Furthermore, the depreciation costs of the da Vinci robot (Intuitive Surgical, Sunnyvale, CA, USA) and its maintenance play a significant role in driving up costs. We opted to include the costs of the robotic system in our analysis due to the specific financial dynamics within our hospital setting and the Dutch health care system. It is a requirement at our hospital that departments cover the infrastructure costs associated with the robotic system, which are determined by the central administration. To determine the fee for using the robot, we calculated the total robotic expenses and divided them by the average number of procedures performed annually in the hospital. It is important to note that this fee is influenced not only by the cardiothoracic use of the robot but also by the hospital’s overall utilization of robotic technology. Although we recognize that this approach might not be standard practice in all settings, it is a financial reality that significantly affects our hospital’s budget and resource allocation decisions. Therefore, it is key to develop a hospital business plan and implementing an interdisciplinary program for robotic activity are crucial to minimize these fees and optimize the cost-effectiveness of the technology.
It is well known that hospital costs of postoperative care after CABG increase exponentially with the occurrence of complications. 8 We demonstrated that the postoperative clinical benefits of RA-MIDCAB (i.e., less complications and faster recovery), translate into postoperative economic benefits. In our analysis, the higher 30-day postoperative costs in the CABG and OPCAB groups were mostly driven by the prolonged ICU stay. Almost 85% of the patients after CABG or OPCAB were admitted to the ICU for 2 days, compared with 60% after RA-MIDCAB. Thus, more than 40% of the RA-MIDCAB group, compared with 10% for CABG and OPCAB, experienced a short ICU stay, just a few hours, allowing for a faster turnover of the ICU beds. This shorter ICU stay facilitated a quicker turnover of ICU beds, enabling the possibility of treating a second patient on the same bed within the same day. This not only maximized the utilization of ICU resources but also allowed for additional daily fees and increased our overall production. Furthermore, the higher costs after CABG and OPCAB were also related to the occurrence of complications, influencing the length of hospital admission and the need for red blood cell transfusion. Consequently, patients in the RA-MIDCAB group showed fewer bleeding complications, fewer reoperations, shorter ICU stay, and were discharged earlier from the hospital. Moreover, up to 75% of the patients undergoing RA-MIDCAB were discharged home, instead of to their referral hospital, compared with 36% and 37% of the patients undergoing CABG and OPCAB, respectively. Home discharge was not considered in our study as it did not affect hospital costs. However, it can be viewed as a cost-saving measure, providing a direct benefit to society. Also, the benefits to patients are important, as an early discharge to home allows for a quicker return to an active society and reduces the economic losses associated with extended hospital stays. Although there is a learning curve, it is encouraging to see that the clinical outcomes after RA-MIDCAB in our study align with recently published studies that reported excellent short-term outcomes after RA-MIDCAB and HCR.17–21
The introduction of innovation and new technology in our hospital positively affected public interest, resulting in economic benefits. In fact, successful implementation of the RA-MIDCAB program led to more cases involving patients with isolated proximal left anterior descending artery (LAD) disease, previously managed by cardiologists, now being referred as new patients for left internal mammary artery (LIMA) to LAD procedures. This, along with the reverse HCR population, played a crucial role in the initial growth and success of the RA-MIDCAB program.
It has been suggested that endoscopic LIMA harvesting may be a more cost-effective option compared with the robotic approach for the MIDCAB operation. 22 However, we firmly believe in the benefits associated with implementing robotics in cardiac revascularization. In fact, we consider the LIMA-LAD procedure as just the initial step for RA-MIDCAB, with its true potential lying in the exploration of using both mammary arteries for the left coronary system. By utilizing both mammary arteries, the need for additional PCIs can be reduced, further amplifying the advantages of RA-MIDCAB.
Limitations
There are some limitations in this study. First, as this study is a nonrandomized, single-center study with a relatively small sample size, there may be bias in the selection of patients, even after PS matching correction. The matching has not been performed on year of surgery, and RA-MIDCAB has generally been performed more recently than CABG and OPCAB. That might have influenced the length of stay in the ICU. Moreover, we limited this study only to our hospital costs, providing only an estimation of the PCI costs and without considering the extra hospital costs related to early discharge of patients to their referral centers and possible hospital readmissions. Further, OPCAB resulted in the highest 30-day postoperative costs and had the highest range in costs. This wide range in costs is caused by a few very high-risk patients experiencing neurologic complications and requiring prolonged ventilation and therefore a longer ICU stay. This is probably the result of a small OPCAB population with a high operative risk. Selection bias in OPCAB patients with calcified ascending aorta or terminal kidney function may also have affected the results. Finally, this study analyzed our early RA-MIDCAB experience; therefore, the learning curve and little experience might have increased the surgical costs due to initial extension of operative time and occurrence of more complications, reducing the postoperative economic benefit of the procedure.
Conclusions
In an era of financial constraints and limited resources, this study has demonstrated that implementing robotic technology for minimally invasive revascularization in The Netherlands did not impose a negative financial burden on hospital resources. While there are high costs associated with robotic implementation during the intraoperative phase, postoperative costs appear to be lower compared with traditional CABG and OPCAB procedures. However, it is important to note that these postoperative cost comparisons may not hold true when the costs of complementary PCIs for HCR are included. In addition, optimizing surgical time and awareness in the depreciation and maintenance fees of robotic technology is crucial to further enhance the cost-effectiveness of robotic procedures.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845241269312 – Supplemental material for Cost Analysis of Robot-Assisted Versus On-Pump and Off-Pump Coronary Artery Bypass Grafting: A Single-Center Surgical and 30-Day Outcomes Comparison
Supplemental material, sj-pdf-1-inv-10.1177_15569845241269312 for Cost Analysis of Robot-Assisted Versus On-Pump and Off-Pump Coronary Artery Bypass Grafting: A Single-Center Surgical and 30-Day Outcomes Comparison by Monica Gianoli, Anne R. de Jong, Pim van der Harst, Niels P. van der Kaaij, Kirolos A. Jacob and Willem J. L. Suyker in Innovations
Footnotes
Acknowledgements
We acknowledge The Healthcare Innovation Center (THINC) for their support in the field of economic statistics.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.G. is a member of the EACTS-endorsed Robotic Cardiothoracic Surgery Taskforce.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.