
Abstract
Objective:
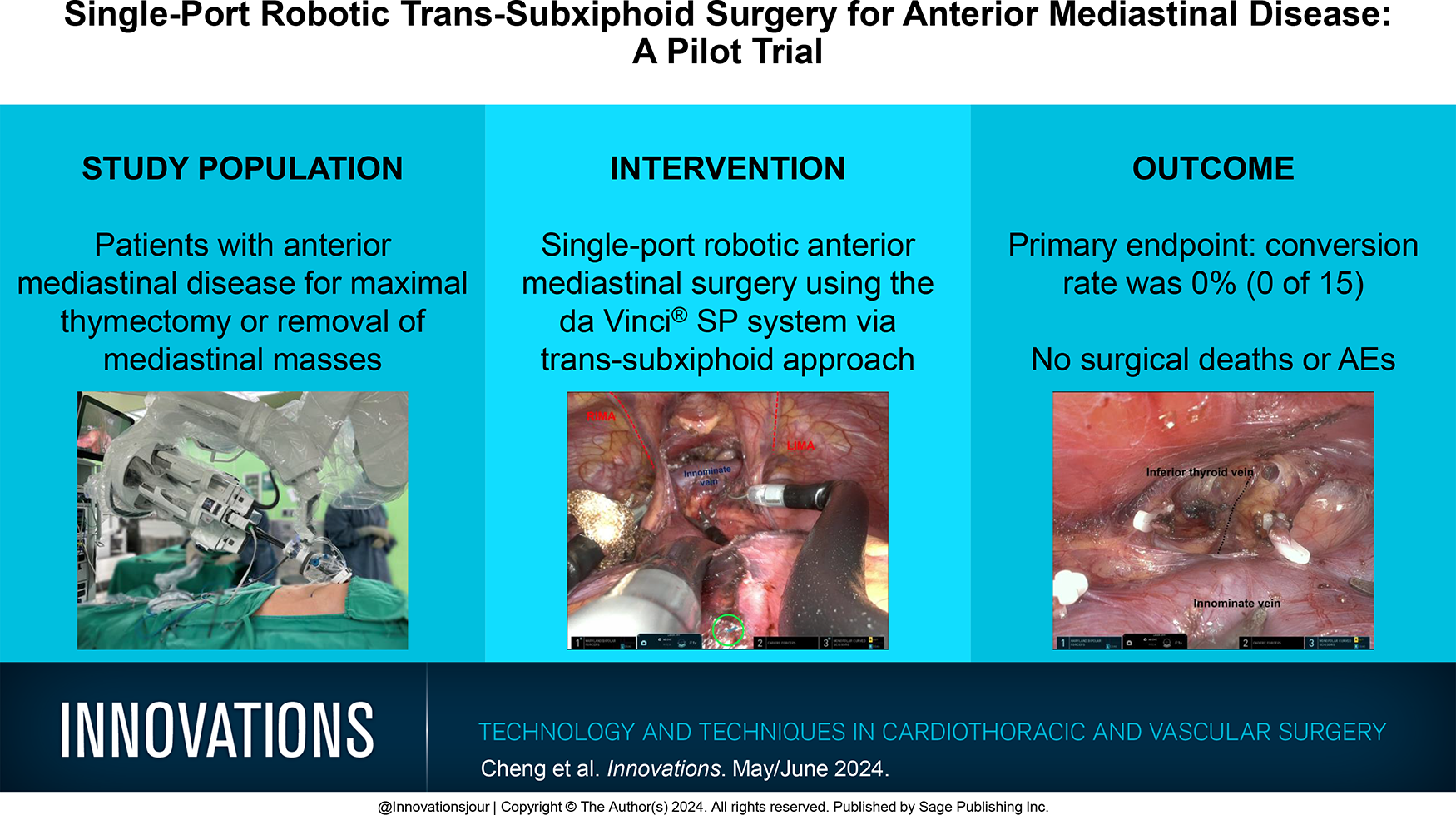
In recent years, there has been an increasing focus on minimally invasive mediastinal surgery using a trans-subxiphoid single-port thoracoscopic approach. Despite its potential advantages, the widespread adoption of this method has been hindered by the intricate surgical maneuvers required within the confined retrosternal space. Robotic surgery offers the potential to overcome the limitations inherent in the thoracoscopic technique.
Methods:
This was a clinical trial (NCT05455840) to evaluate the feasibility and safety of utilizing the da Vinci® SP system (Intuitive Surgical, Sunnyvale, CA, USA) for trans-subxiphoid single-port surgery in patients with anterior mediastinal disease. The primary endpoints encompassed conversion rates and the secondary endpoints included the occurrence of perioperative complications.
Results:
Between August 2022 and April 2023, a total of 15 patients (7 men and 8 women; median age = 56 years, interquartile range [IQR]: 49 to 65 years) underwent trans-subxiphoid robotic surgery using da Vinci SP platform for maximal thymectomy (n = 2) or removal of anterior mediastinal masses (n = 13). All surgical procedures were carried out with success, with no need for conversion to open surgery or the creation of additional ports. The median docking time was 2 min (IQR: 1 to 4 min), while the console time had a median of 152 min (IQR: 95 to 191 min). There were no postoperative complications and patients experienced a median postoperative hospital stay of 2 days with no unplanned 30-day readmission.
Conclusions:
This study shows that trans-subxiphoid single-port robotic surgery employing the da Vinci SP system in patients with anterior mediastinal disease is clinically viable with acceptable safety and short-term outcomes.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.