
Abstract
Objective:
The surgical treatment of aortic stenosis continues to evolve, and sutureless aortic valve replacement (SUAVR) is an emerging technology. With the Perceval S (Corcym, London, UK) as the only true sutureless valve on the market, the objective of this review is to analyze the current literature on Perceval S. Focusing on valve design and deployment as well as applications of the technology for challenging pathology, clinical outcomes are assessed, including a comparison with transcatheter AVR (TAVR).
Methods:
PubMed and MEDLINE were searched by 3 authors for studies analyzing SUAVR from inception to May 19, 2023.
Results:
SUAVR facilitates minimally invasive surgery and offers an alternative strategy for patients with small aortic annuli. It also has a time-saving advantage for patients who require complex operations. SUAVR results in excellent long-term morbidity, mortality, durability, and hemodynamic function. In comparison with conventional surgical AVR (SAVR), SUAVR does have a greater risk of postoperative pacemaker implantation; however, increasing user experience and refinements in implantation technique have contributed to reductions in this outcome. SUAVR results in morbidity and mortality that is similar to rapid-deployment AVR. Midterm outcomes are superior to TAVR; however, further robust investigation into all of these comparisons is ultimately necessary.
Conclusions:
SUAVR bridges the gap in technology between SAVR and TAVR. The application of this exciting technology will undoubtedly grow in the coming years, during which additional investigation is paramount to optimize preoperative planning, valve deployment, and reintervention strategies.
Keywords
Central Message
There is mounting evidence supporting the safety of the Perceval bioprosthetic valve. However, there are also data showing that Perceval should be deployed in appropriately selected patients to minimize the risk of requiring a permanent pacemaker and early structural valve deterioration.
Introduction
Affecting more than 9 million individuals globally and increasing in prevalence with age, aortic stenosis (AS) is the most prevalent valvular disorder.1–3 Definitive treatment of AS is valve replacement, and the gold standard has long been conventional surgical aortic valve replacement (SAVR) with excellent long-term outcomes. 4 By virtue of various technological innovations in transcatheter and minimally invasive techniques over the past 3 decades, therapeutic options for the treatment of AS have rapidly expanded. In recent years, randomized controlled trials have reported noninferior or improved outcomes with transcatheter aortic valve replacement (TAVR) as compared with SAVR for patients with high, intermediate, and low surgical risk.5 –10 Despite the growth of TAVR, advancements in surgical valve technology, including the development of sutureless aortic valves, are likely to maintain SAVR as the best option for many patients.
Rationale and Knowledge Gap
By avoiding suture placement, cardiopulmonary bypass (CPB) and aortic cross-clamp times can be reduced. Both increased CPB and aortic cross-clamp times are independent predictors of increased morbidity and mortality. 11 The potential benefits of efficient valve implantation have been recognized since the 1960s, when Magovern et al. first experimented with a sutureless prosthetic valve. 12 However, sutureless and rapid deployment (SURD) valves did not achieve widespread use until the past 2 decades. Three SURD valves have been brought to market. The 3F Enable (Medtronic, Dublin, Ireland), which is no longer in use; the Intuity Elite (Edwards Lifesciences, Irvine, CA, USA); and the Perceval S (Corcym, London, UK). Focusing on the Perceval S, the Perceval S Valve Pilot Trial (PILOT) and Perceval Pivotal Trial (PIVOTAL) were the initial experiences with this novel valve and deployment system.13,14 It has been the subject of considerable investigation since and has now achieved global use; however, experience remains limited to largely midterm follow-up.
Objective
The following is a review of the current literature on the Perceval S valve, with a particular focus on (1) valve design and deployment, (2) application of this technology in various pathologic conditions, and (3) clinical outcomes, including a comparison with alternative structural heart interventions.
Methods
Data Sources and Search Strategy
PubMed and MEDLINE were searched by 3 authors using the terms Perceval, sutureless aortic valve replacement, rapid deployment aortic valve replacement, SURD, SURD-AVR, aortic valve replacement, AVR, and aortic valve stenosis individually or in combination from inception to May 19, 2023. The reference lists of relevant studies were additionally screened. Three authors (N.F., R.E., A.F.H.) conducted the literature search. Details of the search strategy are available in Table 1 and Supplemental Table 1.
Search Strategy Summary.
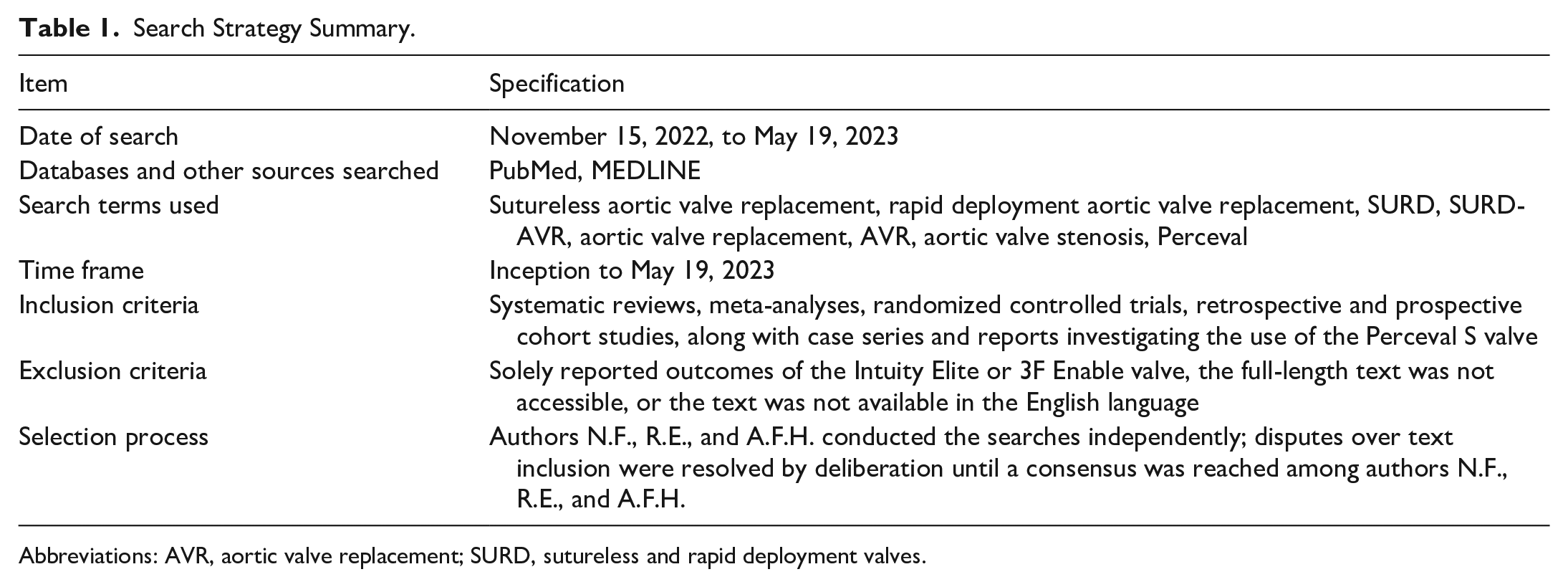
Abbreviations: AVR, aortic valve replacement; SURD, sutureless and rapid deployment valves.
Inclusion and Exclusion Criteria
Systematic reviews, meta-analyses, randomized controlled trials, and retrospective and prospective cohort studies along with case series and reports investigating the use of the Perceval S valve were considered for inclusion in this narrative review. As the focus was on Perceval S outcomes, articles were excluded if they solely reported outcomes of the Intuity Elite or 3F Enable valves. Articles were also excluded if the full-length text was not accessible or if the text was not available in the English language. Disputes over text inclusion were resolved by deliberation until a consensus was reached among the authors (N.F., R.E.A., A.F.H.).
Results
Technical Aspects
Valve design
The Perceval S valve is composed of 3 bovine pericardial cusps mounted between an inflow and outflow ring, which are designed to sit at the level of the aortic annulus and sinotubular junction (STJ), respectively (Fig. 1a). A self-expanding Nitinol cage, in addition to 9 vertical struts coated in Carbofilm, anchors the valve at these 2 anatomical junctions, providing radial force to stabilize the valve without the requirement of permanent sutures. The winged nature of vertical struts occupies the sinuses of Valsalva, further stabilizing the valve in the aortic root. As compared with conventional aortic valves with a fixed diameter, the valve’s expandable property permits sizing to the true diameter of the patient’s annulus.15,16 At present, the Perceval S is available in 4 annular sizes: small (19 to 21 mm), medium (22 to 23 mm), large (24 to 25 mm), and extra-large (27 mm).
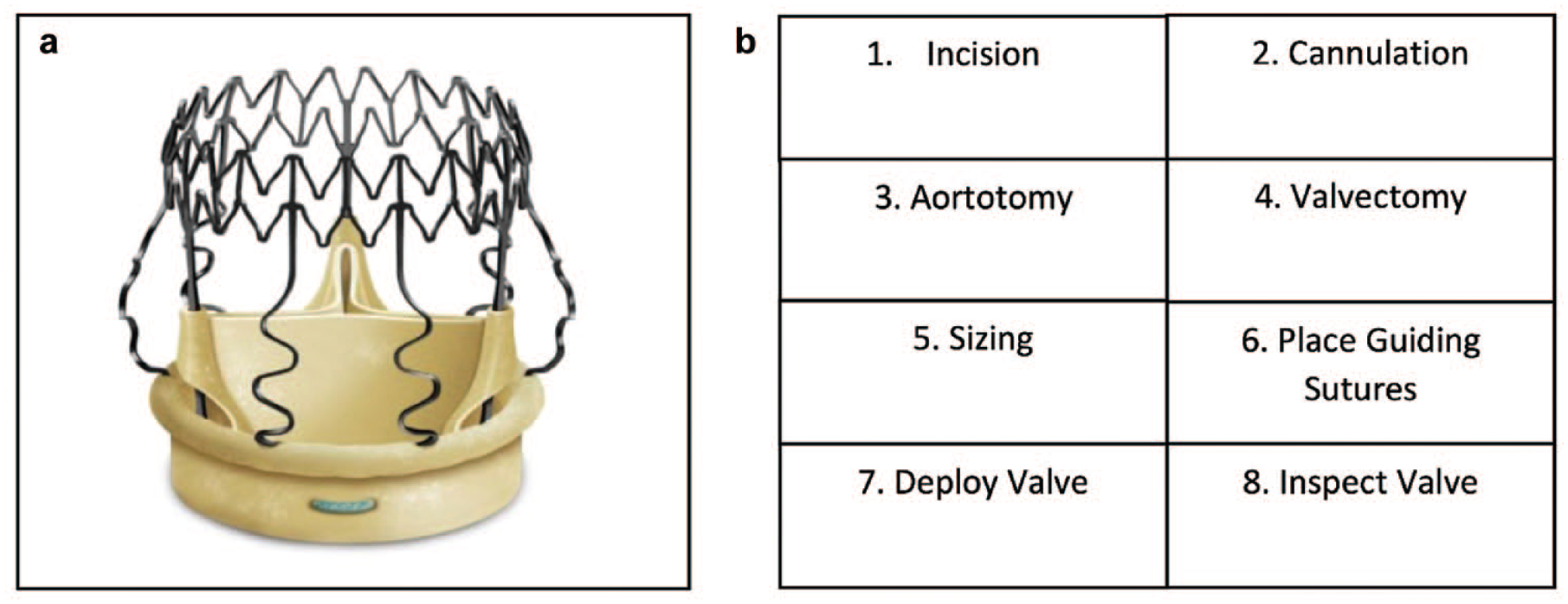
(a) The Perceval S sutureless valve (Corcym, London, UK); reproduced with permission from Corcym. (b) Perceval S valve deployment sequence.
Valve deployment
Akin to conventional SAVR, deployment of the Perceval S requires direct access and visualization of the aortic valve via a surgical incision while on CPB with the heart arrested. Surgical access can be achieved by full median sternotomy or various minimally invasive techniques. A high transverse aortotomy must be done to avoid interference with the Nitinol cage during aortotomy closure. 15 Excision of the pathologic valve, annular decalcification, and meticulous sizing are critical. An expandable prosthesis that adapts to the patient’s true annular size, the sizing strategy in Perceval S valve deployment differs from conventional sutured aortic valve prostheses. Nomogram charts are not used with the Perceval S valve. Both undersizing or oversizing of the prothesis are detrimental. Undersizing may result in central or paravalvular leak (PVL), as opposed to a conventional stented bioprosthesis, for which implantation of a larger prosthesis is the goal to avoid patient-prosthesis mismatch (PPM). Conversely, oversizing the Perceval S valve results in suboptimal expansion, elevated transvalvular pressure gradients, and the potential for PVL. 17 Specifics of the implantation technique, to avoid oversizing, have been previously described in detail.15,17 It is important to begin sizing with the smallest sizer first and to move on to a larger valve size only if there is no friction with the larger, white end of the sizer. The proper size is identified when there is resistance with the white sizer. It is imperative that the sizer be inserted perpendicularly to the annulus to prevent annular deformation and subsequent sizing inaccuracies. An additional strategy proposed in challenging cases is determining the smallest implantable size by dividing the STJ diameter by 1.3. 15 In these borderline cases, it should once again be emphasized to err on the side of undersizing to optimize valve hemodynamics and minimize the risk to conduction tissues. To ensure proper valve alignment and seating throughout deployment, guiding sutures are placed perpendicular to the aortic annulus 2 to 3 mm under each leaflet hinge point at the nadir of each sinus. Placement of traction sutures at the top of the 3 commissures can aid visualization and ultimately ease valve deployment; however, this is largely at the discretion of the surgeon and is not necessary for successful valve deployment. The valve is then lowered into position with the holder, the knob of the holder is rotated clockwise until the valve is fully deployed, and guiding sutures are then removed. Finally, the valve is inspected for 3 adequate lines of coaptation (“Mercedes star” sign). The lack of permanent sutures distinguishes the Perceval S from the 3F Enable and Intuity Elite valves, which require 1 and 3 permanent sutures for valve deployment, respectively. 16 Of note, the deployment process also does not require crimping of the valve, limiting damage to the pericardial leaflet cusps so as to retain their flexibility.18,19 The steps of valve deployment are listed in Figure 1b.
Applications and Indications
Conventional SAVR
The PILOT, PIVOTAL, and Safety and Effectiveness Study of Perceval S Valve for Extended CE Mark (CAVALIER) trials have demonstrated the safety and feasibility of sutureless aortic valve replacement (SUAVR) in conventional SAVR. The primary results of these trials are summarized in Table 2. The specific outcomes of these trials along with additional high-powered analyses will be discussed in greater detail in the “Clinical Outcomes” section of this review.
Summary of Primary Perceval S Valve Trials.
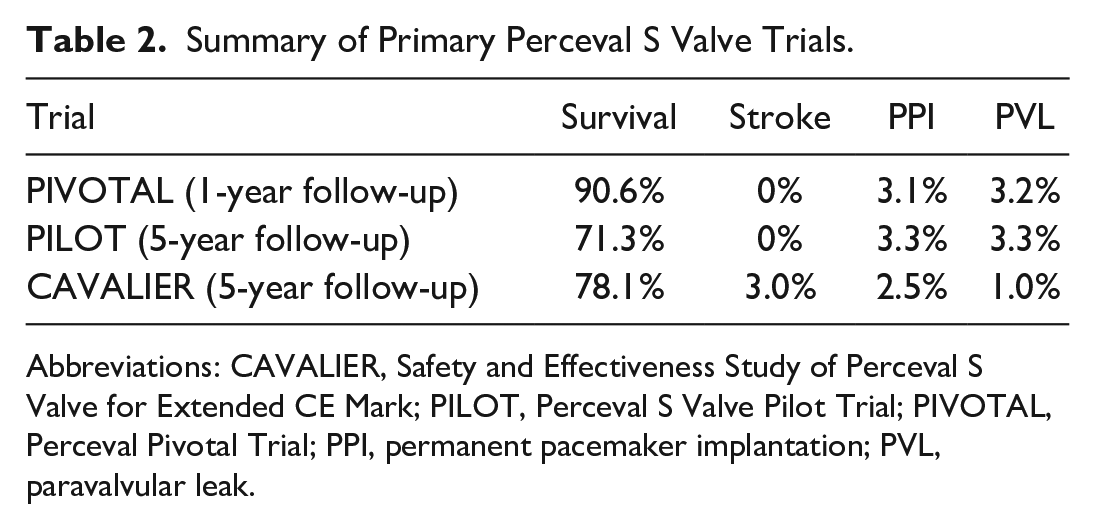
Abbreviations: CAVALIER, Safety and Effectiveness Study of Perceval S Valve for Extended CE Mark; PILOT, Perceval S Valve Pilot Trial; PIVOTAL, Perceval Pivotal Trial; PPI, permanent pacemaker implantation; PVL, paravalvular leak.
There is no doubt that this exciting valve technology has a role in standard SAVR; however, specific characteristics of the Perceval S valve lend to its application in minimally invasive aortic valve surgery.
Minimally invasive AVR
A safe, efficient, and easily reproducible technique, SUAVR facilitates minimally invasive AVR. The 2 principal minimally invasive approaches used for SUAVR deployment are ministernotomy and right anterior minithoracotomy (RAMT).
Ministernotomy
This technique involves a 5 to 8 cm incision at the upper sternum, a J-shaped sternotomy extending from the manubrium into the third or fourth intercostal space on the right, and central cannulation. 20 A subanalysis of the Perceval Sutureless Implant Versus Standard-Aortic Valve Replacement (PERSIST-AVR) trial reported significantly reduced rates of major adverse cardiac and cerebrovascular events (MACCE), stroke, atrial fibrillation, and rehospitalization following SUAVR via ministernotomy as compared with conventional sutured AVR. 21 However, this did come at the expense of an increased permanent pacemaker implantation (PPI) rate. 22 Retrospective analysis of patients undergoing SUAVR via full sternotomy versus ministernotomy indicates equivalent intraoperative time parameters, reduced hospital and intensive care unit (ICU) length of stay (LOS), as well as reduced left ventricular diastolic volume with ministernotomy. Reduced postoperative pain permitting early recovery and involvement in cardiovascular rehabilitation programs as well as reduced intraoperative myocardial handling are postulated to contribute to the observed positive cardiac remodeling with ministernotomy.23,24 Chien et al. further corroborated the feasibility and safety of SUAVR via ministernotomy. In addition, they specifically report a significant advantage with the ministernotomy approach in octogenarians, with reduced ICU LOS and a trend toward reduced hospital LOS. Such improvements in postoperative morbidity and quality of life should be targeted in this high-risk patient population. 25
RAMT
The RAMT involves a 5 cm incision lateral to the sternum into the right second intercostal space, with or without ligation of the right internal mammary artery ± displacement of the third rib at the costochondral junction, and central or femoral cannulation. 20 Rates of in-hospital mortality, stroke, myocardial infarction, PVL, and PPI following SUAVR via RAMT range from 0% to 1.5%, 0% to 2.2%, 0.8% to 1.0%, 4.1%, and 3.6% to 4.1%, respectively.26 –29 In a propensity-matched analysis of 2,257 patients undergoing SUAVR via conventional full sternotomy versus minimally invasive approaches (ministernotomy or RAMT), there was equivalent in-hospital mortality. Patients undergoing full sternotomy experienced significantly lower CPB and aortic cross-clamp times as well as increased rates of acute kidney injury (AKI) and dialysis. Adverse renal outcomes with full sternotomy are not consistent across the literature. A lack of randomization, propensity matching, or specific patient selection not adjusted by propensity matching likely underlies the discrepancy in outcomes. In a subsequent comparison of ministernotomy with RAMT, ministernotomy was associated with lower CPB and aortic cross-clamp times but increased rates of postoperative stroke, atrial fibrillation, renal failure requiring dialysis, mean valve gradient, as well as ICU and hospital LOS. 30 An additional retrospective analysis comparing the 2 minimally invasive techniques similarly indicated lower CPB and aortic cross-clamp times with ministernotomy but noted significantly lower ventilator time, ICU LOS, and hospital LOS with RAMT. Excellent midterm freedom from death, structural valve deterioration (SVD), and valve-related reoperation were noted for the overall cohort (91.5%, 96.2%, and 99.5% at 60 months). 31
Robotic
The feasibility of robot-assisted Perceval S valve deployment was initially established using cadaveric experimentation. 32 Robot-assisted AVR with the Perceval S valve involves 3 endoscopic port sites, 1 working site, and peripheral cannulation. A 12 mm camera port is placed in the right second or third intercostal space approximately 3 cm lateral to the sternum. Two 7 to 8 mm side ports are placed in the intercostal spaces above and below the camera port along the midclavicular line. The working port is located lateral to the camera site and 2.5 to 4 cm in size, permitting insertion of a soft-tissue retractor.32–35 The experience with robot-assisted Perceval S AVR has thus far been limited to case reports and series.33,35 The major challenge with the technique is the anatomical location of the aortic valve minimizing operative space secondary to its proximity to the chest wall. Robotic instruments for aortic valve surgery also lag behind their mitral valve counterparts. Despite these challenges, the ability for enhanced visualization of the aortic root and greater degrees of freedom in instrument manipulation make robot-assisted AVR particularly beneficial for patients with a deep aortic valve position.
Ultimately, the combination of minimally invasive surgery and SUAVR is safe, reproducible, offers excellent valvular hemodynamic function, and appears to enhance patient recovery. This is consistent with a contemporary meta-analysis highlighting the benefits of minimally invasive AVR, with reduced early postoperative morbidity and mortality as compared with full sternotomy. 36 Increased application of minimally invasive SUAVR, as well as further experimentation with additional techniques, is integral to the future treatment of AS. 33
Small aortic annulus
A small aortic annulus presents a unique challenge in AVR as a small prosthesis will increase the risk of PPM as well as inferior long-term myocardial remodeling and outcomes. 37 To mitigate this risk, aortic root enlargement can be done to allow implantation of a valve with a larger effective orifice area (EOA), but this comes at the cost of a longer CPB and aortic cross-clamp time. Lacking a conventional sewing ring, the Perceval valve maximizes the EOA, resulting in the implantation of a valve that better suits the patient’s body surface area for any size and can facilitate shorter CPB and aortic cross-clamp times. However, despite a significantly larger EOA, there is no difference in early or midterm mortality, mean aortic transvalvular gradient, as well as rates of redo AVR or infective endocarditis (IE) between SUAVR and SAVR at 5-year follow-up. 37 Further investigation with long-term data is required to delineate whether the significantly greater efficiency of Perceval S deployment and larger EOA translate into clinically significant improvements in valve hemodynamics and outcomes. Furthermore, the utility and benefits of shorter intraoperative time and quickened recovery should not be overlooked, with equivalent mortality outcomes in patients who are at very high risk, such as octogenarians. 25
Bicuspid aortic valve
Despite being the most common congenital heart lesion, definitive management of bicuspid aortic valve (BAV) stenosis presents a unique challenge. 38 The altered, often asymmetric, aortic root with a large, elliptic annular diameter; different commissural heights; and extensive annular calcification is a risk factor for postoperative conduction abnormalities and PVL. The presence of a BAV has historically been considered a contraindication to SUAVR. 39 However, scrutinizing BAV morphology suggests a greater risk mainly with Sievers type 0 secondary to the asymmetric commissural height, unequal width of the sinuses of Valsalva, and 180° orientation of the coronary ostia, whereas Sievers type 1 and 2 BAVs do not possess these features. 40 Early work by Nguyen et al. indicated the feasibility of SUAVR in patients with BAV stenosis. 41 A larger case series further supported this technique with low (1.4%) in-hospital mortality, PPI (5.7%), and any aortic regurgitation (9.1% overall, 6.8% mild, 2.3% moderate, no severe). However, a 2.5 times higher stroke rate than non-BAV patients undergoing SUAVR was noted and was likely secondary to the increased rate of concomitant procedures observed in the study. 40 Specific technical aspects of Perceval S implantation in high-risk patients with BAV stenosis are thoroughly described by Sa et al. 42 Ultimately, although this is a challenging patient population, the direct visualization of the aortic root during deployment and efficiency of valve implantation are advantages of SUAVR in BAV stenosis. In addition, in a condition in which concomitant procedures such as aortic hemiarch replacement are often indicated, SUAVR offers further benefit.
Concomitant procedures
As compared with isolated AVR, patients undergoing concomitant coronary, valve, or aortic procedures are at higher risk. 43 Despite the uptake of percutaneous techniques in the treatment of AS, TAVR does not permit simultaneous treatment of this additional pathology. SUAVR simplifies aortic valve implantation and consequently shortens operative, CPB, and aortic cross-clamp times, presenting a unique advantage in this patient population. A subgroup analysis of the PILOT, PIVOTAL, and CAVALIER trials reported very low short-term morbidity (PPI 5.7%, stroke 1.3%, myocardial infarction 0.8%), mortality (2.1%), and excellent 2-year hemodynamics (mean gradient preoperatively 40.6 ± 16.6 mm Hg, 2-year 9.0 ± 3.4 mm Hg) following SUAVR with concomitant procedures. 44 Several small case series also support the feasibility and safety of SUAVR with concomitant mitral or tricuspid valve surgery.45–49 Hanedan et al. lend further support for SUAVR in this patient population, reporting significantly better valvular hemodynamics and a trend toward increased survival in patients undergoing SUAVR with concomitant procedures versus SAVR with concomitant procedures. 50 Although direct comparisons to SUAVR without concomitant procedures are required, SUAVR appears to offer an advantage for high-risk patients requiring multiple cardiac procedures.
Redo cases
The management of degenerated bioprosthetic aortic valves remains difficult. The rapid rise of TAVR has resulted in an increasing proportion of bioprosthetic valve implantation and subsequent patients requiring reintervention for SVD. Valve-in-valve (ViV) TAVR as opposed to traditional redo SAVR is an option for select patients; however, this strategy does have limitations. Namely, a small aortic annulus confers inferior valve hemodynamics and early survival. 51 Melding the advantages of both the transcatheter and traditional open approach is SUAVR. Results of the Sutureless and Rapid Deployment International Registry (SURD-IR) indicate that Perceval valve deployment via minimally invasive approaches in redo AVR results in short CPB and aortic cross-clamp times as well as very low postoperative morbidity and 0% early mortality. 52 In their analysis of 22 patients, Dhanekula et al. describe 0% early mortality, low postoperative morbidity, and excellent valve hemodynamics, with a mean gradient of 12.8 ± 1.7 mm Hg at the first clinic visit following SUAVR in a redo setting. 53 Similar to the advantages of SUAVR in complex cases with concomitant procedures, the efficient, easily reproducible nature of SUAVR and maximization of EOA has great potential to benefit patients requiring reoperative AVR.
Infective endocarditis
TAVR has provided an additional therapeutic option for patients with AS at high surgical risk; however, TAVR is not suitable for patients with IE. In addition, SAVR in the setting of IE is challenging, with damaged and extremely friable tissue hindering suture placement. Both Weymann et al. and Zubarevich et al. have described their experience with Perceval S use in 9 and 13 patients with IE, respectively.54,55 Early postoperative results have been promising, with low mortality, no required PPI, and satisfactory valve hemodynamics upon discharge. However, 3-month and 6-month mortality rates of 23.1% and 46.2%, respectively, do raise some concerns, but it is important to note that these were very high-risk patients, with the majority having a history of previous cardiac surgery and requiring concomitant procedures. 54 SUAVR in patients with IE appears feasible; however, much more investigation is ultimately required prior to the more widespread adoption of this practice.
Aortic insufficiency
As opposed to the plethora of data analyzing the use of the Perceval valve in AS, there is a comparative paucity of literature on SUAVR in aortic incompetence (AI). Given that use of the Perceval S valve in this capacity is off-label, this deficiency of data is to be expected, and results on its application in this patient population are limited to small case series. These, albeit limited, analyses have demonstrated excellent technical device deployment and valve hemodynamics as well as low postoperative morbidity and mortality.56,57
Age
The optimal age range for Perceval S valve application remains unclear. Thus far, data have largely been limited to patients 75 to 80 years of age.58 –60 The 11-year results of the SURD-IR have indicated a significant increase in Perceval S utilization in patients <65 years of age over the past decade; however, currently only ~12.7% of patients receiving a SURD valve are <65 years of age. 61 The sole randomized study offering insight into the impact of age on Perceval S valve outcomes is the CAVALIER trial. Undoubtedly secondary to the increased perioperative risk profile, age ≥78 years was associated with a higher risk of cardiac death. 62 Given the inverse relationship between age and bioprosthetic valve durability, caution should be exercised in the application of this valve technology to younger patients prior to more robust investigation.
ViV TAVR following Perceval S implantation
There is very limited experience with ViV TAVR following Perceval S valve replacement. Case reports and series have noted the feasibility and safety of this intervention.63,64 The international ViV registry is thus far limited to the outcomes of 30 patients following SURD valve replacement but has demonstrated successful implantation in all cases as well as comparable hemodynamic outcomes and periprocedural morbidity and mortality as compared with ViV TAVR in patients with previous conventional AVR. 65 Higher TAVR implantation position appears to be beneficial in this patient population. 66
Clinical Outcomes
Mortality
Overall experience with the Perceval S valve indicates a 30-day mortality rate of 1.4% to 3.7%.59,61,67 –69 Previous meta-analyses note a 30-day mortality of 1.4% to 2.5%.70,71 The midterm outcomes of the CAVALIER trial indicated a 1-year, 2-year, and 5-year mortality of 8.4%, 11.5%, and 27.3%, respectively. 62 Similarly, the midterm outcomes of the Perceval Sutureless Aortic Valve Implantation trial reported 8.8% and 13.2% at 1 year and 2 years, respectively. A retrospective analysis of more than 700 patients indicated an 8.5%, 29.2%, and 72.7% mortality rate at 1, 5, and 10 years, respectively. 69 A recent meta-analysis of midterm outcomes indicates a mortality rate of 6.6%, 11.6%, 15.1%, and 21.5% at 1, 2, 3, and 5 years, respectively. 71
Stroke
Overall rates of stroke range from 0.5% to 6%.60,61,67,69,72,73 The midterm outcomes of 2 clinical trials report a 1.8% to 2.4% rate of stroke within 30 days and 94% freedom from stroke at 5 years.59,62 Meta-analyses of studies reporting long-term outcomes report 2.1% to 2.7% and 4.4% to 4.8% rates of 30-day and 5-year stroke, respectively.70,71 Of note, the rate of stroke has improved by ~75% over the past decade. 61
PPI
The high rate of postoperative conduction abnormalities necessitating PPI was one of the principal initial concerns with SUAVR. Among high-powered studies reporting long-term data, rates of PPI range from 5.9% to 17%.62,67,69,72 –74 Contemporary pooled analyses indicate a 6.0% to 6.8% and 7.9% to 8.2% rate of PPI at 30 days and 5 years, respectively.70,71 A separate analysis solely analyzing PPI post-SUAVR indicates an overall rate of 7% that is consistent across low-volume and high-volume centers but does tend to decrease over time with increasing user experience. 58 Several factors influence the risk of PPI following SUAVR, including preexisting conduction abnormalities such as first-degree atrioventricular nodal block or right bundle branch block.75,76 SUAVR is also associated with a significantly increased risk of new-onset left bundle branch block, with longer follow-up indicating that more than one-third resolve and do not require intervention.77,78 Despite considerable improvement in the rate of PPI over the last 11 years (12.8% down to 5.9%) secondary to increased user experience and avoidance of valve oversizing, the rate of PPI remains significantly higher than following SAVR.17,79,80
Paravalvular leak
The rate of overall PVL post-SUAVR ranges from 0.8% to 11%.61,62,67,69,72 Composite analyses indicate a 0.7% to 0.9% and 1.5% to 3.6% rate of severe PVL at 30 days and 5 years, respectively.70,71 A <1% reintervention rate for PVL was observed during the follow-up period. Asymmetric annular geometry and improper valve sizing are postulated to contribute to the risk of PVL. Critically, contemporary pooled analyses report equivalent rates of PVL following SUAVR and SAVR and reduced PVL with SUAVR than with TAVR.80 –82
Patient-prosthesis mismatch
With standard sutured AVR, the rate of PPM ranges from 20% to 70%. 83 Although there is some controversy regarding PPM, current evidence indicates a detrimental effect on myocardial remodeling following AVR and an increased risk of mortality.84,85 The lack of a sewing ring in the Perceval S valve affords a larger EOA. Propensity-matched analysis indicates superior indexed EOA (1.50 ± 0.18 cm2/m2 vs 0.81 ± 0.19 cm2/m2, P < 0.001) and less PPM (0% vs 61.3%, P < 0.001) with the SUAVR as compared with SAVR at 1-year follow-up. 86 Midterm outcomes of Perceval S use indicated an EOA of 1.5 to 1.8 cm2 and indexed EOA of 0.8 to 0.9 cm2/m2.62,69,71 The large EOA and low rates of PPM with Perceval implantation contribute to the excellent hemodynamics observed.
Hemodynamics
Overall mean and peak gradients are 9.0 to 13.6 mm Hg and 16.6 to 24.9 mm Hg at the longest available echocardiography follow-up.59 –62,69,72 Specifically, the CAVALIER and Perceval Sutureless Aortic Valve Implantation trial report mean and peak aortic valve gradients of 9.0 ± 5.0 and 17.1 ± 8.7 mm Hg, and 13 ± 6 and 23 ± 10 mm Hg, respectively.59,62 Technical advancements in valve deployment, namely, avoiding oversizing, have contributed to improvements in the hemodynamic parameters observed. 17
Durability and SVD
Freedom from SVD is 100% at 1 year, 96% at 5 years, and 97% to 98.9% at 10 years.59,62,69 Pooled outcomes from studies reporting midterm outcomes indicate a 98.5% to 99.6% freedom from SVD at 5 years. The rate of reintervention for SVD is <1%.70,71
Infective endocarditis
Among studies reporting long-term outcomes, the rate of IE following SUAVR is 0% to 4.6%.60,62,69,72 Meta-analyses indicate a 1.1% to 1.6% rate of IE at 5-year follow-up and a 1.6% rate of reintervention for IE.70,71 SUAVR does not appear to come with an equivalent risk of IE compared with SAVR and TAVR. 80
Bleeding
Rates of major bleeding following SUAVR range from 1.3% to 9.4%.59 –62,72 Aggregate analysis of pooled outcomes yields a 2.4% rate of severe bleeding at 30 days. 70 SUAVR does not increase the risk of major bleeding or the requirement for blood transfusions as compared with SAVR. 80
Comparison With Other Prosthetic Valve Replacement
SAVR
Several systematic reviews and meta-analyses have sought to determine whether SUAVR is superior to conventional sutured AVR. Early meta-analyses reported decreased CPB and aortic cross-clamp times, a decreased rate of AKI and blood transfusions, but an increased rate of PPI with SUAVR.82,87 The most contemporary network analysis composed of 26 studies and 27,614 patients indicated equivalent 30-day (odds ratio [OR] = 0.99, 95% confidence interval [CI]: 0.85 to 1.16, P = 0.93) and 2-year mortality (OR = 0.99, 95% CI: 0.43 to 2.30, P = 0.98) between these groups but a significantly increased risk of PPI (OR = 2.5, 95% CI: 2.25 to 2.77, P < 0.001) with SUAVR. There were no differences in rates of stroke, AKI, PVL, or valve hemodynamics. 80 The PERSIST-AVR trial was the first randomized controlled trial comparing SUAVR and SAVR. In their per-protocol analysis, Fischlein et al. reported comparable hemodynamics with SUAVR and SAVR at 1-year follow-up. The was no significant difference in the rate of overall PVL for SUAVR and SAVR, respectively (11.3% vs 15.0%, P = 0.315). 21 In a subanalysis of the PERSIST-AVR trial comparing ministernotomy and full sternotomy approaches, SUAVR resulted in significantly lower MACCE (5.2% vs 10.8%), stroke (1.0% vs 5.4%), atrial fibrillation (4.2% vs 11.4%), and rehospitalization (21.8 vs 47.6 days) compared with SAVR when performed via ministernotomy; however, for SUAVR, this came at the expense of a higher PPI rate (11% vs 1.6%). 22 An additional subanalysis of this trial by Lorusso et al. analyzed the influence of prosthesis size on PPI rates and determined that increased rates of PPI following SUAVR came only with implantation of the extra-large device. 88 The results of multiple large retrospective, propensity-matched analyses are largely consistent with these results.89,90 Superior results in various measures of postoperative morbidity, including bleeding, ICU and hospital LOS, low cardiac output syndrome, atrial fibrillation, and mild aortic regurgitation have also been noted following SUAVR.90,91
Rapid deployment valves
Despite rapid deployment and sutureless valves often being categorized together, as previously mentioned, these 2 valve technologies are in fact separate entities and should be analyzed separately. Several studies have examined differences in postoperative outcomes between these 2 valve types. Meta-analyses have indicated essentially equivalent early clinical outcomes, including in-hospital mortality and stroke. SUAVR is consistently associated with reduced CPB and aortic cross-clamp times but comes with a greater risk of mild PVL, PPI, and inferior hemodynamic function.92,93 A contemporary propensity-matched analysis of the SURD-IR was consistent with these results, reporting superior hemodynamic function in the form of lower valve gradients and reduced rates of mild AI with implantation of the Intuity Elite as compared with the Perceval S valve. 94 The superior hemodynamics of Intuity is likely secondary to the inflow frame widening the left ventricular outflow tract and facilitating laminar flow. It should also be noted that these meta-analyses are largely composed of retrospective studies that do not employ propensity matching, and the patient populations differ in their risk profiles. Prospective, randomized controlled trials with long-term follow-up are ultimately required to conclusively determine the superior valve type. In reality, it is likely that both valves are safe and effective and have slight advantages in specific patient populations.
TAVR
SUAVR and minimally invasive surgery have improved the limitations of SAVR and bridged the gap to TAVR. Consequently, a pertinent comparison in the definitive treatment of AS is SUAVR versus TAVR. Various meta-analyses have reported reduced rates of early mortality and PVL with no greater risk of conduction abnormalities or PPI for SUAVR as compared with TAVR.95–98 In an analysis of solely propensity-matched studies by Meco et al., SUAVR was associated with reduced 30-day, 1-year, and 2-year mortality, stroke, moderate to severe PVL, and vascular complications. PPI rates were equivalent between groups; however, SUAVR did come with a greater risk of blood transfusion. 81 The most up-to-date and comprehensive composite analysis indicated reduced odds of 2-year mortality (OR = 0.39, 95% CI: 0.17 to 0.88, P = 0.02) and mild PVL (OR = 0.11, 95% CI: 0.06 to 0.21, P < 0.001) for SUAVR as compared with TAVR. In addition, despite previous concerns over inferior valve hemodynamics with SUAVR versus TAVR, SUAVR displayed no difference and a reduction in mean postoperative valve gradients in the analysis of unadjusted and adjusted studies, respectively. 80 A patient-level simulation has analyzed the potential economic effects of the reduced mortality and morbidity with SUAVR as compared with TAVR, estimating that patients undergoing SUAVR will live 1.25 times longer than their counterparts and save the health care system ~20,000 USD per patient long-term. 99
Discussion
Future Perspectives
Early and midterm results of SUAVR with the Perceval S have been favorable, and the long-term outcomes of the CAVALIER and Perceval Sutureless Aortic Valve Implantation trials will provide more evidence about its durability. As we learn more about SUAVR, it appears that certain patient populations may benefit more from this intervention. Proper sizing is critical to the early success of this valve, which is more nuanced relative to conventional stented bioprostheses. Preoperative multidetector-row computed tomography (MDCT) has shown great promise in aiding in optimal valve sizing. The circumference-derived and area-derived diameters on MDCT are extremely accurate and precise. 100 Therefore, to further optimize valve seating and reduce PVL, PPI, and transvalvular pressure gradients, CT should become the gold standard in preoperative planning, as it is used in TAVR. In addition to enhancing preoperative planning, SUAVR presents a unique opportunity to further develop and refine minimally invasive AVR. In this regard, robotic SUAVR is a relatively unchartered area that will likely become more prominent in the coming years. 33 Finally, despite the excellent durability of the Perceval S valve experienced thus far, there is a need for greater investigation into reintervention strategies. ViV TAVR has been effective in the small proportion of patients requiring reoperative AVR; however, additional analysis is ultimately required. 101
Strengths and Limitations
The present review provides not only an overview of the Perceval S valve’s early and midterm outcomes but also a comprehensive analysis of the indications and applications of SUAVR. With this review, as well as the current literature on the clinical outcomes of the Perceval valve, there are limitations. It is important to note that multiple retrospective studies including a “SUAVR group” have in fact included both the Perceval and Edwards Intuity valves. For instance, the SURD-IR registry collects data on the use of both valves, and individual studies using these data do not always substratify outcomes based on valve type. In addition, most comparisons between SUAVR and TAVR do not employ propensity matching and are largely composed of TAVR patients who are at higher surgical risk than their counterparts. Finally, the data supporting SUAVR in patients with BAV, reoperative AVR, IE, and AI are largely based on a low level of evidence from case series or retrospective cohort studies.
Conclusions
SUAVR represents a hybrid bioprosthetic valve technology, between stented bioprostheses and TAVR. The Perceval S valve is the only true sutureless valve currently on the market. Herein, we have reviewed the valve design and deployment, analyzed various applications of the technology in challenging pathology, and summarized the current literature on early and midterm clinical outcomes. SUAVR facilitates minimally invasive surgery and offers an alternative strategy for patients with small aortic annuli or those undergoing complex operations with concomitant procedures. SUAVR results in excellent long-term morbidity, mortality, durability, and hemodynamic function. In comparison with SAVR, SUAVR does come at a greater risk of postoperative PPI; however, increasing user experience and refinements in implantation technique have contributed to reductions in this outcome. SUAVR results in similar morbidity and mortality to rapid deployment AVR but inferior valvular hemodynamics. Midterm outcomes are superior to TAVR; however, further high-powered investigation is ultimately necessary for all these comparisons.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845241231989 – Supplemental material for The Perceval Sutureless Bioprosthetic Aortic Valve: Evolution of Surgical Valve Technology
Supplemental material, sj-pdf-1-inv-10.1177_15569845241231989 for The Perceval Sutureless Bioprosthetic Aortic Valve: Evolution of Surgical Valve Technology by Nicholas M. Fialka, Ryaan EL-Andari, Shaohua Wang, Aleksander Dokollari, William D. T. Kent and Ali Fatehi Hassanabad in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.