
Abstract

Introduction
Descending thoracic aortic dissection with subsequent rupture is nearly uniformly fatal. When such aortic rupture is contained, survival is possible, although prognosis remains poor. We describe a patient who survived rupture of a dissected descending thoracic aorta after the resulting hematoma was contained within the mediastinum. In this patient, profound external bronchial compression developed following endovascular aortic repair. The patient’s clinical management and outcome hinged on the restoration of airway patency. To our knowledge, this is the first report in the literature of successful management of this complication.
Case Report
The patient was a 57-year-old, morbidly obese woman with chronic obstructive pulmonary disease on chronic steroids for severe rheumatoid arthritis. She had a known, chronic (diagnosed 5 months prior), asymptomatic descending thoracic aortic dissection. Routine, serial, outpatient imaging identified concerning anatomy and significant progression of the dissection, prompting patient transfer to the emergency department. Computed tomography (CT) angiogram revealed pronounced retrograde progression of (originally distal descending aortic) dissection to involve the entire proximal segment with extension into the arch. The proximal-mid descending aorta appeared consistent with rupture with hematoma contained within the mediastinum (Fig. 1, Supplemental Video 1a-c).
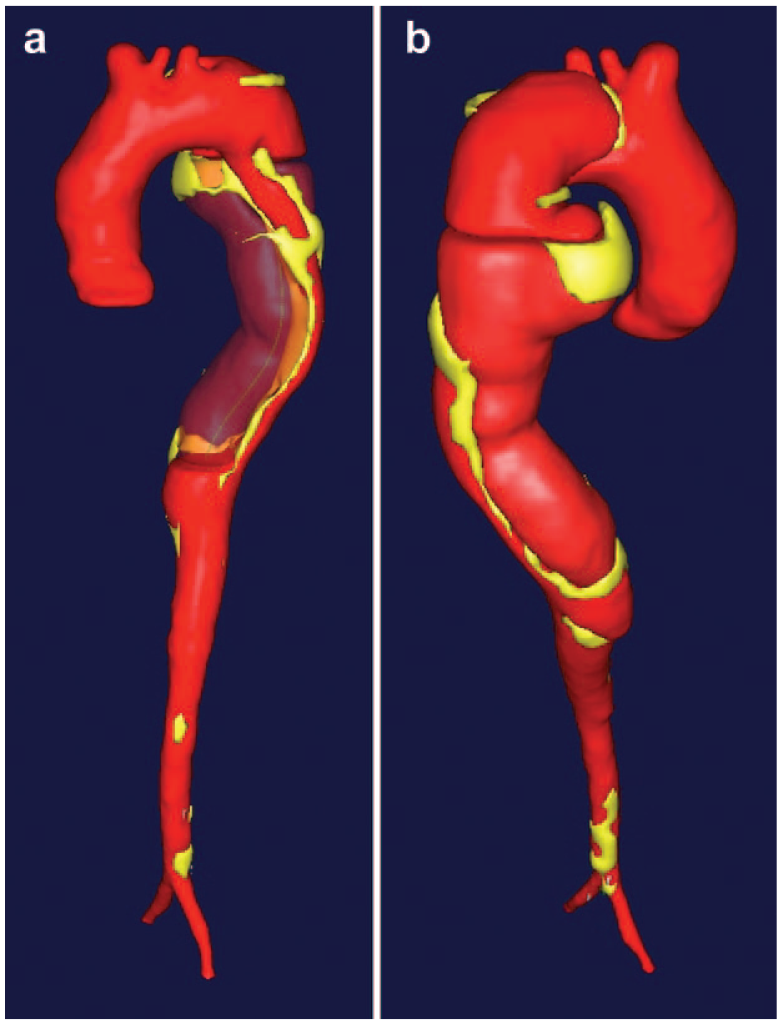
(a) Anterior and (b) posterior views of center-line 3-dimensional reconstructions of computed tomographic angiography (M2S Inc., West Lebanon, NH, USA) demonstrating a large hematoma/contained rupture of a known, chronic descending thoracic aortic dissection in proximity to the left main stem bronchus. In figure part (a), the narrow true lumen and wide false lumen (solid red = true aortic lumen; translucent red = false lumen/hematoma).
Various treatment options were considered, including endovascular approaches, thoracotomy for open aortic repair, and thoracotomy for open repair utilizing circulatory arrest. A hybrid technique was selected using a sternotomy for debranching in combination with antegrade deployment of a Gore (Flagstaff, AZ, USA) TAG 37 mm × 150 mm aortic stent. This approach was selected in this case to avoid the morbidity associated with a thoracotomy and to minimize the handling of dissected aortic tissue, which extended well into the aortic arch.
The primary procedure was successful, but a postoperative chest roentgenogram (Supplemental Fig. 1) demonstrated complete opacification of the left lung field upon arrival to the cardiac surgery intensive care unit. During the immediate postoperative period, multiple fiber-optic bronchoscopy procedures were performed, which demonstrated equivocal findings. Although some evidence of (dynamic) left bronchial narrowing was appreciated, interpretation was difficult, especially when viewed in the context of suspected bronchomalacia. Over the next several weeks, the patient struggled with pulmonary toilet, oxygenation, pneumonia, and tracheostomy/prolonged ventilator dependency.
Postoperative CT identified pronounced left bronchial compression secondary to pressure from the adjacent hematoma (Supplemental Fig. 2). However, the future impact of this finding was not fully appreciated at the time. On postoperative day 21, the patient underwent insertion of a 10 mm × 40 mm self-expandable removable, covered left bronchial stent to restore bronchial patency (Supplemental Video 2a-b). The patient rapidly resolved her pneumonia and subsequently weaned from the ventilator easily. She was discharged from the hospital and made a full recovery. We had planned to remove the stent 8 weeks later; however, the patient refused. CT 6 months after bronchial stent placement (Fig. 2) demonstrates a patent left main bronchus, a fully expanded aortic stent, and resolution of previous mediastinal hematoma.
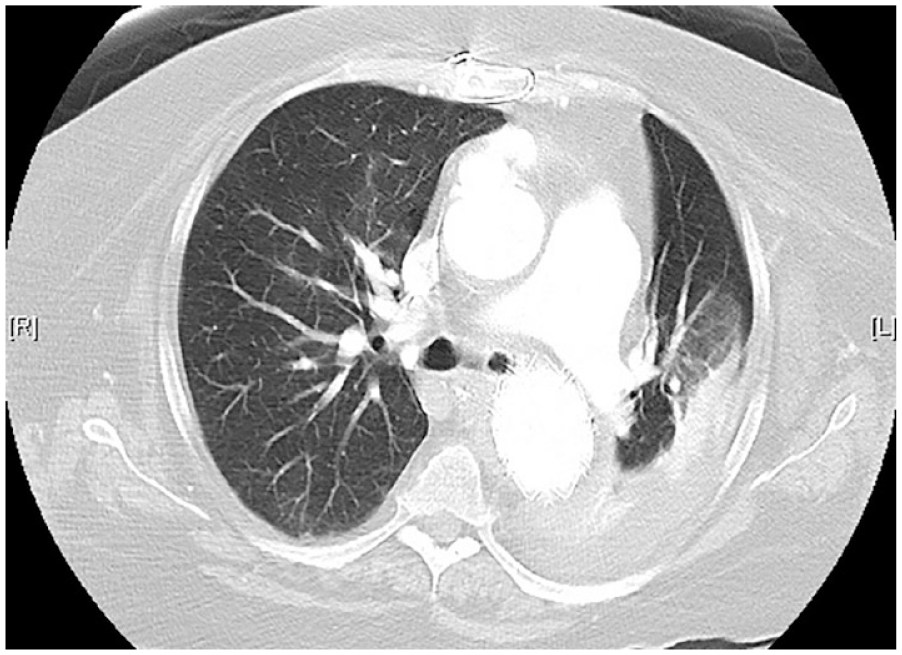
Computed tomography demonstrating left main stem bronchial patency with removable airway stent in position (at 6-month follow-up).
Discussion
Aortic rupture is often fatal. Patients fortunate to survive still face enormous corrective procedures to restore aortic integrity. Large surgical incisions and prolonged hospital stays disrupt pulmonary physiology. Even under the optimized circumstances of elective surgery, the risk of pneumonia and other insults to the respiratory system is not insignificant. Vigilance in identifying pulmonary complications remains a focus of perioperative care in such surgical patients.
As described, we have encountered a case of severe left main stem bronchial compression secondary to a residual mediastinal hematoma (from contained descending thoracic aortic rupture). Retrospective examination of the patient’s original CT scan identified evidence of minor bronchial compression with suggestion of bronchomalacia. A subsequent CT scan obtained immediately preceding aortic stent placement (Supplemental Fig. 3) shows significantly increased left bronchial compression secondary to expansion of the mediastinal hematoma consistent with leakage of blood at the rupture site. The expanding hematoma continued to produce pressure on the adjacent left bronchus. We believe that stent deployment for endovascular repair of the aorta generated additional pressure on the airway (by radial force that translated through the existing hematoma to generate and, possibly, by forces produced by the stent as it navigated curves within the aorta). Compression of the left bronchus impaired pulmonary physiology, which resulted in subsequent pneumonia and inability to wean from ventilator support.
While the cause of the aneurysm and predilection to rupture were addressed, no specific measures were performed to drain the hematoma. The consequences of leaving residual hematomata are being increasingly seen in this era of endovascular aortic interventions.
A similar process of bronchial compromise secondary to extrinsic compression from an adjacent aortic aneurysm (no rupture) has been described by Singh et al. 1 Their group performed open thoracoabdominal aortic replacement using a woven Dacron graft to relieve airway compression by the aneurysm.
In our case, we exacerbated airway compression with our surgical intervention. Bronchial stenting was subsequently required to restore airway patency and bridge the patient to full recovery. In the future, based on this learned experience, we advocate for early intervention.
Conclusions
Airway obstruction secondary to endovascular repair of contained rupture of descending thoracic aortic dissection is a rare, yet treatable complication. A high degree of suspicion is required for airway compression after aortic rupture occurs in proximity to airway structures in the mediastinum. In our case, airway compression was exacerbated by our endovascular intervention as a consequence of the radial force exerted by the stent upon and through the adjacent undrained hematoma. When airway compression is encountered, early consideration should be given to bronchial stenting to restore patency.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845231223570 – Supplemental material for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection
Supplemental material, sj-pdf-1-inv-10.1177_15569845231223570 for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection by Nikola Dobrilovic, Karl Karlson, Jaishankar Raman, Peter Soukas, Immad Sadiq, Lidia Vognar and Arun Singh in Innovations
Supplemental Material
sj-pdf-2-inv-10.1177_15569845231223570 – Supplemental material for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection
Supplemental material, sj-pdf-2-inv-10.1177_15569845231223570 for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection by Nikola Dobrilovic, Karl Karlson, Jaishankar Raman, Peter Soukas, Immad Sadiq, Lidia Vognar and Arun Singh in Innovations
Supplemental Material
sj-pdf-3-inv-10.1177_15569845231223570 – Supplemental material for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection
Supplemental material, sj-pdf-3-inv-10.1177_15569845231223570 for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection by Nikola Dobrilovic, Karl Karlson, Jaishankar Raman, Peter Soukas, Immad Sadiq, Lidia Vognar and Arun Singh in Innovations
Supplemental Material
sj-pdf-4-inv-10.1177_15569845231223570 – Supplemental material for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection
Supplemental material, sj-pdf-4-inv-10.1177_15569845231223570 for Left Bronchial Compression After Endovascular Repair of Contained Rupture of Descending Thoracic Aortic Dissection by Nikola Dobrilovic, Karl Karlson, Jaishankar Raman, Peter Soukas, Immad Sadiq, Lidia Vognar and Arun Singh in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.