
Abstract
Objective:
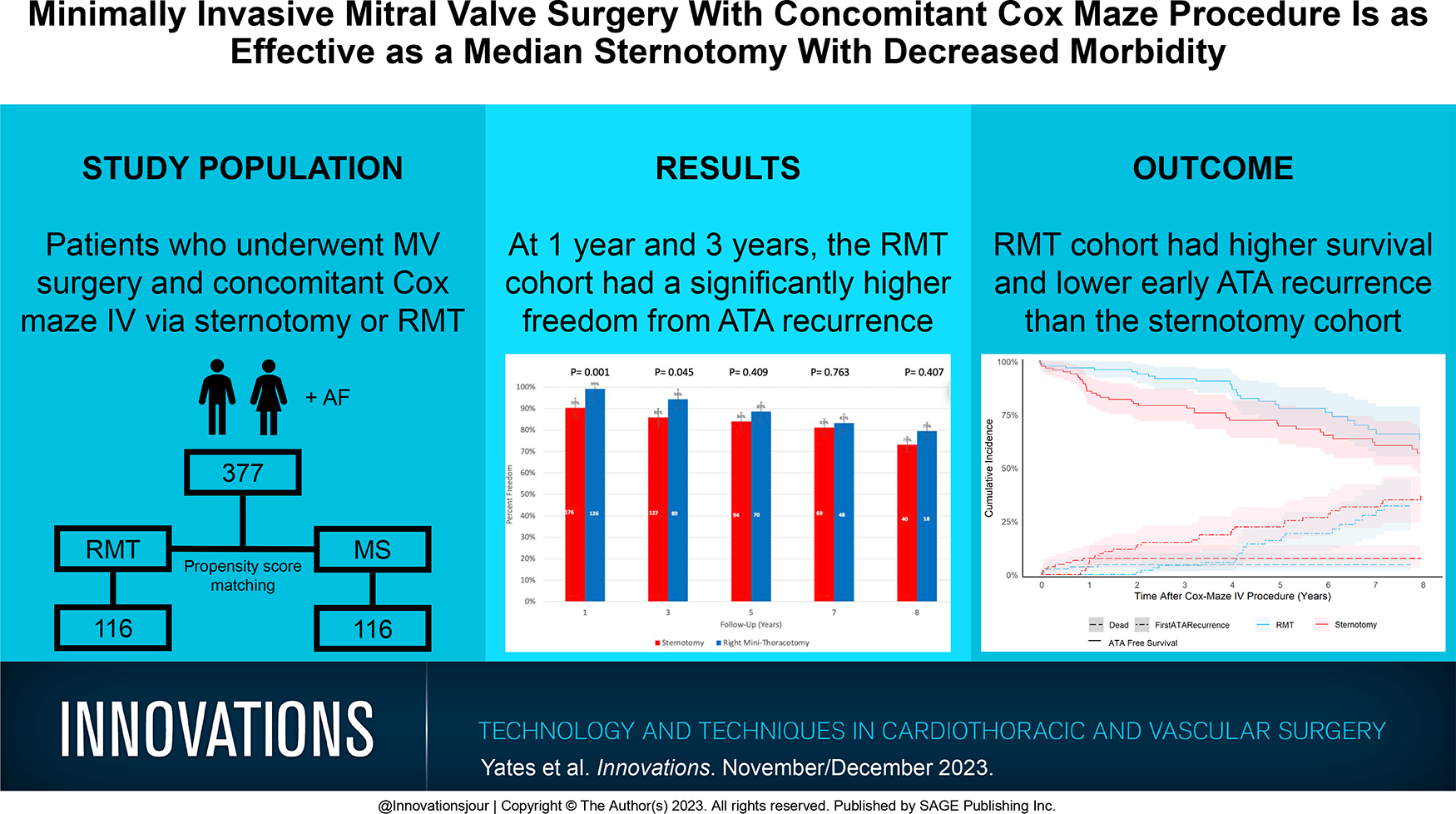
A right minithoracotomy (RMT) is a minimally invasive surgical approach that has been increasingly performed for the concomitant Cox maze IV procedure (CMP) and mitral valve surgery (MVS). Little is known regarding whether long-term rhythm and survival outcomes are affected by the RMT as compared with the traditional median sternotomy (MS) approach.
Methods:
Between April 2004 and April 2021, 377 patients underwent the concomitant CMP and MVS, of whom 38% had RMT. Propensity score matching yielded 116 pairs. Freedom from atrial tachyarrhythmias (ATA) was assessed with prolonged monitoring annually for 8 years. Survival, rhythm, and perioperative outcomes were compared.
Results:
The unmatched RMT cohort had a greater freedom from ATA recurrence at 1 year (99% vs 90%, P = 0.001) and 3 years (94% vs 86%, P = 0.045). The matched RMT cohort had longer cardiopulmonary bypass (median: 215 [199 to 253] vs 170 [136 to 198] min, P < 0.001) and aortic cross-clamp (110 [98 to 124] vs 86 [71 to 102] min, P < 0.001) times but shorter intensive care time (48 [24 to 95] vs 71 [26 to 144] h, P = 0.001) and length of stay (8 [6 to 11] vs 10 [7 to 14] h, P < 0.001). More pacemakers (18% vs 4%, P < 0.001) and postoperative transfusions (57% vs 41%, P = 0.014) occurred in the MS cohort. The 30-day mortality (P = 0.651) and 8-year survival (P = 0.072) was not significantly different between the cohorts.
Conclusions:
Early 1-year and 3-year freedom from ATA recurrence was better in the RMT cohort compared with the MS cohort. Despite longer operative times, the RMT cohort had shorter lengths of stay, fewer postoperative transfusions, and fewer pacemakers placed.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.