
Abstract
Objective:
Robot-assisted minimally invasive direct coronary artery bypass (RA-MIDCAB) surgery and hybrid coronary revascularization (HCR) are minimally invasive alternative strategies to conventional coronary artery bypass surgery in patients with isolated left anterior descending (LAD) stenosis or multivessel coronary disease. We analyzed a large, multicenter data-set based on the Netherlands Heart Registration including all patients undergoing RA-MIDCAB.
Methods:
We included 440 consecutive patients who underwent RA-MIDCAB with the left internal thoracic artery to LAD between January 2016 and December 2020. A proportion of patients underwent percutaneous coronary intervention (PCI) of non-LAD vessels (i.e., HCR). The primary outcome was all-cause mortality at median follow-up of 1 year, which was subdivided into cardiac and noncardiac. Secondary outcomes included target vessel revascularization (TVR) at median follow-up as well as 30-day mortality, perioperative myocardial infarction, reoperation for bleeding or anastomosis-related problems, and in-hospital ischemic cerebrovascular accident (iCVA).
Results:
Among all patients, 91 (21%) underwent HCR. At median (IQR) follow-up of 19 (8 to 28) months, 11 patients (2.5%) had died. In 7 patients, the cause of death was defined as cardiac. TVR occurred in 25 patients (5.7%), of whom 4 underwent CABG and 21 underwent PCI. At 30-day follow-up, 6 patients (1.4%) had a perioperative myocardial infarction, of whom 1 died. One patient (0.2%) developed an iCVA, and 18 patients (4.1%) underwent reoperation for bleeding or anastomosis-related problems.
Conclusions:
The clinical outcomes of patients undergoing RA-MIDCAB or HCR in the Netherlands are good and promising when compared with the currently available literature.
Keywords
Central Message
We included all 440 patients who underwent robot-assisted minimally invasive direct coronary artery bypass and hybrid coronary revascularization in the Netherlands Heart Registration and evaluated their clinical outcomes, which were good and promising when compared with the currently available literature.
Introduction
Robot-assisted minimally invasive direct coronary artery bypass (RA-MIDCAB) is the strategy to bypass the left anterior descending artery (LAD) with the left internal thoracic artery (LITA) in a minimally invasive procedure. In RA-MIDCAB, the LITA is harvested using robotic assistance provided by the da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA, USA) and then anastomosed to the LAD. 1 In conventional coronary artery bypass grafting (CABG), the LITA-LAD conduit has an excellent long-term patency of >95% at 5-year follow-up and provides a survival benefit when compared with medical treatment or percutaneous coronary intervention (PCI).2–4 In patients with multivessel disease, when RA-MIDCAB is combined with PCI and stenting of non-LAD coronary arteries, it results in what is called hybrid coronary artery revascularization (HCR). 5 It has been reported that, compared with CABG, RA-MIDCAB is safe and effective in patients with proximal LAD lesions or chronically occluded LAD coronary arteries and leads to a reduced length of hospital stay, less use of red blood cell transfusion, and an early quality of life benefit. 6 It has also been shown that, in comparison with PCI, RA-MIDCAB is associated with a reduced need for repeat revascularization and a survival benefit 3 years after the original procedure. 7 Despite these promising outcomes, criticism still persists as many cohort studies were hampered by small sample sizes and being single-center studies. 6 In this article, we report the clinical outcomes for all patients in the Netherlands who received RA-MIDCAB, to evaluate its benefits in a relatively large study population, also illustrating the benefits of a nationwide registry.
Methods
Patient Population
A post hoc analysis of prospectively collected data was performed in 440 consecutive patients undergoing RA-MIDCAB in the Netherlands between January 2016 and December 2020. Three cardiac centers performed RA-MIDCAB during that time frame: the University Medical Center Utrecht, Maastricht University Medical Center, and Isala Zwolle. All patients underwent RA-MIDCAB with the LITA-LAD conduit. In addition, a proportion of patients underwent HCR in a separate stage for PCI of non-LAD vessels. The procedure was qualified as HCR if this revascularization strategy was the documented treatment intention during the heart team meeting. Separate designations were introduced to distinguish the treatment sequences for HCR: “two-staged HCR” if a patient received RA-MIDCAB followed by PCI and “reversed two-staged HCR” if a patient received a PCI with stenting because of, for example, an emergent myocardial infarction with the culprit in either the circumflex coronary artery or the right coronary artery. To be included, patients had to be adults (>18 years) with proximal LAD lesions or chronically occluded LAD with or without additional lesions in the left circumflex artery and/or right coronary artery accessible for PCI. Patients were excluded if they had contraindications for RA-MIDCAB, such as no possibility for single-lung ventilation due to severe pulmonary disease or an intramural LAD limiting the technicality of an RA-MIDCAB procedure. Contraindications for HCR were a history of major bleeding complications due to dual antiplatelet therapy (DAPT), the latter being essential after PCI with stenting. Patient written consent and ethics approval from the Medical Ethics Review Committee at every institution performing RA-MIDCAB was acquired.
Data Collection
We set out to analyze data from the multicenter Netherlands Heart Registration (NHR), the nationwide database that monitors all patients undergoing RA-MIDCAB with or without HCR since 2015.8,9 This large, nationwide registry collects the data of all patients undergoing open heart surgery and other cardiac-related interventions such as PCI and is updated on a yearly basis. All variables were collected prospectively and systematically in a protocolled manner using standardized definitions by the NHR handbook. The data of the registry are also accessible for research, enabling large cohort studies, which are essential for quality monitoring and improvement implementation. We (A.R.J and H.F.N.) manually checked all NHR provided data for each participating center for inconsistencies and missing entries. Missing data, such as conversion reasons, reason for reoperation, and cause of death, were reported back to the NHR and manually completed by data managers from each participating center. Preoperative patient characteristics, perioperative variables, and postoperative 30-day as well as midterm outcomes were assessed. Patient characteristics were diagnosed and scored according to the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II. 10 Preoperative conditions and postoperative outcomes were scored according to the definitions used by the NHR.8,9 The NHR verified the collected data, assessed the implemented statistical analyses, and reviewed this article before they approved its publication on behalf of the Cardiothoracic Surgery and PCI Registration Committees of the NHR (Appendix 1).
Outcomes
The primary outcome of interest was all-cause mortality at median follow-up. Follow-up intervals varied between patients, and we defined follow-up as a median follow-up of 1 year after the original procedure. Mortality was subdivided into cardiac and noncardiac. Cause of death was specified by the cardiothoracic surgeon at the institution where the patient underwent RA-MIDCAB by searching their medical records. All deaths were considered cardiac unless a definite noncardiovascular cause was established. Mortality was verified by cross-checking with the Nationwide Personal Records Database of the Netherlands. Secondary outcomes included repeat target vessel revascularization (TVR) at median follow-up. TVR was scored when repeat revascularization of the target vessel from the original procedure occurred between 30 days postoperative and follow-up. In addition, at 30-day follow-up, mortality (all-cause and cardiac), perioperative myocardial infarction, reoperation for bleeding or anastomosis-related problems, and in-hospital ischemic cerebrovascular accident (iCVA) were included as secondary outcomes.
Surgical Technique
The RA-MIDCAB procedure was performed in a standardized fashion by a dedicated team in each institution. In each institution, there was a single surgeon who performed the RA-MIDCAB procedures. Standard surgical procedures of each institution were followed. In summary, patients were placed in the supine position with a 10 cm soft roll or balloon under the chest between the scapulae and the left arm, allowing the left shoulder to be deflected posteriorly. The camera port was placed in the fourth/fifth intercostal space (ICS) medial to the anterior axillary line. Working ports were typically placed in the second/third and the sixth/seventh ICS medial to the anterior axillary line. Preferably, the distance between the ports was at least 10 cm to avoid instrument collisions and to maximize the working area. Once adequate port placement was achieved, LITA harvesting occurred. Single-lung ventilation or a bronchial blockage was used to deflate the left lung and therefore optimize the intrathoracic working space. In addition, CO2 insufflation from 5 to 10 mm Hg was exploited, and a 0° or 30° up-scope was used in most cases. The LITA was taken down with care using a combination of blunt dissection and electrocautery in either a skeletonized or pedicled fashion. Once the LITA was harvested, a pericardiectomy was performed robotically, and the target coronary vessel, namely, the LAD, was identified. Appropriate heparinization was achieved if the activated clotting time was >300 s. With the robotic camera still in place, a needle was used to identify the optimal intercostal space for the small thoracotomy, usually 4 to 7 cm long. After robot undocking, the minithoracotomy was made and a soft tissue retractor placed. The endoscopic Octopus Nuvo (Medtronic, Dublin, Ireland) or Acrobat-i Stabilizer (MAQUET, Getinge, Göteborg, Sweden) off-pump stabilizer was inserted via a previous port site or direct through the minithoracotomy and was used to stabilize the target vessel while off-pump coronary anastomosis was performed in the usual fashion. If a conversion to sternotomy was required, a conventional on-pump or off-pump CABG was performed.
Percutaneous Coronary Intervention
PCI with stenting of the non-LAD coronary arteries was performed by an interventional cardiologist, mostly during a second procedure. The cardiologist used standardized procedures according to the participating center. In summary, access was gained using either the femoral artery or the radial artery. A catheter was inserted and threaded through the coronary artery until it reached the stenosis. A small wire was put in place, and a balloon catheter covered with a stent was advanced over the wire. Inflation of the balloon expanded the stent. Once the plaque was compressed against the wall of the coronary artery and the stent was in place, the balloon was deflated and withdrawn. Patients received second-generation drug-eluting stents (DES) and lifelong aspirin combined with ticagrelor or clopidogrel for a period of 12 months in most cases, depending on the individual risk of bleeding.
Statistical Analysis
Dichotomous variables were displayed as absolute numbers with percentages, and normally distributed continuous variables were displayed as means with standard deviations (SDs). Non-normally distributed continuous variables were displayed as medians with interquartile ranges (IQRs). A Kaplan-Meier curve was generated for the primary outcome. Statistical analyses were performed with IBM SPSS Statistics for Windows, Version 26 (IBM Corp., Armonk, NY) and R version 4.0.3. (The R Foundation for Statistical Computing Platform). 11
Results
Data were available for all 440 patients who underwent RA-MIDCAB or HCR between January 2016 and December 2020 in the Netherlands. The mean patient age was 65 ± 9 years, and 80% of patients (n = 354) were male. Nine patients (2%) underwent a conventional on-pump or off-pump CABG with sternotomy instead of the scheduled RA-MIDCAB at the heart team. Among those 9 patients, 3 patients (0.7%) underwent a conversion after surgical incision. The reasons for conversion were an intramural LAD, a nonviable LITA-LAD anastomosis, and a ministernotomy to obtain adequate access for making the LITA-LAD anastomosis. Six patients did not undergo RA-MIDCAB and were converted to a CABG before surgical incision due to hemodynamic instability at the start of the anesthesia (n = 4) or due to respiratory instability because of difficulty with unilateral ventilation of the right lung (n = 2).
In 84% of patients (n = 371), the RA-MIDCAB was elective, and 91 patients (21%) underwent an additional PCI. HCR was performed as a two-staged procedure in all cases, and in 53% of patients (n = 48) it was a reversed two-staged procedure. All HCR patients received PCI with second-generation DES. Baseline characteristics of the study population are shown in Table 1.
Patient Demographics for All Patients Who Underwent RA-MIDCAB or HCR Between 2016 and 2020 in the Netherlands.
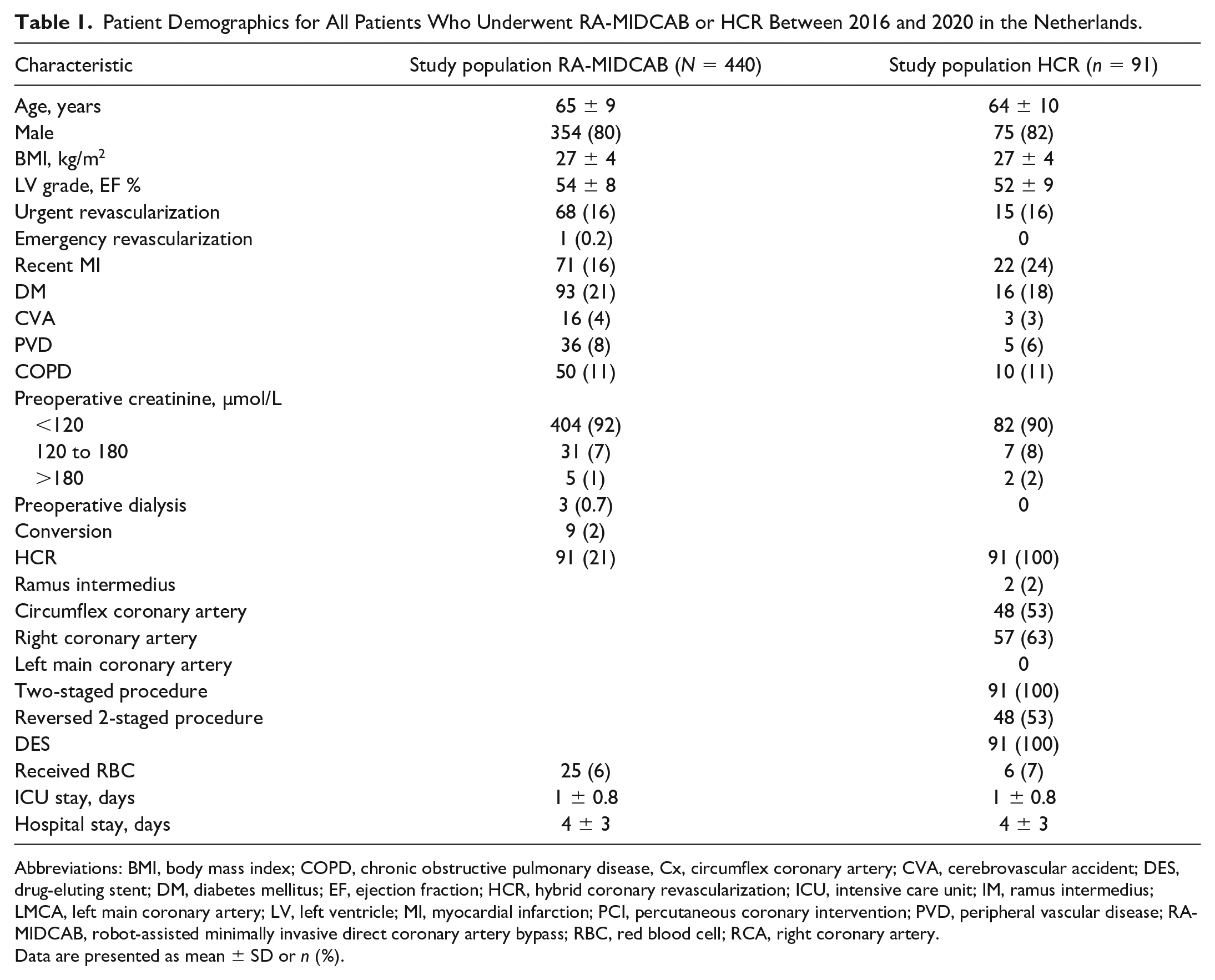
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease, Cx, circumflex coronary artery; CVA, cerebrovascular accident; DES, drug-eluting stent; DM, diabetes mellitus; EF, ejection fraction; HCR, hybrid coronary revascularization; ICU, intensive care unit; IM, ramus intermedius; LMCA, left main coronary artery; LV, left ventricle; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; RA-MIDCAB, robot-assisted minimally invasive direct coronary artery bypass; RBC, red blood cell; RCA, right coronary artery.
Data are presented as mean ± SD or n (%).
All-Cause Mortality
Complete follow-up was achieved. Median follow-up was 19 (8 to 28) months, at which time 2.5% of patients (n = 11) had died (Fig. 1). All-cause mortality was subdivided into cardiac mortality and noncardiac mortality. Two patients died of a myocardial infarction of whom 1 had died within the first 30 days postoperatively. Furthermore, 1 patient died of an arrhythmia. For 4 patients, no information regarding the cause of death was available. This resulted in a total of 7 patients who were classified as having a cardiac cause of death. Additionally, 1 patient died of respiratory failure and 3 patients died of a neurological cause other than CVA.
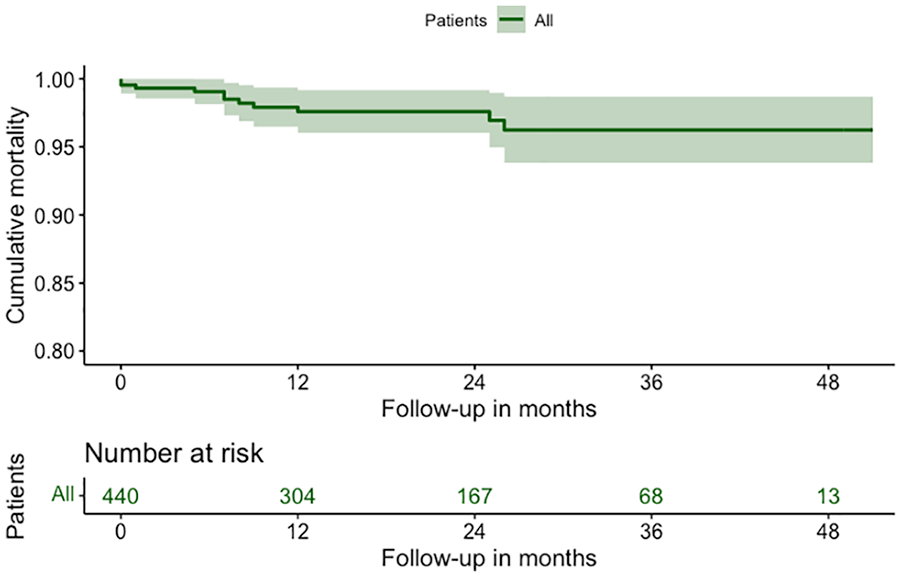
Kaplan-Meier curve with estimated fraction of patients surviving over time after robot-assisted minimally invasive direct coronary artery bypass and hybrid coronary revascularization for 440 consecutive patients in the Netherlands.
Secondary Outcomes
TVR occurred in 5.7% of patients (n = 25) at median follow-up of 19 (8 to 28) months. Four patients underwent repeat CABG, and 21 patients underwent repeat PCI. Among those who underwent repeat PCI, 17 patients had a restenosis of the LAD distal to the LITA-LAD anastomosis, and 1 of these 17 patients had an additional stenosis of the circumflex coronary artery, which was treated with PCI. Two patients had a stenosis of the LITA-LAD anastomosis, and 2 patients underwent repeat PCI of the left main coronary artery due to progression of preexisting lesions. Among those who underwent repeat CABG, 1 patient received a bypass of the LAD and the circumflex coronary artery. In the original procedure, the circumflex coronary artery was not included in the revascularization strategy. The other 3 patients underwent CABG of the LAD only. Among those who underwent repeat TVR, 3 patients initially had undergone HCR. The outcomes at median follow-up are shown in Table 2.
Primary Outcome All-Cause Mortality and Secondary Outcome TVR at Median (IQR) Follow-Up (19 [8 to 28] Months).
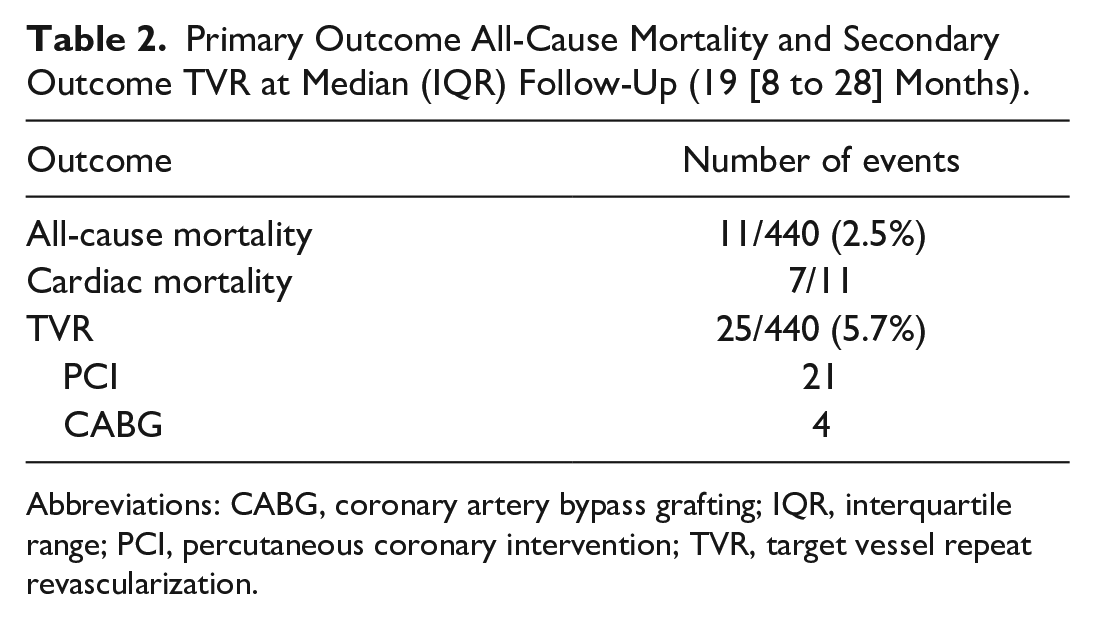
Abbreviations: CABG, coronary artery bypass grafting; IQR, interquartile range; PCI, percutaneous coronary intervention; TVR, target vessel repeat revascularization.
At 30-day follow-up, 1 patient had died (0.2%). That patient experienced a perioperative myocardial infarction, was reoperated for revision of the anastomosis, and died a couple of days later. In total,1.4% of patients (n = 6) had experienced a perioperative myocardial infarction. Of these, 4 patients underwent PCI of the LAD, 1 patient underwent PCI of the LITA-LAD conduit, and 1 patient, as described above, was reoperated for revision of the anastomosis.
One patient (0.2%) developed an iCVA, and 4.1% of patients (n = 18) underwent reoperation for bleeding or anastomosis-related problems. In all cases, the reoperation was either a rethoracotomy or a video-assisted thoracic surgery. In 11 patients, the reason for reoperation was bleeding. In addition, 1 patient was reoperated because of a tamponade, and in 5 cases, the patients underwent reoperation for revision of the LITA-LAD conduit. In 1 patient, the reason for reoperation was not reported and could not be retrieved. Among the 11 patients who underwent reoperation for bleeding, 9 patients received red blood cell transfusions. Among all RA-MIDCAB and HCR patients, 5.7% (n = 25) needed a transfusion of red blood cells. The outcomes at 30-day follow-up are shown in Table 3.
Secondary Outcomes Including All-Cause and Cardiac Mortality, Perioperative MI, iCVA, and Reoperations for Bleeding or Anastomosis-Related Problems at <30-Day Follow-Up.
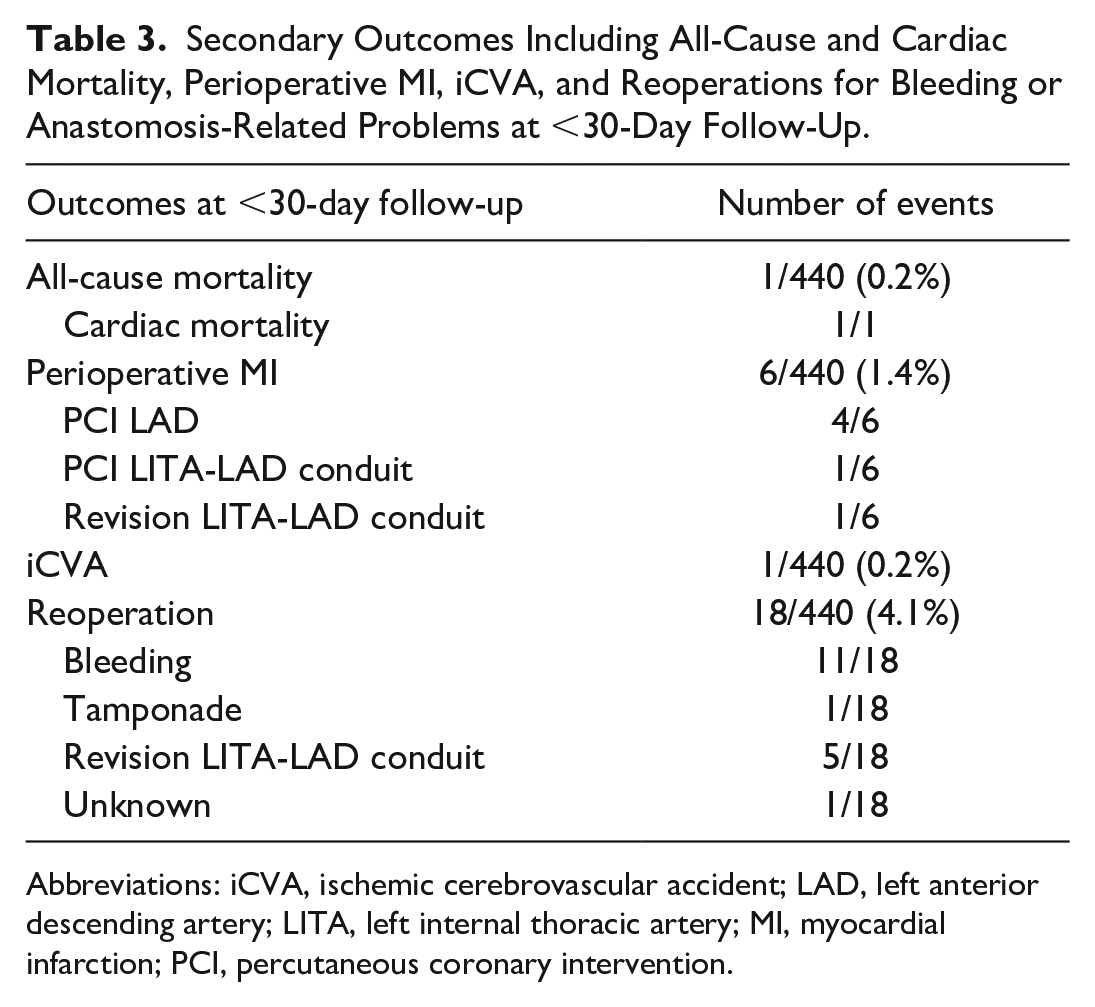
Abbreviations: iCVA, ischemic cerebrovascular accident; LAD, left anterior descending artery; LITA, left internal thoracic artery; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Discussion
We described the clinical outcomes of all 440 patients who underwent RA-MIDCAB or HCR in the Netherlands between January 2016 and December 2020. At 19 (8 to 28) months of follow-up, we found a survival rate of 97.5% and a TVR rate of 5.3%. Among the 11 patients who died, 7 patients were classified as having a cardiac cause of death. In addition, 1 patient developed an in-hospital iCVA, 6 patients developed a perioperative myocardial infarction, and 18 patients underwent reoperation for bleeding or anastomosis-related problems.
Retrospective cohort studies and meta-analyses have reported all-cause mortality rates between 0% and 3% in patients undergoing HCR or MIDCAB, at 12 to 18 months of follow-up.7,12 Our all-cause mortality rate of 2.5% at follow-up supports these prior findings.13–17 We found a cardiac mortality rate of 1.6%, which is higher than what was found by others (0% to 1%) in cohort studies and randomized controlled trials. 7 However, of the 7 cases we classified as cardiac deaths, the cause of death was unknown for 4 patients. We can therefore not exclude other noncardiac causes of death, poor patient selection, or an unsuccessful rehabilitation after surgery in these cases. Learning curve complications or technical interventional adverse events are less likely to be the cause of the cardiac-related deaths because we would expect a higher rate of cardiac complications at 30-day follow-up, such as myocardial infarctions. Our 30-day cardiac mortality rate is lower than previously reported cardiac mortality rates. 7
In our population, 1 patient died at 30-day follow-up due to a myocardial infarction related to the procedure. Meanwhile, other comparable studies reported 30-day mortality rates of 1% to 1.8%.18–20 At short-term follow-up, cardiac death is most likely related to the occurrence of myocardial infarction and its complications. Our low cardiac death rate is the result of our awareness and clinical follow-up with cardiac enzymes and electrocardiograms. We found a myocardial infarction rate of 1.4%, which is similar to prior reports.15,16 Patients presenting with myocardial infarction were treated aggressively: 4 patients underwent PCI with stenting of the LAD, 1 patient underwent a PCI with stenting of the LITA-LAD conduit, and 1 patient underwent a reoperation for revision of the LITA-LAD conduit.
TVR occurred in 5.7% of patients, of whom 4 patients underwent repeat CABG and 21 patients underwent repeat PCI between the first 30 days postoperatively and median study follow-up. RA-MIDCAB and PCI differ in revascularization mechanisms. RA-MIDCAB with the LITA-LAD conduit provides an alternative vascularization route addressing existing and preventing future atherosclerotic lesions by surgical collateralization and has shown excellent long-term patency rates.5,21–23 In addition, it is known that the first 3 months are the most critical for surgically related LITA-LAD conduit failure, and our follow-up period is still within that time frame.24,25 Twenty-two patients underwent TVR because of LAD disease. Coronary catheterization showed either progression of disease of the LAD or anastomosis-related issues, which was treated accordingly. One patient underwent repeat revascularization of the LAD and had an additional lesion of the circumflex coronary artery at 6 months of follow-up. This raises the question of whether the stenosis was already present when the patient was accepted for the RA-MIDCAB procedure. It is of utmost importance that when a patient is accepted for RA-MIDCAB or HCR, all lesions are treated; otherwise, incomplete revascularization will occur. We know, in conventional CABG or PCI, that incomplete revascularization is associated with an increased risk of mortality, myocardial infarction, and repeat myocardial revascularization. 6 It is known that PCI has a higher repeat revascularization rate than CABG or MIDCAB.6,7 Nevertheless, only 3 patients who underwent TVR initially underwent HCR. Our TVR rate is similar to prior reports.7,14
In 9 cases, the RA-MIDCAB was converted to conventional on-pump or off-pump CABG (2%). In this study, we have included all patients who ever underwent RA-MIDCAB in the Netherlands. It is known that the higher the experience with RA-MIDCAB and HCR, the lower the conversion rate is. Conversion rate is influenced by the experience of the institution. Nevertheless, our conversion rate is a lower than has been reported in comparable study populations by Christidis et al. and Daniel et al., at 5.7% and 5.5%, respectively.26,27
Only 21% of RA-MIDCAB patients additionally underwent HCR, because most patients referred for RA-MIDCAB had single-vessel disease. Most of our patients were young (mean age 65 ± 9 years) males (80%) with an isolated LAD lesion who did not have an increased postoperative risk. We believe that the LITA-LAD conduit is superior to PCI with stenting of the LAD and therefore we think those patients received the optimal therapy with the best long-term prognosis. This is confirmed by the meta-analysis that we performed in collaboration with our cardiologists. 7 In addition, when a patient also had a stenosis in the circumflex coronary artery or the right coronary artery, we considered HCR but also total arterial CABG. In our center, we routinely perform total arterial CABG in younger patients, but we are reluctant to treat low-grade stenosis (<80%) with an arterial graft due to the risk of inducing flow competition. 28 In those patients, we prefer a hybrid approach. In addition, we consider frailty to be an important indication for considering the hybrid approach instead of conventional CABG. It is known that HCR provides an early quality of life benefit and a faster recovery.
At 30 days postoperatively, we reported a 4.1% reoperation rate, which is higher when compared with other studies. Giambruno et al. reported a reoperation rate of 2.8% after HCR but included only reoperation for bleeding. In our study, we combined reoperation for bleeding and anastomosis-related issues. When we focus on reoperation for bleeding alone, we have a reoperation rate of 2.8%, which is similar to the reoperation rate in comparable study populations, namely, 1.8% and 2.3%.19,29,30 Nevertheless, in our study, we included the early outcomes of our first patients, which could have resulted in a higher reoperation rate for both bleeding and anastomosis-related problems. For example, 1 patient had a re-bleed from the thoracotomy site, and 1 patient had a re-bleed from the lung. These are complications due to an initial small experience with the procedure. We are aware of our higher reoperation rate, and we expect this rate to go down when we become more experienced. Noteworthy, a certain number of patients were operated on DAPT during MIDCAB because of a reversed two-staged HCR or due to unstable angina. In addition, patients received DAPT because of the severity of their coronary artery disease. It is known that the use of DAPT can increase the risk of postoperative bleeding. 31 Nevertheless, we reported a red blood cell transfusion rate of 5.7%. RA-MIDCAB and HCR are known for a reduced need in the transfusion of red blood cells due to the minimally invasive character of the procedure when compared with convention CABG. The meta-analysis by Nolan et al. reported blood transfusion rates after HCR varying from 11% to 30% perioperatively and postoperatively. 32 Our transfusion rate is lower partly because of the awareness in the participating centers of the adverse effects of the use of transfusions but also because we have a low conversion rate, which reduces the need for transfusions.
We acknowledge that this study has some limitations. First, we performed a descriptive study only and did not compare our results to patients who underwent conventional CABG or PCI. A matched comparison group could help us define patient risk profiles and lesion complexity to determine the subgroup of patients with coronary artery disease who are best eligible for RA-MIDCAB and HCR. Second, we did not differentiate between target vessel and target lesion repeat revascularization, and therefore, we did not differentiate between in-stent restenosis and anastomosis-related problems and progression of coronary artery disease. Finally, no long-term data are yet available on outcomes of RA-MIDCAB and HCR in the Netherlands.
RA-MIDCAB is a technically demanding procedure, and the clinical results depend on the experience of the team and case volumes.30,33 This study was performed in highly experienced centers. Robot-assisted harvesting of the LITA and anastomosing of the LITA-LAD conduit is a technically demanding procedure, and the clinical results might not be as good in centers with less experience.
Conclusions
RA-MIDCAB and HCR in the Netherlands appear to be safe and promising procedures. They provide a minimally invasive approach that has resulted in clinical outcomes at short-term and midterm follow-up that are in line with previous published literature. Further, multicenter, adequately powered, comparison cohort studies and randomized controlled trials are needed to definitively assess the absolute short-term, midterm, and long-term outcomes after RA-MIDCAB and HCR.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845231154046 – Supplemental material for A Nationwide Study of Clinical Outcomes After Robot-Assisted Coronary Artery Bypass Surgery and Hybrid Revascularization in the Netherlands
Supplemental material, sj-pdf-1-inv-10.1177_15569845231154046 for A Nationwide Study of Clinical Outcomes After Robot-Assisted Coronary Artery Bypass Surgery and Hybrid Revascularization in the Netherlands by Anne R. de Jong, Monica Gianoli, Hanae F. Namba, Maaike M. Roefs, Sandeep Singh, Patrique Segers, Kirolos A. Jacob and Willem J.L. Suyker in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.