
Abstract
Objective:
Robot-assisted surgery is a minimally invasive approach for repairing the mitral valve. This study aimed to assess its safety and clinical efficacy when compared with conventional sternotomy, partial sternotomy, and right minithoracotomy.
Methods:
A systematic review of peer-reviewed studies comparing robot-assisted mitral valve repair with conventional sternotomy, partial sternotomy, and right minithoracotomy was conducted following Cochrane Collaboration guidelines. Meta-analyses were performed where possible.
Results:
The search strategy yielded 15 primary studies, of which 12 compared robot-assisted with conventional sternotomy, 2 compared robot-assisted with partial sternotomy, and 6 compared robot-assisted with right minithoracotomy. The overall quality of evidence was low, and there was a lack of data on long-term outcomes. Individual studies and pooled data demonstrated that robotic procedures were comparable to conventional sternotomy and other minimally invasive approaches with respect to the rates of stroke, renal failure, reoperation for bleeding, and mortality. Robot-assisted mitral valve repair was superior to conventional sternotomy with reduced atrial fibrillation, intensive care unit and hospital stay, pain, time to return to normal activities, and physical functioning at 1 year. However, robot-assisted mitral valve repair had longer cardiopulmonary, aortic cross-clamp, and procedure times compared with all other surgical approaches.
Conclusions:
Based on current evidence, robot-assisted mitral valve repair is comparable to other approaches for safety and early postoperative outcomes, despite being associated with longer operative times. Ideally, future studies will be randomized controlled trials that compare between robot-assisted surgery, conventional surgery, and other minimally surgery approaches focusing on hard clinical outcomes and patient-reported outcomes.
Keywords
Central Message
Robot-assisted mitral valve repair is recognized as a less invasive alternative to conventional sternotomy, but literature comparing the robotic approach to other approaches is lacking. This review found comparable outcomes for robot-assisted mitral valve repair compared with conventional sternotomy, partial sternotomy, and right minithoracotomy.
Introduction
Mitral valve regurgitation (MR) from degenerative mitral valve disease is common, affecting approximately 2% of the population. 1 Depending on severity, valve lesion, and patient characteristics mitral valve repair (MVr) is the preferred surgical treatment. Traditionally, MVr has been performed via conventional sternotomy (CS). In recent years, there has been increased interest in minimally invasive surgical techniques, including robot-assisted MVr (ROB), partial sternotomy (PST), and right minithoracotomy (RMT).
A previously published review of ROB versus CS for MV surgery found that ROB was associated with shorter length of hospital stay. 2 However, literature comparing ROB to other minimally invasive strategies is lacking. This systematic review aimed to assess the safety and clinical effectiveness of ROB compared with CS, PST, and RMT for patients with degenerative MR.
Methods
A systematic review of published peer-reviewed primary clinical studies was conducted following a predetermined protocol in compliance with Cochrane guidelines and Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines (Fig. 1).3,4
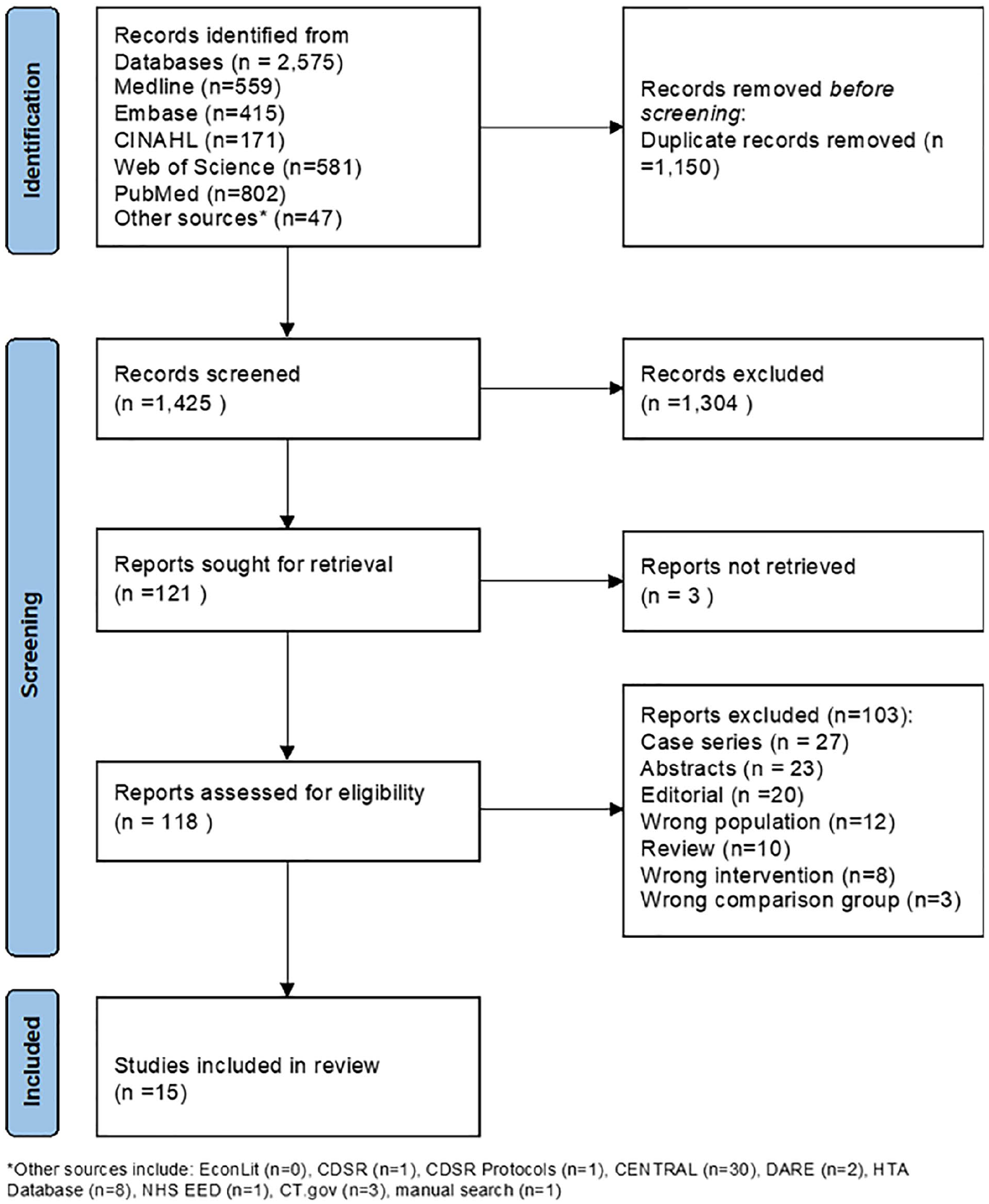
PRISMA diagram.
Literature Search
An experienced medical information specialist developed and tested the search strategies to identify studies through an iterative process in consultation with the review team. A literature review was conducted covering publications from 1964 to July 20, 2022. Another senior information specialist peer reviewed the MEDLINE strategy before execution using the PRESS Checklist. 5 All searches were performed on the following databases: Ovid MEDLINE® ALL, Embase, CINAHL, EconLit on Ebsco, Web of Science, the Cochrane Library (Wiley version), Database of Abstracts of Reviews of Effects, Health Technology Assessment, and NHS Economic Evaluation Database on Ovid, PubMed, and ClinicalTrials.gov.
The strategies combined a variety of controlled vocabulary (e.g., “Robotic Surgical Procedures,” “Mitral Valve Insufficiency,” “Mitral Valve/su [Surgery]”) and free text (e.g., “da Vinci,” “mitral annuloplasty,” “mitral repair”). A manual search of the reference lists of relevant papers located through the electronic searches was also conducted. Vocabulary and syntax across the databases were adjusted and searched without any language or date restrictions, but animal-only records and opinion pieces were removed where possible. Records from the search strategy were recorded and managed using EndNote version 9.3.3 (Clarivate Analytics, London, UK) and uploaded to Covidence. Specific details on the search strategy and the quality assessment of the included studies are provided in Supplemental Table 1.
Study Selection and Data Extraction
Two reviewers independently screened the titles and abstracts. Both reviewers assessed the full-text articles, which were subsequently retrieved for inclusion or exclusion according to predetermined eligibility criteria (Table 1). In the case of disagreements, a third party was consulted. One reviewer extracted information on key elements described in the extraction form, and the second reviewer double-checked the entries. The components in the form were study design, setting, methods, sample size, baseline characteristics of patients, details of the intervention and comparator, and outcome measures.
Study Eligibility Criteria for the Review on Safety and Clinical Effectiveness of Robot-Assisted MVr.
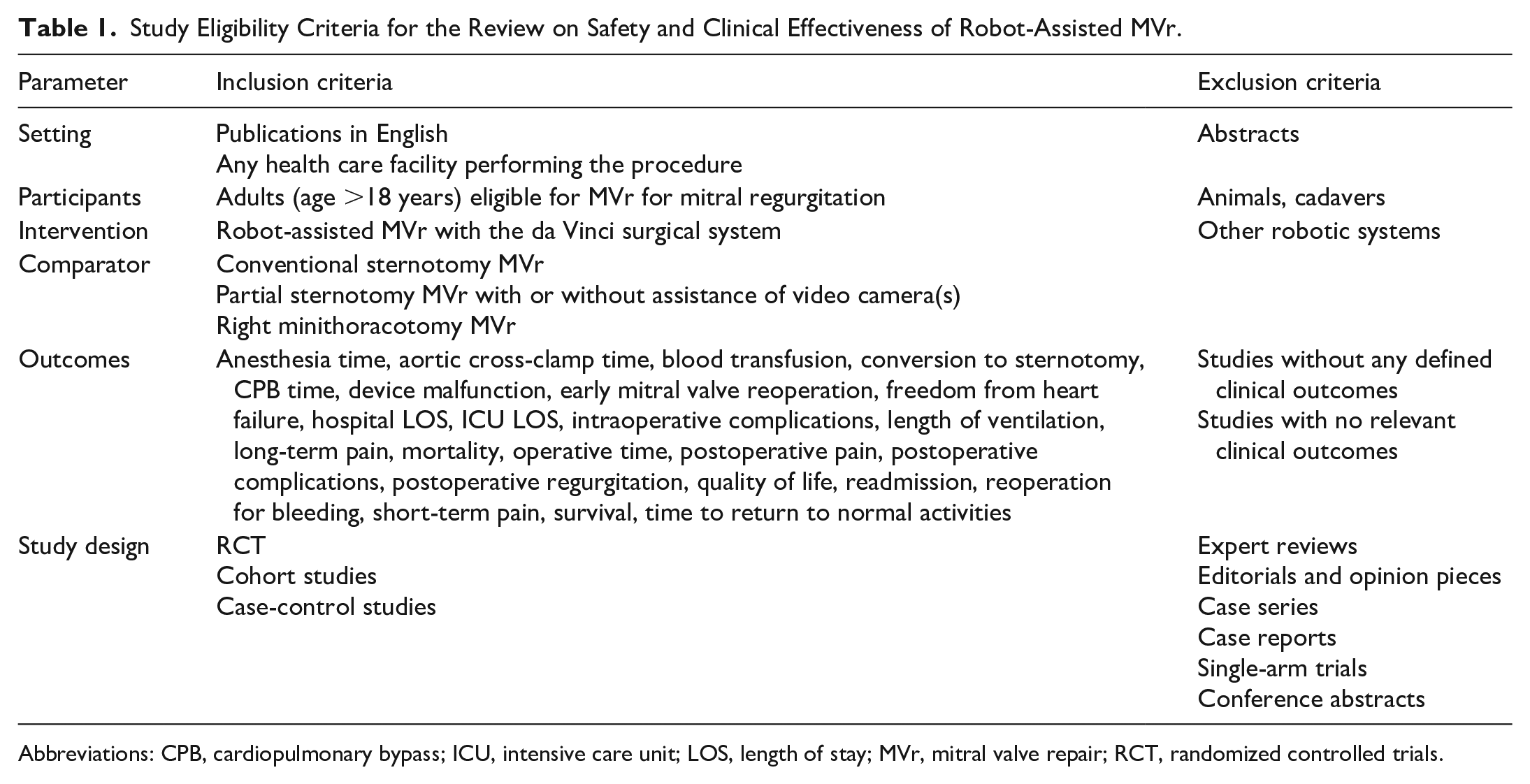
Abbreviations: CPB, cardiopulmonary bypass; ICU, intensive care unit; LOS, length of stay; MVr, mitral valve repair; RCT, randomized controlled trials.
Quality Assessment of Studies
The methodological quality of the observational studies was appraised with the Newcastle-Ottawa Scale (NOS). 6 In addition, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the overall quality of the body of evidence based on the following outcomes: length of hospital stay, reoperation for bleeding, readmission rates, stroke, operative time, postoperative pain scores, heart failure readmission, and overall survival at 1 year. 7 GRADE assessment of the included studies is presented in Supplemental Table 2, Supplemental Table 3, and Supplemental Table 4. The NOS assessment of the methodological quality of clinical studies is summarized in Supplemental Table 5.
Data Analysis and Synthesis
Data extracted from included studies were tabulated to facilitate quantitative and qualitative analyses. Characteristics of included studies and findings were synthesized narratively. In the case of multiple studies conducted in a single institution with an overlap of patients and reporting the same outcome measures, only the most recent publication with the largest sample size for data synthesis was considered. Meta-analyses were conducted using a random-effects model as described by DerSimonian and Laird. 8 A P value of <0.05 was used to determine statistical significance. Studies reporting continuous data were pooled using the mean difference between surgical groups, and those reporting categorical data were pooled using odds ratios (OR). In the case of continuous data, studies were not pooled if the mean and standard deviation were not reported. Studies were pooled only if they compared the same surgical interventions and outcome measure. In addition, these outcomes were required to be measured at the same point in time. Heterogeneity was assumed to be too substantial to pool data when the I2 statistic was greater than or equal to 50%. 3 The software Review Manager (RevMan), version 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, 2014), was used to conduct the meta-analyses.
Results
The literature search identified 2,575 citations, of which 120 were subsequently retrieved for full-text review. Fifteen studies met the eligibility criteria and were included in the systematic review (Fig. 1).9–23
Description of Included Studies
Of the 15 clinical studies included, 10 were conducted in the United States,10,12,13,15–20,23 2 in Europe,14,22 2 in Asia,9,11 and 1 in Australia. 21 Patients were recruited between 1992 and 2020, and study sample sizes ranged from 50 to 1,305 patients. Most studies compared ROB with CS (n = 12), whereas 2 studies, both from the same center, compared ROB with PST,15,19 and 6 studies compared ROB with RMT.9–11,15,17,19 None of the studies were randomized controlled trials, 1 was a prospective study, 18 and the rest were retrospective cohort studies (Table 2). Nine studies excluded patients who underwent concomitant MVr and other cardiac surgical procedures, although some made exceptions for patent foramen ovale closures and ablations for atrial fibrillation (AF).12,13,15–20,23
Characteristics of Included Studies, Summary of Baseline Demographics of Participants, and Clinical Outcomes.
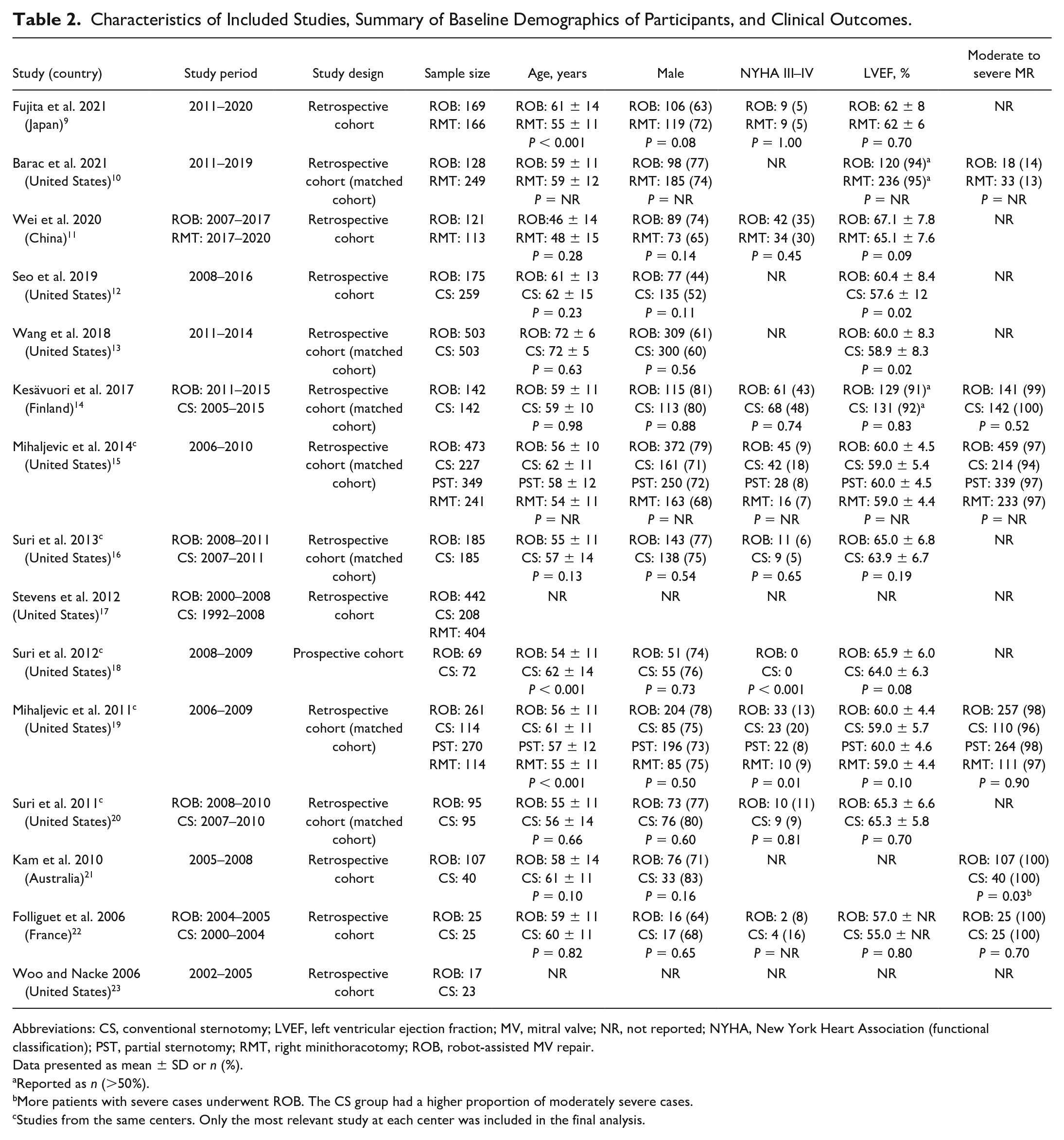
Abbreviations: CS, conventional sternotomy; LVEF, left ventricular ejection fraction; MV, mitral valve; NR, not reported; NYHA, New York Heart Association (functional classification); PST, partial sternotomy; RMT, right minithoracotomy; ROB, robot-assisted MV repair.
Data presented as mean ± SD or n (%).
Reported as n (>50%).
More patients with severe cases underwent ROB. The CS group had a higher proportion of moderately severe cases.
Studies from the same centers. Only the most relevant study at each center was included in the final analysis.
Baseline Characteristics of Patients
The mean age of participants across studies ranged from 46 to 72 years. When reported, studies had a high proportion of patients with none to mild heart failure symptoms (New York Heart Association class I and II), and the prevalence of preoperative AF varied from 1% to 33%. The mean/median left ventricular ejection fraction ranged from 55% to 67%, suggesting most studies included participants within the normal range (50% to 70%). Three studies, 2 from the same hospital, included only patients with MR involving the posterior leaflet.15,19,22 In the remaining studies, where information was available, bileaflet pathology was included, but the majority still had posterior leaflet pathology (range, 54% to 85%). Baseline patient demographics and clinical outcomes of the included studies are summarized in Table 2.
Description of Instruments Used and Procedure Performed
Six studies provided information on the model of the robot. One study used the da Vinci® Si Surgical System (Intuitive, Sunnyvale, CA, USA), 14 2 studies used different models including the latest da Vinci® Xi Surgical System (Intuitive),9,10 and the remaining 3 studies used the da Vinci® S Surgical System (Intuitive).16,18,20 In 4 studies, patients underwent unplanned MV replacement after unsuccessful repair.9,13,14,19 In 1 study, the proportion of unplanned replacements was lower in the ROB group (2%) than in the control group (10%). 13 Seven studies reported the number of surgeons performing MVr and their experience, with 3 of these studies from the same center. Four studies presented outcomes based on surgeons’ initial experience with ROB.14,16,18,20 Three studies involved experienced robotic cardiac surgeons.12,15,21
Quality Assessment of Included Studies
The overall quality of the evidence, based on GRADE, was low. Detailed results of the quality assessment are reported in the Supplemental Material. In addition, based on the NOS, the methodological quality was deemed “good” in 1 study, 13 “fair” in 7 studies,10,12,14,16,19,20,22 and “poor” in the remaining studies.9,11,15,17,18,21,23
Selection bias was likely present in all the included studies since recruitment was based on the availability of the robot technology and surgeon and patient preferences. In all studies, information on the baseline characteristics of patients was obtained from medical records or institutional databases. Seven studies used propensity scoring to match patients and to control for possible confounders. They selected age, gender, and cardiac and noncardiac comorbidities as factors to consider in the calculation of scores.10,13–16,19,20 One study assessed the outcomes of interest through a mailed survey at 1 and 2 years of follow-up. 18 The remaining studies collected such information from medical charts and institutional databases. Nine studies had an appropriate follow-up time since their purpose was to assess operative and early postoperative outcomes associated with ROB.9,11,14,16,19–23 However, 4 studies failed to provide information on follow-up times or the number of patients in each group lost to follow-up.10,17–19 Thus, the potential for attrition bias was unclear.
Safety
Conversion
A meta-analysis comparing ROB and RMT found no significant difference between both minimally invasive approaches (Fig. 2). One study compared rates of conversion to CS for ROB, PST, and RMT. This study reported rates of 3%, 2%, and 1% for ROB, PST, and RMT, respectively (P value was not provided). 15 Rates of conversion to CS ranged from 0% to 9%.9–11,14,15,22
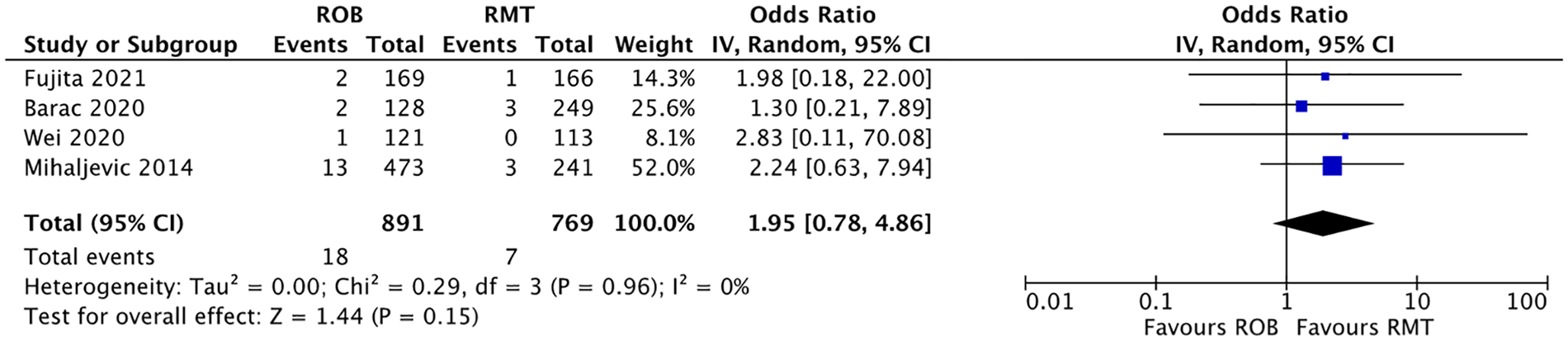
Meta-analyses of conversion to conventional sternotomy from ROB versus RMT studies. CI, confidence interval; RMT, right minithoracotomy mitral valve repair; ROB, robot-assisted mitral valve repair.
Postoperative complications
Three studies demonstrated that rates of empyema, femoral and coronary artery occlusion, hypoperfusion, and gastrointestinal complications were similar for ROB, CS, PST, and RMT.14,16,19 However, 1 study observed statistically significantly higher rates of pleural effusion in patients who had CS (8%) or PST (9%) compared with those who underwent ROB (0% to 2%). 19 No statistically significant differences in pleural effusion rates between ROB and RMT were found.11,19
Myocardial infarction
Two studies of ROB versus CS assessed postoperative myocardial infarction (MI) and found no difference between ROB and CS. Rates varied between 0% and 2%.14,16 One study found no statistically significant differences between ROB (1%) and RMT (0%). 9 No information on rates of MI following PST was provided.
Atrial fibrillation
Pooled analysis showed a reduction in the odds of AF with ROB compared with CS (OR = 0.61, 95% confidence interval [CI]: 0.50 to 0.74; Fig. 3). One study reported significantly higher AF rates after PST than ROB (35% vs 22%) but no difference in rates between ROB and RMT. 19 Overall, the rates of AF varied from 13% to 40%.
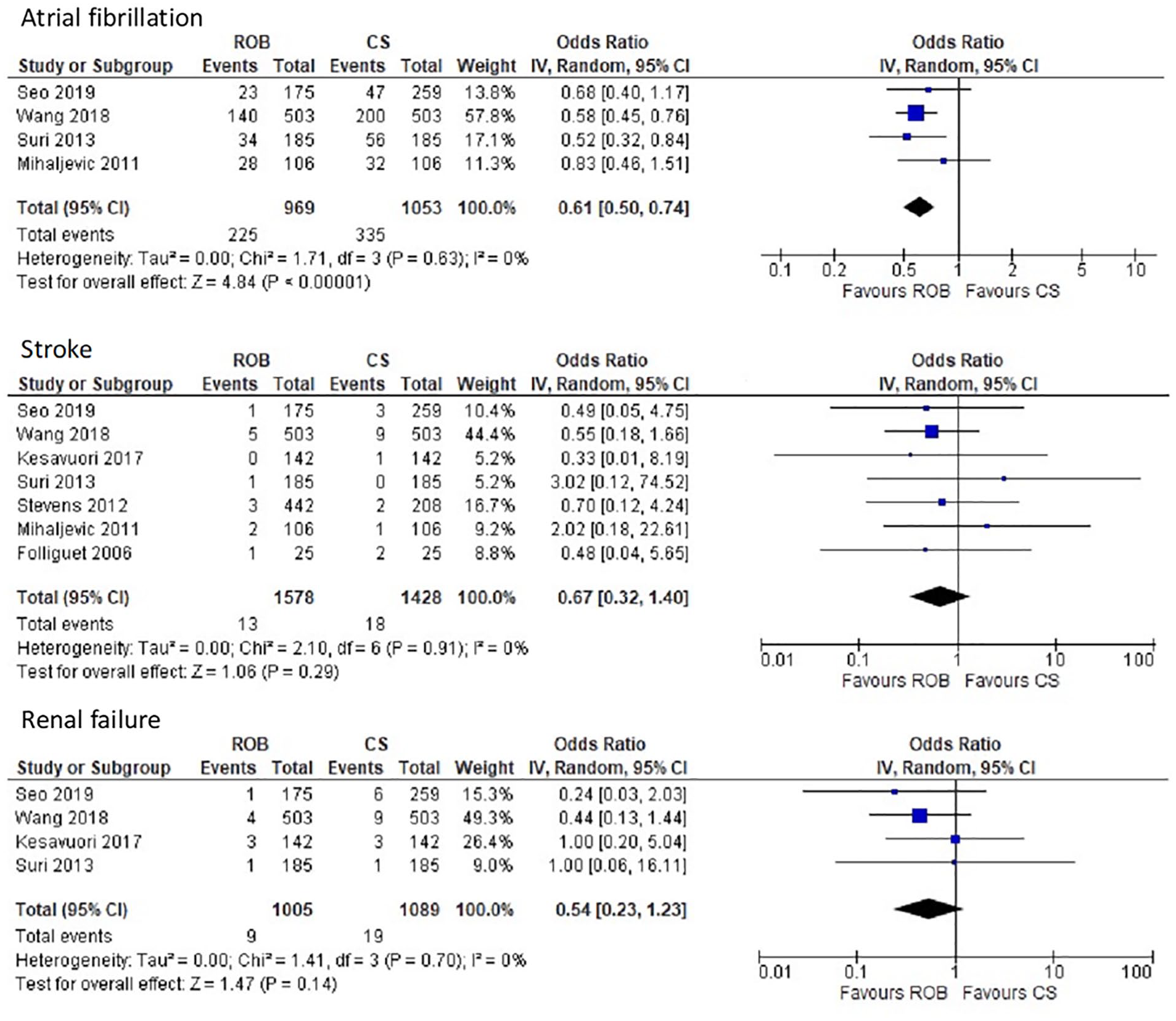
Meta-analyses of safety outcomes from ROB versus CS studies. CI, confidence interval; CS, conventional sternotomy mitral valve repair; ROB, robot-assisted mitral valve repair.
Stroke
Nine studies reported rates of stroke after surgery were low and ranged from 0% to 8%.9,10,12–14,16,17,19,22 The pooled estimates from the meta-analysis showed no significant difference in rates between ROB and CS (Fig. 3). Four studies reported similar stroke rates, ranging from 0% to 2%, between ROB and RMT,9,10,17,19 and 1 study reported the same rates for ROB and PST (3%). 19
Infection
Studies comparing ROB with CS found low and comparable rates of sepsis,12,14,18 pneumonia,12–14 and wound infection.12–14,18 Two studies also reported similar rates of wound infection between ROB and RMT.9,11 None of the studies comparing ROB with PST provided information on infection rates.
Renal failure
The rates of renal failure after MVr were low (range, 0% to 2%), and the meta-analysis found no significant differences between ROB and CS (Fig. 3). One study found no statistical difference in renal failure rates after ROB and RMT. 9
Clinical Efficacy: Operative Outcomes
Operative time
Five studies reported significantly longer operative times for ROB (mean/median range, 239 to 387 min) than for CS (mean/median range, 188 to 278 min).12,14,19,21,22 One study found that operative time for ROB was significantly longer than for PST (mean, 387 vs 277 min) and RMT (mean, 387 vs 327 min). 19 However, a second study reported a significantly longer time for RMT (mean, 233 min) than ROB (mean, 210 min). 9
Cardiopulmonary bypass time
Eight studies reported significantly longer cardiopulmonary bypass (CPB) times during ROB than CS, with the mean/median times ranging from 113 to 239 min and 48 to 162 min, respectively.13,14,17,19–23 CPB times were also significantly longer for ROB when compared with PST (median, 76 min). 19 Five studies compared CPB times during ROB and RMT procedures. While 3 studies found significantly longer times for ROB,10,17,19 1 study found no difference between interventions, 9 and another study reported longer CBP times for RMT. 11
Aortic cross-clamp time
Twelve studies assessed aortic cross-clamp time. Across studies, the mean/median time during ROB varied from 81 to 152 min. However, apart from 2 studies,9,11 all studies reported significantly longer times for ROB than CS (range, 36 to 110 min), PST (59 min), and RMT (range, 66 to 119 min).12–14,17,19–23
Clinical Efficacy: In-Hospital Postoperative Outcomes
Duration of invasive ventilation
Seven studies provided information on the length of ventilation. Five found no significant differences in length of ventilation and number of patients ventilated for more than 24 h between ROB and CS.13,16,19,21,22 However, 1 study reported the median length of ventilation was significantly longer (2 h) in ROB than in CS patients. 14 One study that compared ROB with PST and RMT found no significant differences in the number of patients requiring ventilation 24 h after surgery. 19 However, another study comparing ROB with RMT found significantly more patients required longer invasive ventilatory times after a robotic procedure. 11
Blood transfusion
Four studies comparing ROB with CS reported no significant differences in blood transfusions between approaches.14,19,21,22 However, 2 studies found that CS was associated with significantly higher transfusion rates based on the absolute number of patients requiring more than 2 units of packed red blood cells.12,16 There were no significant differences between ROB and PST. 19 Two studies comparing ROB and RMT presented mixed results, with 1 study reporting higher blood transfusion rates after ROB 11 and the second study finding no differences among surgical techniques. 19
Reoperation for bleeding
Meta-analyses comparing ROB with CS and RMT found no significant differences between approaches (Fig. 4). One study also found no significant differences between ROB and PST. 19
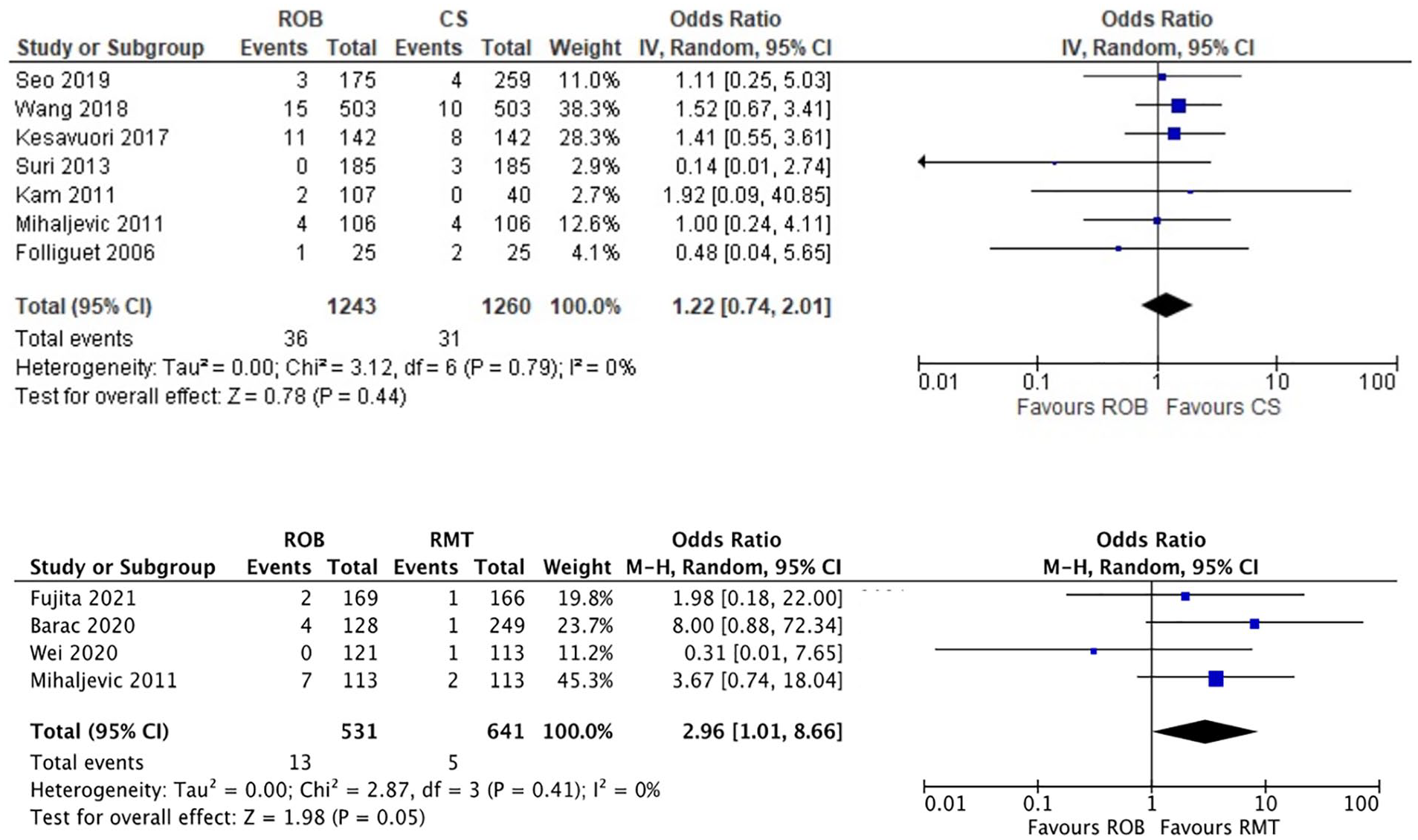
Meta-analysis of reoperation for bleeding from ROB versus CS and ROB versus RMT studies. CI, confidence interval; CS, conventional sternotomy mitral valve repair; RMT, right minithoracotomy mitral valve repair; ROB, robot-assisted mitral valve repair.
Length of intensive care unit stay
Six studies demonstrated that intensive care unit (ICU) lengths of stay were shorter for ROB than CS, with 5 reporting that differences were significant.12–14,16,21,22 The mean/median lengths of stay ranged from 24 to 84 h for ROB and 24 to 144 h for CS. However, 2 studies, in which 1 reported a significant difference, found longer stay after ROB than RMT.9,11
Length of hospital stay
Eight studies compared length of hospital stay between ROB and CS. Seven of them found that ROB was associated with significantly shorter length of stay than CS.12,13,16,17,19,21,22 One study reported the same median length of stay for both procedures. 14 The mean/median length of stay for ROB patients ranged from 3 to 7 days, whereas for CS patients, it ranged from 5 to 11 days. A shorter length of stay was also reported for ROB compared with PST. 19 Findings from studies comparing ROB with RMT were mixed. Half of the studies reported significantly shorter hospitalization after ROB,17,19 and the remaining 2 studies reported either comparable stays or more extended hospitalizations with the robotic procedure.9,10
Clinical Efficacy: Early Postoperative Outcomes
Early reoperation
Studies reported similar reoperation rates for ROB, CS, and RMT (range, 0% to 7%), but measures were taken at different points in time.11–14,16,22 None of the studies assessed early reoperation rates after PST.
Postoperative residual MR
Studies of ROB versus CS, ROB versus PST, and ROB versus RMT reported postoperative MR at different timepoints after surgery but found no significant differences between ROB and CS.9,11–14,19–22
Mortality
Three studies comparing ROB with CS reported no deaths during surgery.16,19,21 Neither meta-analysis comparing 30-day mortality of ROB versus CS and ROB versus RMT found significant differences between approaches (Fig. 5). One study of ROB versus PST reported no intraoperative deaths during surgery. 19
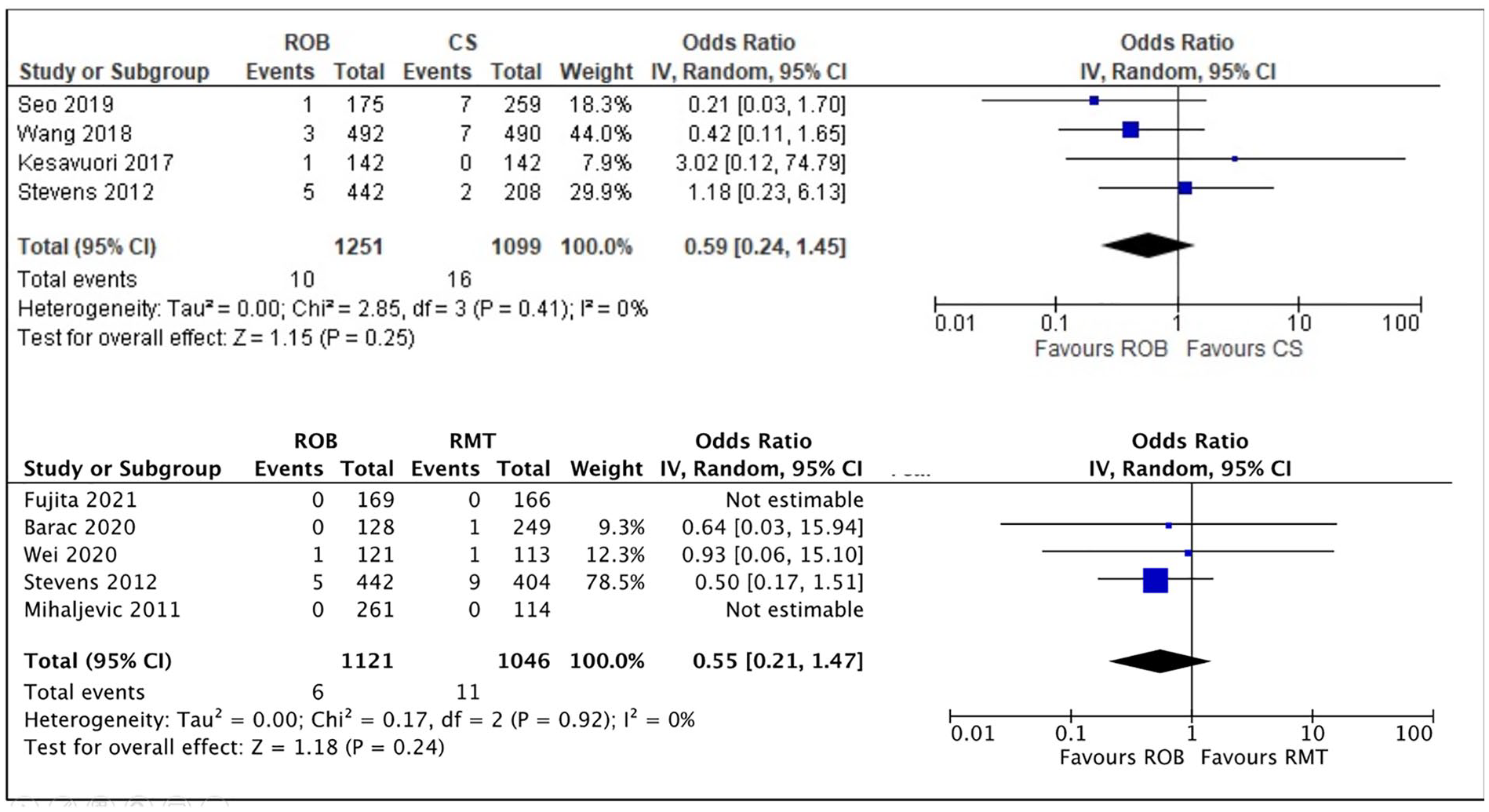
Meta-analyses of 30-day mortality from ROB vs CS and ROB vs RMT studies. CI, confidence interval; CS, conventional sternotomy mitral valve repair; RMT, right minithoracotomy mitral valve repair; ROB, robot-assisted mitral valve repair.
Clinical Efficacy: Long-Term Postoperative Outcomes
One study found no differences in the 3-year heart failure readmission rates between ROB and CS (hazard ratio [HR] = 1.4, 95% CI: 0.5 to 2.5). 13 The 3-year mortality rate reported in 1 study was not different between ROB and CS (HR = 1.2, 95% CI: 0.7 to 2.2), 13 and the 5-year survival rate in another study was not statistically different between ROB (96% ± 3%) and RMT (97% ± 1%). 10
Clinical Efficacy: Patient-Reported Outcomes
One study reported the proportion of patients without pain 4 days after surgery. It was similar for those who underwent ROB, CS, and PST but lower among patients who had RMT. 19 Although none of the studies assessed short-term pain after surgery, 1 study examined the frequency and severity of chest pain at 1 and 2 years after ROB and CS. 18 While ROB was associated with significantly less pain at 1 year, the difference was no longer obvious at 2 years. 18 None of the studies assessed long-term pain following treatment with the other minimally invasive surgical approaches.
Two studies of ROB versus CS reported time to return to work after MVr.15,18 In both studies, times were shorter following ROB, and in 1 study, the difference was statistically significant. 18 The single study that compared ROB to other minimally invasive approaches found that the median time to return to work for ROB was 35 days, while PST and RMT were 56 and 42 days, respectively. 15
Finally, 1 study comparing ROB and CS assessed quality of life through different instruments at 1 and 2 years after surgery. CS patients experienced significantly more fatigue-related symptoms and reported worse physical functioning at 1 year. However, no significant differences were found at 2 years. Mental health measures were similar for ROB and CS at both follow-up intervals. 18
Discussion
For the past 3 decades, MVr using a CS approach has resulted in excellent clinical outcomes for patients with degenerative MV disease. Recently, minimally invasive approaches have become more common, as they have purported benefits of shorter hospital stay and quicker recovery. Perhaps the least invasive approach is robot-assisted MVr, which may also be the least common. Many studies support the safety of this innovative approach.24–42 In addition to confirming the safety of robot-assisted MV surgery, some of these studies have demonstrated that ROB can be used in patients with previous sternotomies, 25 those with a high body mass index, 27 the elderly, 28 those with complex valvular pathologies, 29 and in concomitant procedures.30,34 Indeed, there is also evidence that ROB can be undertaken in lower volume 24 and nonacademic centers without compromising outcomes. 40 In some instances, groups have been able to specifically address the learning curve and the technological evolution associated with ROB.31,32 Collectively, given the clinical outcomes and the continued improvement in ROB devices, these studies should encourage further adoption of ROB in the appropriate patient population.
Nevertheless, a few studies have compared ROB to other minimally invasive options for MVr. Herein, we have conducted a systematic review and meta-analysis, determining that, despite longer operative times, ROB was comparable to other surgical approaches with respect to safety and early postoperative outcomes. 43 Furthermore, there is some evidence that ROB promotes an earlier return to work and shorter length of ICU and hospital stay. Variations in surgical technique, surgeon experience, limited enrollment, and hospital selection protocols produce selection bias and limit the ability to draw firm conclusions from this generally poor-quality evidence. While these results are encouraging, there is a lack of evidence on long-term and patient-reported outcomes such as overall survival, rates of heart failure, and cardiac-specific health-related quality of life.
The acceptance of robotic systems has been limited in cardiac surgery compared with other specialties. The 2018 trend analysis from the Society of Thoracic Surgeons Adult Cardiac Surgery Database reported that only 11.5% of MVr was performed with robotic technology, up to 20% were through a minimally invasive approach, 44 and 68% were CS. 45 There are many reasons for this, including the cost of robotic technology, the technical complexity, and the limited number of high-quality studies suggesting an advantage to the technique. 13 While our study found some benefits for patients undergoing ROB, it is unclear if this approach offers any advantage for surgeons. Further studies are needed to also understand surgeon attitudes and perspectives on ROB.
It is important to acknowledge the limitations of this study. First, no randomized clinical trial was identified, and all but 1 study were retrospective cohort studies. Thus, in many cases, the groups were not similar, and confounding variables may have been present. Second, the overall quality of evidence comparing ROB to other surgical approaches was low, with only 3 studies comparing ROB to other minimally invasive techniques. This limited our ability to make strong conclusions regarding the advantages and disadvantages of ROB relative to other MVr surgical techniques. Third, the generalizability of the findings of this review to all patients requiring MVr and health care settings is limited. We found only 1 study reporting results from multiple health care centers of patients who were 65 years and older. The remaining studies were from single centers with relatively young patients (aged 46 to 63 years) who did not require concomitant cardiac procedures. Fourth, the difference in surgical techniques and surgeon experience was broad, which might have also impacted the outcomes.14,46–49 Finally, since the studies included in this systematic review and meta-analysis span from before 2006 to 2021, it is important to highlight that ROB technology has changed significantly over this period. It is plausible and prudent to assume that earlier techniques and instruments may not be routinely or commonly used in present clinical practice. Likewise, some of the earlier ROB practitioners are no longer actively performing ROB, so differences in outcomes should be considered in the context of different eras. As this area of cardiac surgery grows and evolves, future studies may be able to assess how different iterations and eras of ROB and ROB operators influenced outcomes.
Conclusions
Robot-assisted MVr appears to be safe when compared with other surgical approaches, including minimally invasive RMT. There is some evidence that it may offer benefits of shorter ICU and hospital stay and quicker return to work, with less pain. However, as the procedure is relatively new, the long-term outcomes are not clear, and the quality of outcome data is poor. It is essential that patients are carefully followed after ROB procedures, and future randomized trials should be designed to compare ROB to CS-based and other minimally invasive approaches for degenerative MV disease. In addition to hard clinical outcomes, such trials should also incorporate factors such as postoperative recovery, rehabilitation, and quality of life.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845221141488 – Supplemental material for A Systematic Review and Meta-Analysis of Robot-Assisted Mitral Valve Repair
Supplemental material, sj-pdf-1-inv-10.1177_15569845221141488 for A Systematic Review and Meta-Analysis of Robot-Assisted Mitral Valve Repair by Ali Fatehi Hassanabad, Fernanda N. I. Nagase, Ameen M. Basha, Fadi Hammal, Devidas Menon, William D. T. Kent, Imtiaz S. Ali, Jeevan Nagendran and Tania Stafinski in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Supplemental Material
Visual abstract – Supplemental material for A Systematic Review and Meta-Analysis of Robot-Assisted Mitral Valve Repair
Supplemental material, sj-pptx-2-inv-10.1177_15569845221141488 for A Systematic Review and Meta-Analysis of Robot-Assisted Mitral Valve Repair by Ali Fatehi Hassanabad, Fernanda N. I. Nagase, Ameen M. Basha, Fadi Hammal, Devidas Menon, William D. T. Kent, Imtiaz S. Ali, Jeevan Nagendran and Tania Stafinski in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by a financial contribution from the Government of Alberta. The views expressed herein do not necessarily represent the official policy of the Government of Alberta.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.