
Abstract
Descending thoracic aortic thrombus (DTAT) is an under-recognized source of systemic emboli with potential catastrophic consequences. Imaging modalities such as echocardiography, computed tomography, magnetic resonance imaging, and angiography can help identify and characterize the extent of embolic events. Established guidelines regarding the management of DTAT are currently lacking. Multiple treatment modalities are available; however, the effectiveness of each approach remains to be determined. In this study, we performed a review to examine the clinical presentation, diagnostic methods and findings, and outcomes of various treatment options for patients with DTAT. Medical management is the least invasive and most frequently chosen initial approach, offering a high reported success rate, whereas endovascular therapy can have a role in thrombus exclusion should conservative management fail.
Medical management is the least invasive and most frequently chosen initial approach for DTAT, whereas endovascular therapy can have a role in thrombus exclusion should conservative management fail.Central Message
Introduction
Descending thoracic aortic thrombus (DTAT) is a rare entity that can lead to systemic arterial thromboembolism, a serious and potentially life-threatening condition. 1 Therefore, early detection and treatment are critical for a good prognosis. Although DTAT could be detected incidentally, most cases present with peripheral embolic events, which makes early detection challenging.2–6 Recent developments in diagnostic imaging have contributed significantly to the accurate diagnosis of various aortic pathologies such as DTAT, including echocardiography, computed tomography (CT), angiography, and magnetic resonance imaging (MRI).7–11 Although thrombi in the ascending aorta, aortic arch, and abdominal aorta have all been previously described, reported thoracic thrombi were most commonly (38.0%) located in the descending thoracic aorta. 12 Currently, there are no established guidelines on the management of DTAT.13–16 Different approaches have been reported with varying degrees of invasiveness and effectiveness, ranging from conservative medical management to endovascular intervention and open surgery. 1
The present review aims to describe and summarize the clinical presentation, diagnostic methods, treatment, and reported outcomes for thrombi localized in the descending thoracic aorta.
Methods
Literature Search Strategy
Articles were identified following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines through electronic searches of Ovid Medline, Embase, Cochrane Database of Systematic Reviews, and Scopus databases, performed in August 2020. Studies describing DTAT were found using a combination of variations of the key terms “thrombus,” “aorta,” “descending thoracic aorta,” “atheroma,” “thromboembolism,” “emboli,” and relevant medical subject heading (MeSH) terms. A closely related but distinct condition termed “shaggy aorta” (SA) has been increasingly described in the literature.17–19 SA refers to an aorta with irregular mural thrombus as demonstrated on imaging studies. Because of severe atherosclerotic process, the aorta becomes extremely degenerate and friable and likely to cause atheroembolism spontaneously or during procedural manipulations.20,21 SA is a different entity from floating aortic thrombus in terms of etiology and management. Therefore, articles describing SA were not included in this study. In addition, relevant sources cited within retrieved articles were also reviewed for further identification of potentially relevant publications. After removal of duplicates, articles were screened by 2 independent contributors using the eligibility criteria, as described below.
Selection Criteria
Inclusion and exclusion criteria were determined before data collection. Articles were limited to those involving human subjects and written in English. We included only contemporary studies, defined as published in the year 2000 and onward, with clear descriptions of the management strategy used for the DTAT. Cases describing patients younger than 18 years and those with congenital heart lesions, structural heart problems, aortic dissection pathologies, or previous cardiac surgical operations were excluded. Our goal was to describe the clinical experience, management, and outcomes of patients with de novo DTAT rather than those with preexisting cardiac pathologies, as these complex cases are often managed on a case-by-case basis. Studies reporting intracardiac thrombi, or thrombi located in the ascending aorta, aortic arch, abdominal aorta or pulmonary artery were also excluded.
Data Extraction
All data were manually extracted from article texts, tables, and figures. Variables included study sample size, age, sex, cardiovascular risk factors, presence of coagulation disorders, symptoms at presentation, diagnostic modalities, thrombus characteristics, medical management, surgical management, follow-up, and early and late outcomes. Discrepancies were resolved by group discussion and consensus.
Descriptive statistics were performed using GraphPad Prism version 8.4.3 (GraphPad Software, La Jolla, CA, USA). Categorical variables were presented as counts (n) and frequency (%). Continuous variables were presented as mean ± standard deviation if normally distributed or median and interquartile range (IQR) if not normally distributed.
Results
A total of 1,611 articles were identified after removing duplicates, with 51 articles included in this study involving 64 patients.
Clinical Presentation
In terms of patient demographics, DTAT can present at various ages, ranging from 21 to 77 years. The median age at presentation was 54 years (Table 1). DTATs were more commonly reported in female patients (59% of cases) than in male patients.
Demographic and Clinical Presentation of Previously Described Cases of Thrombus in the Descending Thoracic Aorta.
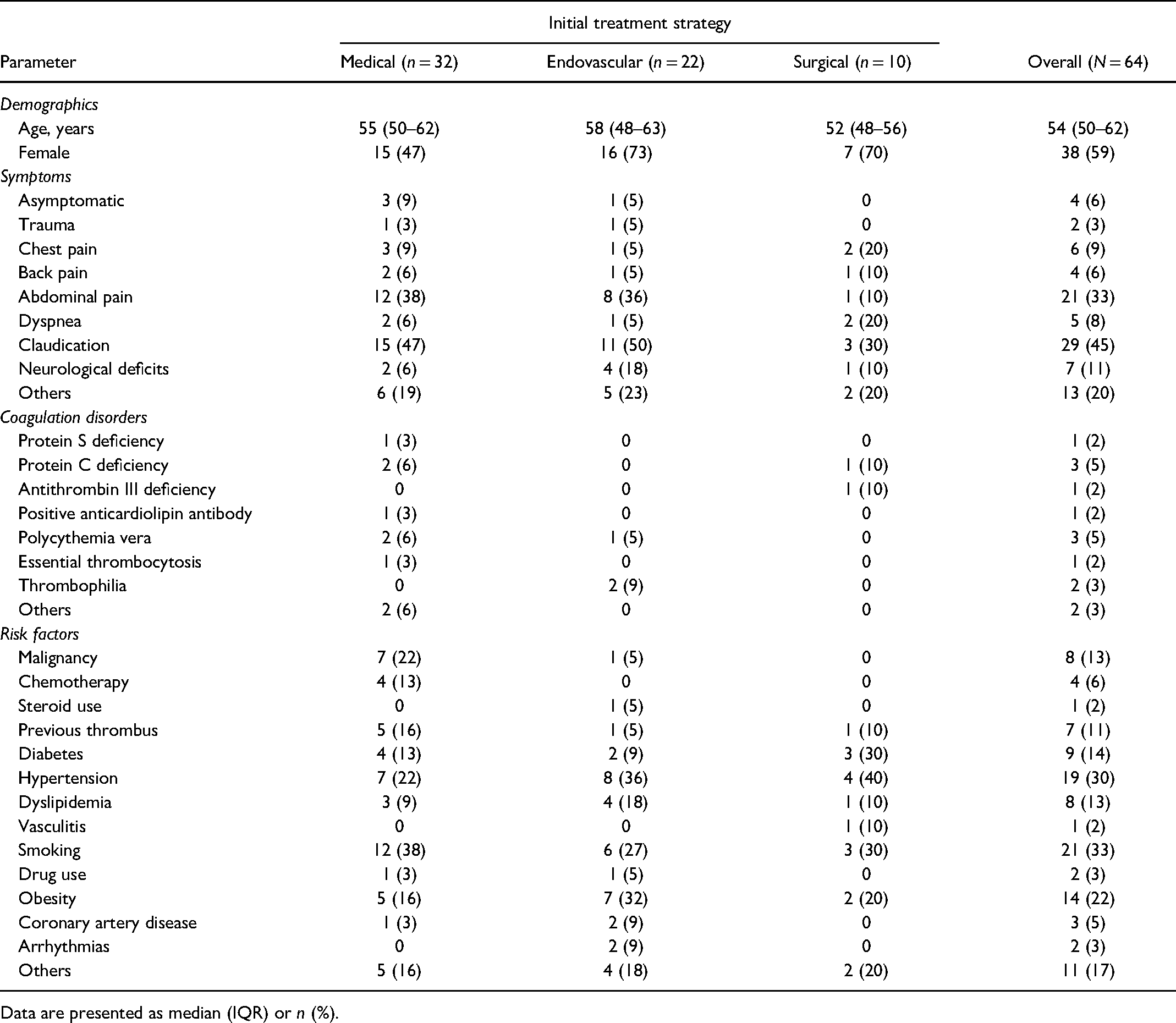
Data are presented as median (IQR) or n (%).
Although patients with DTAT can be asymptomatic, most reported cases presented with manifestations of thromboembolism. Claudication symptoms such as extremity pain, ischemic rest pain, skin discoloration, gangrene, and necrosis were the most common initial presentation, accounting for 45% of the cases. Abdominal pain was also reported in 33% of patients, followed by neurologic deficits such as sudden visual impairment, dysarthria, aphasia, paraplegia, or paresthesia in 11% of cases. Less common initial presentations included chest pain, dyspnea, and back pain. Three percent of DTAT was identified in the context of traumatic events.
Hypercoagulable states can contribute to the occurrence of DTAT. Protein C deficiency and polycythemia vera have each been reported in 5% of cases. Other coagulation disorders that were identified in patients with DTAT include thrombophilia, protein S deficiency, antithrombin III deficiency, positive anticardiolipin antibody, and essential thrombocytosis.
As with other types of thromboembolic diseases, various risk factors for cardiovascular disease and arterial thrombosis were reported in patients with DTAT. Smoking (33%), hypertension (30%), obesity (22%), diabetes (14%), and dyslipidemia (13%) were the most commonly reported cardiovascular risk factors among the included cases. With regard to thrombosis risk factors, malignancy and chemotherapy were associated with 13% and 6% of DTAT cases, respectively. Other conditions such as previous thromboembolism, vasculitis, and steroid or drug use have also been described in the context of DTAT.
Diagnosis
Echocardiography, CT, MRI, and angiography have all been used for the diagnosis of DTAT (Table 2). CT and CT angiography were the most frequently used imaging (78%), although the diagnosis of DTAT was often revealed on transesophageal echocardiography (TEE), which was used in 64% of the cases. Despite its great diagnostic value, TEE was unable to detect DTATs that were identified on CT imaging in 2 cases. In contrast, transthoracic echocardiography (TTE) was performed in 16% of patients as part of the initial workup for potential aortic sources of arterial embolism. Multiple imaging studies were often necessary to confirm the diagnosis of DTAT and to identify the extent of thromboembolic events.
Diagnostic Findings in Previously Described Cases of Thrombus in the Descending Thoracic Aorta.
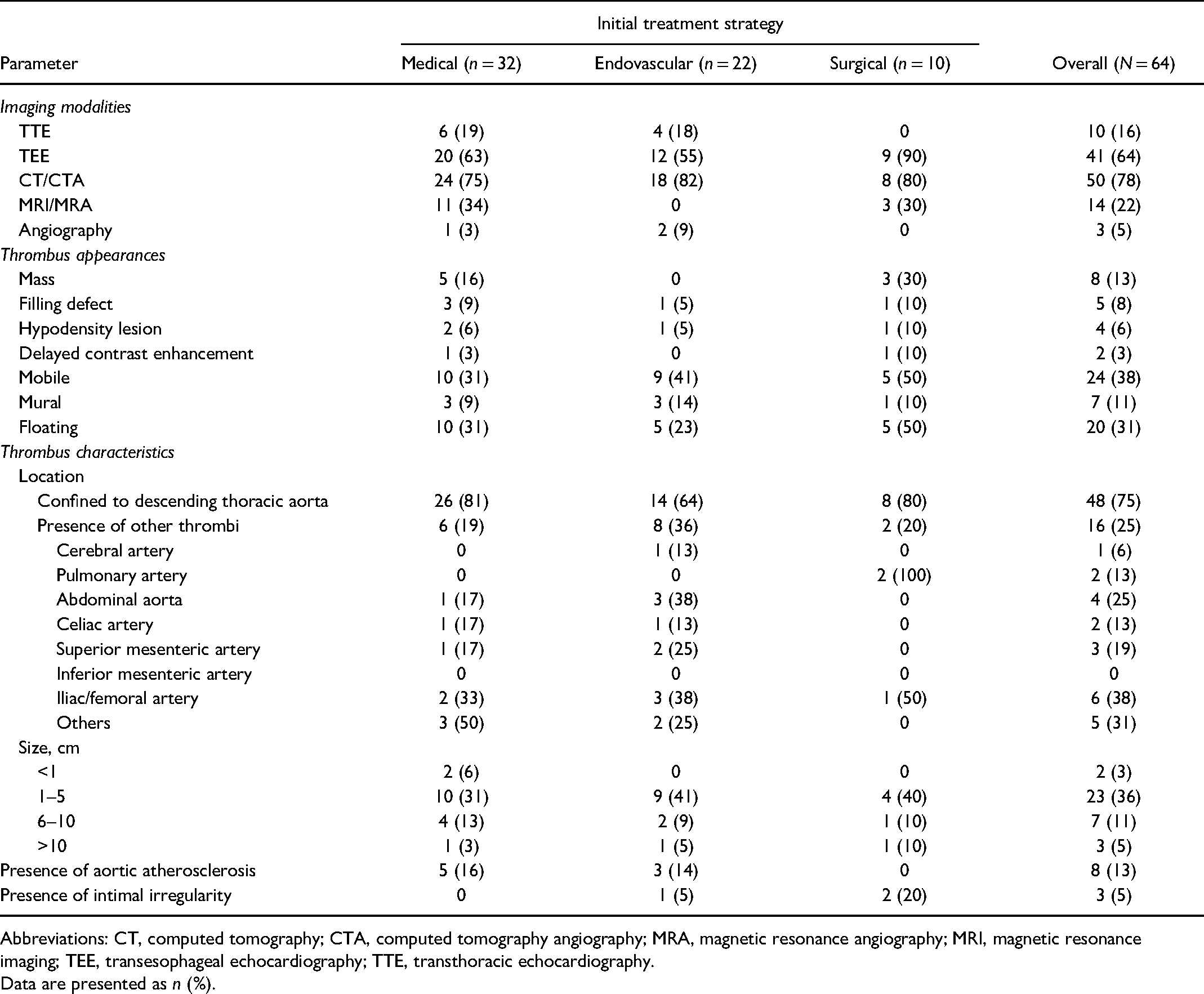
Abbreviations: CT, computed tomography; CTA, computed tomography angiography; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
Data are presented as n (%).
DTAT can manifest in different shapes on imaging. DTAT was described as a mass, a filling defect, and a hypodensity lesion in 13%, 8%, and 6% of cases, respectively. Delayed contrast enhancement was observed in 3% of the cases. Most reported DTAT cases were either mobile (38%) or floating (31%). The definition and characterization of the floating DTATs were not available on the reported cases. Mural thrombus was identified in 11% of patients.
Most reported DTAT cases were confined to the descending thoracic aorta (75%). Other thrombi were identified in 25% of cases. Distally, 38% were located in the iliac or femoral artery, 25% in the abdominal aorta, 19% in the superior mesenteric artery, and 13% in the celiac artery. Thrombi in the pulmonary artery were found in 13% of cases. Retrograde embolism was reported in 1 case with a thrombus identified in the cerebral artery.
With regard to thrombus size, 3% of reported DTATs were less than 1 cm, 36% were 1 to 5 cm, 11% were 6 to 10 cm, and 5% were greater than 10 cm. Aortic atherosclerosis was found in 13% of patients. In addition, 5% of patients also showed aortic intimal irregularity on imaging studies.
Management
Multiple treatment options with varying degrees of invasiveness are available for the management of DTAT, although established guidelines are lacking. Current treatment approaches include conservative management, endovascular intervention, and surgery. Most patients in this review received conservative medical management (50%) as the initial approach. Endovascular intervention was the treatment of choice in 34% of cases, whereas the remaining 16% were managed surgically.
Conservative management
Conservative management was frequently used as the initial treatment strategy in patients diagnosed with DTAT. This approach was also recommended for patients who were not surgical candidates or those who did not wish to receive invasive treatment. Antithrombotic agents were administered in most patients, namely, 30 of the 32 cases (94%; Table 3). All 30 patients (100%) received anticoagulant medication, whereas 5 patients (17%) additionally received an antiplatelet drug. Thrombolytic therapy using streptokinase or alteplase was reported in 2 of the 32 cases (6%). Information on maintenance therapy was scarce, with only 5 of 32 cases (16%) explicitly mentioning long-term antithrombotic therapy using anticoagulants after initial treatment. The length of hospital stay ranged from 14 to 28 days, with a median of 16 days.
Conservative Treatment and Outcomes of Thrombus in the Descending Thoracic Aorta.
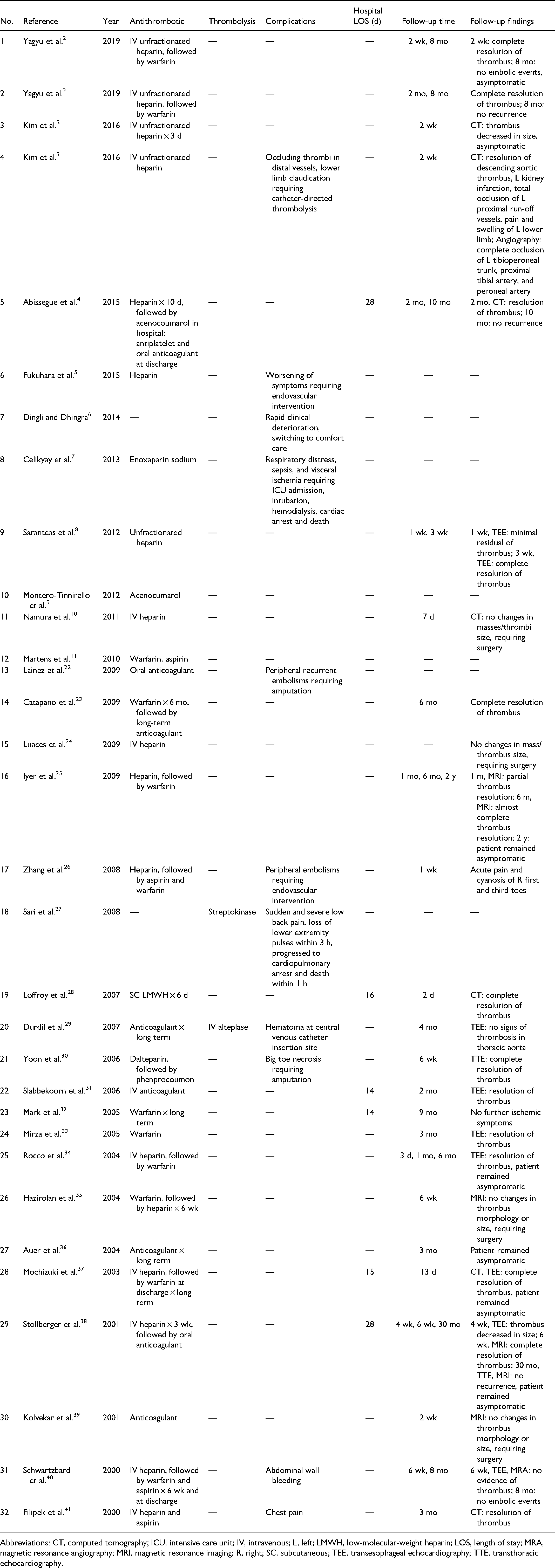
Abbreviations: CT, computed tomography; ICU, intensive care unit; IV, intravenous; L, left; LMWH, low-molecular-weight heparin; LOS, length of stay; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; R, right; SC, subcutaneous; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
Endovascular management
Indications for endovascular intervention were mentioned in 12 cases (Table 4). Among these cases, most DTATs were managed with an endovascular intervention to prevent embolic events (58%, 7 of 12 cases). The stability of the patient's clinical condition, such as having multiple embolic events or a rapidly deteriorating condition, was an indication for intervention in 2 cases (17%). Thrombus location and mobility were also taken into consideration when deciding upon the most appropriate treatment approach (17%, 2 of 12 cases). In some cases, failure of conservative management or recurrent thrombus after surgical thrombectomy necessitated further intervention (25%, 3 of 12 cases). Endovascular management was also selected in cases in which antithrombotic therapy was contraindicated and the patient was not fit for surgery (8%, 1 of 12 cases). In some situations, the lack of underlying aortic pathology may favor an endovascular approach as opposed to open surgery (8%, 1 of 12 cases). In addition, endovascular management was performed in cases of diagnostic uncertainty, for example, when aortic dissection could not be ruled out (8%, 1 of 12 cases).
Endovascular Treatment and Outcomes of Thrombus in the Descending Thoracic Aorta.
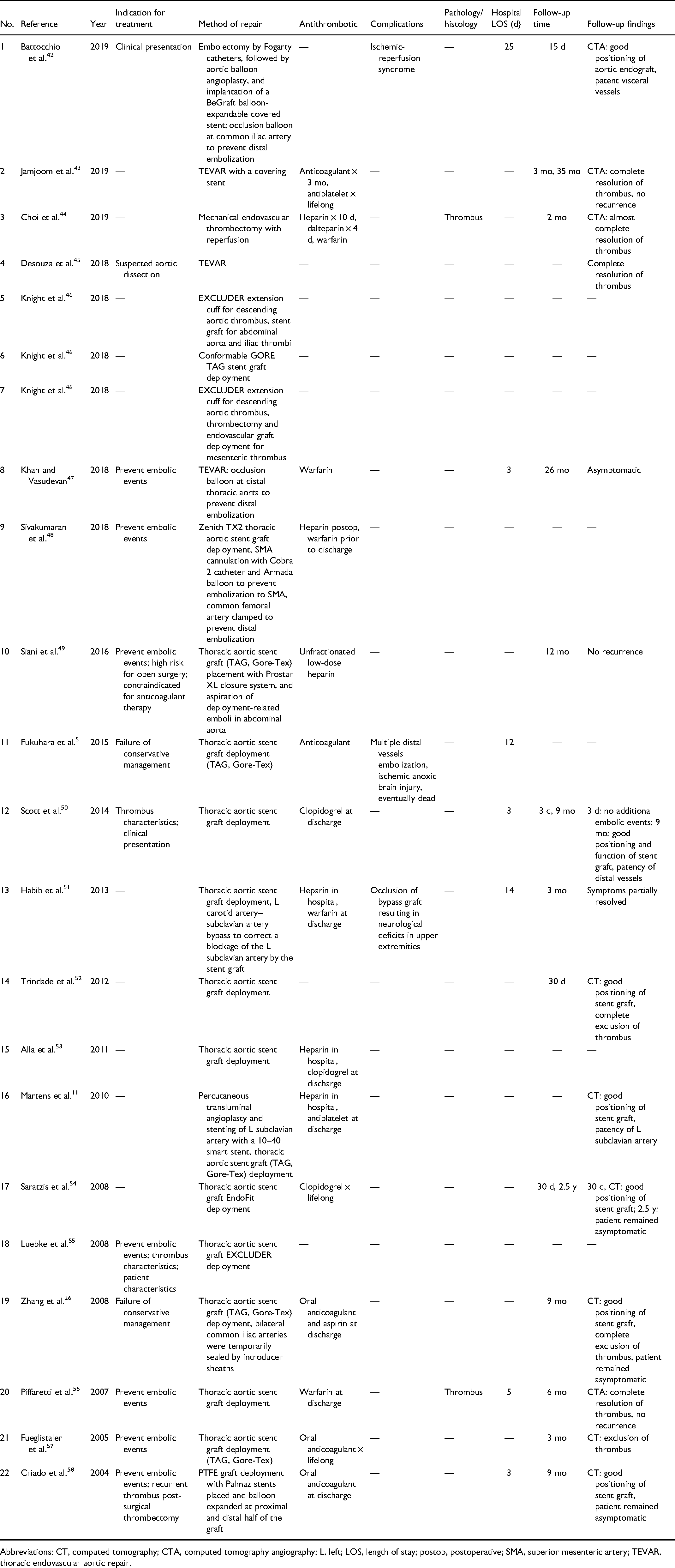
Abbreviations: CT, computed tomography; CTA, computed tomography angiography; L, left; LOS, length of stay; postop, postoperative; SMA, superior mesenteric artery; TEVAR, thoracic endovascular aortic repair.
Thoracic endovascular aortic repair (TEVAR) using stent graft was reported in 21 of 22 cases (95%) to exclude DTAT. Mechanical endovascular thrombectomy without stent graft implantation was used in only 1 patient (5%). Antiembolization devices in the forms of occlusion balloons (3 cases) or introducer sheaths (1 case) were used in 4 of 22 cases (18%). Left carotid-subclavian artery bypass was performed in 1 case to correct a blockage of the left subclavian artery by the stent graft. Antithrombotic use was reported in 15 cases (68%). Patients who underwent endovascular intervention spent 3 to 25 days in the hospital, with a median stay of 5 hospital days.
Surgical management
Common indications for surgical management included failure of conservative management (40%, 4 of 10 cases), thrombus size and mobility (40%, 4 of 10 cases), patient clinical presentation (20%, 2 of 10 cases), prevention of embolic events (20%, 2 of 10 cases), and for diagnostic purposes (20%, 2 of 10 cases; Table 5). Surgery was also chosen in 1 case (10%) because of the perceived lower embolic risk compared with endovascular intervention, as well as the lack of experience with the endovascular approach.
Surgical Treatment and Outcomes of Thrombus in the Descending Thoracic Aorta.
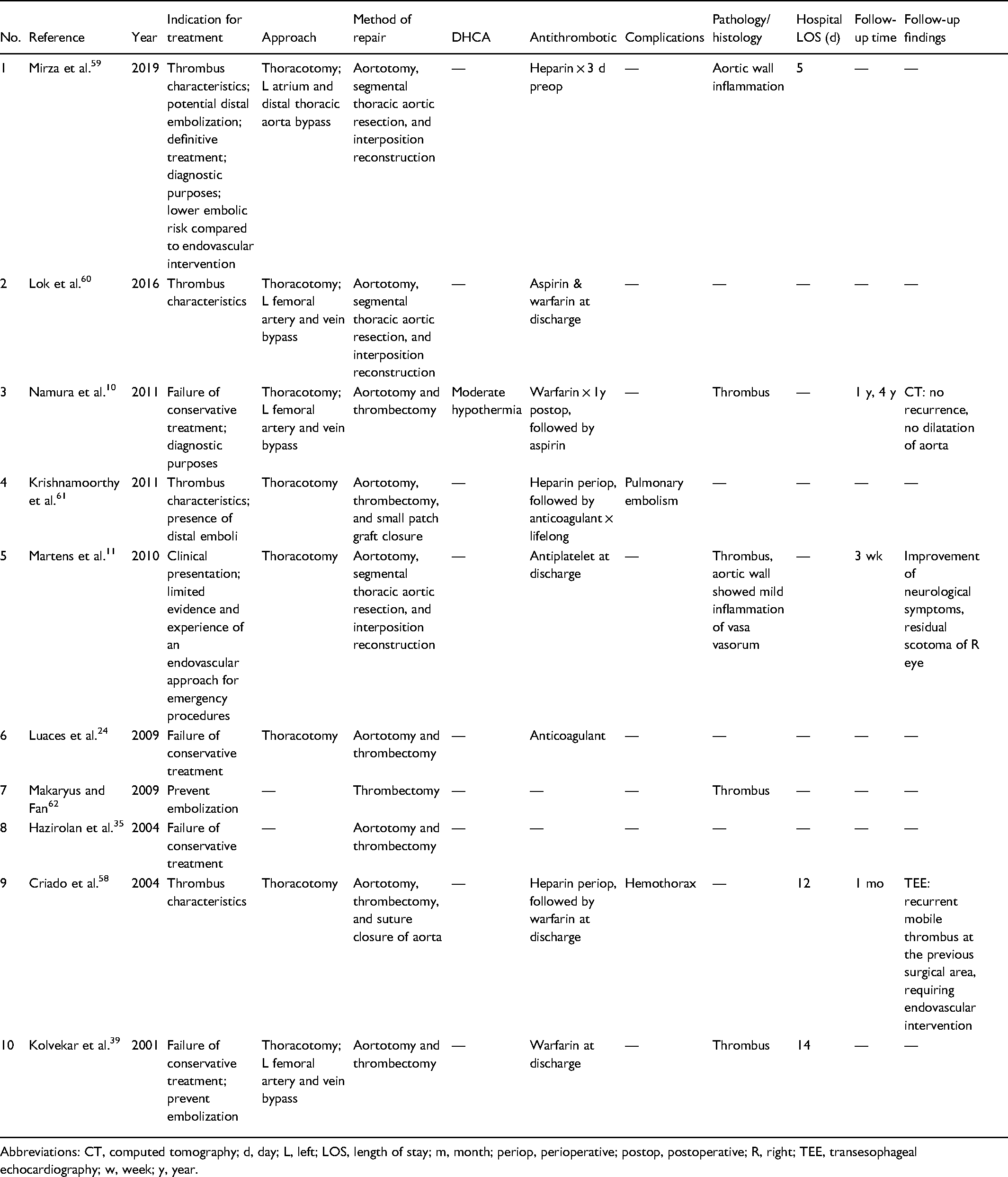
Abbreviations: CT, computed tomography; d, day; L, left; LOS, length of stay; m, month; periop, perioperative; postop, postoperative; R, right; TEE, transesophageal echocardiography; w, week; y, year.
Thoracotomy was the surgical approach of choice for all the reported cases. Once access to the descending thoracic aorta is established, the aorta is opened, the thrombus is removed, and the aortotomy is closed by direct suture or patch repair. In 2 cases (20%), the thoracic aortic segment that contained the thrombus was resected, and the aorta was reconstructed with an interposition graft. Moderate hypothermia was reported in 1 case (10%). Central cardiopulmonary bypass (CPB) strategy via left atrium and distal thoracic aorta cannulations was performed in 1 case (10%). Peripheral CPB via left femoral artery and vein were reported in 3 cases (30%). Adjunctive antithrombotic therapy was described in 8 cases (80%). Patients who underwent surgical intervention spent 5 to 14 days in the hospital, with a median stay of 12 hospital days. Pathological studies confirmed the presence of a thrombus in 4 cases (40%) and indicated an inflammatory process of the aortic wall in 2 cases (20%).
Outcomes and Prognosis
Information on treatment outcomes was available for 94% of patients who received conservative treatment, 73% of patients who received endovascular treatment, and 40% of patients who received surgical treatment, resulting in an overall 78% of patients in this study (Table 6). Complications were described in 26% of all cases with outcomes reported. The most common complication in patients diagnosed with DTAT was recurrent embolism, which was identified in 7 cases (14%). Among these 7 patients, 5 were managed conservatively (17%), 1 was managed with endovascular treatment (6%), and 1 was managed surgically (25%). Other reported complications for patients who were managed conservatively include bleeding (3%, 1 of 30 cases), hematoma at the central venous catheter insertion site for thrombolysis (3%, 1 of 30 cases), and chest pain (3%, 1 of 30 cases). In patients who received endovascular intervention, ischemic reperfusion syndrome and occlusion of the left carotid artery–subclavian bypass graft after TEVAR, which was conservatively managed, were each reported in 1 of 16 cases (6%). For surgically treated patients, hemothorax requiring exploration of the chest and evacuation of the hematoma was reported in 1 of 4 cases (25%). Mortality was reported in 4 of 50 patients with information on outcomes (8%). Of these 4 patients, 3 received medical treatment, 1 had endovascular intervention, and all 4 patients died of multiorgan failure secondary to ischemia.
Summary of Outcomes for Different Treatment Approaches for Thrombus in the Descending Thoracic Aorta.
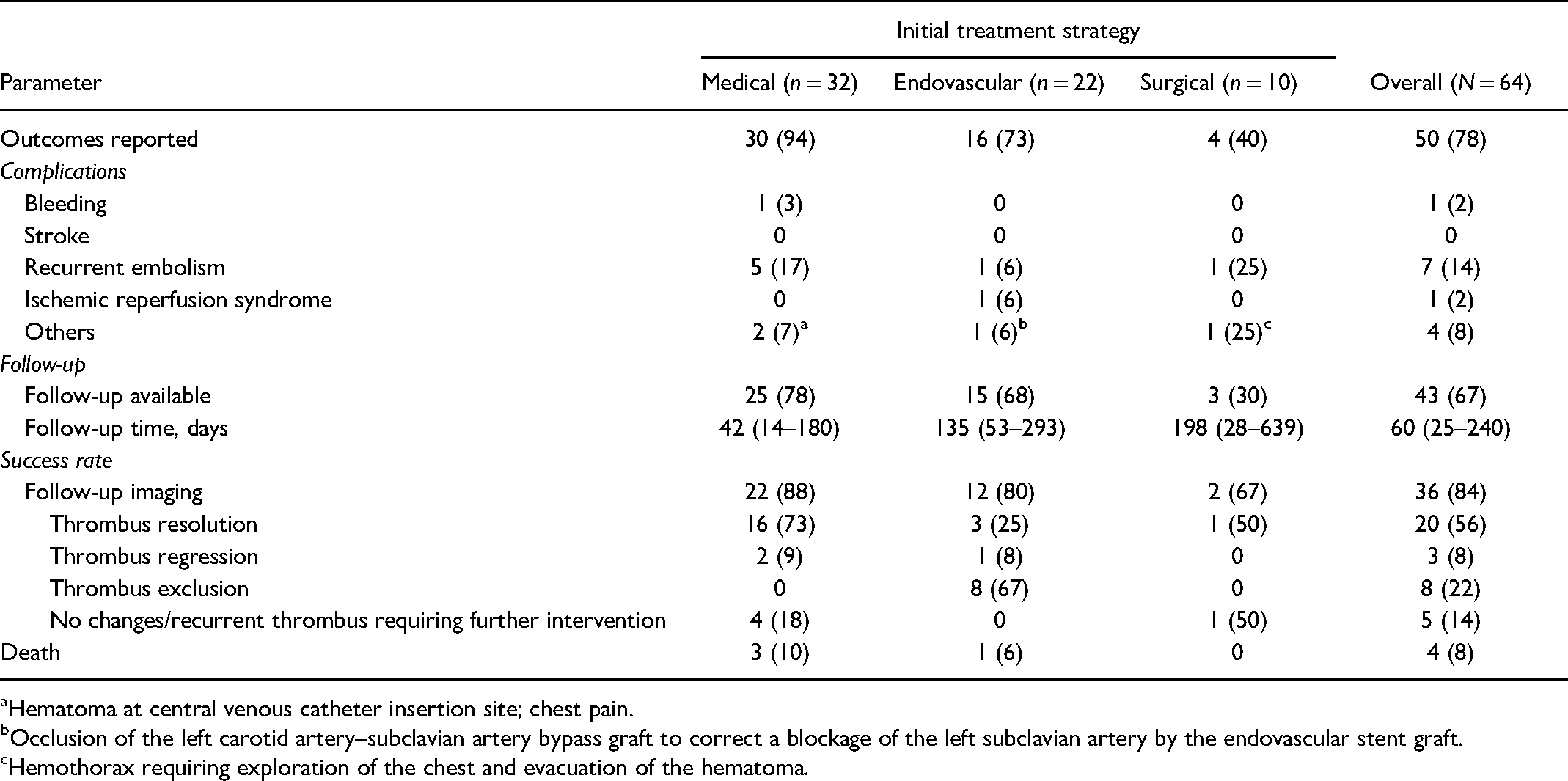
Hematoma at central venous catheter insertion site; chest pain.
Occlusion of the left carotid artery–subclavian artery bypass graft to correct a blockage of the left subclavian artery by the endovascular stent graft.
Hemothorax requiring exploration of the chest and evacuation of the hematoma.
Follow-up information regarding patient survival, resolution/recurrence of thrombus and symptoms, or graft positioning was available in 67% of patients in our review, of whom 78% received conservative treatment, 68% received endovascular treatment, and 30% received surgical treatment. The median duration of follow-up was 42 days (IQR: 14 to 180 days) in conservatively managed patients, 135 days (IQR: 53 to 293 days) in those treated with the endovascular approach, and 198 days (IQR: 28 to 639 days) in those who had surgical treatment—overall, 60 days (IQR: 25 to 240 days) in all included cases.
Follow-up imaging was mentioned in 84% of all patients with follow-up information. Successful management, as defined by thrombus resolution, regression, or exclusion, was achieved in 82% of patients receiving medical treatment, 100% receiving endovascular treatment, 50% receiving surgical treatment, and 86% overall. The rest of the cases either showed no changes in thrombus size or a recurrent thrombus requiring further endovascular or surgical intervention (14% overall).
The proposed algorithm for the management of DTAT is included in Figure 1.
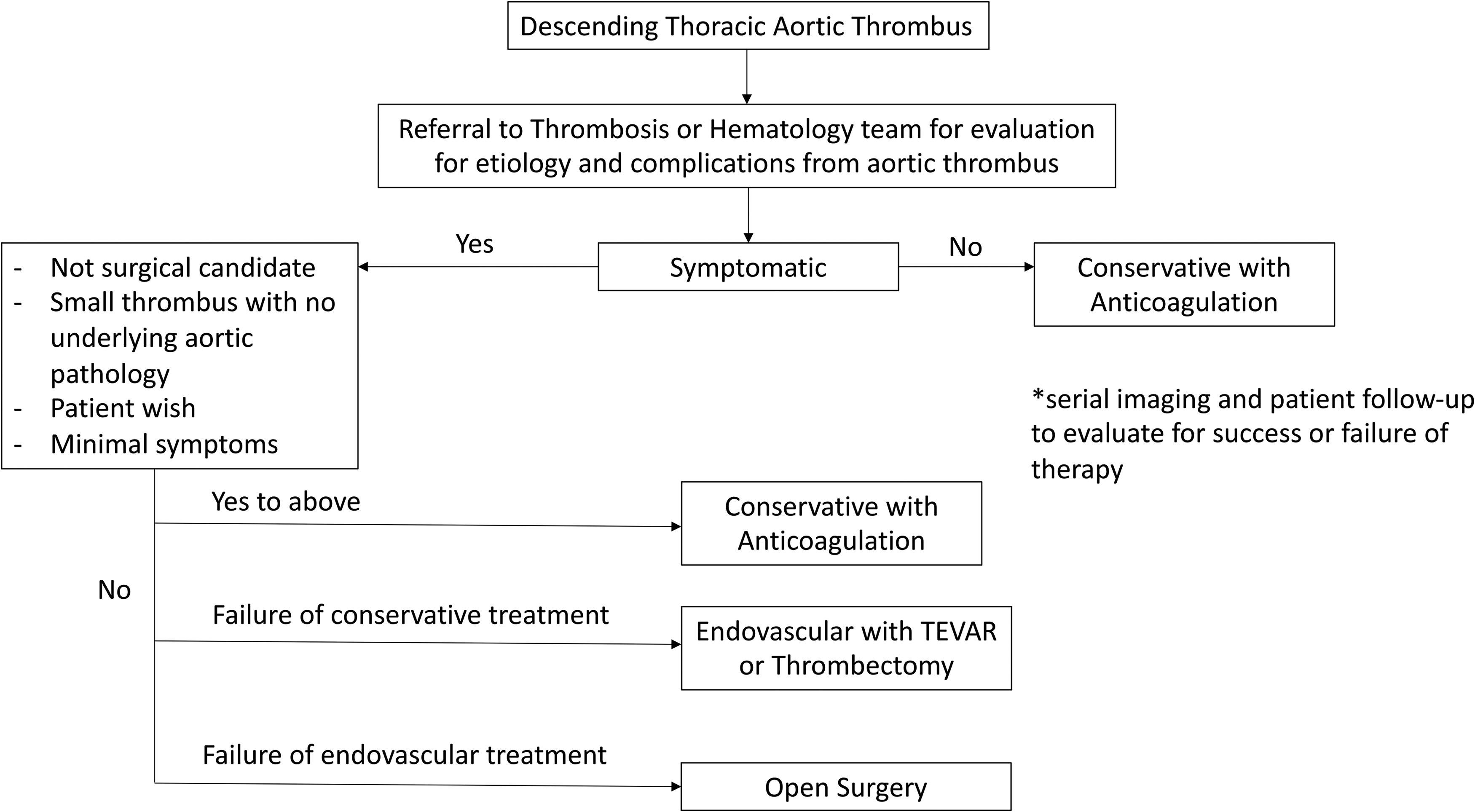
Proposed algorithm for the management of descending thoracic aortic thrombus. TEVAR, thoracic endovascular aortic repair.
Discussion
Overall, the main predisposing factors for DTAT include (1) hypercoagulability either genetically or acquired, such as in the case of malignancy, and (2) risk factors for vasculopathy such as smoking, hypertension, obesity, diabetes, and dyslipidemia. The median age of presentation was mid-50s, and DTAT was more commonly found in females than in males. DTAT could be identified incidentally or from manifestations of downstream embolization causing gut ischemia and claudication symptoms or retrograde embolization causing neurologic symptoms. The natural course of untreated DTAT is either asymptomatic or symptomatic systemic embolization, multiorgan failure, and eventually death, which further emphasizes the importance of early diagnosis and treatment.
There are 3 major treatment modalities for managing DTAT: conservative management with thrombolysis or antithrombotic agents, endovascular with TEVAR or thrombectomy, and open surgery. It is important to take into account the clinical presentation, characteristics of the DTAT, patient comorbidities, and patient preference, as well as center-specific experience, before deciding on the best treatment approach. Conservative treatment is the most common initial approach. It is easily accessible, noninvasive, and does not require technical expertise. This approach is suitable for stable patients, those with small DTAT and no underlying aortic pathology, those who are not surgical candidates, or who do not wish to undergo more invasive treatment. Endovascular stenting or thrombectomy have been indicated in patients with worsening clinical course, failure of conservative treatment, and recurrent thrombus after surgical treatment. This treatment modality is also suitable for patients who are not surgical candidates or for those in whom antithrombotic therapy is contraindicated. The endovascular approach can be used for both therapeutic and diagnostic purposes in cases of diagnostic uncertainty. Open surgery is often used as the last resort when other less invasive approaches fail or in cases of diagnostic uncertainty when a concomitant surgical pathology cannot be ruled out.
DTAT is a rare condition, and information on the prevention of DTAT or recurrent DTAT is very limited. Anticoagulant after initial treatment was the only prevention strategy mentioned in all of the included case reports. However, the effectiveness of anticoagulants in this context remains to be determined because of the lack of long-term data.
Limitations
This study has several key limitations. Our study was limited by the available parameters reported in previous case reports and case series. Important data such as characteristics of the aorta or whether the thrombus was acute or chronic were mostly lacking. The heterogeneity in our study population due to center experience, interventional and surgical techniques, and other center-specific practices may affect treatment approaches and patient outcomes. Furthermore, treatment outcomes were unspecified in 22% of all patients and particularly in 70% of surgical patients, coupled with a lack of follow-up information in an already small population of patients. Therefore, pooled results of therapeutic outcomes may not comprehensively reflect the true outcomes. Given that our review article includes only published articles, it may also be subject to publication bias.
Conclusions
DTAT is a rare condition that can result in significant morbidity and mortality with therapeutic options including conservative management with antithrombotic or thrombolytic agents, endovascular intervention with thrombectomy or TEVAR, and surgical treatment with thrombectomy or segmental aortic resection. Medical management is the least invasive and most frequently chosen initial approach, offering a high reported success rate, whereas endovascular therapy can have a role in thrombus resolution, regression, or exclusion should conservative management fail.
Supplemental Material
Visual abstract - Supplemental material for Management Strategies for Descending Thoracic Aortic Thrombus: A Review of the Literature
Supplemental material, sj-pptx-1-inv-10.1177_15569845221107011 for Management Strategies for Descending Thoracic Aortic Thrombus: A Review of the Literature by Quynh Nguyen, Xiya Ma, Dominique Vervoort and Jessica G. Y. Luc in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.