
Abstract
Background:
Total shoulder arthroplasty (TSA) is an effective treatment for advanced osteonecrosis (ON) of the humeral head, a condition involving vascular disruption and bone necrosis. However, systemic comorbidities in ON patients may impact postoperative outcomes.
Purposes:
We sought to evaluate health care utilization, systemic complications, and implant-related outcomes in TSA patients with and without ON.
Methods:
Using the TriNetX research database, we identified patients who underwent TSA between December 9, 2002, and December 9, 2022. Two cohorts were created: The TSA + ON cohort included patients with any ON diagnosis of the humerus within 1 year leading to their TSA, and the TSA-only cohort excluded patients with ON of the humerus within the same timeframe. Propensity score matching was used to balance comorbidities. Outcomes—including emergency department (ED) visits, readmissions, adverse events, and prosthetic complications—were assessed at 30th day, 90th day, and 1st year. The Benjamini-Hochberg method was applied to control the false discovery rate.
Results:
The query identified 1281 patients with ON and 71 201 patients without ON who underwent primary TSA. After matching, each group consisted of 1218 patients. There were no significant differences in ED visits or readmissions between cohorts after correction. Systemic complications were similar, except for acute kidney injury at the 90th day, which was more frequent in the TSA + ON group. No other adverse events reached significance. Implant-related outcomes, including prosthetic joint infection and revision, were comparable.
Conclusion:
The findings of this retrospective cohort database study suggest that TSA may be safe and effective in ON patients, with similar implant outcomes to non-ON patients. However, the increased rate of acute kidney injury we found at the 90thday in the TSA + ON cohort suggests the need for closer perioperative renal monitoring and supports individualized risk stratification to improve outcomes in this population.
Level of Evidence:
Level III: retrospective cohort database study.
Introduction
Osteonecrosis (ON) of the humeral head is a progressive condition characterized by a disruption in the vascular supply to the bone, leading to osteocyte death and eventual structural compromise. 1 This process initiates a cascade of bone resorption and formation, resulting in subchondral fractures, deformity, and articular surface collapse. 2 In the early stages, increased subchondral sclerosis and radiographic evidence of osteolysis are commonly observed, particularly along the superior and central portions of the humeral head.3,4 As the disease advances, deformation of the humeral head occurs, leading to subchondral plate fractures and glenoid cartilage erosion, ultimately culminating in glenohumeral arthritis. The etiology of ON is not well understood; it may be multifactorial, encompassing both traumatic and atraumatic causes, the latter of which may include prolonged corticosteroid use, sickle cell disease, chemotherapy, alcohol misuse, and other hematological disorders.2,5
Unlike ON of the femoral head (which commonly presents earlier due to the weightbearing nature of the hip joint), ON of the humeral head is often diagnosed at a more advanced stage, thereby delaying diagnosis and significantly limiting nonsurgical treatment options. 6 Surgical management, including core decompression, hemiarthroplasty, and total shoulder arthroplasty (TSA), represents the mainstay of treatment. 7 TSA has demonstrated excellent outcomes, providing significant pain relief, improved range of motion, and durable implant survivorship. Despite this, ON accounts for fewer than 5% of all indications for shoulder arthroplasty, 8 and much of the existing literature is limited to small case series, precluding generalizability to broader populations.
Wang et al 9 reported on the long-term outcomes of 16 shoulders treated with hemiarthroplasty and TSA for ON, demonstrating an 80% implant survivorship rate at 10 years, alongside improvements in pain, range of motion, and overall shoulder function. While these findings are encouraging, the limited sample size highlights the need for studies utilizing larger and more diverse cohorts in order to identify potential complications at a larger scale. Additionally, given the systemic comorbidities often associated with ON, such as sickle cell disease and chronic corticosteroid use, the potential impact of these factors on postoperative outcomes remains poorly understood.10,11
To address these knowledge gaps, this study compared postoperative surgical complications and adverse outcomes in patients undergoing TSA with and without ON of the humeral head. By leveraging a large multi-institutional database, this analysis seeks to provide insights into how ON influences outcomes and inform strategies to optimize the management of this challenging patient population. We hypothesized that patients with ON would be at higher risk of surgical complications and increased health care utilization.
Methods
This retrospective study utilized data collected on December 10, 2024, from the TriNetX research network (https://trinetx.com/solutions/real-world-datasets/), a database containing electronic medical records (diagnoses, procedures, medications, laboratory values, genomic information) of ~138 million patients across 101 health care organizations. Data were acquired as discrete elements or extracted from natural language processing of clinical notes, harmonized syntactically and semantically to ensure consistent data definitions. Cryptographic tokens were used to maintain patient continuity across health care systems, enabling longitudinal data tracking. All data were coded using the International Classification of Diseases, 10th Revision (ICD-10), Clinical Modification, Current Procedural Terminology (CPT), and Systematized Nomenclature of Medicine Clinical Terms systems.
This study was exempt from institutional review board approval as it involved secondary analysis of de-identified data, without direct interaction or intervention with human subjects. The de-identification process adheres to the standards defined in Section §164.514(a) of the HIPAA Privacy Rule, with confirmation by a qualified expert under Section §164.514(b)(1). The most recent certification of de-identification was conducted in December 2020. No funding was obtained or required for this study.
The TriNetX research database was queried to identify patients who underwent TSA between December 9, 2002, and December 9, 2022. Two cohorts were created: the TSA + ON cohort included patients with any ON diagnosis of the humerus within 1 year leading to their TSA, and the TSA-only cohort excluded patients with ON of the humerus within the same timeframe. The timeframe includes any patient with a diagnosis within their chart, either new or history of ON. This included patients with any history of ON. Patients were excluded if they had <30 days of follow-up or if their ON was trauma-related. Patients who underwent shoulder hemiarthroplasty were not included in this study.
To reduce the impact of confounding variables and ensure balanced comparisons between cohorts, propensity score matching was performed using a 1:1 ratio with greedy nearest-neighbor matching and a caliper of 0.1 pooled standard deviations. Propensity scores were estimated using logistic regression. Covariates included in the matching process were age, sex, race, ethnicity, diabetes mellitus, liver disease, nicotine dependence, sickle cell disorders, coagulation disorders, antiphospholipid syndrome, long-term steroid use, and kidney disease. These variables were selected based on prior studies and to minimize selection bias. Matching was conducted with a tolerance of 0.01 to ensure comparability between matched pairs (Table 1).
Characteristics of Patients in the TSA-Only and TSA-ON Cohorts Before and After Matching.
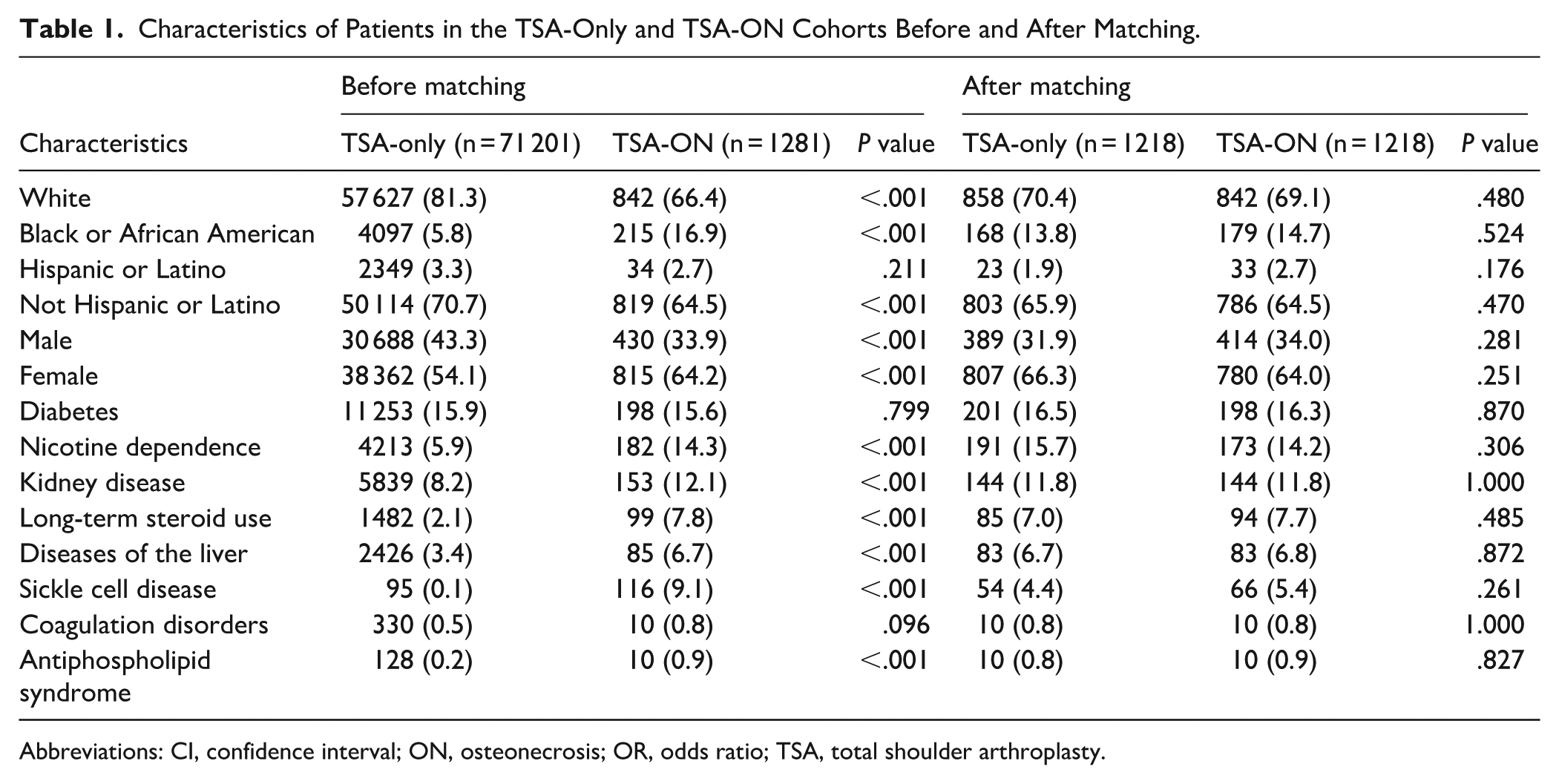
Abbreviations: CI, confidence interval; ON, osteonecrosis; OR, odds ratio; TSA, total shoulder arthroplasty.
Outcomes were identified using ICD-10 and CPT codes and included health care utilization, adverse events, and implant-related complications. Health care utilization outcomes included emergency department (ED) visits and inpatient hospitalizations analyzed at the 30th day, 90th day, and 1st year postoperatively. Adverse events were classified as severe or minor. Severe adverse events included sepsis, myocardial infarction, deep vein thrombosis, pulmonary embolism, and cardiac arrest. Minor adverse events included pneumonia, acute kidney injury, urinary tract infection, transfusion, wound dehiscence, and hematoma. Orthopedic implant-related complications were assessed at the 30th day, 90th day, and 1st year postoperatively. These included prosthetic joint infections, surgical site infections (superficial and deep), dislocations, periprosthetic fractures, prosthesis mechanical loosening, hardware breakage, and revision TSA.
Statistical Analysis
Statistical analyses were conducted using the TriNetX platform, which incorporates Java, R, and Python for statistical computing. Pairwise analyses were performed between groups, and Z-tests were used to determine the significance of risk differences. Statistical significance was set at a threshold of P < .05. For each outcome, the number of instances per patient was recorded. To protect patient anonymity, TriNetX reports outcomes with fewer than 10 patients as N = 10. No statistical inferences or tests can be determined from these data points, as they reflect the database’s privacy standards rather than the actual number of cases. To account for the large number of outcome comparisons and reduce the risk of false-positive findings, the Benjamini-Hochberg (BH) procedure was applied to control the false discovery rate. This correction ensures that statistically significant results are more robust and less likely to reflect random variation.
Results
The query identified 1281 patients with ON undergoing primary TSA and 71 201 patients without ON undergoing primary TSA. Patients with ON were significantly younger (56.6 vs 68.4 years, P < .001) and were more likely to be black or African American (16.9% vs 5.8%, P < .001) and female (64.2% vs 54.1%, P < .001) than patients without ON. Additionally, patients with ON had higher rates of comorbidities including liver disease (6.7% vs 3.4%, P < .001), nicotine dependence (14.3% vs 5.9%, P < .001), sickle cell disorders (9.1% vs 0.1%, P < .001), antiphospholipid syndrome (0.9% vs 0.2%, P < .001), long-term steroid use (7.8% vs 2.1%, P < .001), and kidney disease (12.1% vs 8.2%, P < .001). After matching, each group consisted of 1218 patients and there were no significant differences between the 2 cohorts (Table 1).
Following adjustment for multiple comparisons using the Benjamini-Hochberg correction, no statistically significant differences in health care utilization were observed between the TSA + ON and TSA-only cohorts at any postoperative time point. Although ED visits and hospital readmissions were numerically higher in the ON group across 30, 90 day, and 1 year intervals, these trends did not meet the corrected threshold for statistical significance. For example, ED visits at 30 days were more frequent in the ON group (61 vs 38; BH-adjusted P = .238), and readmissions at the 90th day were similarly higher (114 vs 84; BH-adjusted P = .264), than in the TSA-only group, but both findings lost significance after correction. These results suggest that previously-observed differences may have been driven by type I error, and no conclusive increase in short-term or long-term health care utilization could be confirmed in this cohort (Table 2).
Thirty day, 90 Day, and 1 Year Health Care Utilization for the Matched TSA-Only and TSA-ON Cohorts.
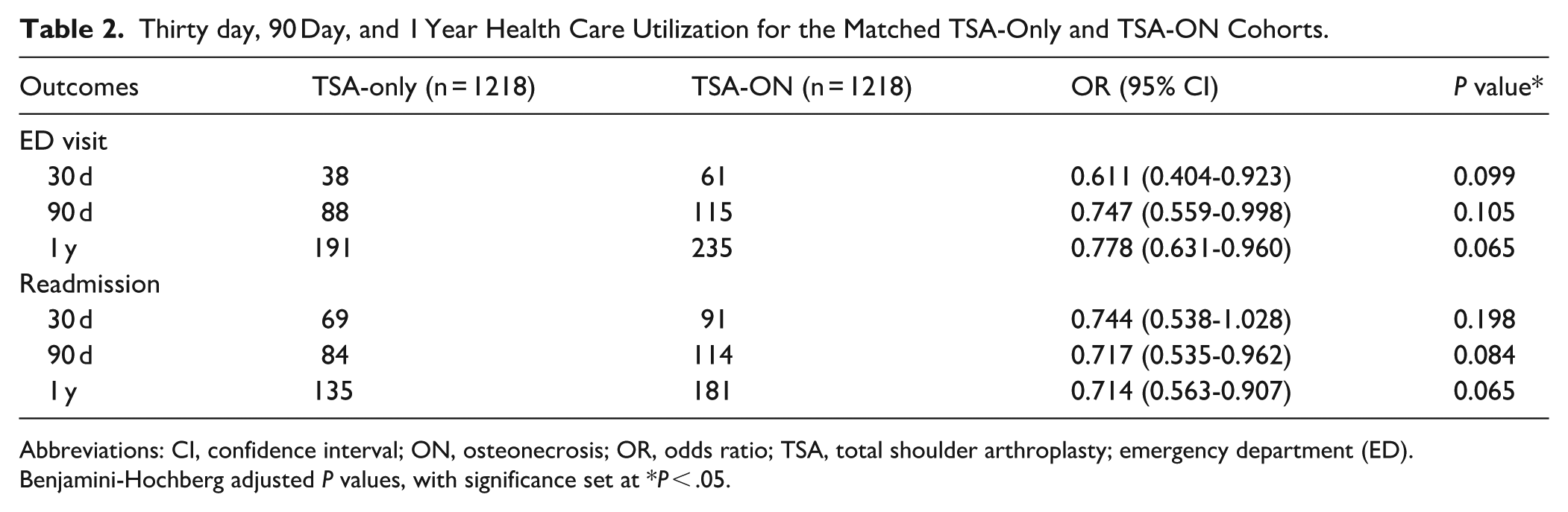
Abbreviations: CI, confidence interval; ON, osteonecrosis; OR, odds ratio; TSA, total shoulder arthroplasty; emergency department (ED).
Benjamini-Hochberg adjusted P values, with significance set at *P < .05.
Initial unadjusted analyses suggested that patients with ON experienced significantly-higher rates of systemic complications across multiple postoperative time points. However, after applying the Benjamini-Hochberg correction, nearly all of these comparisons lost statistical significance. For example, severe adverse events occurred in 33 ON patients versus 15 non-ON patients at the 30th day (OR = 0.448, 95% CI = 0.242-0.829; raw P = .009), and in 91 versus 66 patients at the 1st year (OR = 0.710, 95% CI = 0.511-0.984; raw P = .039), but none of these differences remained significant following multiple comparison adjustment. Similarly, minor adverse events appeared elevated in the ON group at the 90th day (108 vs 76; OR = 0.684, 95% CI = 0.504-0.928; raw P = .014) and 1st year (207 vs 166; OR = 0.771, 95% CI = 0.617-0.962; raw P = .021), yet these also did not meet the Benjamini-Hochberg threshold for significance. Among individual complications, pneumonia, urinary tract infection, and myocardial infarction were all more common in the ON cohort numerically, but only 1 outcome—acute kidney injury at the 90th day—remained significantly elevated after correction (36 vs 14 patients; OR = 0.382, 95% CI = 0.205-0.712; BH-adjusted P = .030). Cumulative rates of any adverse event, severe or minor, were also not significantly different following statistical adjustment (Table 3).
Thirty day, 90 Day, and 1 Year Systemic Complications for the Matched TSA-Only and TSA-ON Cohorts.
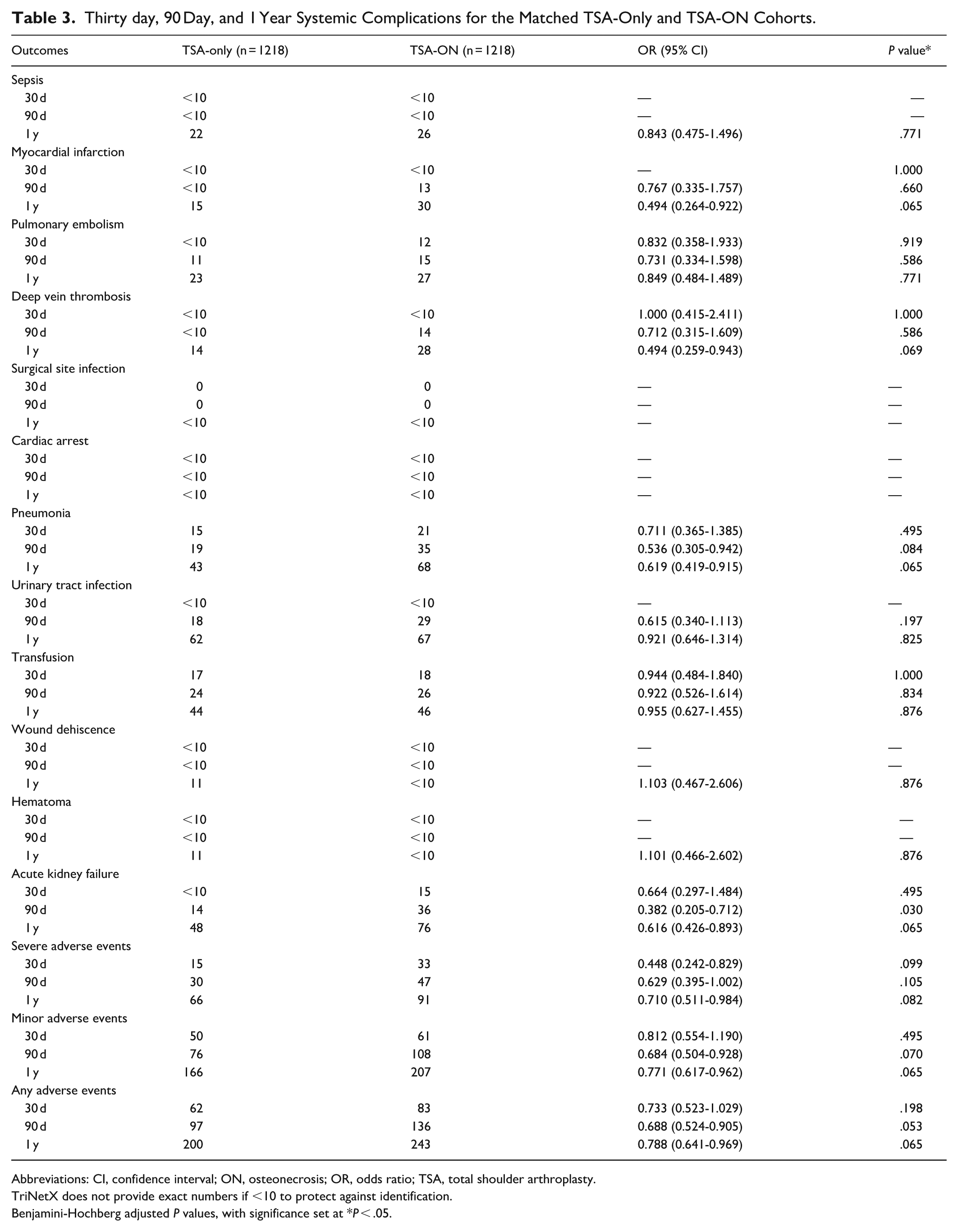
Abbreviations: CI, confidence interval; ON, osteonecrosis; OR, odds ratio; TSA, total shoulder arthroplasty.
TriNetX does not provide exact numbers if <10 to protect against identification.
Benjamini-Hochberg adjusted P values, with significance set at *P < .05.
There were no statistically significant differences in implant-related complications between the TSA + ON and TSA-only cohorts at any postoperative time point. Prosthetic joint infections occurred in 25 patients in each cohort at the 1st year (OR = 1.007, 95% CI = 0.575-1.763; BH-adjusted P = .981), and prosthesis dislocations were observed in 21 ON patients and 29 non-ON patients at the 1st year (OR = 1.393, 95% CI = 0.790-2.456; BH-adjusted P = .432). Periprosthetic fractures remained rare, with fewer than 10 cases in each cohort across all time points, and prosthesis mechanical loosening occurred in 11 ON patients and 14 non-ON patients at the 1st year (OR = 1.312, 95% CI = 0.593-2.902; BH-adjusted P = 0.771). Cases of broken prostheses, superficial surgical site infections, and deep surgical site infections were infrequent and did not differ significantly between groups. Revision TSA was also comparable, occurring in 31 ON patients versus 44 in the TSA-only cohort at the 1st year (OR = 1.491, 95% CI = 0.934-2.378; BH-adjusted P = .175). No implant-related outcomes met the threshold for statistical significance after correction (Table 4).
Thirty day, 90 Day, 1, and 2 Year Orthopedic Complications for the Matched TSA-Only and TSA-ON Cohorts.
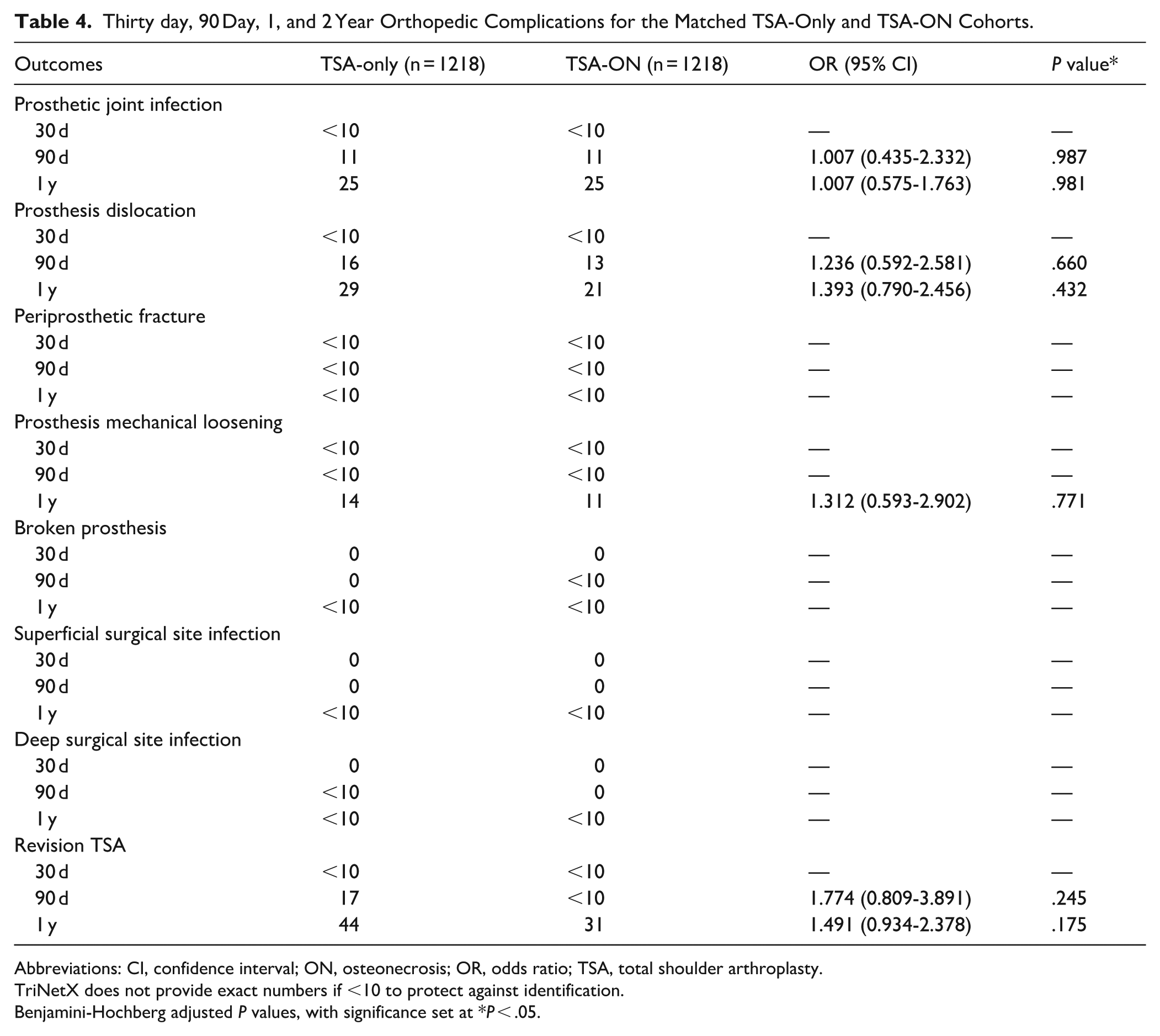
Abbreviations: CI, confidence interval; ON, osteonecrosis; OR, odds ratio; TSA, total shoulder arthroplasty.
TriNetX does not provide exact numbers if <10 to protect against identification.
Benjamini-Hochberg adjusted P values, with significance set at *P < .05.
Discussion
ON of the humeral head presents both systemic and local challenges that may influence surgical and postoperative outcomes. This study represents one of the largest multi-institutional analyses comparing TSA outcomes between patients with and without ON. While initial analyses suggested increased health care use and complication rates in ON patients, most of these observed differences did not remain statistically significant after correction for multiple comparisons. These findings provide a nuanced understanding of the potential risks associated with TSA in this population and highlight the importance of rigorous statistical methodology in large observational data sets.
Several limitations should be noted. First, the retrospective design and reliance on a large database introduce potential sources of bias, including misclassification and incomplete documentation. While a large study interval allowed for a large sample size, surgical indications, and techniques throughout the years may serve as potential confounders. Due to the database structure, we could not stratify the exact number of patients per year. Due to the retrospective nature of the database and the lack of additional information, we did not consider patient-reported outcomes. Although propensity score matching was employed to minimize confounding, residual bias from unmeasured variables could not be excluded; this included the inability to understand what led to the diagnosis of ON. Different causes of ON may pertain to different complication profiles among those undergoing TSA. For example, patients with sickle cell disease may present with ON at younger ages, thus having a different complication. As such, we are unable to comment on specific preoperative measures that may be necessary in specific patient populations. Additionally, the TriNetX database does not provide granular clinical or radiological data, which limits our ability to analyze disease severity, implant positioning, or other factors influencing outcomes. Importantly, this study was not designed to evaluate hemiarthroplasty as a treatment for ON; therefore, patients undergoing hemiarthroplasty were excluded, which limited our ability to compare potential differences in complication profiles or outcomes between this treatment modality and TSA. We also could not differentiate between patients who underwent anatomic and reverse arthroplasties. The selection regarding the type of TSA could reflect some of the complication profiles that cannot be assessed in a database study. Finally, the reporting of outcomes with fewer than 10 patients as N = 10, a privacy measure implemented by the TriNetX database, restricted our ability to perform statistical analyses on rare events. Future prospective studies incorporating detailed clinical data and radiographic evaluations will be critical to corroborating and expanding upon our findings.
Although we found elevated health care utilization among ON patients, these differences did not reach statistical significance following correction for multiple comparisons. ED visits and inpatient readmissions were consistently higher in the ON cohort across all time points, including 61 versus 38 ED visits at the 30th day and 114 versus 84 readmissions at the 90th day, but none reached statistical significance after the Benjamini-Hochberg correction (Table 2). Despite propensity matching to balance baseline characteristics, these nonsignificant differences may still reflect underlying disease severity, functional limitations, or more complex postoperative recovery profiles among ON patients. 12 This aligns with findings by Reddy et al, who emphasize that preoperative management of comorbidities—such as anemia and hyperlipidemia—may help mitigate postoperative risk, even in populations where differences in utilization are not statistically significant. 13 These results suggest that ON patients may not experience a significantly-higher burden of health care use following TSA. Future studies may help confirm whether these trends persist in larger or more granular data sets and clarify the extent to which perioperative management needs to be tailored for this population.
Systemic complication rates were generally similar between cohorts, with few differences emerging in the postoperative period. Several complications—such as pneumonia, myocardial infarction, urinary tract infections, and venous thromboembolism—were more frequently observed in the ON group based on raw counts. However, when adjusted for multiple comparisons, none of these trends met statistical significance. The only systemic complication that remained significantly-more frequent in the ON cohort was acute kidney injury at the 90th day, which occurred in 36 ON patients versus 14 TSA-only patients. This may reflect increased baseline renal vulnerability in ON patients, particularly in the context of long-term corticosteroid exposure or comorbid conditions such as hypertension, diabetes, and sickle cell disease. 12 Furthermore, endothelial dysfunction, which is a proposed key factor in ON pathogenesis, may contribute to these outcomes by impairing vascular repair and increasing susceptibility to venous thromboembolic events and poor tissue healing.14,15 These findings highlight the importance of perioperative renal monitoring in this patient population while reinforcing that ON patients do not appear to face a broadly-elevated risk of systemic complications following TSA.
Implant-related complications—including prosthetic joint infections, dislocations, loosening, and revision TSA—were infrequent and comparable between groups across all postoperative time points. For example, at the 1st year, prosthetic joint infections occurred in 25 patients in each cohort, and revision TSA was performed in 31 ON patients and 44 TSA-only patients. These findings suggest that ON does not confer additional risk for implant-related failure following TSA. This aligns with prior reports that have found similar implant survivorship and mechanical failure rates among patients with and without ON.16,17 However, it is important to note that, despite the large sample size of this study, implant complications were very rare, often with fewer than 10 occurrences, and the limitations of the database’s reporting standards may have restricted the depth of our analysis.
In conclusion, initial analyses in this retrospective database study comparing postoperative outcomes between ON and non-ON patients undergoing TSA suggested increased risks in the ON cohort, but most observed differences in health care utilization and systemic complications were not statistically significant. Acute kidney injury at the 90th day in the ON cohort was the only complication to remain significantly elevated. In addition, implant-related outcomes were comparable between groups, suggesting that TSA may be a viable treatment option for patients with ON. These findings also suggest the importance of individualized perioperative planning, while suggesting that ON alone does not appear to broadly increase postoperative risk. Future studies integrating radiographic data, extended follow-up, patient-reported outcome measures, and clinical assessments will be critical to further optimizing patient care and understanding long-term functional outcomes and quality of life.
Supplemental Material
sj-docx-1-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-1-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-2-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-3-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-4-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-5-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316251380577 – Supplemental material for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-6-hss-10.1177_15563316251380577 for Complications in Osteonecrosis Patients After Shoulder Arthroplasty: A Propensity-Matched Cohort Study by Tuckerman Jones, Akhil Katakam, Daniella Ogilvie, Avani Chopra, Tej Joshi and John Erickson in HSS Journal®
Footnotes
Consent to Participate
Informed consent was waived and institutional review board (IRB) approval was not required for this retrospective database study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
CME Credit
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki declaration.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.