
Abstract
Background:
Arthroscopy can be used to assist the open reduction internal fixation (ORIF) approach in the treatment of acute ankle fractures. Arthroscopy can also help to assess the articular surface but is performed in only 1% of ankle fracture cases.
Purpose:
We aimed to investigate (1) whether arthroscopy-assisted ORIF (AORIF) would lead to improved postoperative functional outcomes compared to conventional ORIF and (2) whether differences in postoperative complication rates exist between these 2 techniques.
Methods:
A systematic review was performed; 2 researchers independently searched the online databases of PubMed, Scopus, Embase, Cochrane, and Google Scholar. All studies that directly investigated the outcomes of AORIF versus conventional ORIF in the treatment of ankle fractures and contained quantitative data were eligible for inclusion. The Cochrane tools for bias assessment were applied independently by 2 researchers.
Results:
Six articles (2 randomized controlled trials and 4 retrospective cohort studies) were included in this systematic review. The meta-analysis of functional outcome scores resulted in a standardized mean difference of 0.6 (confidence interval [CI]: [0.3, 0.9]) favoring AORIF, after excluding 2 studies due to missing standard deviations. The overall complication rate was similar between the 2 groups, with a pooled odds ratio of 1.1 (CI: [0.4, 3.0]).
Conclusion:
The findings of this systematic review and meta-analysis suggest that AORIF might improve postoperative outcomes without increasing the complication rate when compared to conventional ORIF. However, due to the inherent clinical heterogeneity of the included studies, further well-designed randomized controlled trials are required.
Keywords
Introduction
Ankle fractures are among the most common fractures encountered in orthopedic surgery, occurring at an incidence rate of 187 per 100,000 person-years, with the majority related to athletic activities [10,11]. The standard of surgical treatment of ankle fractures is open reduction internal fixation (ORIF), which yields good to excellent results that vary by fracture type [4,21,29]. Stufkens et al [29] included 1822 patients in their systematic review of long-term outcomes after surgically treated ankle fractures, reporting that 79.3% of well-reduced fractures had a good to excellent outcome after a mean follow-up of 5.1 years.
Some patients, however, experience poor results after surgical repair with ORIF [5,13]. In their observational study of 25 patients, Day et al [13] reported a good to excellent functional outcome in only 52% and a poor outcome in 24% of patients with a follow-up of 10 to 14 years. Bhandari et al [5] pointed out less satisfactory outcomes in several observational studies, ranging from 17% to 24%. The occurrence of poor outcomes following ankle fractures is theorized to be connected to concomitant intra-articular injuries not detectable with conventional ORIF [9,34,17,22]. Imaging techniques like plain radiographs or magnetic resonance imaging scans are unable to detect these lesions reliably [6,30].
The incidence of intra-articular injuries has been reported to range from 20% to 88.9% [8]. Williamson et al [35] reported in their systematic review that, on average, 54.5% of ankle fractures showed evidence of osteochondral or chondral lesions. Osteochondral lesions may be present in up to 90% of patients with residual long-term pain after an ankle fracture [32]. Stufkens et al [28] reported that intra-articular lesions had been identified to be an independent predictor of developing posttraumatic osteoarthritis. Leontaritis et al [20] observed that intra-articular lesions occur at higher rates when more severe fracture patterns are encountered. These findings underscore the importance of early detection and intervention for chondral lesions.
Arthroscopy has been proposed as an additional tool to discover and treat these lesions, potentially improving patients’ postoperative outcomes [8,17,18]. Arthroscopy supports the process of fracture reduction by making it possible to assess the articular surface directly [31]. Despite encouraging findings in favor of assistance [19], arthroscopy was performed in just 1% of ankle fracture cases between 2005 and 2011 [1].
We aimed to investigate the differences in functional outcome scores between ORIF and arthroscopic assistance and to compare their postoperative complication rates to elucidate whether arthroscopic assistance is a useful addition in the treatment of ankle fractures.
Methods
This systematic review was conducted according to the PRISMA guidelines [24]. The PICO framework was constructed to support the search process. The population was identified as adults with ankle fractures. The intervention was arthroscopy-assisted open reduction internal fixation (AORIF), which was compared with ORIF. Outcomes measured were functional outcome scores, overall and specific complication rates, chondral lesions, and operative time.
The electronic databases of PubMed, Scopus, Embase, Cochrane, and Google Scholar were searched for articles containing the key terms: ankle OR malleol* OR distal tibia* OR distal fibula* AND fracture* AND arthroscop* OR AORIF OR ORIF OR “open reduction internal fixation.” Articles up to January 28, 2022 were evaluated. The reference lists were manually searched in articles identified for full-text review (Supplemental Table 1).
Inclusion criteria for studies were those (1) directly comparing arthroscopy-assisted ORIF versus conventional ORIF for the treatment of acute ankle fractures, (2) reporting quantitative outcome data, and (3) available in the English language. Exclusion criteria were (1) studies using arthroscopy only for diagnosis without changes in the operative procedure, (2) systematic reviews or meta-analyses, and (3) studies investigating radiologic outcomes only.
Two researchers (MM and MH) independently conducted the search and screened the titles and abstracts of identified articles according to the inclusion and exclusion criteria. Full-text articles matching the topic of interest were extracted and evaluated. The authors discussed any divergences that arose during the selection process and reached a mutual agreement. Zotero was used for managing references and citations.
The Cochrane Risk of Bias 2 (RoB2) tool was used to assess the quality of studies of randomized controlled trials [27]. For the assessment of observational studies, the Risk of Bias in Non-Randomized Studies—of Interventions (ROBINS-I) tool was used [26]. Two researchers (MM and MH) assessed the quality of each study independently. After this process, any aberrations were thoroughly discussed and agreed on.
Two authors (MM and MH) independently identified and extracted the data of interest (authors, publication year, study design, sample size, patient demographics, mean follow-up, fracture types, and concomitant injuries) using a standardized extraction form in a spreadsheet program. In addition, functional outcomes, operative time, incidence of chondral lesions, and information on postoperative complication rates and complication types were extracted. The independently collected data were confirmed by the study investigators. In the case of missing data, the study authors were contacted by e-mail with a reminder sent 1 week after initial contact in case of nonresponse.
Quantitative synthesis was performed for 2 outcomes: functional scores and complication rates. Standardized mean differences (Hedges’ g) for functional scores between AORIF and ORIF were calculated for each study and were pooled together using inverse-variance random-effects meta-analysis with a restricted maximum likelihood heterogeneity estimator. Complication rates were pooled in a Mantel-Haenszel random-effects meta-analysis, with a treatment arm continuity correction in studies with zero events. Heterogeneity across studies was assessed with the I2 statistic. We planned to formally assess small-study effects using funnel plots and the Egger regression asymmetry test, provided we could identify at least 10 studies. All analyses were performed in the R statistical environment version 4.2 using the meta and metafor packages. Results are presented with their corresponding 95% confidence interval (CI).
Results
The flow chart in Supplemental Fig. 1 reports the summary of the study selection process. A poster identified during the literature search process [14] led to the identification of an additional article by searching for corresponding author names [23]. The search process led to the final inclusion of 6 articles (4 retrospective cohort studies and 2 randomized controlled trials) in this systematic review. A search of the reference lists of included articles did not yield any additional studies. The researchers of an ongoing randomized controlled trial [6] were contacted to seek preliminary data but did not have any data available at the time. Supplemental Figs. 2 to 5 depict the risk of bias for each study, using the Cochrane tools for bias assessment [26,27]. For both randomized controlled trials [32,34], there were some concerns regarding the overall level of bias, according to the RoB2 tool. When the ROBINS-I tool was applied, a high risk of overall bias was identified in 3 retrospective observational studies [15,23,25] and a moderate risk in 1 article [3].
A total of 453 patients were included in this systematic review, of which 192 patients were treated with AORIF and 261 with conventional ORIF. The mean follow-up after the procedure ranged from 20.4 to 67 months. Fracture types were characterized by 3 different classification systems. Two studies used the AO/OTA classification [3,15], 3 studies used the Lauge-Hansen classification [23,31,33], and 2 studies used the Danis-Weber classification system [25,31]. One article classified their fractures by both the Lauge-Hansen and the Danis-Weber classification [31]. A summary of data from included articles can be found in Supplemental Table 2.
Standard deviations of their functional outcome scores were not included in 2 of the 6 articles, and their authors did not reply to our request for additional data. Therefore, they had to be excluded from the meta-analysis. Four of the 6 articles were included in the meta-analysis of functional outcome scores and resulted in a standardized mean difference of 0.6 (CI: [0.3, 0.9]) in favor of AORIF (Fig. 1). A summary of outcome scores can be found in Table 1. Given that we identified fewer than 10 studies, we did not formally assess for small-study effects.
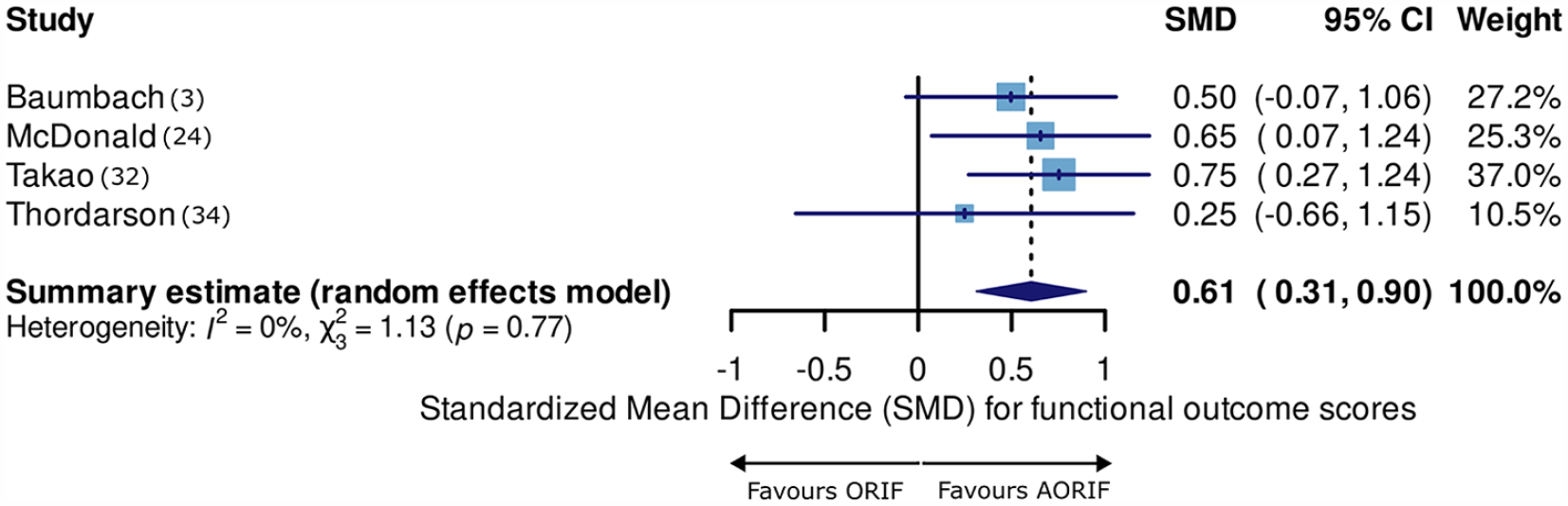
Forest-plot of functional outcome scores.
Summary of functional outcome scores.
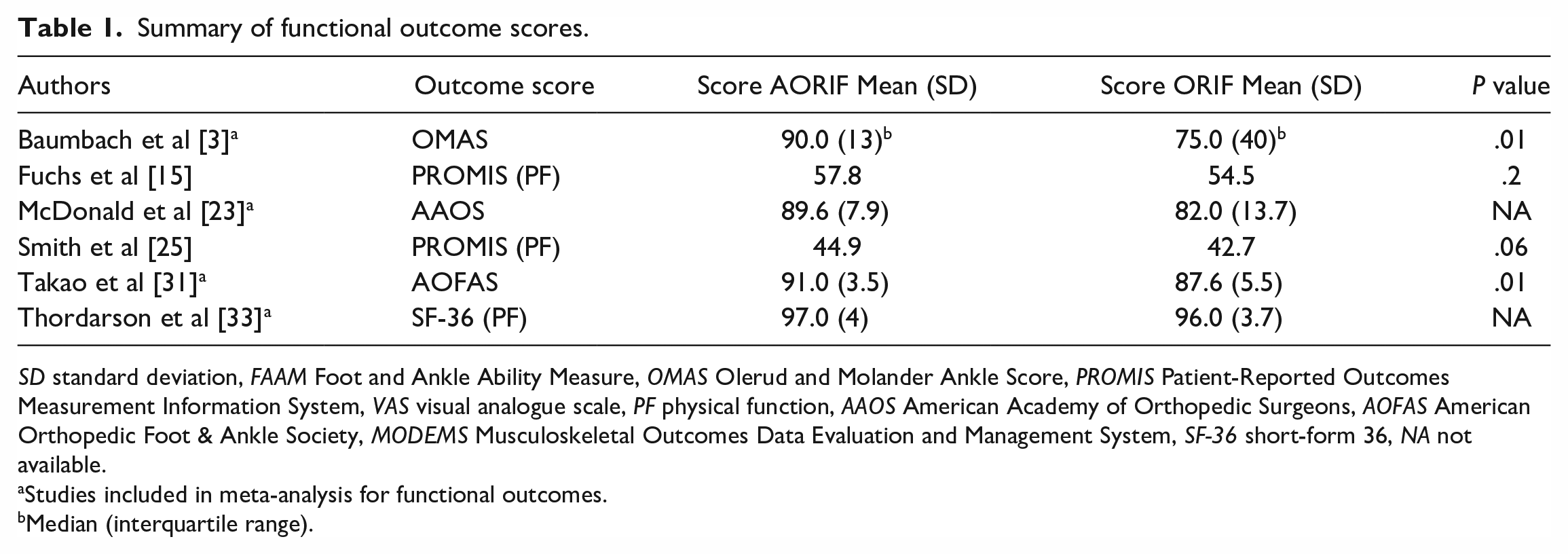
SD standard deviation, FAAM Foot and Ankle Ability Measure, OMAS Olerud and Molander Ankle Score, PROMIS Patient-Reported Outcomes Measurement Information System, VAS visual analogue scale, PF physical function, AAOS American Academy of Orthopedic Surgeons, AOFAS American Orthopedic Foot & Ankle Society, MODEMS Musculoskeletal Outcomes Data Evaluation and Management System, SF-36 short-form 36, NA not available.
Studies included in meta-analysis for functional outcomes.
Median (interquartile range).
The incidence of chondral or osteochondral lesions was identified in 27% to 89% of AORIF patients [3,15,23,25,31,33]. The highest incidence of 89% was noted in the article by Baumbach et al [3], who reported chondral lesions in 22 out of 25 patients with complex ankle fractures. The therapeutic arthroscopic procedures for osteochondral injuries consisted of debridement, shaving, excision, drilling, chondroplasty, and microfracture surgery. Lower graded chondral lesions were mainly treated by debridement and higher-grade lesions, by microfracture procedures [3]. A summary of the incidence of chondral lesions is shown in Supplemental Table 2.
Three studies reported on the operative time, which increased by 10 to 15 minutes when arthroscopy was performed [15,23,25]. McDonald et al [23] allocated a maximum time of 10 minutes for the concomitant arthroscopic procedures. Smith et al [25] observed an extra 10 minutes of tourniquet time in the AORIF group with an overall time of 89 minutes compared to 79 minutes in the ORIF group (P = .6). The article by Fuchs et al [15] described an operative time of 59 minutes for the ORIF group and 74 minutes for the AORIF group (P = .03), meaning an average increase of 15 minutes was noted when arthroscopy was used.
All studies reported equivalent complication rates between the 2 groups [3,15,23,25,31,33] (Table 2). The meta-analysis for any complication resulted in a pooled odds ratio (OR) of 1.1 (CI: [0.4, 3.0]; Fig. 2) after excluding 1 article due to missing information on complication rates per cohort [25].
Summary of complications.
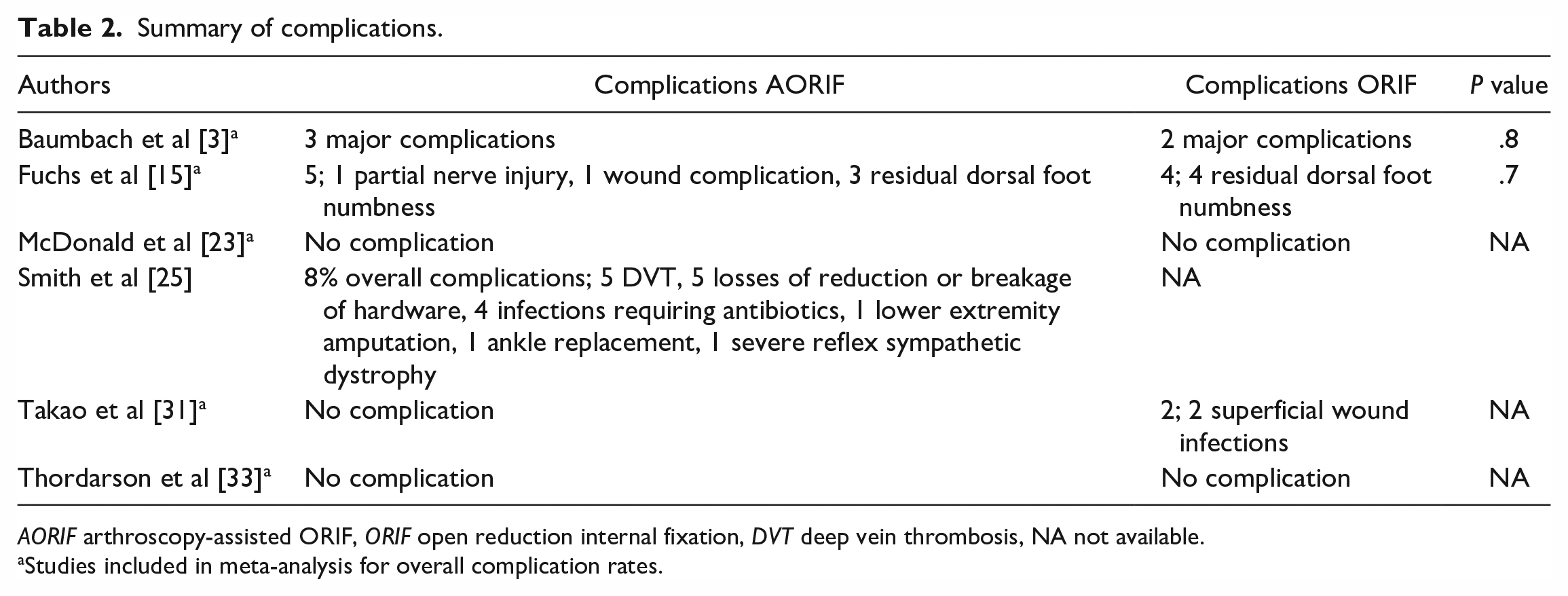
AORIF arthroscopy-assisted ORIF, ORIF open reduction internal fixation, DVT deep vein thrombosis, NA not available.
Studies included in meta-analysis for overall complication rates.
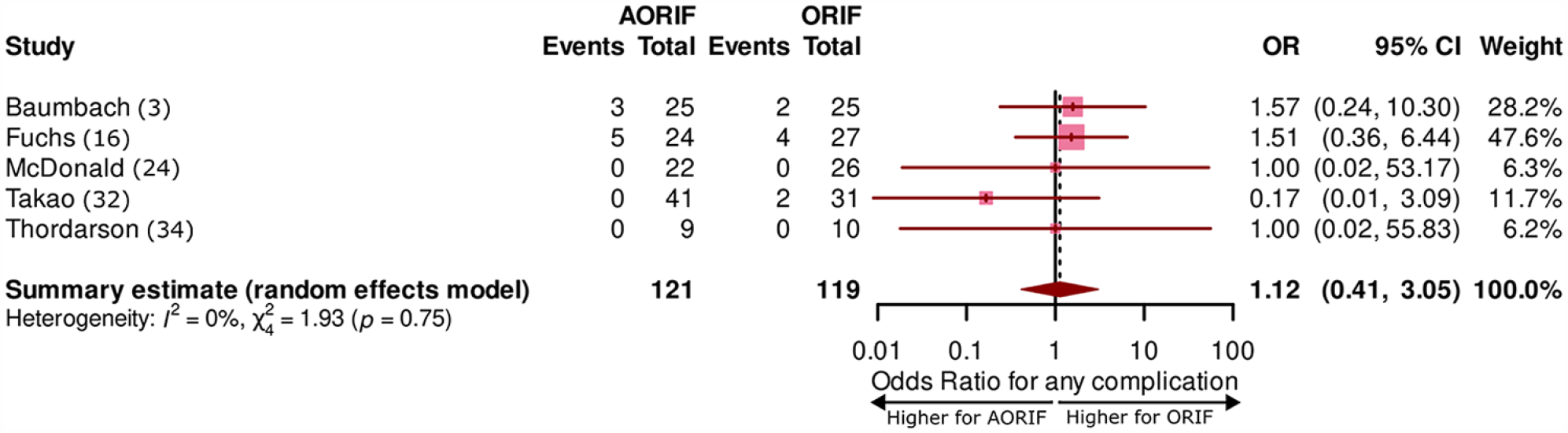
Forest-plot of overall complication rates. AORIF arthroscopy-assisted ORIF, ORIF open reduction internal fixation.
Discussion
The purpose of this systematic review was to investigate whether AORIF improves postoperative functional outcomes compared to conventional ORIF. In addition, it examined whether differences in postoperative complication rates exist between these 2 techniques. The meta-analysis suggests that AORIF may provide for improved functional outcomes following ankle fracture repair compared to ORIF alone. The analysis also suggests there is no increased risk of complications when AORIF is performed.
This systematic review had several limitations. Concomitant injuries like the presence of osteochondral lesions could not be assessed reliably in the ORIF cohort. Thus, it remains unclear how intra-articular lesions affect the outcomes in the ORIF group. As functional outcome scores were reported by different scoring systems, this might play a role in the homogeneity of findings, as the scores assess similar factors in patients’ outcomes but are not identical to each other. Hence, a standardization of the reporting of functional outcomes would greatly benefit future studies. Heterogeneity also was present in the classification systems of fracture types. Furthermore, the study population of this systematic review was relatively small, with the majority of patients coming from retrospective cohort studies. In addition, 2 articles had to be excluded from our meta-analysis of functional outcomes scores due to missing information on standard deviations [15,25]. One article had to be excluded from our analysis of overall complication rates as it was missing information about the specific numbers per group [25]. Owing to the limited number of studies that exist on the topic, randomized controlled trials and observational studies were combined in our meta-analysis, which might yield additional heterogeneity. However, we decided to pursue the meta-analysis to achieve the best possible comparison between the 2 interventions. Overall, the statistical heterogeneity as shown by the I2 approached 0%, but because the methodologic heterogeneity of included studies appeared to be relatively high, the meta-analysis findings need to be interpreted with caution.
No consensus exists on the optimal management of concomitant intra-articular lesions in the treatment of acute ankle fractures. Gonzalez et al [16] conducted a systematic review and concluded that the evidence was insufficient to deduce that AORIF could provide improved functional outcomes over ORIF. A meta-analysis by Lee et al [19] included 4 articles and reported a pooled effect size of 0.5, favoring the AORIF technique. Our findings are in line with previously reported results, pointing toward a possible improvement in outcomes when AORIF is used. These findings are likely attributable to the increased diagnostic accuracy in the detection of intra-articular lesions or loose bodies that arthroscopy provides. Furthermore, these pathologies can be treated directly when visualized [17,18].
Compared to previous systematic reviews, our study additionally includes a meta-analysis of complication rates to further improve a clear comparison between the 2 approaches. A potential increase in complication rates might be expected due to the addition of arthroscopy, but our analysis did not point toward this trend. The rates of complications were equivalent between the 2 intervention groups [3,15,23,31,33]. However, we observed a wide CI; hence these findings should be interpreted with caution. Complications specific to arthroscopy (for example, injuries to neurovascular structures such as the greater saphenous vein or the saphenous nerve) have been previously reported [7]. However, when analyzing the complication types, we did not observe an increase in specific complications when arthroscopy was performed. This might suggest that the proper placement of arthroscopy portals by an expert surgeon does not increase the number of specific complications. Nevertheless, this could also be related to the relatively small population of cases included in this systematic review and the lack of standardized complications reporting system across the included studies.
For the overall assessment of AORIF, it is essential to consider both the benefits and drawbacks compared to conventional ORIF. One of the drawbacks of AORIF is the additional time needed per procedure, which was reported to be between 10 and 15 minutes [15,23,25]. This increase in operative time has been reported as not statistically significant (P = .06) by Smith et al [25] and as statistically significant (P = .03) by Fuchs et al [15]. The additional operative time of AORIF has been described by only half of the studies included in this review, and therefore, future studies should consider reporting the operative times per technique. Other disadvantages of arthroscopy are the surgeon’s expertise required to perform the operation and the additional expenses connected to the procedure. However, additional costs of arthroscopy have been reported by Aziz et al [2] as little burdensome and by Danilkowicz et al [12] as statistically insignificant. As no data about operative costs have been described by the articles included in this systematic review, an analysis of the cost-effectiveness could not be conducted.
In conclusion, arthroscopy is a promising tool that can be used in conjunction with ORIF for the treatment of acute ankle fractures. It can increase the precision of fracture reduction and add the ability to detect concomitant intra-articular injuries reliably. This systematic review suggests that AORIF leads to improved functional outcomes for patients with similar morbidity compared to conventional ORIF, but AORIF comes with drawbacks such as additional operative time, expense, and needed expertise. Owing to the clinical heterogeneity and risk of bias of the included articles, further high-quality studies are required to clarify the benefits of AORIF and its place in clinical practice.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-1-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-2-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-3-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-4-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-5-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-6-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-7-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-8-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-jpg-9-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-9-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-png-10-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-png-10-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-png-11-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-png-11-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Supplemental Material
sj-png-12-hss-10.1177_15563316231204616 – Supplemental material for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis
Supplemental material, sj-png-12-hss-10.1177_15563316231204616 for Arthroscopy-Assisted Open Reduction Internal Fixation Versus Conventional Open Reduction Internal Fixation in the Treatment of Ankle Fractures: A Systematic Review With Meta-Analysis by Marc Meyer-Pries, Melika Hajymiri, Theodoros Lytras, Philip Manolopoulos and Dimitrios Ntourakis in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this review article.
Level of Evidence
Level IV, systematic review of level-III and level-IV studies.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.