
Abstract
Hip osteoarthritis (OA) is common but understudied compared with knee OA, and insights into the impact of this condition on the general population are needed. This review article summarizes findings from the 30-year, longitudinal, population-based Johnston County Osteoarthritis Project cohort to address the prevalence, incidence, and progression of hip OA and differences by sex and race; similarities and differences related to other joints; and impact on morbidity and mortality.
Compared with knee osteoarthritis (OA), hip OA is common but understudied, and insights into its impact on the general population are needed. The Johnston County Osteoarthritis (JoCo OA) Project is a vital source of such information. A longitudinal cohort involving more than 4000 unique participants, the JoCo OA followed participants for 30 years, from 1991 to 2018. It is a population-based prospective cohort, sampled from Black and White men and women 45 years of age and over living in Johnston County, North Carolina. This design provides a representative sample of the community because enrollment does not require symptoms, disease diagnosis, or risk factors; it includes both healthy people and those with OA at various joint sites [11]. The cohort is also generalizable to the U.S. population.
This article will summarize published research from the JoCo OA and address the following questions: How common is OA of the hip in the general population, and are there differences in key demographic subgroups? How is hip OA progression defined, and what is the frequency of progression in the general population? Compared with OA at other joint sites, does hip OA have unique risk factors or associations? Does hip OA contribute to morbidity and mortality?
The Johnston County Studies
The original JoCo OA cohort was enrolled in 1991 to 1997, and new participants were added to the study in 2003 to 2004. Participants had up to 4 main follow-up visits, approximately 5 years apart. Because JoCo OA was designed to be to assess potential differences by race, Black participants were oversampled to allow for meaningful analyses. This was done to allow for meaningful stratified analyses by race (which would not be possible with very small numbers in 1 category).
Given the aging of the cohort, we are now building on this extensive community infrastructure to enroll a new study, the Johnston County Health Study (JoCo HS), which has enrolled more than 650 at the time of the writing of this article. In recognition of the changing demographics of Johnston county and of OA, the JoCo HS includes Black, White, and Hispanic men and women aged 35 to 70 years in proportions reflective of the county as a whole.
The goal of the JoCo HS cohort is to be representative of the county’s population (~15% Black, 12% Hispanic). All visits included extensive self-report data (pain, function, medications, medical conditions, employment, etc), clinical examination, performance-based functional assessments, biospecimen collection, and multi-joint radiographs. Additional information such as dietary questionnaires, knee ultrasound, environmental exposures, and detailed psychosocial questionnaires is available at some time points. Extensive and unique information around OA, its risk factors, phenotypes, and progression, has been obtained from this remarkable resource over time, despite the significant challenges of maintaining a large longitudinal observational cohort for 30 years.
Both cohorts obtain full informed consent from all participants at all visits, and both are approved by the University of North Carolina Institutional Review Board.
Hip Osteoarthritis Prevalence, Incidence, and Progression
Although symptomatic hip OA affects up to 1 in 4 individuals by age 85 [15], it remains understudied compared with knee OA. In addition, while hip and knee OA are almost universally grouped together in management guidelines [5,12], the 2 entities have different prevalence, risk factors, phenotypes, and progression patterns indicating that optimal therapies may differ.
Hip OA is more difficult to diagnose than knee OA. Hip OA generally requires imaging for diagnosis, unlike knee OA which is a clinical diagnosis and does not require imaging in most cases (Fig. 1). The American College of Rheumatology (ACR) criteria for classification of hip OA (which have not been updated in more than 30 years) include frequent hip pain, a low sedimentation rate, femoral and/or acetabular osteophytes, and joint space narrowing [2]. Part of the challenge is in differentiating hip joint pain from that of the surrounding structures, including low back pain, trochanteric pain, and even intra-abdominal and intrapelvic pathologies [13]. In contrast, knee pain is more readily localized.
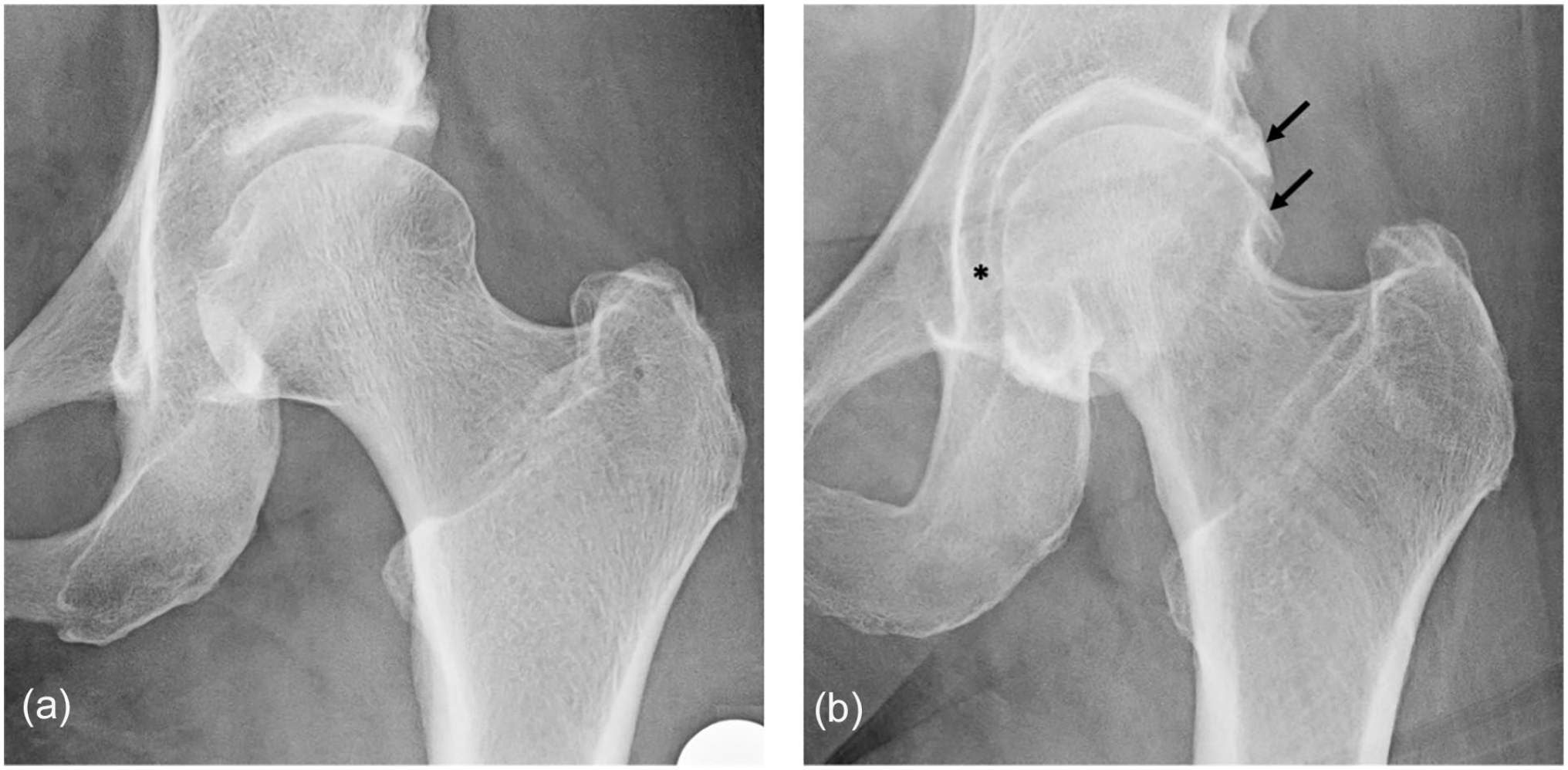
Radiographs of the right hip from 2 female JoCo OA participants: (a) Kellgren-Lawrence Grade (KLG) = 0 and (b) KLG = 3 with large osteophytes (arrows) and joint space narrowing (*). JoCo OA Johnston County Osteoarthritis Project.
Hip symptoms are frequent in the population, as is radiographic hip OA (rHOA), defined as a KLG of 2 or more (Fig. 1). Symptomatic hip OA (sxHOA), the combination of symptoms and rHOA, is less common, often around 10% [10]. Of note, while older studies [1,9] suggested that hip OA was uncommon among populations with African ancestry, in the JoCo OA we found the prevalence to be similar if not slightly higher among participants self-reporting as Black [10]. However, incidence rates for both rHOA and sxHOA were lower among Black compared with White participants [14]. As these data were from baseline, we recently updated the point prevalence of hip outcomes [18], demonstrating predictable increases in prevalence over time for rHOA and sxHOA with relatively stable reporting of hip symptoms. Prevalence was not consistently different by sex, race, or body mass index (BMI). Lifetime risk was slightly higher among women but relatively similar across race and BMI subgroups [15]. Therefore, hip OA is at least as common among Black people as it is in White people and is similar in frequency by sex. This is critical epidemiologic information, given the known disparities by race in hip arthroplasty [26].
In considering definitions of hip OA progressions that take race into account, we have found that radiographic progression (KLG increase of 1 or more, which occurred in about 15% of the sample) was less common in Black than in White participants. However, when progression was defined by worsening disability or loss of range of motion, Black participants experienced more progression [7]. Regarding radiographic progression, while KLG is a useful metric to define rHOA, it is insensitive to change. Joint space width (JSW), the distance between the femur and the acetabulum, is a more sensitive measure but can be assessed at several locations in the joint (eg, minimal JSW, or at fixed, defined locations), and as either a semiquantitative (ie, 0 to 3 joint space narrowing) or a quantitative 1 (qJSW, in mm). We used fixed qJSW, with locations (ie, 10°, 30°, and 50°) defined with respect to a polar coordinate system [24] as a more responsive measure of change in relation to development of rHOA [21]. We found that over a mean of 18 years, 20% and 12% of participants in the JoCo OA developed incident KLG-defined rHOA or sxHOA, respectively. Fixed qJSW at 50° was most sensitive to change over time with marked sex differences: while qJSW was stable among men, it declined over time in women. In addition, while heavier women lost more qJSW, other changes in qJSW were not significantly associated with race, education, or injury in women or men. In women only, loss of qJSW over time was associated with 2 to 3 times higher odds of rHOA and sxHOA; having a narrower baseline qJSW was associated with these outcomes among both women and men [21]. These data indicate that the choice of progression metric (eg, KLG change vs qJSW change) has substantial impact on the frequency of progression in a given population. This choice should, therefore, be carefully considered in the context of a given analysis.
Morphology
The shape of the proximal femur and acetabulum, both alone and in combination, constitutes an important risk factor for development of hip OA [16,27]. We have explored hip shape using standard geometric measures, and we have used statistical shape modeling to examine more subtle global shape variations [4,19,23]. Our initial work confirmed that variations in proximal femoral shape were associated with incident hip OA [19]. Due to limitations in utilizing principal component analysis for statistical shape modeling, we applied novel methodologies tailored to high-dimensional, low-sample-size data to better understand potential subgroups in hip shape by sex and race [4]. This approach improved understanding of shapes associated with rHOA and identified shape associations that occurred exclusively in Black women with rHOA [4].
In addition, because of the population-based design of JoCo OA, we were able to estimate the prevalence of various hip morphologies by sex and race from the baseline visit, in more than 5000 hips. Cam morphology was present in more than 25% of men and 10% of women, while mild dysplasia was common in about 33% of hips overall. Pincer morphologies (<10% overall) were seen less commonly in men than in women. Overall, prevalence by race was similar although Black participants had higher frequencies of protrusio acetabuli [25].
Using a nested case-control design, we then identified hips that developed definite rHOA (KLG of 3 or more or total hip replacement) more than 13 years of follow-up (cases, n = 71) and compared these to control hips (KLG <3 at all visits, n = 168) using radiographic measures of cam and pincer morphologies. We found that case hips had more evidence of cam morphology in both men and women, while protrusio acetabuli (which occurs when the femoral head overlaps the ilioischial line) was associated with hip OA only among women. Coxa profunda (when the floor of the acetabular fossa touched or overlapped the ilioischial line medially) was very common and not associated with the development of OA [23], and is likely a shape variant without significant clinical impact.
Hip Osteoarthritis Does Not Exist in Isolation
Although “generalized OA” is a common phrase, it does not have a standard clinical or research definition. Its meaning is often simplified as hand OA with involvement of any other site—this overlooks the complexity of the presentation and burden of OA at joints across the body [22]. Of note, hip OA is sometimes postulated to exist separately from the idea of multiple-joint OA (MJOA). Indeed, in our work, we have seen that the hip is more often affected in isolation than in combination with other sites [20]. However, Black participants in the JoCo OA were more likely to have multiple large joint (knee, spine, and/or hip) involvement, despite having substantially less frequent hand involvement, for both radiographic and symptomatic MJOA constructs [17,20]. The overall burden of MJOA is high in JoCo OA, and involvement of other joints should be a part of OA assessment, regardless of the index joint [8]. The hip may be part of the MJOA construct in the lower extremity and may impact populations differently.
Morbidity and Mortality
Hip symptoms are related to other chronic conditions and are associated with higher mortality rates. We have studied patterns of transition in hip OA, from no symptoms and no rHOA to radiographic and/or symptomatic states in conjunction with comorbid conditions. We found that while obesity was associated with the development of symptoms, diabetes and/or cardiovascular disease made resolution of symptoms less likely (or more persistent). In addition, Black participants with diabetes had increased hazards of developing sxHOA in this analysis [3].
The presence of hip symptoms is also associated with excess mortality. In comparison with individuals with neither pain nor rHOA, participants in the JoCo OA with hip symptoms had approximately 30% increased hazards of mortality [6]. This was regardless of whether the symptoms were in conjunction with or separate from structural changes of OA on radiographs, and independent of age, sex, race, education, hip injury, use of nonsteroidal anti-inflammatory drugs, smoking, alcohol use, physical activity, disability, 6 comorbidities, BMI, and the presence of low back pain. Understanding the association between symptoms and mortality, even without concomitant OA changes, is an area of active study.
Conclusion
The JoCo OA project has provided many insights into the epidemiology of hip OA in diverse populations. Its population-based design makes these findings more generalizable than other study designs, and the JoCo HS will extend this generalizability into a current, inclusive cohort studying OA and other chronic conditions. Hip OA is a common condition with substantial impact on morbidity and mortality in affected individuals and has risk factors that are unique to this body site. Improved understanding of such risk factors will inform improved targeted management strategies in the future.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231192372 – Supplemental material for Epidemiology of Hip Osteoarthritis: The Johnston County Osteoarthritis Project
Supplemental material, sj-docx-1-hss-10.1177_15563316231192372 for Epidemiology of Hip Osteoarthritis: The Johnston County Osteoarthritis Project by Amanda Nelson in HSS Journal®
Footnotes
Acknowledgements
Many thanks to Yvonne Golightly, PT, PhD, for inputs and edits on this manuscript, and to the staff and participants of the Johnston County studies, without whom none of this work would be possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Arthritis Foundation and Hospital for Special Surgery funded the 2023 Hip Osteoarthritis Clinical Studies Conference, with support from Stryker, Alexion, and Smith+Nephew. Cited work funded in part by NIH/NIAMS K23AR061406, L30AR056604, P60AR064166, and P30AR072580; CDC U01DP006266.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was obtained for all patients included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.