
Abstract
Background: Spinal instrumentation in children with congenital spine deformity poses challenges to the surgeon, given the small patient size and the anomalous anatomy often encountered. Purpose: We aimed to investigate the accuracy of screw placement when robotics coupled with real-time navigation was used for surgical treatment of pediatric congenital spine deformity at 1 institution. Methods: We conducted a retrospective search of our institution’s database for all patients younger than 18 years of age with congenital spine deformity who were treated with the robotics surgical platform coupled with navigation between June 2019 and December 2020. We recorded data on demographics, location and type of anomaly, procedure performed, and intraoperative variables related to robotics and navigation. We reviewed the images of patients who had intraoperative 3-dimensional imaging or postoperative computed tomographic scans to determine the accuracy of screw placement using the Gertzbein-Robbins scale. Results: In 14 patients identified, a total of 95 screws were attempted, with 94 successfully placed using robotics coupled with navigation. There were no noted screw-related complications (neurologic or visceral) and no return to the operating room for screw malposition. Conclusion: Patients with congenital spine deformity present potentially unique challenges due to variant anatomy. This retrospective series suggests that robotics coupled with navigation for congenital spine deformity correction in the pediatric population may aid in accurate screw placement and reduce complication rates. More rigorous study is warranted.
Introduction
The surgical treatment of congenital spine deformities ranges from in situ fusion to complex osteotomies. Regardless of the magnitude of surgery, stable fixation leads to improved arthrodesis rates and patient outcomes [6]. Spinal instrumentation has evolved to 3-column fixation using pedicle screws even in the smallest of children. Pedicle screw instrumentation remains challenging given the patient size and anomalous anatomy; malpositioned implants are the most common cause of reoperation in pediatric spine deformity [1,10,12,14].
The advent of computer-assisted navigation (CAN) in pediatric spine deformity has led to increased screw accuracy and diminished return to the operating room for screw malposition [9]. While the majority of the pediatric spine literature reporting on CAN safety and accuracy focuses on adolescent idiopathic scoliosis (AIS), there are reports of screw accuracy rates of 99% when CAN is used for congenital scoliosis [8]. Similarly, initial reviews of robotic-assisted spine surgery have been centered around AIS, with Devito et al [2] reporting on increased accuracy rates for pediatric spine deformity compared with freehand techniques. Previously, robotic platforms have not been associated with CAN until the Food and Drug Administration clearance of robotics coupled with navigation in 2019. The promise of this technology is based on the ability to study anatomy and plan screw placement, the use of a robotic arm to guide trajectory of instrumentation and screw placement, and the coupling with real-time navigation that confirms appropriate implant placement.
Currently, there are few reports in the literature on robotics coupled with navigation in pediatric spine deformity [5]. We found no reports on this evolving technology in patients with congenital spine deformity. We present our initial experience with robotics coupled with real-time navigation to address pediatric congenital spine deformity.
Methods
Our Institutional Review Board approved this study. We searched our surgical database for patients aged less than 18 years old who were treated with the surgical platform of robotics coupled with navigation since June 2019. The database search was then refined to include patients with a congenital spine deformity. Recorded data included demographics, location and type of anomaly, and the procedure performed. Data on intraoperative variables related to robotics and navigation were also recorded. Intraoperative problems with the surgical platform, failure to place pedicle screws, and any complications were documented. We reviewed images of patients who had intraoperative 3-dimensional (3D) imaging or postoperative computed tomographic (CT) scans to determine the accuracy of screw placement using the Gertzbein-Robbins scale. This grading system reflects deviation of the screw from the intrapedicular trajectory, with grade A being fully intrapedicular, grade B exceeding the pedicle cortex <2mm, grade C exceeding the cortex 2–4 mm, grade D exceeding the cortex 4–6 mm, and grade E exceeding the cortex >6 mm [4].
Case Example
The patient was a 33-month-old girl who presented to an outside institution with a noted lumbar deformity and gait abnormality related to calf atrophy and heel cord tightness. Imaging studies revealed a congenital dislocation of the lumbar spine with thecal sac compression and spinal cord syrinx (Figs 1 and 2). She had normal urodynamic studies with gross motor strength intact, heel cord tightness, and calf atrophy. Given her significant deformity, neurologic compression, and potential for deformity progression, a decision was made to proceed with vertebral column resection with decompression and short-segment fusion with longer instrumentation to enhance stability and minimize fusion length.

Sagittal MRI of 33-month-old patient with congenital dislocation of spine, lumbar compression, and spinal cord syrinx. MRI magnetic resonance imaging.

Sagittal CT scan of patient detailing bony anatomy. CT computed tomography.
She was taken to the operating room where standard anesthetic techniques were used with neurophysiologic monitoring. Standard midline exposure was performed between L2 and L4 with extraperiosteal exposure of L1 and L5 to preserve the facet joints and prevent exposure in a subperiosteal manner.
A preoperative CT scan was done under a pediatric robotic protocol to allow for intraoperative registration by fluoroscopy to be coupled with the CT scan. The preoperative CT scan images were evaluated with computer software to allow for planning of screw length, diameter, and trajectory. A Schanz pin was placed in the right posterior superior iliac spine (PSIS), and the robotic mount was performed, followed by registration of the navigation system. Two orthogonal fluoroscopic images were taken and successfully registered to the preoperative CT scan.
Next, we placed pedicle screws under robotic guidance and navigation bilaterally at L1 and L2, followed by screws at L4 and L5 on the left side. Given the patient’s small size, the robotic mount interfered with the robotic trajectory on the right side. We then elected to place a left-sided PSIS pin and reregistered the anatomy using 2 fluoroscopic images. Successful registration was followed by robotic-assisted placement of screws at L4 and L5 on the right side (Fig. 3).
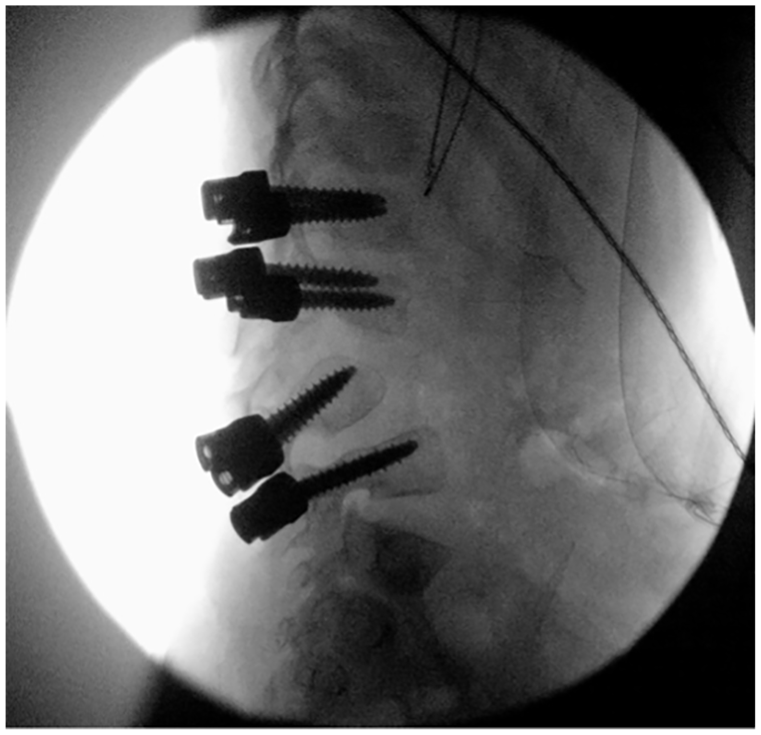
Intraoperative fluoroscopic view showing anatomical trajectory of robotically placed screws.
We proceeded with a complete vertebral column resection of L3 with disk removal at L2–L4 (Fig. 4), followed by placement of an interbody cage and compression instrumentation with correction of the deformity. Neurophysiologic monitoring remained normal throughout. Decortication between L2 and L4 was performed, taking care not to expose any more of the adjacent levels. The patient woke from anesthesia with a normal neurologic examination. Postoperative CT scan revealed complete containment of all pedicle screws with excellent thecal decompression and local alignment (Figs 5 and 6). The patient was scheduled to return in 6 months to shorten the instrumentation to include only L2–L4 into the final fusion.
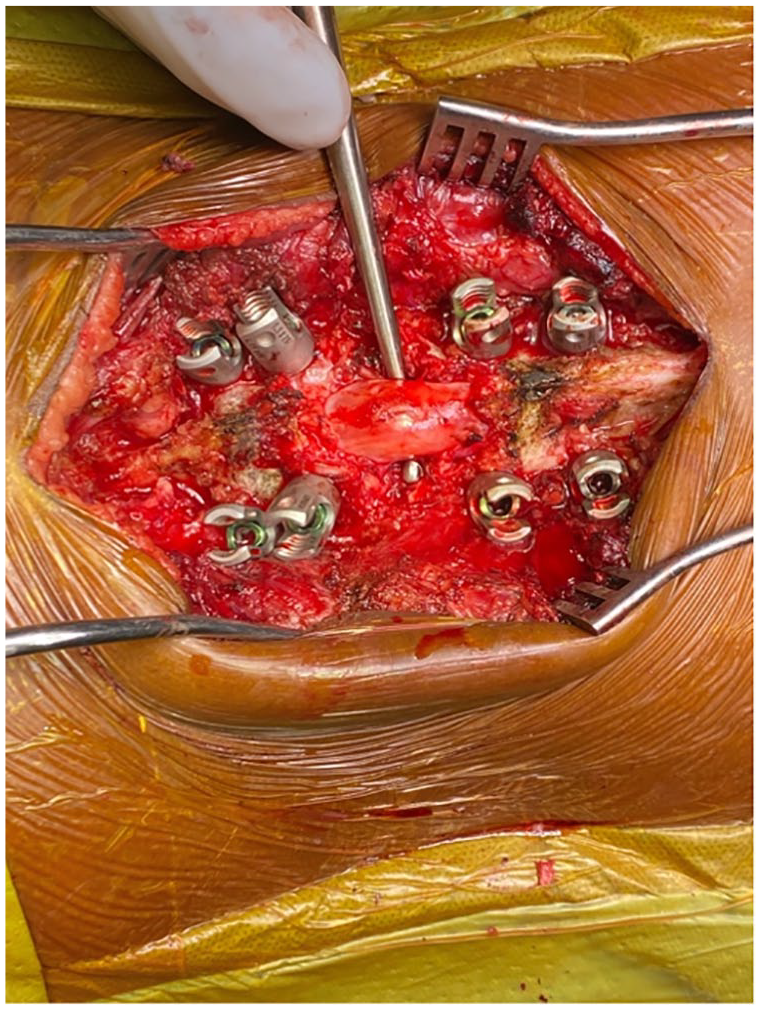
Intraoperative photo showing complete VCR with circumferential decompression of dural sac. VCR vertebral column resection.

Coronal CT documenting containment of pedicle screws. CT computed tomography.

Sagittal CT documenting decompression and restoration of alignment with intervertebral cage placement for anterior column support and arthrodesis. CT computed tomography.
Results
We identified 14 patients at Boston Children’s Hospital who underwent surgical treatment for a congenital spine deformity with the assistance of robotics coupled with navigation between June 2019 and December 2020. The mean age of the patients was 11.8 (3–16) years, and the mean body mass index was 18.1 (16.3–23.6) kg/m2. The diagnoses treated were 4 hemivertebra, 1 congenital kyphosis, 3 congenital spondylolisthesis, 4 mixed anomalies, and 2 lumbosacral anomalies. The mode of registration included 4 patients who had a preoperative CT registered to intraoperative fluoroscopy and 10 patients who had an intraoperative registration using 3D imaging (O-arm). The mean number of levels fused was 5 (range, 2–13). The mean operative time for the robotic portion of the case was 57 (range, 33–100) minutes. This time is defined from beginning of placing the robotic mount to the end of robotic screw placement. The total mean operating room time was 5.1 (2–8.42) hours, and the mean estimated blood loss was 250 (50–650) mL.
A total of 95 screws were attempted, with 94 successfully placed using robotics coupled with navigation. The mean number of screws placed was 7 (range, 3–11). Eight of the 14 patients had sacral-pelvic fixation. All screws were placed successfully with the exception of 1 screw noted on fluoroscopy to be laterally deviated in the pedicle of L5 that was subsequently replaced by freehand technique. The lateral deviation was thought to be caused by excessive soft tissue pressure on the robotic arm. Of the 94 executed screws, 52 had additional postscrew placement using either O-arm or postoperative CT scans. All these scans were reviewed and screws graded per the Gertzbein-Robbins classification. Ultimately, all the 52 screws were noted to be accurate and graded as either A or B. The mean operative time for the robotic portion of the case was 57 (range, 33–100) minutes. This time is defined from the beginning of robotic mount to the end of robotic screw placement. There were no noted screw-related complications (neurologic or visceral) in this series and no return to the operating room for screw malposition; no intraoperative problems related to the robotic platform, no registration difficulties, and no technical problems that altered the operative plan were noted.
Discussion
Stable fixation of the spine via pedicle screws is crucial in spinal deformity surgery. Malpositioned screws, while uncommon, may lead to neurologic deficit, diminished correction, pseudarthrosis, and return to the operating room for revision [12]. Multiple techniques exist for placement of pedicle screws and include freehand placement, fluoroscopically assisted placement, and navigation-assisted placement. The use of CAN was developed to reduce error pedicle screw placement, with the greatest promise in cases where anatomical distortions are present [8,9], most notably revision cases, syndromes such as neurofibromatosis, and congenital spine deformities. Little literature exists on the optimal techniques for placing instrumentation in pediatric patients with congenital deformities despite studies concluding its use is safe and efficacious.
The adoption of robotics by the spinal deformity community has evolved over the last 2 decades; multiple studies suggest improved accuracy and decreased radiation exposure for pedicle screw placement [6,7,11,13]. Although many of these studies focus on the adult spinal deformity population, the use of robotics in children with idiopathic scoliosis is described with positive results [8]. One of the pitfalls in robotics has been the surgeon’s lack of tactile feel when placing screws, coupled with no visual feedback on the anatomical trajectory. The coupling of navigation with robotics has evolved over the last decade to involve systems with a platform that includes preoperative planning software, a robotic arm for trajectory guidance, and real-time computer navigation allowing for visual confirmation of 3-dimensional anatomy [5]. The robotic arm includes an optic camera that allows the robot to perform a 3D assessment of the work to self-reference its location and provide collision avoidance intraoperatively [3].
Our series is the first description of using this technology for congenital spine deformities. Patients with congenital spine deformities remain a challenging subset of patients with pediatric spine deformity given their small stature and their anomalous anatomy. The standard means of registration for this platform may done in 1 of 2 ways: a preoperative CT scan registered to intraoperative fluoroscopic images or by obtaining intraoperative 3D imaging such as with an O-arm. This population of patients presents potentially unique challenges with robotics and navigation, which is worthy of study. Notably, from a planning standpoint, registering the patient’s variant anatomy could present a problem for the computer software, as the programs are built according to normal vertebral anatomy. We had no issues with registering the patient’s anatomy with the computer software program and thus the surgical planning program. There were no noted screw-related complications in this series and no return to the operating room for screw malposition. All screws were placed accurately with Gertzbein-Robbins classification grade A or B. We noted no intraoperative problems related to the robotic platform. We hope to study patient outcomes and complication rates of robotics coupled with navigation in a larger cohort of pediatric patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV: Retrospective Therapeutic Study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.