
Abstract
Many institutional review board (IRB) members often classify online sexual and behavioral health surveys as not meeting the minimal risk standard under the Code of Federal Regulation (CFR) due to concerns that answering sensitive or controversial topics may cause discomfort. However, college students’ comfortability in responding to such topics remains unknown. Undergraduate college students (n = 123) were asked about their comfort level in answering online survey questions about their sexual behaviors, alcohol use, drug use, and mental health. Additionally, the study examined demographic differences in comfort levels. Few participants reported overall discomfort when answering online survey questions about their sexual and behavioral health, and minimal demographic differences were found. Some IRB members may overestimate the discomfort participants experience when answering surveys about sexual behaviors, substance use, and mental health. Findings support the argument that online sexual and behavioral health surveys may meet the CFR criteria for minimal risk.
Introduction
Many institutional review board (IRB) members (Peter & Friedland, 2017; Petrie et al., 2013) and experts (Gfroerer & Kennet, 2014; Smith, 2014; Tourangeau & Smith, 1996; Tourangeau & Yan, 2007) perceive survey questions about sex, substance use, and mental health as exceeding the minimal risk standard. The Code of Federal Regulations (CFR) defines minimal risk as, “the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests” (U.S. Department of Health and Human Services, 2021).
Although IRB members and experts assume sexual and behavioral health survey questions could cause discomfort, embarrassment, and other distress in respondents, studies have contradicted this assumption. Indeed, prior studies reported that few participants reported feeling discomfort when answering survey questions about these health behaviors, with discomfort levels comparable to or lower than those experienced during routine daily activities or medical tests, such as taking a school exam or being asked about substance use by a doctor (Fendrich et al., 2003; Fendrich et al., 2007; Jacomb et al., 1999; Kaniuka et al., 2022; Kuyper et al., 2012; Langhinrichsen-Rohling et al., 2006; Macapagal et al., 2017; Macapagal et al., 2019; Mustanski, 2011; Petrie et al., 2013).
Ethics research on participants’ discomfort, distress, and other attitudes toward answering sensitive health topics has largely been overlooked in the literature (Fendrich et al., 2003; Fendrich et al., 2007), a gap that is especially evident for college students. However, college students exhibit higher rates of adverse health outcomes and risky health behaviors, particularly poor mental health, substance misuse, and risky sexual behaviors (American College Health Association, 2024; Stroud et al., 2015). Most research on participant distress when answering controversial health topics has focused on lesbian, gay, bisexual, transgender, queer, and other sexual and gender minority (LGBTQ) adolescents and young adults (Fendrich et al., 2007; Kaniuka et al., 2022; Macapagal et al., 2017; Macapagal et al., 2019; Montemayor & Owens, 2025; Mustanski, 2011). We found only one study, conducted in New Zealand, that compared university students’ distress while participating in various research protocols (including health surveys) to routine daily activities and medical examinations (Petrie et al., 2013). Petrie et al. (2013) revealed that most university students do not experience distress when answering various health topics (e.g., sex, drug use) compared to completing routine daily and medical tests.
Despite college students being over-sampled in health behavior survey research (Pokhrel et al., 2014), their opinions about the risks and benefits of participating in such research is not well understood. Furthermore, existing studies have almost exclusively reported descriptive data on comfort levels, despite some studies demonstrating demographic differences in comfort levels (Fendrich et al., 2003; Fendrich et al., 2007; Jacomb et al., 1999; Langhinrichsen-Rohling et al., 2006). These gaps in the literature highlight a critical need for research that explores college student's comfort in answering questions around sensitive health behaviors, while also examining demographic differences in comfort levels. It is crucial to investigate research participants’ attitudes towards research protocols to better understand the unique benefits, risks, and protections that may differ from the perspectives of investigators or IRB members (Fisher, 2004). The aims of this study were to: 1) assess undergraduate college students’ comfort levels in answering health questions in online surveys, and 2) identify demographic differences in these comfort levels. A better understanding of their comfort and demographic differences can help inform best practices in the conduct of research.
Methods
Recruitment
This study was conducted at a large public university in the Southern U.S. region, with an undergraduate population of over 55,000 students during the 2023–2024 academic year. The research team requested a simple random sample of 500 undergraduate students from the university's institutional research office, drawn from students who were attending the university during the Spring 2024 semester. Students were randomly selected using the institutional research office's enrollment portal to ensure the sample was representative of the undergraduate student body. Accordingly, no stratification by academic major, gender, or class standing was requested. The office provided the research team a list with the students’ email address, gender, academic class standing, and academic major. The sample size of 500 was selected based on the financial restraints of the project, as participants who completed the study received a $15 Amazon e-card ($7,500 maximum in participation incentives).
The research team then created a Qualtrics directory comprised of the 500 students’ email addresses and invited them to complete an online cross-sectional survey. The survey itself was part of a more extensive study of the sexual behaviors, sexual health testing preferences, and health research attitudes of university undergraduate students. Individuals were eligible if they were 18 years old or older and enrolled as an undergraduate student at the university. The recruitment period lasted from February 7 to 28, 2024. The Texas A&M University IRB approved the study protocol on January 9, 2024 (STUDY2023-0057). Participants provided electronic informed consent.
Participants
One-hundred and twenty-three students completed the survey, resulting in a 25% response rate. Gender, academic class standing, and academic major (Science, Technology, Engineering, and Mathematics [STEM] and non-STEM) were compared among respondents and nonrespondents (see Supplemental Table 1). Female students were significantly more likely to complete this survey than male students (χ2 = 9.99, p = .002). This finding is consistent with prior research showing higher survey response rates among women (Jouriles et al., 2022; Porter & Whitcomb, 2005; Standish & Umbach, 2019). No other significant differences were found.
Additionally, Table 1 presents the demographic characteristics of the 123 respondents and compares them to institutional enrollment data for Fall 2024 (when available). Most respondents were female (59.3% v. 47.0% of the total student body). The vast majority self-identified as heterosexual (83.7%), followed by 10.6% as bisexual, 4.9% as gay or lesbian, and 0.8% as pansexual. Racial/ethnic proportions were similar to undergraduate enrollment: Non-Hispanic White (46.3% v. 52.7%), Hispanic (25.2%v. 25.0%), Asian (18.7% v. 13.9%), Black (1.6% v. 3.1%), and other racial/ethnic identities (8.1% v. 5.4%). About one-quarter of respondents were first-generation students (24.4%), compared to about one-fifth of the total student body (19.7%).
Demographic Characteristics (N = 123).
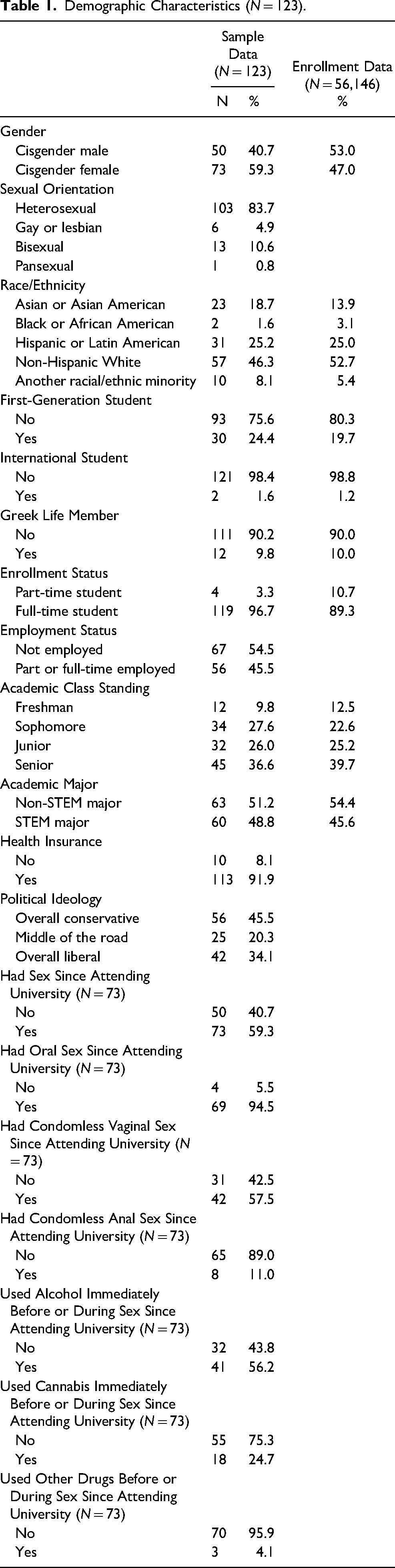
Domestic and international student status was comparable (1.6% of our sample v. 1.2% campus-wide). Fraternity and sorority membership (9.8% v. 10.0%), full-time enrollment (96.7% v. 89.3%) and academic class standing (freshmen: 9.8% v. 12.5%; sophomores: 27.6% v. 22.6%; juniors: 26.0% v. 25.2%; seniors: 36.6% v. 39.7%) were all proportionate. Nearly half of our sample (48.8%) majored in a STEM field, comparable to the full student body (45.6%). Nearly all respondents had health insurance (91.9%), and half were politically conservative (45.5%).
Over half of the respondents reported having sex since attending the university (59.3%). Of the students who reported having sex, 94.5% reported engaging in oral sex, 57.5% reported engaging in condomless vaginal sex, and 11.0% reported engaging in condomless anal sex. Finally, over half of the students who reported having sex also reported using alcohol immediately before or during sex (56.2%), while 24.7% reported using cannabis immediately before or during sex. Additionally, 4.1% reported using other drugs immediately before or during sex.
Measures
Comfort with Health Survey Topics
Participants answered the question matrix, “How comfortable or uncomfortable would you be in answering online survey question about:” and rated four topics separately on a 5-point scale (1 = very uncomfortable, 5 = very comfortable). These matrix items asked participants about their sexual behaviors, alcohol use, drug use, and mental or emotional health. The researchers did not formally provide a definition of “comfort,” thus, participants responded based on their own interpretation of the term which was guided by our wording. Responses were then recoded as overall uncomfortable (coded as 0, very uncomfortable/somewhat uncomfortable/neither comfortable nor uncomfortable) or overall comfortable (coded as 1, very comfortable/somewhat comfortable). We coded neither comfortable nor uncomfortable as overall uncomfortable, consistent with prior studies (Kaniuka et al., 2022; Macapagal et al., 2017; Montemayor & Owens, 2025).
Demographics
Academic major was reclassified as STEM and non-STEM. STEM majors included if the academic major was in agricultural science, natural resource and conservation, architecture, computer and information science, engineering, biological and biomedical science, mathematics and statistics, and physical science disciplines (National Science Foundation, n.d.). Academic class standing was reclassified as upper level (senior or junior-level credit) and lower level (freshman or sophomore-level credit).
Variables were recoded for analyses with the reference group (ref) coded as 0: gender (0 = cisgender male, 1 = cisgender female), sexual orientation (0 = sexual minority, 1 = heterosexual), race/ethnicity (0 = Non-Hispanic White, 1 = racial/ethnic minority), first-generation student status (0 = no, 1 = yes), international student (0 = no, 1 = yes), Greek Life member (0 = no, 1 = yes), enrollment status (0 = part-time enrollment, 1 = full-time enrollment), employment (0 = not employed, 1 = employed part or full-time), academic class standing (0 = lower division, 1 = upper division), academic major (0 = non-STEM, 1 = STEM), health insurance (0 = no, 1 = yes), political ideology (0 = overall liberal or middle of the road, 1 = overall conservative), had sex (0 = no, 1 = yes), had oral sex (0 = no, 1 = yes), had condomless vaginal sex (0 = no, 1 = yes), used alcohol before/during sex (0 = no, 1 = yes), used cannabis before/during sex (0 = no, 1 = yes), and used other drugs before/during sex (0 = no, 1 = yes).
Analysis
We conducted analyses using SPSS (Version 29). There was no missing data to address. We analyzed data with descriptive statistics: number (n) and percentage (%). A series of chi-square tests of independence (χ2) were conducted to assess the correlation between demographic independent variables and the four dependent variables: overall comfortable answering sexual behavior questions, alcohol use questions, drug use questions, and mental health questions. Statistically significant (p < .05) and marginally significant variables (p ≤ .10) in the bivariate analyses were added to a series of multiple logistic regression models. Adjusted odds ratio (aOR), 95% confidence intervals (CI), and p of < .05 was statistically significant.
Results
Demographic Characteristics
Aim 1: Comfort Levels Answering Online Health Surveys
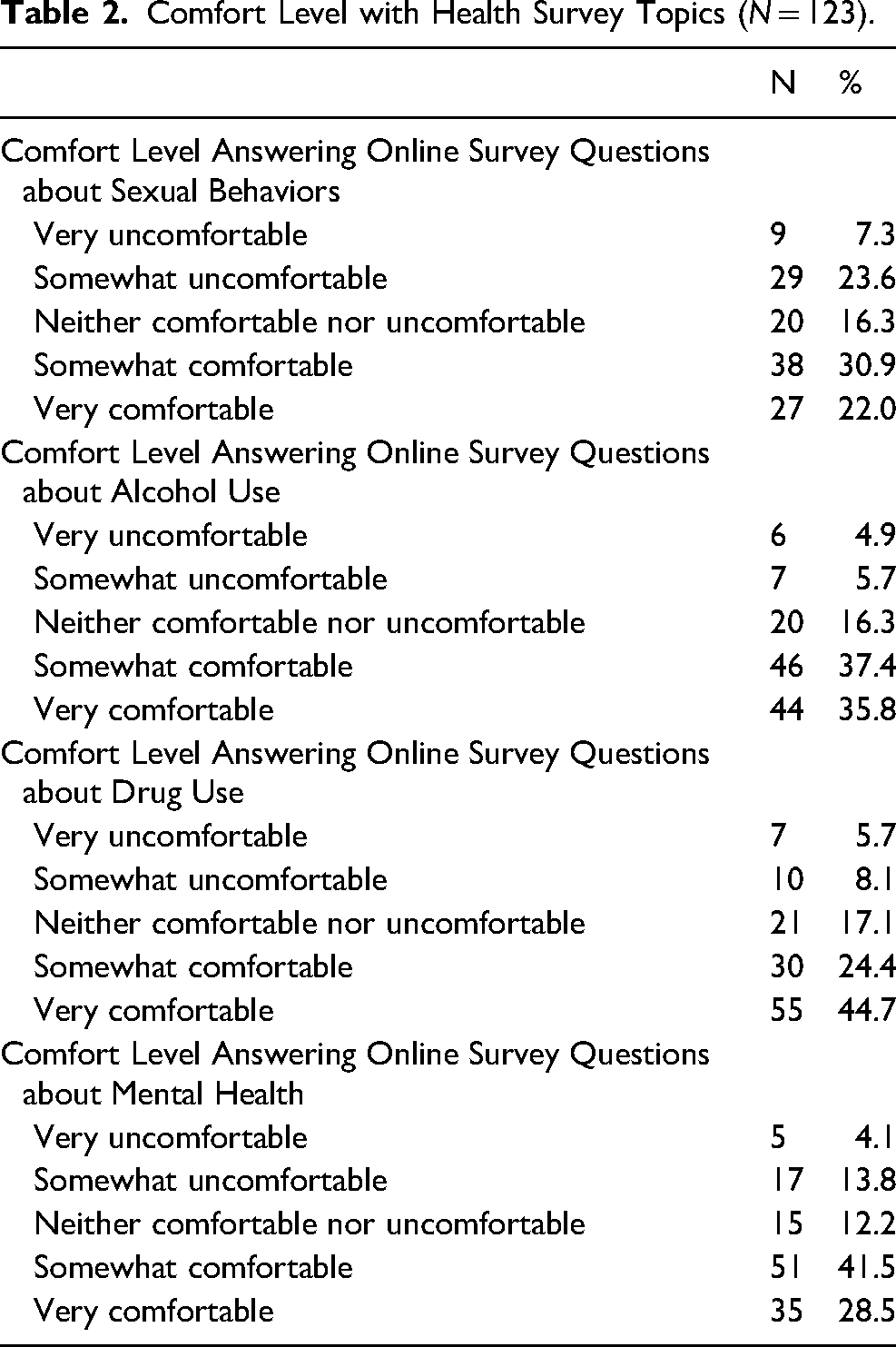
Table 2 shows the descriptive statistics of comfort level in answering various health topics. Though an overwhelming majority of students reported being very or somewhat comfortable answering online survey questions about their alcohol use (73.2%), drug use (69.1%), and mental health (69.9%), only about half of students reported being overall comfortable answering questions about their sexual behaviors (52.8%). Alternatively, less than ten students reported being very uncomfortable answering online survey questions about their sexual behaviors (n = 9, 7.3%), alcohol use (n = 6, 4.9%), drug use (n = 7, 5.7%), and mental health (n = 5, 4.1%).
Comfort Level with Health Survey Topics (N = 123).
Aim 2: Comfort Level Variation by Demographics
Sexual Behavior Online Survey Questions
As displayed in Table 3, sexual orientation was marginally correlated with being overall comfortable answering online survey questions about sexual behaviors (χ2 = 2.82, p = .093). Additionally, using alcohol before/during sex was significantly correlated with being overall comfortable answering online survey questions about sexual behaviors (χ2 = 12.76, p < .001). The multiple logistic regression model examining the association of these two demographic factors (i.e., sexual orientation and alcohol use before/during sex) with comfort answering online survey questions about sexual behaviors was statistically significant, χ2(2) = 16.89, p < .001 (see Table 4). The model explained 28% of the variance, and the data fit the model well (p = .546). Students who used alcohol immediately before/during sex were six times more likely to be very or somewhat comfortable answering sexual behavior online survey questions compared to students who did not use alcohol before/during sex (aOR = 6.76, 95% CI: 2.31–19.73, p < .001).
Bivariate Analyses.
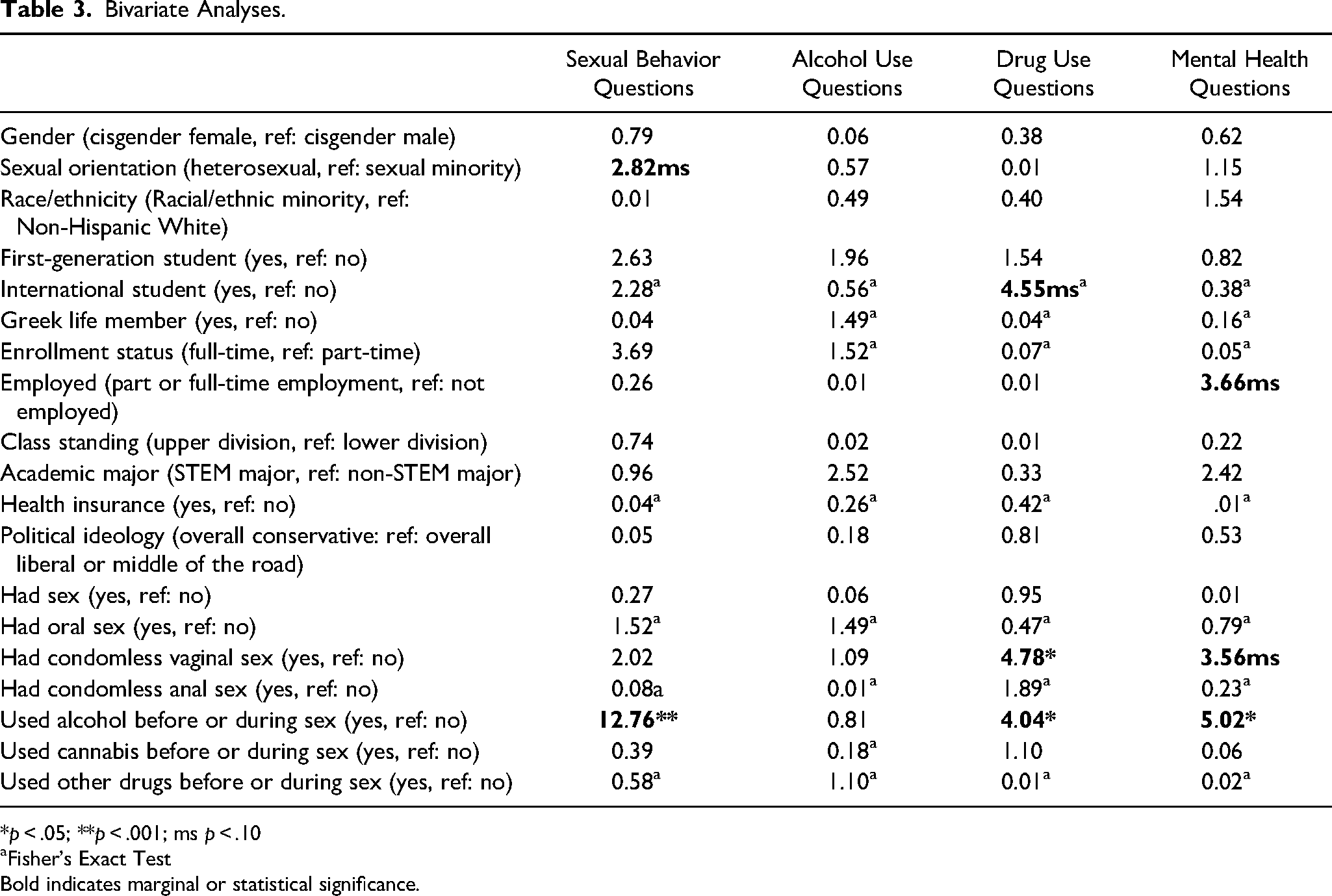
*p < .05; **p < .001; ms p < .10
Fisher's Exact Test
Bold indicates marginal or statistical significance.
Multiple Logistic Regressions: Comfort with Health Survey Topics.
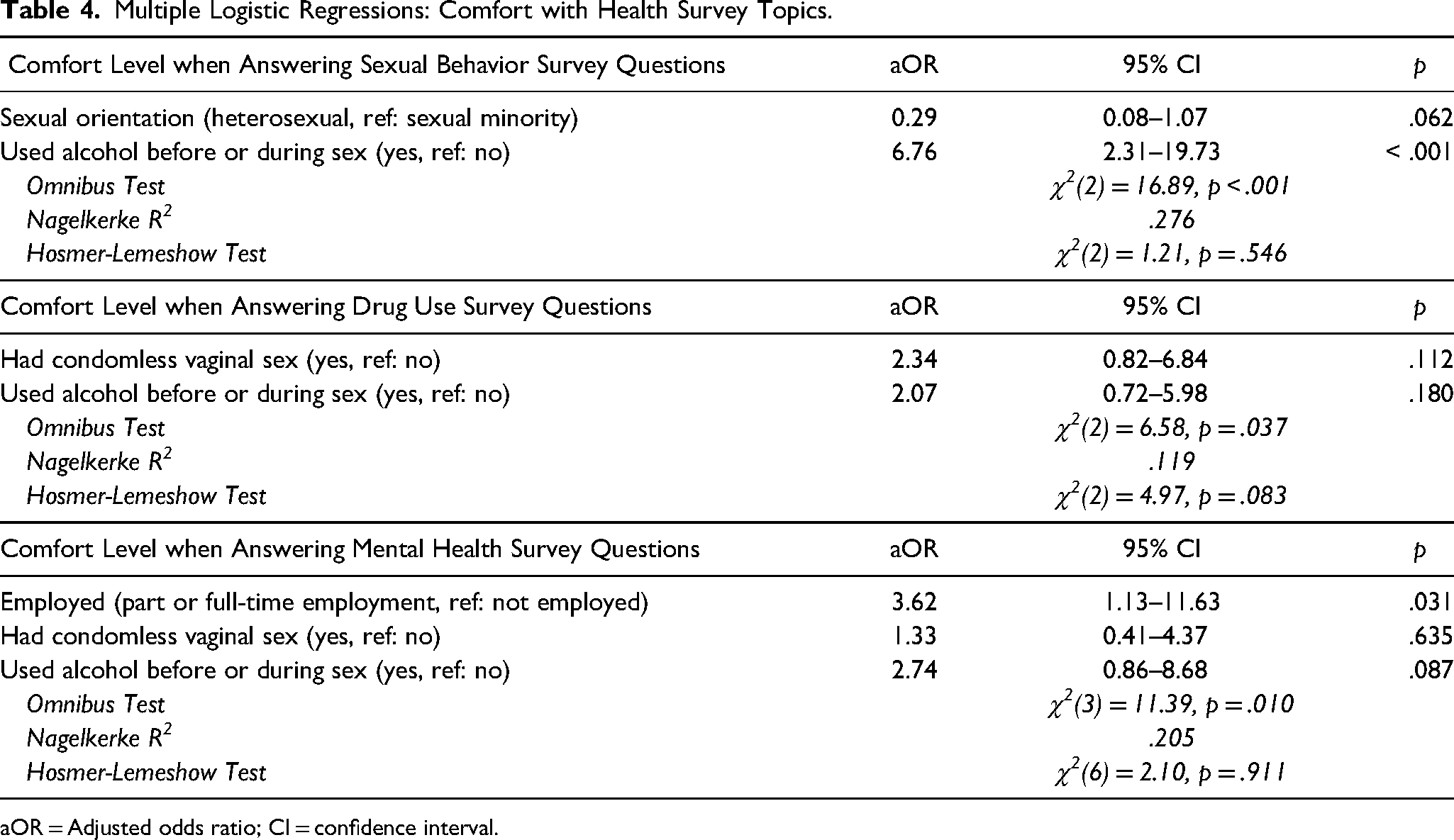
aOR = Adjusted odds ratio; CI = confidence interval.
Alcohol use Online Survey Questions
As seen in Table 3, there were no demographic differences found to be of marginal or statistical significance with comfort levels associated with answering online survey questions about alcohol use.
Drug use Online Survey Questions
The data in Table 3 reveals that being overall comfortable answering online survey questions about drug use behaviors was correlated with international student status (χ2 = 4.55, p = .094), condomless vaginal sex (χ2 = 4.78, p = .029), and using alcohol before/during sex (χ2 = 4.04, p = .045). However, none of these demographic variables predicted comfort level in answering drug use survey questions, as seen in Table 4.
Mental Health Online Survey Questions
Employment status (χ2 = 3.66, p = .056), condomless vaginal sex (χ2 = 3.56, p = .059), and using alcohol before/after sex (χ2 = 5.02, p = .025) were correlated with being very or somewhat comfortable answering mental health online survey questions. As displayed in Table 4, the logistic regression model was statistically significant (p = .010), explained 20.5% of the variance, and fit the data well (p = .911). Students who were working part or full-time were three times more likely to be overall comfortable answering online survey questions about mental health (aOR = 3.62, 95% CI: 1.13–11.63, p = .031) than unemployed students.
Discussion
Undergraduate college students are often asked to participate in online health surveys that ask controversial questions about relevant issues, such as their sexual behaviors, their substance use, and their mental health. However, little is known about college students’ comfort in answering such questions or how comfortability may vary across different demographics. Additionally, there is a standing belief among IRBs and other experts that these questions do not meet the minimal risk standard for adolescents, college students, and other young adults. Our study tested this assumption by examining the comfort levels in answering online survey questions about four health topics and assessing demographic differences among undergraduate students attending a large public university in the Southern region of the U.S. We describe below how the implications of our findings counter the opinions of some IRB members and other experts, inform the conduct of health behavior survey research, and guide future research.
Findings Compared to the Literature
Our findings suggest that among respondents, who were mostly cisgender heterosexual women, upperclassmen, and majoring in STEM, the majority reported feeling comfortable answering survey questions about their alcohol use, drug use, and mental health. This finding aligns with the literature where most adolescents (Langhinrichsen-Rohling et al., 2006; Macapagal et al., 2017; Macapagal et al., 2019; Mustanski, 2011) and adults (Fendrich et al., 2003; Fendrich et al., 2007; Jacomb et al., 1999; Kaniuka et al., 2022; Petrie et al., 2013) are comfortable answering survey questions about their substance use and mental health.
However, we observed that most of our sample experienced higher levels of discomfort when answering online survey questions about their sexual behaviors compared to the other three topics. The literature is mixed when comparing comfort levels across topics. Kaniuka et al. (2022) reported similar levels of comfort for sexual behavior and drug questions. In contrast, Mustanski (2011) and Petrie et al. (2013) found that answering sexual behavioral questions was slightly more uncomfortable than behavioral health questions. Yet, findings from multiple studies conducted by Macapagal et al. (2017, 2019) suggested that answering sexual behavior questions is slightly more comfortable than answering substance use questions. Our finding that few students reported being very uncomfortable is similar to that of Kuyper et al. (2012), who found low levels of distress and high levels of positive feelings among adolescents and young adults when participating in sex research. None of the studies cited above involved a sample of college students – a population known for poor mental health, alcohol and drug misuse, risky sexual behaviors, and high rates of sexually transmitted infections. Despite college students receiving numerous invitations to participate in alcohol use research, they remain underrepresented in studies examining comfort levels with these presumably sensitive topics (Khatamian Far, 2018).
Limitations
Study findings should be interpreted with caution due to several limitations. This study was conducted at a single university in the Southern region of the U.S. with a small sample size (n = 123) and a relatively homogenous demographic profile, particularly overrepresenting cisgender heterosexual women, upperclassmen, and STEM majors. Additionally, the 25% response rate raises the possibility of self-selection bias, as factors such as older age or longer time on campus could influence comfort levels. However, respondents were randomly selected and their demographics largely aligned with those of the broader undergraduate student body, helping to contextualize the sample's representativeness. Another limitation is the use of single-item measures and dichotomizing variables to increase statistical power. However, separating alcohol use from drug use is a strength of this study, as previous studies often combined these items (Macapagal et al., 2017; Macapagal et al., 2019; Mustanski, 2011). While Mustanski (2011) did examine comfort levels using similar methodologies, that work focused solely on LGBTQ adolescents. Finally, the cross-sectional design allows for correlation interpretations than causal interpretations.
Best Practices
Many IRB members consider online survey protocols that asks participants (especially adolescents, college students, and young adults) about their sexual and behavioral health as sensitive or controversial, believing these topics may cause discomfort or distress among participants. Therefore, many IRB members may consider such research protocols to exceed the minimal risk standard as defined by the CFR (U.S. Department of Health and Human Services, 2021). Our data supports the argument that online survey research on sexual behaviors, substance use, and mental health could meet the CFR criteria for minimal risk, thus challenging the opinions and practices of most IRB members (Petrie et al., 2013). These findings add to the existing evidence that survey research on these health topics may indeed meet the minimal risk standard, according to the opinions of the general public (Fendrich et al., 2003; Jacomb et al., 1999), LGBTQ people (Fendrich et al., 2007; Kaniuka et al., 2022; Macapagal et al., 2017; Macapagal et al., 2019; Montemayor & Owens, 2025; Mustanski, 2011), and adolescents and young adults (Kuyper et al., 2012; Langhinrichsen-Rohling et al., 2006; Petrie et al., 2013).
Thus, some IRB members may be overcautious about such protocols, believing that participants, especially those from vulnerable groups, perceive such questions as distressing (Peter & Friedland, 2017). However, few participants in this study reported they were very uncomfortable answering online survey questions about their sexual and behavioral health, including participants from vulnerable groups (e.g., sexual minority students, racial/ethnic minority students, female students). These findings suggest that future research using surveys on sensitive health topics with similar populations could reasonably be evaluated as exempt rather than automatically defaulted to expedited review, provided that the study poses no more than minimal risk. While some IRBs may still opt for expedited review in certain cases, our results highlight that exempt review could be more appropriate given few participants from this study reported discomfort answering health topic questions. Incorporating these insights could help IRBs more accurately assess risk and avoid imposing procedural burdens on minimal-risk survey studies.
Although the risk of discomfort may be rare in online sexual and behavioral health surveys, some participants could still feel distress while answering such questions. We argue that researchers should continue to note discomfort as a potential risk in informed consent protocols for online sexual and behavioral health survey research, as not all participants in this study noted feeling very comfortable answering such questions. Investigators might consider utilizing more tailored and person-centered strategies to identify individuals who feel uncomfortable during the eligibility screening, data collection, and post-survey procedures (Labott et al., 2016). For example, participants could be asked their comfort and distress level after answering survey questions about their sexual, substance, and mental health behaviors. Individuals who report discomfort could be reminded of their right to skip questions, offered a less intrusive question that still addresses the study's aim, or be provided with additional resources (e.g., a referral list to resources and organizations, access to an on-call licensed counselor from the research team).
Research Agenda
Further investigation into the comfort levels of students who participate in online college sexual and behavioral health survey research is necessary, especially with larger and more diverse samples. Given that participant comfort in answering sensitive questions depends on the methodology employed (e.g., online survey v. interview, confidentiality v. anonymity) (Tourangeau & Smith, 1996; Tourangeau & Yan, 2007), it is important to understand how study design considerations influence college students’ comfort when answering health behavior questions. Comparison, vignette, and discrete choice experiment studies could be used to explore these differences. Additionally, exploring attitudes beyond comfort, such as perceived risks and benefits of participation, confidentiality and privacy protections, and investigator and university responsibilities, is essential to understanding participants’ intention and expectations to participate in these studies. Future research could also compare comfort levels between specific behaviors within a health domain (e.g., oral and vaginal sex, alcohol use v. cannabis use). Moreover, conducting longitudinal research would provide valuable insights into how college students’ comfort and attitudes toward college health research ethics evolve over time.
Educational Implications
It is critically important to train public health doctoral students and early-stage investigators how to conduct empirical ethics research to advance best ethic practices in college health research. However, research indicates that only a few accredited public health schools and programs require their graduate and doctoral students to enroll in research ethics or ethics courses (Agee & Gimbel, 2009; Lee et al., 2013; Simón-Lorda et al., 2015). According to Simón-Lorda et al. (2015), few public health ethics courses cover topics or offer mentoring in areas like HIV ethics (22%), alcohol and other drugs ethics (28%), evaluation of risk (11%), and research ethics (44%). Moreover, cognitive interviewing courses and methods often include debriefing respondents on their comprehension of the survey question rather than their discomfort, distress, and other attitudes towards the question itself (Balza et al., 2022; Willis, 2014). Public health programs, public health ethic courses, and survey design courses in public health programs could educate students on how to conduct empirical ethics research. With the curricula gap that does exist, national training programs could be necessary. The HIV/Drug Abuse Research Ethics Training Institute (RETI), a program that has been proven to be effective in equipping early-career investigators with these necessary skills, is currently the only program providing training for conducting empirical research on sexual health and drug abuse research ethics (Fisher & Yuko, 2015). Similar programs could consider adopting and customizing the RETI curriculum to empower trainees to engage in empirical research on college health research ethics, such as exploring college students’ perceived risks and benefits of participating in health research.
Supplemental Material
sj-docx-1-jre-10.1177_15562646251347580 - Supplemental material for Comfort of Sexual and Behavioral Health Survey Research Participation among Undergraduate Students: Findings from a Random Sample of a Southern University
Supplemental material, sj-docx-1-jre-10.1177_15562646251347580 for Comfort of Sexual and Behavioral Health Survey Research Participation among Undergraduate Students: Findings from a Random Sample of a Southern University by Benjamin N. Montemayor, Joy DeLeon and Christopher Owens in Journal of Empirical Research on Human Research Ethics
Footnotes
Consent to Participate
Respondents provided electronic written informed consent prior to participation.
Consent for Publication
Respondents provided electronic written informed consent to have their data published in aggregate.
Data Availability
The data are available from the corresponding author, CO, upon reasonable request and institutional review board approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was performed in alignment with the principles of the Declaration of Helsinki. The Texas A&M University institutional review board approved the study protocol on January 9, 2024 (STUDY2023-0057).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.