
Abstract
The feedback of individual results of genomics research is an ethical issue. However, which genetic results African participants would like to receive and why, remains unclear. A qualitative study was conducted to collect data from 44 adolescents and 49 parents/caregivers of adolescents enrolled in a genomic study in Botswana. Almost all the participants wanted to receive genetic results. Parents and caregivers wanted to receive results across all categories of genetic conditions discussed in the study, while adolescents were reluctant to receive results for severe, non-preventable, and unactionable conditions. Participants expressed different reasons for wanting feedback of results, including for awareness, improving lifestyle, accepting one’ situation, and preparing for the future. Our findings also reveal that participants’ context, relations, and empowerment are important to consider in interpreting their preferences for feedback of results.
Introduction
Whole Genome Sequencing (WGS) sometimes reveals information about individuals that are unrelated to the original research question but may be important for patient care (Bijlsma et al., 2018; Green et al., 2013; Recommendations from the presidential commission: The international research panel of the presidential commission for the study of bioethical issues released, 14 recommendations it says were needed to improve safety & reduce risk when conducting clinical trials nationally & internationally, 2013). For example, researchers may identify that a participant carries a mutation that predisposes them to a particular illness or that influences their drug metabolism (Hegde et al., 2015). These findings are usually categorized as “incidental” or “secondary” findings (Ortiz-Osorno et al., 2015). Secondary findings often refer to results that are not associated with the primary motive of testing but are, nevertheless, intentionally sought, while incidental findings involve variants that were discovered unintentionally (Darnell et al., 2016).
Generally, incidental and secondary findings from genomic sequencing are classified into the following three main groups: (a) clinically actionable results, (b) results with clinical validity for a disease but not usually expected to be clinically actionable, and (c) results with little or no clinical validity for disease and harm (Berg et al., 2011). Most studies conducted in high-income countries (HICs) revealed that participants generally would like to be provided with feedback of their individual results (Bollinger et al., 2012; Coors et al., 2015; Facio et al., 2013; Regier et al., 2015; Yu et al., 2013; Yushak et al., 2016). However, opinions from research participants vary from wanting to receive all findings to only certain subsets of genetic information. Some studies and reports in clinical trials indicated that research participants recommend the return of results, regardless of their negative implications (Fernandez et al., 2009; Miller et al., 2010; Murphy et al., 2008). Other participants mainly wanted to receive genetic results that they were able to act on or “do something about”. In this case, “actionability” is generally defined as the ability to treat or prevent the disease (Yu et al., 2013).
Many of the studies conducted on this topic originate in high-income countries and such work has hardly been extended to low- and middle-income countries (LMICs), particularly in Africa (Marsh et al., 2013a; Marsh et al., 2013b). According to Beskow and Burke (2010), the research context needs to be taken into consideration in discussions around the feedback of individual genetic results from genomics research as the findings cannot be generalized across different contexts. With the increase in genomics research in the continent brought about by initiatives such as the Human Heredity and Health in Africa (H3Africa), this issue has become more urgent than before. H3Africa has provided funding to 51 projects spread across 30 African countries to conduct population-based genomics studies of common non-communicable and communicable diseases. It was envisaged that samples from 50,000 to 75,000 participants would be analyzed through this initiative (Consortium et al., 2014), generating extensive individual (secondary and incidental) genetic results that could be beneficial to participants’ clinical and personal utility. As a result, this has brought about ethical challenges regarding the feedback of findings generated in African genomic sequencing. Whether participants in African genomic studies would like to receive genetic results, and if they do, which type of result and why, are still unclear. To address this gap in knowledge, we conducted an empirical study to explore the preference of adolescent participants, their parents and caregivers, regarding receiving feedback of genetic results of an HIV-TB genomics research project in Botswana. In this paper, we present participants’ views on receiving genetic results, their preference and reason for wanting certain results.
Methods
Study Setting and Population
We conducted an empirical qualitative study using data from individuals that participated in a genomics research study based in Botswana, an upper-middle-income country in Southern Africa with a gross domestic product per capita of US$7080.12 United States dollars (USD) (Botswana, 2018). For many years, HIV and TB have remained among the most serious diseases confronting children in Botswana, and there is a long track record of research on these conditions. The overall HIV prevalence in Botswana is 17.6%, with 20.3% in cities and towns, 16.6% in urban villages, and 16.9% in rural areas (Kandala et al., 2012). This is coupled with a high HIV/TB co-infection rate estimated at 60% (WHO, 2014). The rising prevalence of HIV among adolescents, from 3.7% in 2008 to 5.0% in 2013 (Botswana, 2013), is concerning. This situation prevails despite the country's extensive healthcare system including hospitals, clinics, health posts, and mobile stops spread across 27 health districts. Health care (inclusive of hospital care, laboratory tests, and medications) is provided free of charge in public sector facilities for all citizens, and almost 95% of Botswana's population lives within 8 kilometers of the nearest health facility (Botswana, 2015). However, genetic testing in Botswana is limited to the context of research.
As a result of the HIV/TB burden and other aforementioned characteristics, the Collaborative African Genomics Network (CAfGEN) was initiated to study genes in children with HIV and TB, for the development of new therapies to prevent or suppress these infections (BBCCCE, 2020b). The CAfGEN study is a collaborative project which is part of the H3Africa consortium (Consortium, 2014), and uses genomics approaches to identify host genetic factors that are important for the progression of HIV and HIV-TB infection in pediatric and adolescent African populations (Mboowa et al., 2018). The CAfGEN study was conducted at Botswana-Baylor Children's Clinical Center of Excellence (BBCCCE), which is a pediatric and adolescent clinic that provides free of charge state-of-the-art HIV care, treatment, and support to children, adolescents, and their families (BBCCCE, 2020a).
As a result, many of the adolescents participating in the CAfGEN study recruited into our study also received care from BBCCCE. The adolescent cohort in this study provided an opportunity to explore adolescents’ perspectives regarding questions around the feedback of results, as well as that of their parents and caregivers. The participants in our study included: (1) parents and caregivers of children aged 2–18 years and (2) adolescents aged 15–18 years enrolled in the CAfGEN study. Previous research has suggested that age may play a role in adolescents’ views on participating in genetic studies (Geller et al., 2003). According to Petersen and Leffert (1995) and Santelli et al. (1995), under most circumstances, adolescents aged at least 14 or 15 years are able to make conscious decisions similar to adult participants. As a result, recruiting adolescents of appropriate age was important to ensure that they could comprehend the complex issues related to feedback of results as well as provide sound opinions. However, in Botswana, minors below the age of 18 cannot consent to participate in research nor can receive results without the permission of their parents or caregivers. As a result, for this study, we obtained assent from both adolescents and their parents or caregivers.
Considering that the CAfGEN study included only adolescents who had been perinatally infected with HIV, all the adolescents in our study and probably most parents, were HIV positive. The number of HIV-positive non-parent caregivers is not known because their HIV status was not assessed in the study. The CAfGEN cohort was targeted for this study because they were likely generally knowledgeable about health and genetics than the general population. Consequently, they could participate better in meaningful discussions regarding feedback of genetic research results as they are part of a genetic study that has a strong community engagement aspect. Over the years, the BBCCCE has empowered the adolescent cohort as well as their parents and caregivers with information regarding the association between heredity and health. For example, four Genome Adventure Comic books were published by the institution (BBCCCE, 2020c) and translated into various languages as part of a community engagement project for the CAfGEN study.
Data Collection
We purposively selected 93 participants (44 adolescents enrolled in a genomic study in Botswana and 49 parents and caregivers of children and adolescents enrolled in the same study). While some adolescents were recruited with their parents or caregivers, they participated in separate meetings. No comparative responses from parent-adolescent dyads were conducted, as it was not the focus of the study. The study primarily used deliberative focus group discussions (dFGDs) (Rothwell et al., 2016) for data collection. These were augmented with in-depth interviews (IDIs) to explore a broad range of issues relating to the return of genetic research results, including participants’ views on receiving results, and their preference and reasons for certain results. A dFGD manual providing a step-by-step guide for data collection was developed for this study based on an extensive literature review (see Annex 1). The manual provided several scenarios and questions to elicit participants’ views regarding a range of ethical issues related to return of results. The scenarios explored several issues, including those relating to the return of results to adults and children, the return of adult-onset and early-onset conditions, roles and responsibilities for the identification and return of results. The interview topic guides were developed after identifying gaps in the dFGD data to further probe any issues that still needed clarification. The dFGD manual, in-depth interview guide, and consent forms were all translated into Setswana (the local language spoken in Botswana) by a research assistant who is a native speaker also fluent in English. The guides were also checked for consistency by the lead author, a native speaker of Setswana and fluent in English. The dFGD manual was pilot tested with 2 groups of parents and caregivers (16 participants in total) and 1 group of adolescents (5 participants), and the IDI tool was pilot tested with 3 parents or caregivers and 2 adolescents. The pilot testing aimed at the following: (i) assessing the feasibility of the dFGD and IDI methods, (ii) ensuring the fitness of the scenarios and topic guides with the study purpose, (iii) assessing participants’ comprehension concerning the issues discussed, and (iv) estimating the duration of the dFGDs and IDIs. The pilot dFGD suggested the introduction of a 30-min break in the first session of the dFGD that lasted approximately 3 h. In addition, some sentences and Setswana translations were revised both in the dFGD and the IDI tools with guidance from participants. Data from the pilot dFGDs and IDIs were excluded from the analysis.
The participants were recruited in person during their visit to the BBCCCE as well as telephonically, where necessary. The CAfGEN staff, particularly the study nurse and research assistant, was responsible for recruiting participants. The participants were informed about the study and interested parties were referred to the researchers. The purpose of the study was then explained to prospective participants, and consent was obtained by the primary author and the research assistant. Participants recruited by phone were taken through the consent process in person before participating in the dFGDs or IDIs. In each event, the participants decided whether to use Setswana or English. English and Setswana are both official languages in Botswana, and most official communication involves English. The members of the study team conducting these events were fluent in both languages, and all study materials were available in both languages. The parents and caregivers preferred Setswana for their discussions, the younger generation preferred English. Data were collected from February 2019 to March 2020.
The research team used deliberative focus group discussions because it combines a traditional FGD approach with extended opportunities for learning and discussion in an attempt to allow participants to engage with the study topic in an in-depth manner. The dFGD technique adopted for this study involved an interactive information-sharing session with the participants. Case studies elaborating on particular ethical considerations in the return of genetic results were used for information sharing during the first meeting. This allowed participants to learn about genes, their functions, and their impact on health. Data were collected until saturation was reached. Data saturation was discussed by DR, MK, and JDV. A total of 24 dFGD meetings were held with 12 groups of participants (6 groups of adolescents and 6 groups of parents and caregivers). These were complemented with 12 in-depth interviews (6 adolescents and 6 parents or caregivers) with people that had also participated in the dFGDs. The interviews were conducted on a one-on-one basis. The authors selected a range of participants from the dFGDs, from those that were quieter in the discussions to those that were more engaged. The IDIs focused on further clarifying and probing some of the early insights from the study.
Both groups of participants (adolescents, parents and caregivers) were asked the same questions about their views on wanting the feedback of genetic results. They were asked questions about their preference on the feedback of results for adult participants as well as those of children. A scenario of a mother found with a breast cancer gene while participating in a mental health study was used to solicit participants’ opinions on this topic (see Annex 1). This was followed up with a scenario where a daughter participating in an HIV-TB genomic study was found to be a carrier of a breast cancer gene. Participants were then asked about issues related to returning early-onset and adult-onset results. However, in this paper, we do not present the data pertinent to the feedback of pediatric genetic results but only the views of adolescents, parents and caregivers on wanting to receive feedback of results, and the preference and reasons for certain results.
To get participants’ preference on receiving feedback of results, we gave each participant a print-out of Table 1 with four categories that genetic results could fall into. This approach was guided by findings from Holm et al. (2015) who found that allowing research participants to make choices about which genetic conditions they would like to receive feedback of enhanced their satisfaction as compared to giving them no options for feedback or allowing them to choose either “yes” or “no” regarding receiving results.
Categories of Possible Individual Genetic Research Results.
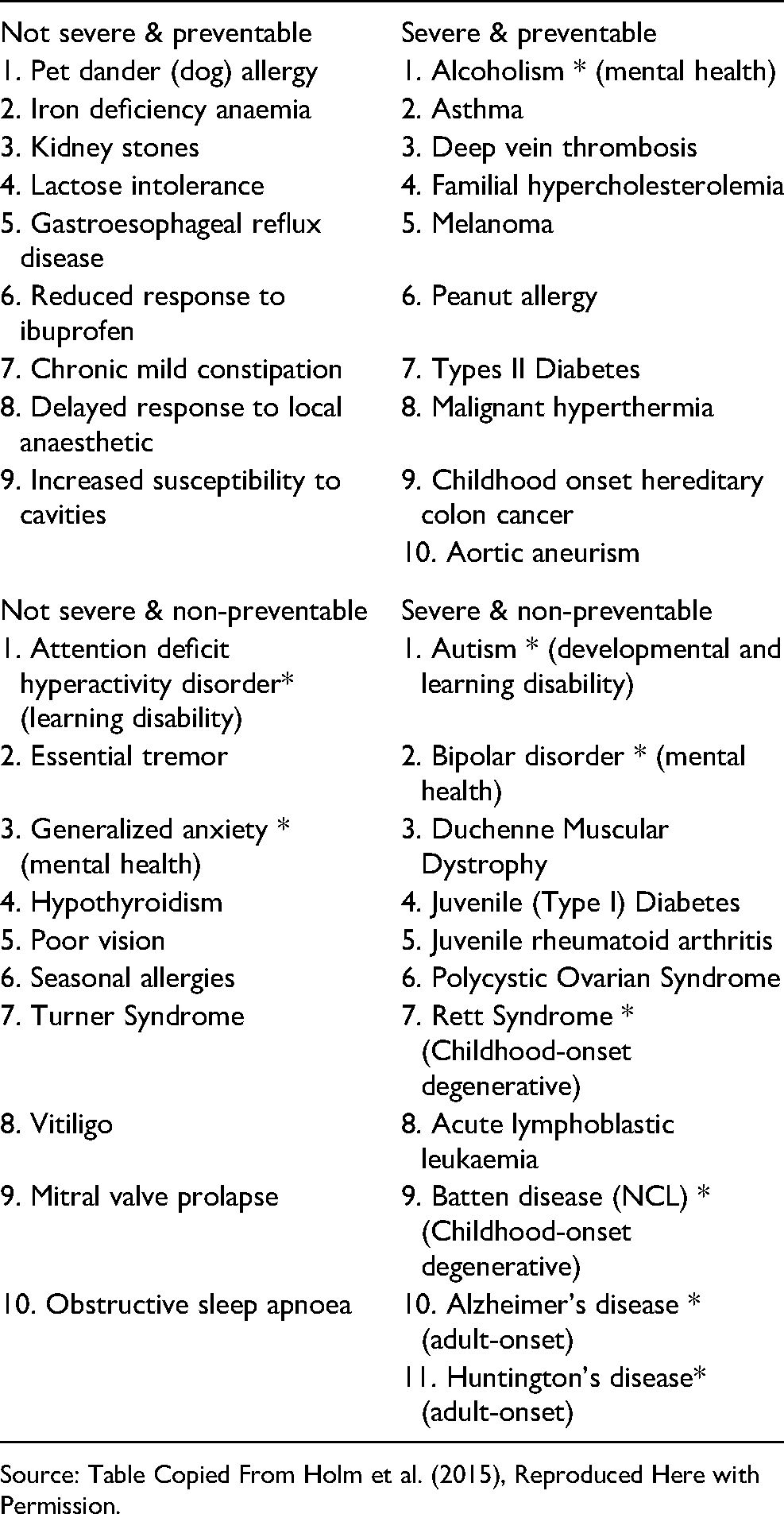
Source: Table Copied From Holm et al. (2015), Reproduced Here with Permission.
This table categorizes genetic conditions by severity, that is, how sick can the condition make a person and preventability, that is, the likelihood that the condition will develop in a person. We used the table to concretize the kinds of findings genomics research could reveal among the participants. We then moderated discussions around each category, exploring whether participants would want to receive such results and why.
Most participants in the study were females among both adolescents (61%) as well as parents and caregivers (92%). The 16–17 age group represented 61% of the adolescent participants while the most represented age group among parents and caregivers was 41–50 (39%). As most of the adolescents were in the 16–17 age group, the majority were either in junior secondary school or senior secondary school or had attained either of the qualifications (93%). Most (94%) of the parents and caregivers had educational qualifications ranging from primary to tertiary education. There was near uniformity in the residential location of participants in both categories—they were from villages around the city of Gaborone where this study was conducted (adolescents = 50%, parents and caregivers = 57%) or the city of Gaborone (adolescents = 39%, parents and caregivers = 43%). A few adolescents (11%) did not record their place of residence (for more details on the study procedures and methods, see Ralefala et al. (2020).
Data Analysis
All audio recordings of the dFGDs and IDIs were transcribed for data analysis. The content recorded in Setswana was translated to English. Each transcript comprised verbatim transcription of the audio recordings. Codes denoting the type of participant (“P” for parent and “A” for adolescent), speaker number, and group number were used to describe each participant in the transcript. For example, P1G1 denoted the first parent to speak in the first group of dFGD. The data were transcribed by the research assistant. Transcribed data from the dFGDs and IDIs were verified by the primary author (DR) by listening to the recordings while reading the transcripts. Any misquoted text and typographical errors were corrected. Upon completion of data cleaning and verification, transcripts were uploaded into the NVivo qualitative data analysis software Version 12 (QSR International Pty Ltd, 2012) to facilitate data organization and analysis. Both inductive and deductive approaches were applied to the coding. Data analysis for this study was guided by the stipulated study objectives and the framework method for data analysis (Gale et al., 2013).
However, the dFGD data relevant to this paper drew heavily from Holm et al. (2015). For instance, each participant in our study was given a print-out of the Table extracted from Holm et al. (2015) to demonstrate the four categories in which genetic results could fall into and it was found to be very compelling. Consequently, themes that emerged during discussions on which genetic results participants would want to receive aligned with those of Holm et al. (2015).
Ethical Review
This study was reviewed and approved for ethics compliance by the Health Research Ethics Committee of the Faculty of Health Sciences at the University of Cape Town, the University of Botswana Institutional Review Board, the Health Research and Development Committee of the Ministry of Health and Wellness in Botswana, and the Institutional Review Board of Botswana-Baylor Children's Clinical Centre of Excellence. Written assent was obtained from all adolescents, as well as written permission from their parents or caregivers before enrolling them in the study. Parents and caregivers also provided written informed consent for their participation in the study. Verbal permission for audiotaping was obtained from all participants. Separate written consent was obtained for participating in the dFGDs and IDIs in Setswana or English, according to the participant's preference. All participants were offered a snack and reimbursement for transport. Unique identifiers were used to protect participants’ identities during dFGDs and IDIs.
Results
Participants’ Preferences for Feedback of Individual Genetic Research Results
Overall, the majority of adolescents, and parents and caregivers expressed that they would like to receive genetic results, except a few adolescents and one parent preferring to not receive any genetic results. These findings are consistent with some studies and reports in clinical trials that document that research participants recommend the return of genetic results, often regardless of possible negative implications of the results (Fernandez et al., 2009; Miller et al., 2010; Murphy et al., 2008). After ascertaining whether or not participants wanted to receive results, the research team was interested in knowing which kinds of results the participants would prefer receiving. An investigation guided by Holm et al. (2015) was carried out to engage participants on which kinds of research findings they would like to receive. The four categories include the following genetic conditions: (a) not severe and preventable, (b) severe and not preventable, (c) severe and preventable, and (d) severe and not preventable. Parents and caregivers showed a desire to receive results across all four categories regardless of severity, preventability, or actionability. Interestingly, adolescents indicated preference to receive results encompassing three categories (a, b, and c) and reluctance to receive results for genetic conditions that are severe, not preventable, and unactionable.
Participants’ Reasons for wanting feedback of individual genetic research results
It is Important to Know
When probed about receiving unactionable results, a parent said, “For me, knowledge is power, irrespective of the consequences that come with it because you can exercise some proper management practices that will enhance the quality of your life …” (IDI P004). Parents and caregivers shared that knowledge about the genetic conditions that they are predisposed to and their cause could help to dispel the misconceptions of witchcraft. In Setswana culture and other cultures in Africa, it is common to associate certain ailments with witchcraft, especially where the cause of the disease is unknown. Parents and caregivers also expressed that knowing their genetic results could save them money and time as it would prevent them from searching for treatment of a genetic condition with no cure yet. These findings are in line with results from a study conducted in the United States of America by Sanderson et al. (2016) among healthy adults who had their genomes sequenced, wherein 94% of the participants wanted to receive all types of results. In a study by Christensen et al. (2017), two-thirds of participants wanted to receive all categories of genetic results about their children, including for non-preventable conditions. Participants gave several reasons for wanting to receive genetic research results, as outlined below.
Improve Lifestyle or look for Help
Adolescents expressed that even though some genetic results could reveal unexpected information, it could facilitate them to take better care of themselves and improve their health. Parents and caregivers also wanted to know their own results so that they could engage in healthy lifestyles that could help prevent the progression of genetically predisposed diseases, such as exercising, being aware of their environment to avoid any triggers, and taking up any other necessary preventative measures. This view was particularly strong for preventable conditions. Both adolescents and parents and caregivers also shared that once they knew their results, they could look for help to address the genetic condition, including going for counseling, looking for treatment, and exploring other ways of managing the condition. One parent expressed the following: “When (you are) told you have a certain gene, since it's a gene, it doesn't mean you have the illness. There is a 50/50 chance you might get it, so you would keep on going for regular tests to make sure that you treat the illness. You take care of yourself by always checking since you would have been informed on it…’ (IDI-P002).
Similar reasons have been reported elsewhere, in which participants expressed willingness to adopt healthier lifestyles, undertake preventive measures to reduce their future risk of getting sick, or look for treatment (Bijlsma et al., 2018; Facio et al., 2013; Sanderson et al., 2016).
Accept One's Situation
Adolescents also expressed that knowing their genetic results could help them accept their condition and prepare for the future. One adolescent said that “it's just like when you have HIV, you accept your situation and live on” (A5G4), while another shared that, “I would want to know so that I accept the possibilities of what could happen in the future, so that when it develops, I would already be in a good state of mind” (A5G2). Similarly, parents and caregivers also shared that knowing their genetic results could help them “stay mentally prepared to accept the situation if the gene develops into an illness”. According to a parent, “…You see accepting your situation is powerful, you have to consider yourself blessed to have known your status, the best medication even better than a pill is accepting oneself, then everything becomes better despite the results one receives…”(P8G4).
Prepare for the Future
One adolescent also said, “I want my results back because like I said, I want to be prepared for whatever might come my way, if it's breast cancer then I should be prepared for what will happen” (IDI-A006). Likewise, parents and caregivers also wanted to know their genetic results so that they could get their affairs in order in cases where the worst is expected to come. According to them, this will also help them to be alert about their health and prepare themselves for any situation that might arise. The importance of accepting one's situation and preparing for the future was mostly expressed with regard to receiving genetic results that are severe and non-preventable, as well as those that are unactionable. This finding resonates with views from participants in the study by Sanderson et al. (2016) where some participants wanted their personal genetic risk information, including for conditions that they could do nothing to prevent or treat so that they could prepare or plan for the future. Similar views were also shared in studies by Holm et al. (2015), Basson et al. (2007), Futter et al. (2009). In addition, one parent reasoned that treatment for an unactionable genetic condition today could be developed in the future and they could benefit from it. According to her, “Knowing your results is very important, even when there is no treatment, it can be developed at a later stage, like when HIV started in our country there wasn't any treatment. Then it was discovered at a later stage. So just because the doctors tell you that the genetic disease doesn't have any treatment doesn't mean you shouldn't receive the results” (P4G2).
Some participants in the study by Bollinger et al. (2012) and Sanderson et al. (2016) also shared a similar view, indicating that their genetic information could be useful to them in the future as research advances.
Participants’ Reasons for not Wanting Feedback of Individual Genetic Research Results
Although many participants expressed that they would like to receive their genetic results, some adolescents and a few parents and caregivers were uncomfortable with receiving results, especially those that were severe, non-preventable, and unactionable. Their main concern about receiving such results was the subsequent psychological implications. Some adolescents shared that it is not very useful to know about genetic conditions that are unactionable because, “…there is no help […], then it's the same as not knowing anyway’ (A1G2). A couple of other adolescents also expressed that they would not want to know their genetic results “if there is no treatment or cure” as it would be traumatizing and could make one lose hope in life. This view resonated with several parents and caregivers. One parent indicated the following: “…this will really disturb my mind because it will be too emotional. The human mind gets afraid when it receives certain news, I will get so confused even when you know it's just in the genes and there are possibilities I do not get the illness or has not developed, I guess its human nature” (P3G4).
Likewise, some participants in the Sanderson et al. (2016) study were also concerned about possible negative psychological implications of receiving genetic results, especially for conditions or diseases that are untreatable.
Few adolescents and one parent in our study also indicated that it is not necessary for them to know the results of genetic conditions that are not severe because if the condition develops, they will experience some changes or discomforts in their bodies that are not life-threatening, and they could always get help for them. A parent said, “I see it as not that important to know, you know it is not dangerous; they are just signs that you will just realize and take action to that so there is no need to be told” (P4G5).
Only one parent strongly opposed receiving feedback of extra genetic results in general. He said, “…they [researchers] should keep those results to themselves, I would not want to know them, I will find out some other time. I would not want to be stressed by something that might occur in 20 years that would disrupt my life in the present” (P1G1).
He also believed that “a lot of things are driven by faith, if you tell me and I believe I will get sick, then I will get sick (P1G1).” This parent was also concerned that knowing his genetic results could also place a burden on his children as genetic conditions are hereditary. However, stigma was not a concern for almost all participants. Only one adolescent expressed that some people may not want to know their results because they would not want to be “…stigmatized, ignored, or rejected by people since they would have seen that they have a certain gene. This may embarrass them, while some may just accept it since it concerns their health” (IDI-A001).
Context Matters for Interpretation of Preferences for Feedback of Individual Genetic Research Results
It seems that the choice of the kind of results people want is influenced by their experiences. For instance, parents and caregivers in our study wanted to receive all genetic results, while adolescents were reluctant to receive genetic results for conditions that are severe and not preventable, especially if they are unactionable. This may be because the parents and caregivers in our study survived a time where there was no treatment for HIV and have experienced a period where there is treatment and other ways to manage the disease. This experience seems to have influenced their views on receiving genetic results despite their severity, preventability, and actionability. One parent attributed their ability to “accept their situation” to their HIV experience and said, “…if we were able to accept our HIV status and counsel ourselves then what more can you fear…” (P9G3). This observation is similar to other observations (Kleiderman et al., 2014; Sapp et al., 2014) seen in the case of parents of children with rare genetic diseases. Parents in the study by Kleiderman et al. (2014) wanted to be notified about all results affecting their children's health, regardless of the severity of the disease. Likewise, Sapp et al. (2014) reported that parents also preferred to receive all types of results for their children and ascribed this to their success in coping with their child's condition for managing any other negative health information. The adolescents’ real time experience of learning about their HIV status and how it affects their health differs from those of the parents and caregivers as most adolescents were only recently learning to live with the knowledge of their HIV status. During dFGD meetings, we learned that most parents disclosed their children's HIV status to them during their adolescent years. This situation seems to have affected adolescents’ views on wanting feedback of unactionable genetic results, that, unlike their parents, are living in a period where HIV is manageable and may not easily imagine dealing with an unactionable result. The other reason could be that having a life-long condition could already be burdensome for these adolescents and may have made them fearful of knowing about the possibility of having another condition that they could do nothing about. When asked about wanting feedback on severe, non-preventable, and unactionable results, there was often a sobering silence during the adolescents’ dFGDs, indicating their apprehension in processing the information, with some of them eventually expressing that receiving such results would be emotionally traumatizing.
Participants’ Placed Value in Sharing Their Genetic Research Results with Family Members
Both adolescents, parents and caregivers expressed that as the results may also be relevant to other family members, it is imperative that they are also made aware of the genetic research results. According to a parent, “I believe that I want to get all the results back. I wouldn't want to be in the dark about my health or my family's health. I have to have information that could save our lives. If one of the family members has cancer, diabetes, or any illness in the family, it is important to know if the family has that gene and the possibility of anyone getting sick. So, it is important to have that information” (IDI-P003).
Participants described that their lives are not theirs alone and that there are people in their lives who should know about their health. Others indicated that it is important for them to know their results so that they could inform their caretakers, should they get sick, so that they know their situation upfront and be informed about the care that would be needed. Almost all participants preferred to receive results with limited direct benefit to themselves but potential clinical benefits to their family members. For example, in the case of a breast cancer predisposition in males that elevates their risk to disease only slightly but increases the risk for their children and female siblings considerably. According to a participant, “Yes, it is important that the results are returned even if the gene won't affect the participant. (As) They would still be helpful to others, and even (if) his children might not be at risk, his grandchildren could be at risk. So, the results are important to be returned to the participant” (PIDI-P001).
This highlights the interconnection of lives. Similarly, other studies have found that participants consider sharing their results with family members. For instance, a questionnaire administered to oncology patients revealed that most patients (75%) would share hereditary results revealing susceptibility to preventable conditions with family members and 62% would share information regarding unpreventable conditions (Yushak et al., 2016). In addition, participants in the study by Bijlsma et al. (2018) suggested that they would like to receive their genetic results so that they could share them with “their close family members, with some feeling responsibility towards their children” (p. 313).
Discussion
This study revealed that the research participants in Botswana generally wanted to receive genetic results, which largely resonates with empirical data from other studies (Bollinger et al., 2012; Coors et al., 2015; Facio et al., 2013; Regier et al., 2015; Yu et al., 2013; Yushak et al., 2016). In this study, we discovered three significant reasons for participants wanting feedback of genetic research results. First, the preference of the participants in receiving feedback of genetic results changes depending on their context, hence, must be inquired before reporting results. This is evident in our finding wherein most adult participants (parents and caregivers) that have lived with the knowledge of their HIV status for a long time and who experienced the transition from HIV being an ‘unactionable’ condition to a manageable one, wanted to receive their genetic research results regardless of severity, preventability, and actionability. Whereas adolescents that do not share this experience may have only recently come to terms with the knowledge of their HIV status are more reluctant to receive results relating to severe, non-preventable, and unactionable conditions. Long-term HIV patients may have developed resilience and may better handle challenges, including dealing with unactionable genetic research results.
Second, the participants valued the importance of sharing genetic information with family members. The participants seemed to view their lives to be interconnected with others, especially family members. This view is consistent with the African way of life, which is communal and where there is a strong emphasis on solidarity. The principle of solidarity encourages people and societies to account for the interests of others in their actions (Onuoha, 2007). In this context, individuals demonstrate solidarity with each other by assisting one another or acting in ways that profit others (Metz, 2017). With regard to medical care, solidarity requires that each individual's basic healthcare requirements be satisfied and each individual contribute towards a healthier society (Onuoha, 2007); this was reflected in our participants’ interest in sharing their genetic results with family members. Therefore, there may be an increased obligation for researchers to return results of genetic conditions, such as familial kidney disease or breast cancer genes in male participants, which often have implications in other family members.
Third, the participants in our study attributed a lot of power to knowledge. They wanted to know their genetic results for the sake of knowledge. These findings reflect the status and value of knowledge in Botswana culture as depicted in commonly used expressions like “education is a shield,” “education is an inheritance that cannot be taken from you” or “knowledge is power,” as expressed by some participants. According to Foucault (1977), the expression “knowledge is power” means that “power and knowledge directly imply one another…there is no power relation without the correlative constitution of a field of knowledge, nor any knowledge that does not presuppose and constitute at the same time power relations” (p. 27). Therefore, providing knowledge permits one to act; hence, power is present only in action (Gordon, 1980, p. 248). This raises questions regarding the meaning of returning meaningful knowledge. Drawing on this study, it is considered that knowledge about genetic predispositions is knowledge that emancipates and empowers. In this case, this could mean receiving feedback of genetic results that could explain the cause of a genetic condition that participants may be predisposed to, genetic results for conditions that participants may either prevent or treat, or those that could inform them to prepare for their future. This information could empower participants to make decisions about their lives or help those around them. Consequently, this suggests that the results from all the four aforementioned categories of genetic conditions should be considered for receiving feedback, except those with unknown significance or interpretation. Such results may neither have any importance to participants nor would they be of use to improve health. The desire by participants to receive all the four aforementioned categories of genetic conditions challenges the recommendation of several guidelines to report only genetic results that are clinically actionable (providing dependable information about medical conditions that can be clinically averted or treated) (Knoppers et al., 2015).
Although our findings are similar to those of other studies, they contribute to the literature on preference for wanting feedback of results of genomic research in Botswana and Africa. The emphasis on reciprocity and solidarity expectations for researchers to report genetic results is different from what has been reported previously (Ralefala et al., 2020). In addition, participants’ strong desire to receive genetic results could be influenced by Botswana's universal health care system and degree of reliance on the government to provide treatments, which is different from that in the US and other places but similar to Europe.
Conclusion
Participants in genomic studies often have varying preferences as well as reasons for receiving feedback of individual genetic results. Although participants in this study also presented various perspectives surrounding feedback of genetic results, most perspectives suggested that the participants wanted feedback of their genetic information but the kind of information preferred varied based on severity, preventability, and actionability of the results. As a result, there seems to be a stronger case to have actionable genetic results returned to participants, regardless of age, as this information was highly desired. Our findings also reveal that participant’ context, relations and empowerment are important aspects to consider in interpreting participants’ preferences for wanting feedback of genetic results. During the study, other issues related to the feasibility of feedback of results and cost for the study as well as issues related to the actionability of results were discussed. However, these findings have not been presented in this paper.
Strengths and Limitations
Our study has a few limitations that may limit the generalization of these findings to other contexts. First, the availability of free state-of-the-art care at BBCCCE may have encouraged participants to want to know their genetic results with the hope of receiving help from BBCCCE. Second, although the researchers took time during the dFGD process, it may not have been sufficient to educate people about the complexity of genetic results. This may be because the feedback of individual genetic results was presented as a hypothetical situation or because of participants’ knowledge of genetic research. As a result, these findings may not be generalizable to other contexts in Botswana or elsewhere in Africa. Considering that the participants had all been involved in a multi-year study that focused on heredity and health, their knowledge of genetics and heredity may be higher than that of the general public. Despite these limitations, this study contributes important findings to the literature on the feedback of genetic results in genomics research conducted in LMICs, particularly Botswana. One advantage of this study was the use of the dFGD method, a novel approach that allows participants to be educated and engaged in deliberation for a long period, which makes them more comfortable in sharing their views than do normal FGDs. This could be an effective way to engage participants in complex concepts such as genetics. The scenarios in the dFGDs could also have been a strength because they allowed participants to speak to an outsider without having to speak directly about their experience. Lastly, dFGDs and IDIs allowed researchers to delve into the research questions at a deeper level.
Best Practice
There is a need for Africa-specific guidelines for the feedback of individual genetic research results that takes into account the African genetic variation and context (Wonkam & de Vries, 2020). The findings from this study are an initial step toward achieving this goal.
Research Agenda
The mitigation of mistrust between participants and researchers warrants further research that consider the preferences of African participants on the kind of genetic results they want to receive. Further studies examining the views of healthy participants regarding wanting feedback of individual genetic results also need to be conducted. Quantitative studies with larger samples also need to be conducted to investigate participants’ preferences and priorities in the feedback of individual genetic results. This will allow for generalization and contribute to the scarce African literature on this topic.
Educational Implication
Findings from this study will be important to research professionals conducting genomic research in Africa. They will provide guidance on why and which individual genetic results must be reported to research participants. This is important in building trust between researchers and participants. Institutional review board members should also be aware of participants’ preferences and expectations for receiving feedback of individual genetic results to ensure their consideration in protocols developed for reporting the results of African genomics studies.
Supplemental Material
sj-pdf-1-jre-10.1177_15562646211043985 - Supplemental material for Participants’ Preferences and Reasons for Wanting Feedback of Individual Genetic Research Results From an HIV-TB Genomic Study: A Case Study From Botswana
Supplemental material, sj-pdf-1-jre-10.1177_15562646211043985 for Participants’ Preferences and Reasons for Wanting Feedback of Individual Genetic Research Results From an HIV-TB Genomic Study: A Case Study From Botswana by Dimpho Ralefala, Mary Kasule, Olivia P. Matshabane, Ambroise Wonkam, Mogomotsi Matshaba and Jantina de Vries in Journal of Empirical Research on Human Research Ethics
Footnotes
Author’s Note
All the authors contributed to the conceptualisation of this work. DR collected the data. DR and JdV developed the data analysis strategy and MK commented. DR prepared the first draft of the manuscript and all authors commented. Revisions were made by DR and all the other authors read and approved the final manuscript. JdV, MK and MM supervised the overall work.
Acknowledgments
The authors would like to thank the participants and staff at BBCCCE especially Keofentse Mathuba, Keboletse Mokete and Pinkie Gobuamang for assisting with participants recruitment, as well as Refilwe Monnakgosi and Ludo Bitsang who were both Research Assistants in this study. The authors additionally thank Dr Vicki Marsh and the broader IFGeneRA study team, particularly Elsie Breet and Marlyn Faure for developing the dFGD manuals and for discussions about project findings. We would also like to sincerely thank the anonymous reviewers for their constructive feedback which has improved the quality of this paper and Editage (![]() ) for English language editing.
) for English language editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Human Genome Research Institute (grant number U54HG009790).
Supplemental Material
Supplemental material for this article is available from the corresponding author on reasonable request.