
Abstract
There is increasing support for sharing individual-level data generated by medical and public health research. This scoping review of empirical research and conceptual literature examined stakeholders’ perspectives of ethical best practices in data sharing, particularly in low- and middle-income settings. Sixty-nine empirical and conceptual articles were reviewed, of which, only five were empirical studies and eight were conceptual articles focusing on low- and middle-income settings. We conclude that support for sharing individual-level data is contingent on the development and implementation of international and local policies and processes to support ethical best practices. Further conceptual and empirical research is needed to ensure data sharing policies and processes in low- and middle-income settings are appropriately informed by stakeholders’ perspectives.
Keywords
Policies mandating the sharing of individual-level data from biomedical and public health research are becoming widespread and commanding increasing support from large funding bodies, regulatory agencies, and the pharmaceutical industry (Medical Research Council, 2011; National Institutes of Health, 2003; Nisen & Rockhold, 2013; Research Information Network, 2008; Toronto International Data Release Workshop Authors 2009; UK Data Archive, 2011; Walport & Brest, 2011; Wellcome Trust, 2009). Discussions of data release in the literature highlight the importance of taking seriously both ethical arguments for sharing individual-level data from health research and the need to develop appropriate governance and protections (Antman, 2014; Eichler, Petavy, Pignatti, & Rasi., 2013; Greenhalgh, 2009; White, 2013; Zarin, 2013).
The increasing amount of clinical and public health research being conducted in low- and middle-income settings has the potential to generate datasets of significant value to researchers seeking to address disease burdens in such settings (Manju & Buckley, 2012). Consequently, there is a pressing need to determine how best to develop effective, ethical, and sustainable approaches to data sharing in such contexts. Experiences of data release for genomic research suggest that challenges raised by individual-level data sharing in low- and middle-income settings will be different in important and morally significant ways from those arising in high-income settings (Parker et al., 2009). In particular, although timely data sharing may be particularly important in low- and middle-income settings to inform effective and urgently needed public health interventions, it is important that data sharing is conducted in a way that does not disadvantage or harm researchers, research institutions, communities, and participants in such settings. Potential benefits and harms of data sharing are discussed in more detail below and summarized in Table 1.
Summary of Potential Benefits of and Concerns About Data Sharing.
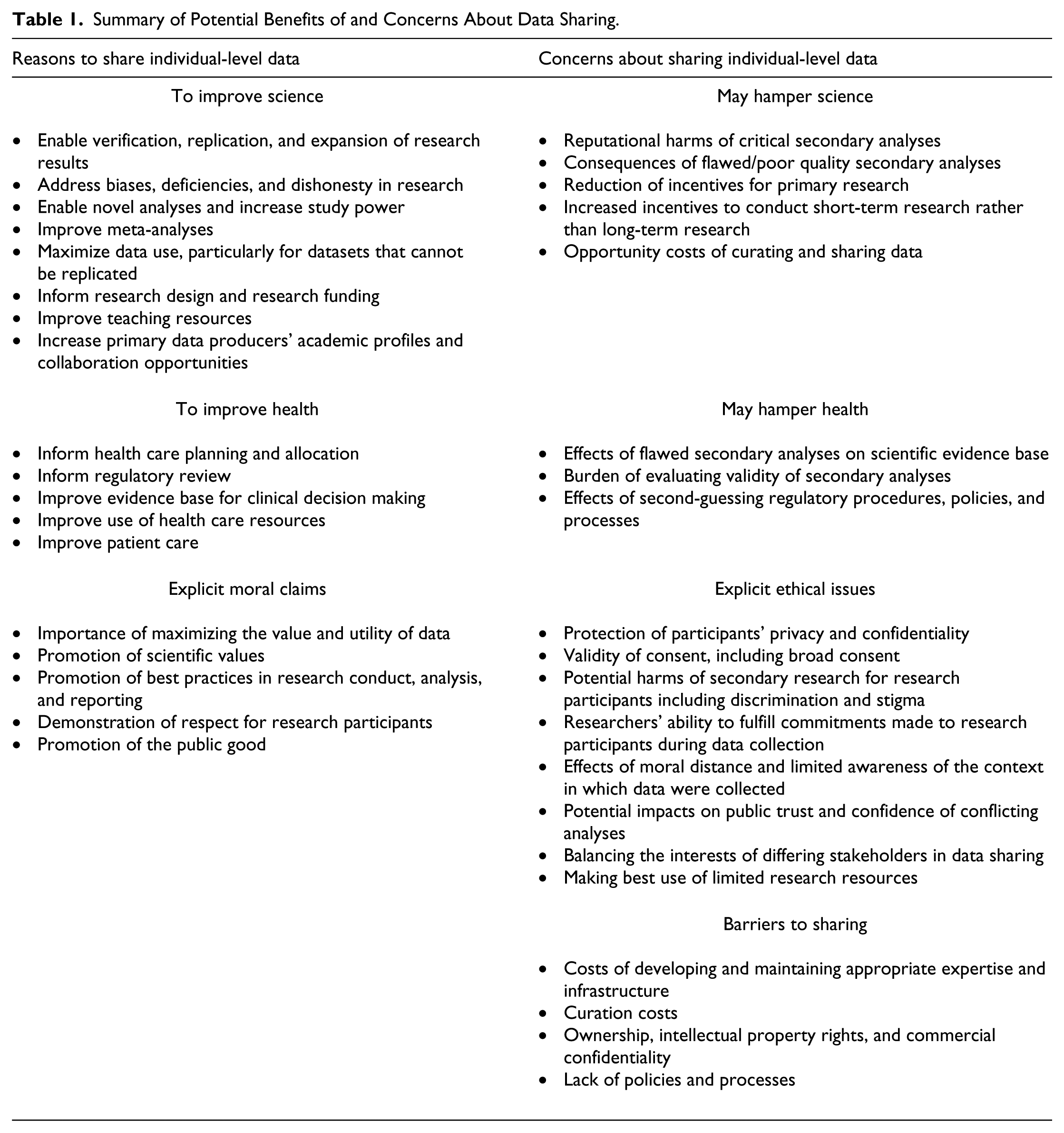
Potential Advantages of Data Sharing
Sharing individual-level data from clinical and public health research can be valuable in multiple ways. Sharing data allows for independent scrutiny of research results to ensure they are reliable and reproducible, and increases the accountability of researchers (Estabrooks & Romyn, 1995; Godlee & Groves, 2012; Kuntz, 2013; Manju & Buckley, 2012; Mello et al., 2013; Sieber, 2006). This may be particularly important where there are differing approaches to analyses (Smith, 1994) or where there are concerns that reports of research have been selective, biased, or dishonest (Doshi, Goodman, & Ioannidis, 2013; Gotzsche, 2011b; Rathi et al., 2012; Rodwin & Abramson, 2012; Ross, Gross, & Krumholz, 2012). Sharing data also enables identification of gaps in research and can inform both future research priorities and research design (Eichler et al., 2013; Gotzsche, 2011a; Sandercock, Niewada, Czlonkowska, & International Stroke Trial Collaborative Group, 2011; Strech & Littmann, 2012). Some datasets of particular value may not be able to be re-collected due to changes in available treatment and disease incidence, and may be useful as reference datasets, particularly in different contexts, such as low- and middle-income settings (Eichler et al., 2013; Sandercock et al., 2011).
Many commentators have discussed the value of conducting novel analyses with shared datasets, including testing innovative statistical methods and alternative analytical approaches (Coady & Wagner, 2013; de Wolf, Sieber, Steel, & Zarate, 2005; Hrynaszkiewicz & Altman, 2009; Pisani & AbouZahr, 2010; Toronto International Data Release Workshop Authors, 2009; Vickers, 2006; Whitworth, 2010). Meta-analyses combining individual-level datasets may provide more reliable results than those based on summary data (Chan et al., 2014; Pisani & AbouZahr, 2010). Meta-analyses may also provide different results from the primary studies and permit examination of topics such as the heterogeneity of treatment effects, subgroup effects, temporal and geographical effects, and identification of rare safety events (Anderson & Merry, 2009; Chan et al., 2014; Dawson & Verweij, 2011; Manju & Buckley, 2012; Mello et al., 2013).
Additional arguments in favor of sharing data are that it can be an efficient and cost-effective means of maximizing the utility of a dataset for research purposes and for teaching and methodology development (Gotzsche, 2011b; Manju & Buckley, 2012; Smith et al., 2014; Walport & Brest, 2011). Increasing use of collected data can also reduce unnecessary duplication of research, which in turn limits potential harms to and burdens on research participants (Eichler et al., 2013; Rani, Bekedam, & Buckley, 2011; Strech & Littmann, 2012).
These claims suggest that data sharing can make a very important contribution to public health, by improving the evidence base used to make regulatory, funding, and clinical decisions, and to make the best use of available resources (Hrynaszkiewicz & Altman, 2009; Hughes, Wells, McSorley, & Freeman, 2014; Rathi et al., 2012; Rodwin & Abramson, 2012; Ross, Lehman, & Gross, 2012). As a routine best practice in research, it may contribute to improving public faith in research and drug regulation, particularly by promoting accountability and transparency in processes where there are potential conflicts of interest (Haines & Gabor Miklos, 2011; Hampton, 2011; Rani et al., 2011; Zarin, 2013).
In addition to the potential of advancing scientific development and health, commentators have discussed ethical imperatives for promoting data sharing. Principles of fairness and reciprocity require data be shared to benefit communities that fund research indirectly and that provide the data on which research relies (Langat et al., 2011; Pisani & AbouZahr, 2010; Strech & Littmann, 2012; Tangcharoensathien, Boonperm, & Jongudomsuk, 2010; Walport & Brest, 2011). In addition, respect for research participants requires that their contributions to research be maximized by making the best use of their data. In particular, expectations that the results of research will be disseminated to advance science must be honored (Gotzsche, 2011b; Mello et al., 2013; Pisani & AbouZahr, 2010; Walport & Brest, 2011).
Potential Disadvantages of Data Sharing
Numerous concerns and issues about sharing individual-level health research data have been discussed in the literature in addition to potential benefits. A core concern is to ensure that the privacy of participants is protected during secondary uses of data (Castellani, 2013; de Wolf, Sieber, Steel, & Zarate, 2006a; Eichler et al., 2013; Nisen & Rockhold, 2013; Savage & Vickers, 2009; Walport & Brest, 2011; Zarin, 2013). Processes for de-identifying data must be not only robust but also proportionate if the utility of the data is to be preserved (Antman, 2014; de Wolf, Sieber, Steel, & Zarate, 2006b; Eichler et al., 2013). Concerns have been raised about the ability of primary researchers to guarantee that re-identification will not take place (Mello et al., 2013), particularly when reverse engineering and/or the combination of datasets may increase chances of identifying specific participants (Estabrooks & Romyn, 1995; Geller, Sorlie, Coady, Fleg, & Friedman, 2004; Nisen & Rockhold, 2013; Rabesandratana, 2013; Wieseler, McGauran, Kerekes, & Kaiser, 2012).
Although curating and sharing data may make the most efficient and effective use of datasets, preparing data for research and implementing appropriate policies and processes require significant effort, expertise, and resources (Anderson & Merry, 2009; Mello et al., 2013; Rathi et al., 2012; C. T. Smith et al., 2014; Walport & Brest, 2011). Lack of resources needed to share data has been identified as an impediment to data release in empirical research in higher income settings (Mello et al., 2013; Rathi et al., 2012; Reidpath & Allotey, 2001; Savage & Vickers, 2009; C. T. Smith et al., 2014) and as a serious obstacle in low- and middle-income settings (Manju & Buckley, 2012; Pisani & AbouZahr, 2010; Rani et al., 2011; Whitworth, 2010).
Concerns have been raised that if sufficient safeguards are not in place, inappropriately prepared or shared data may hamper, rather than promote, public health (Nisen & Rockhold, 2013; Pearce & Smith, 2011; Piwowar, Becich, Bilofsky, Crowley, & on behalf of the caBIG Data Sharing and Intellectual Capital Workspace, 2008; Spertus, 2012). Data may be misinterpreted, or the subject of biased, inappropriate, or poorly designed studies (Greenhalgh, 2009; Kirwan, 1997; Pisani, Whitworth, Zaba, & Abou-Zahr, 2010a; Rathi et al., 2012; Spertus, 2012; Wieseler et al., 2012). The results of such studies may mislead health care providers and regulators, lead to false hopes or unfounded concerns about treatments, reduce public confidence in research, and result in litigation (Anderson & Merry, 2009; Castellani, 2013; Kuntz, 2013; Mello et al., 2013; Nisen & Rockhold, 2013; Ross & Krumholz, 2013). In addition, incentives for novel biomedical research may be reduced, if secondary data users can “free-ride” on the efforts of those collecting the data (Castellani, 2013; Langat et al., 2011; Rabesandratana, 2013; Rathi et al., 2012; Ross & Krumholz, 2013; Zarin, 2013).
Stakeholders’ Interests in Data Sharing
Sharing individual-level research data will affect the interests of stakeholders in different ways. Primary researchers have interests in conducting initial analyses of data they have collected, and in receiving appropriate acknowledgment for dataset production (Castellani, 2013; Lopez, 2010; Pisani & AbouZahr, 2010; Tangcharoensathien et al., 2010; Whitworth, 2010). Research participants and the communities from which they are drawn have interests in understanding that data may be shared, the consequences of sharing, and ways in which potential harms of sharing can be minimized (Mello et al., 2013; Pearce & Smith, 2011; Piwowar et al., 2008). Research funders have interests in promoting the utility of datasets and may also have interests in commercial exploitation of research results (Anderson & Merry, 2009; Castellani, 2013; Eichler et al., 2013; Kmietowicz, 2013; Mello et al., 2013).
Data sharing policies and process must recognize and respond to the differing interests of stakeholders appropriately if they are to effectively promote the benefits of data sharing and minimize potential harms. Calls have been made for policies and processes for data sharing to be informed by, and developed in consultation with, relevant stakeholders (Manju & Buckley, 2012; Vallance & Chalmers, 2013; Whitworth, 2010). This scoping review sought to map evidence about stakeholders’ experiences of data sharing and their perspectives of best practices, particularly in low- and middle-income settings, with the aim of informing future policy development and research agendas (Parker & Bull, 2015).
Method
Scoping reviews seek to identify literature relevant to the research objective and may include a variety of research formats and conceptual literature (Arksey & O’Malley, 2005; Armstrong, Hall, Doyle, & Waters, 2011). This study sought to review published literature on stakeholders’ experiences of sharing individual-level data from medical and public health research and views of ethical best practices reported in peer-reviewed journals. Inclusion criteria for the study encompassed a broad range of article types, including empirical studies, news articles, opinion pieces, features, editorials, reports of practice, and theoretical articles. The initial search strategies for capturing views in this range of article formats were developed through an iterative process and used a combination of text words and subject headings (see Online Supplementary Materials 1 at http://jre.sagepub.com/supplemental).
The following databases were searched for relevant studies: Embase (OvidSP)[1974-present], Global Health (OvidSP)[1973-present], Global Health Library–Regional Databases (Virtual Health Library) [http://www.globalhealthlibrary.net], MEDLINE(R) In-Process & Other Non-Indexed Citations and MEDLINE(R) (OvidSP) [1946-present], ABI Inform (Proquest) [1971-current], PAIS International (Proquest)[1977-current], Science Citation Index (Web of Science Core Collections, Thomson Reuters) [1945-present] and WHOLIS (Virtual Health Library) [http://www.globalhealthlibrary.net]. The original search was conducted on June 24, 2013, and searches were repeated on December 9, 2013, and June 27, 2014, to update findings. No language or publication date limits were applied. Research relevant to low- and middle-income countries was isolated and grouped using a geographic search filter; however, all references were screened. (The full search strategy for Medline is available in Online Supplementary Materials 2).
The total of 6,430 abstracts identified by the strategy were screened, 958 of which were flagged as being particularly relevant in low- and middle-income settings. A matrix of inclusion and exclusion criteria was developed to inform screening (see Figure 1).
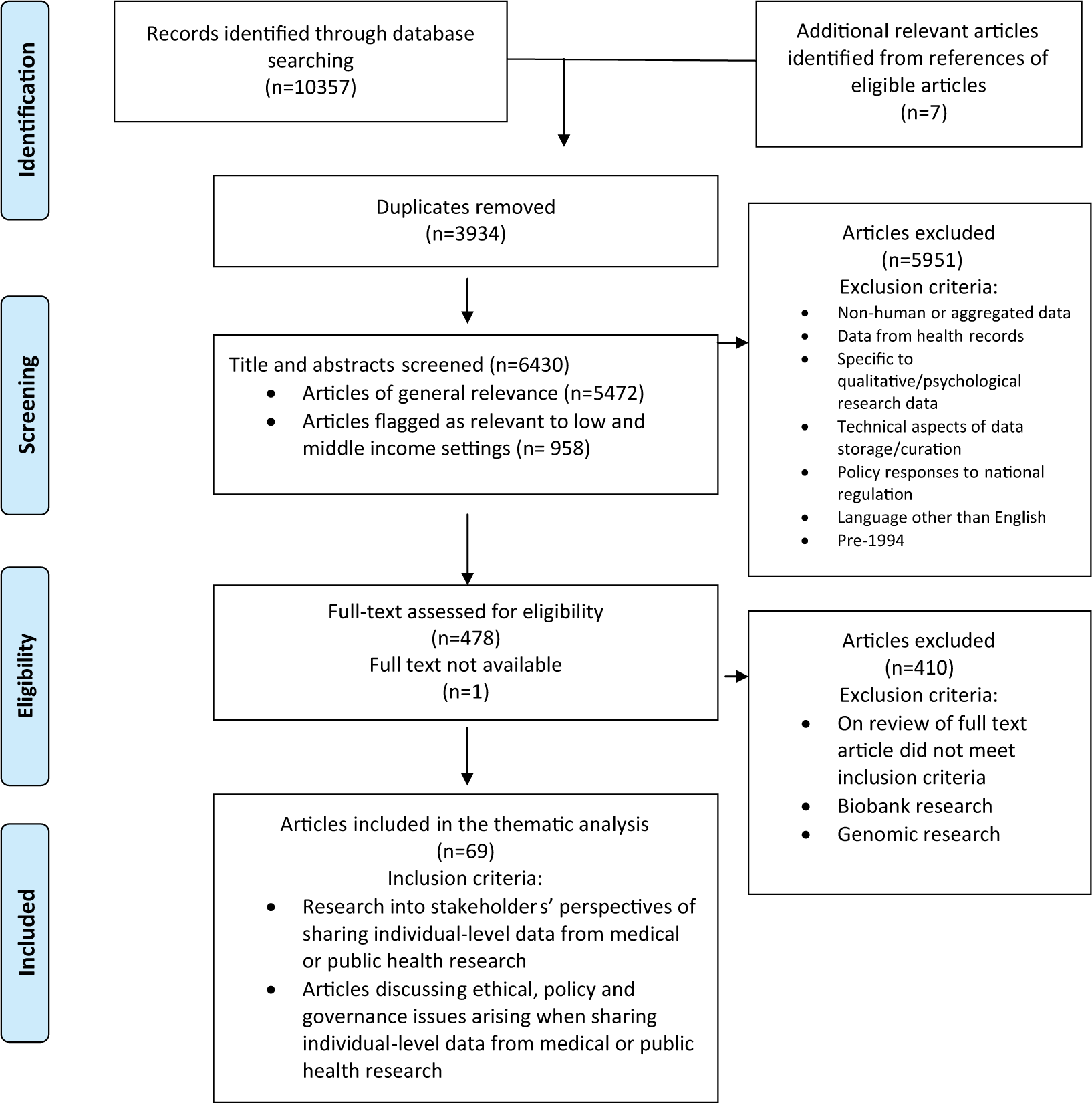
PRISMA 2009 flow diagram of the scoping review.
All abstracts were reviewed by a single researcher, with sample of 20% of abstracts being co-reviewed by additional researchers using a trial outline of inclusion and exclusion criteria. After co-reviewing 20% of abstracts, the value of a dual review was assessed. Given the complexity of consistently determining from abstracts which articles contained discussions of relevant ethical, policy, and governance issues, and the large number of abstracts to be screened, multiple review of all the abstracts was considered inefficient. Instead, a single reviewer applied revised inclusion and exclusion criteria consistently, marking articles that were potentially relevant (228), and additional articles that required full text review to determine relevance (246). References from these two categories were imported into bibliographic software (Endnote X6), which was then used to track decisions during a detailed review (King, Hooper, & Wood, 2011).
In scoping reviews, to ensure appropriate identification of the literature, it may be important to adopt an iterative approach to study selection (Arksey & O’Malley, 2005; Armstrong et al., 2011). Following screening of full text articles, five empirical studies of stakeholders’ perspectives of sharing individual-level data from clinical and public health research were identified, all of which reported views and practices of researchers and research institutions from high-income settings. During full-text screening, articles focusing on samples and individual-level data from biobanks and genomic research were not routinely excluded, particularly when they reported on perspectives from data subjects or from stakeholders in low- and middle-income settings. A subsequent review of ethical, policy, and governance issues raised in such papers demonstrated some important differences with issues raised by sharing data from clinical and public health research, and they were subsequently excluded from the review.
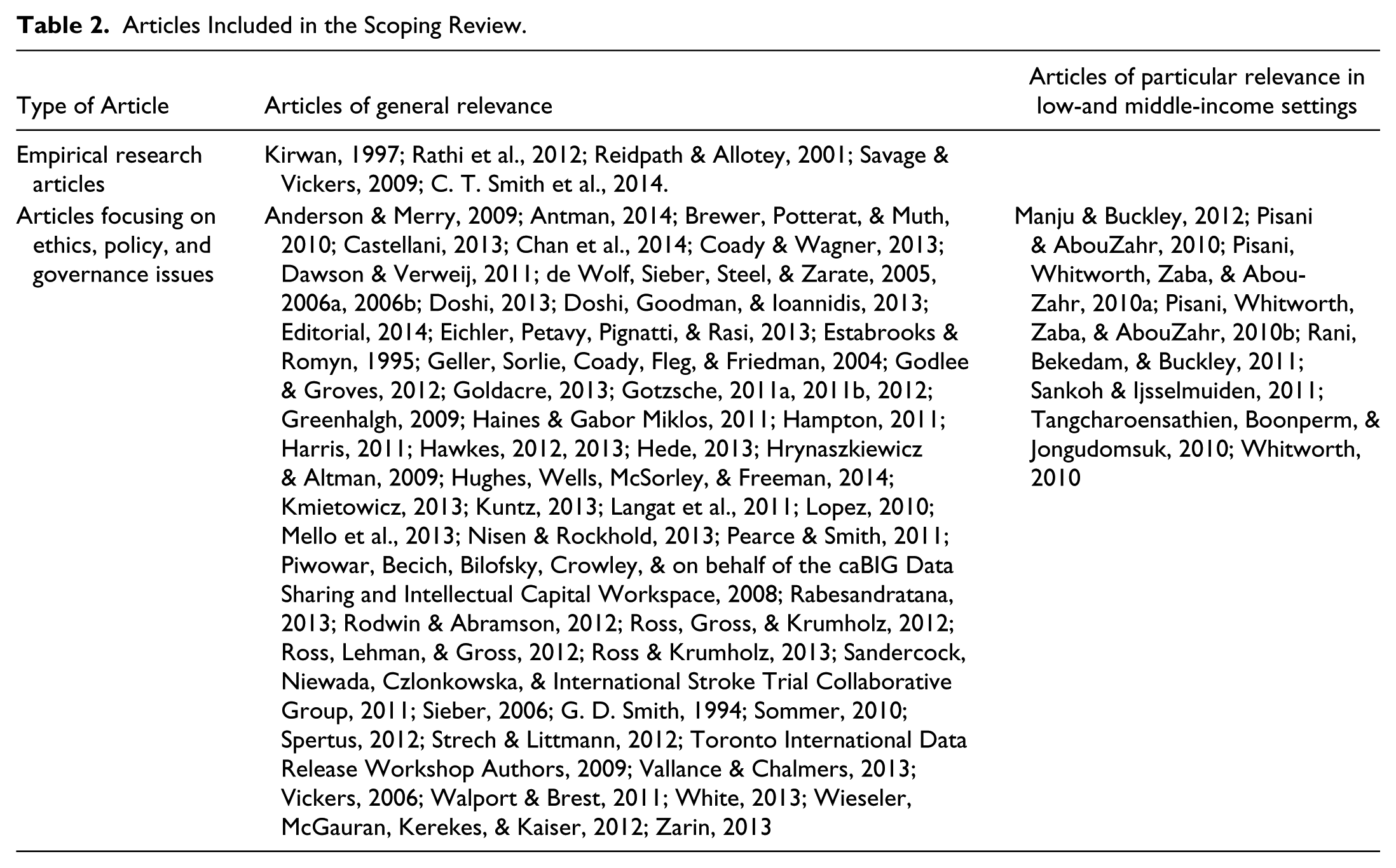
The full text of the final 69 shortlisted papers was imported into qualitative data analysis software (NVIVO 10; see Table 2). Descriptive codes were developed to chart perceived advantages of data sharing, barriers and concerns about data sharing, and recommendations for best practices in governing data sharing.
Articles Included in the Scoping Review.
Results
This section begins by reviewing empirical research into stakeholders’ experiences of, and views about, best practices in sharing individual-level data from medical or public health research. It then outlines the views expressed in articles focusing on ethical, policy, and governance issues arising when sharing such data. It concludes by focusing on issues identified as particularly relevant to best practices when sharing data from low- and middle-income settings.
Empirical Research
There is very limited empirical research into stakeholders’ experiences of sharing individual-level data from clinical or public health research, and their views about best practices when doing so. This review identified five empirical studies, all of which sampled researchers and reviewers from high-income settings. Details of the studies, including the primary findings reported in the original articles, are set out in Table 3.
Empirical Research Into Stakeholders’ Experiences and Perspectives.

Best Practices in Data Sharing
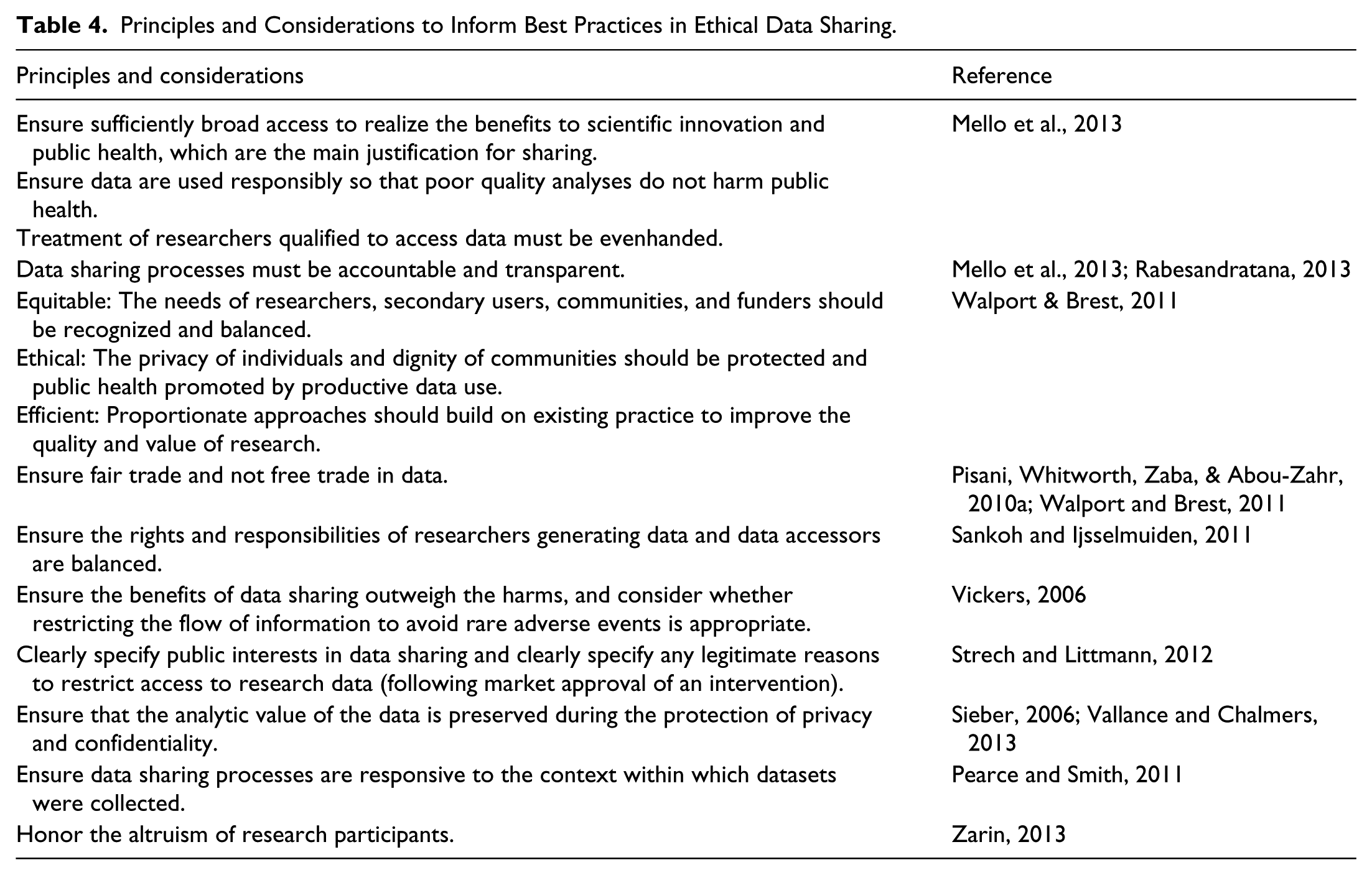
In the introduction to this article, stakeholders’ views about potential benefits and harms of sharing individual-level data were outlined. When considering the implications of such potential benefits and harms for best practices in data sharing, the fundamental importance of protecting the privacy of research participants was universally acknowledged in the reviewed literature. Some authors went further and set out additional specific principles and considerations for best practices in ethical data sharing (see Table 4).
Principles and Considerations to Inform Best Practices in Ethical Data Sharing.
Governed Data Sharing
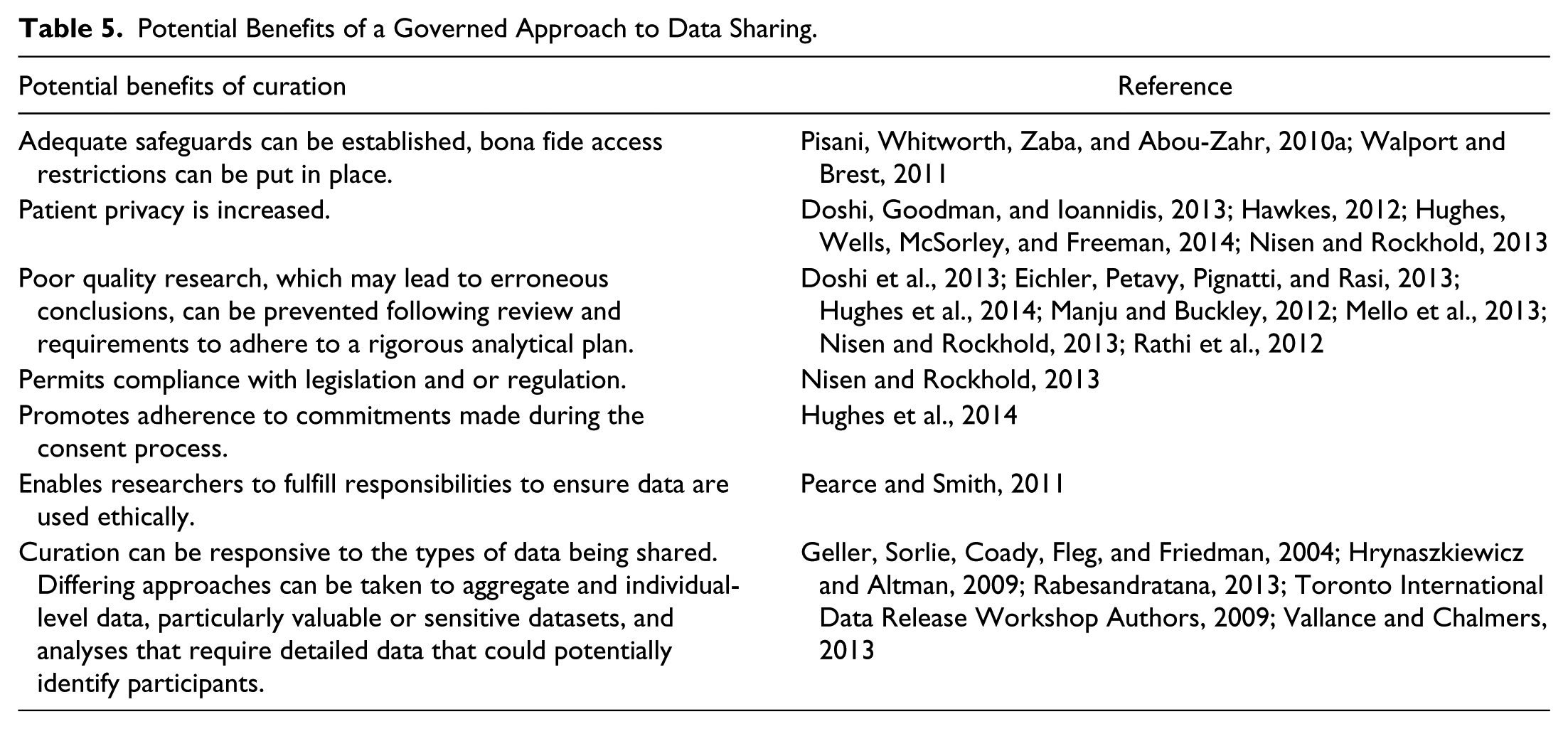
To maximize the potential benefits of sharing de-identified data, some stakeholders recommended that de-identified datasets should typically be made available publicly, with minimal restrictions (Doshi et al., 2013; Eichler et al., 2013; Gotzsche, 2011a, 2011b; Haines & Gabor Miklos, 2011; Harris, 2011; Ross, Gross, & Krumholz, 2012; Strech & Littmann, 2012; Vallance & Chalmers, 2013). In contrast, in the majority of reviewed papers, a governed approach to data release was considered valuable to minimize potential harms and maximize potential benefits. Some authors discussed specific advantages of adopting a governed approach to data sharing, as outlined in Table 5.
Potential Benefits of a Governed Approach to Data Sharing.
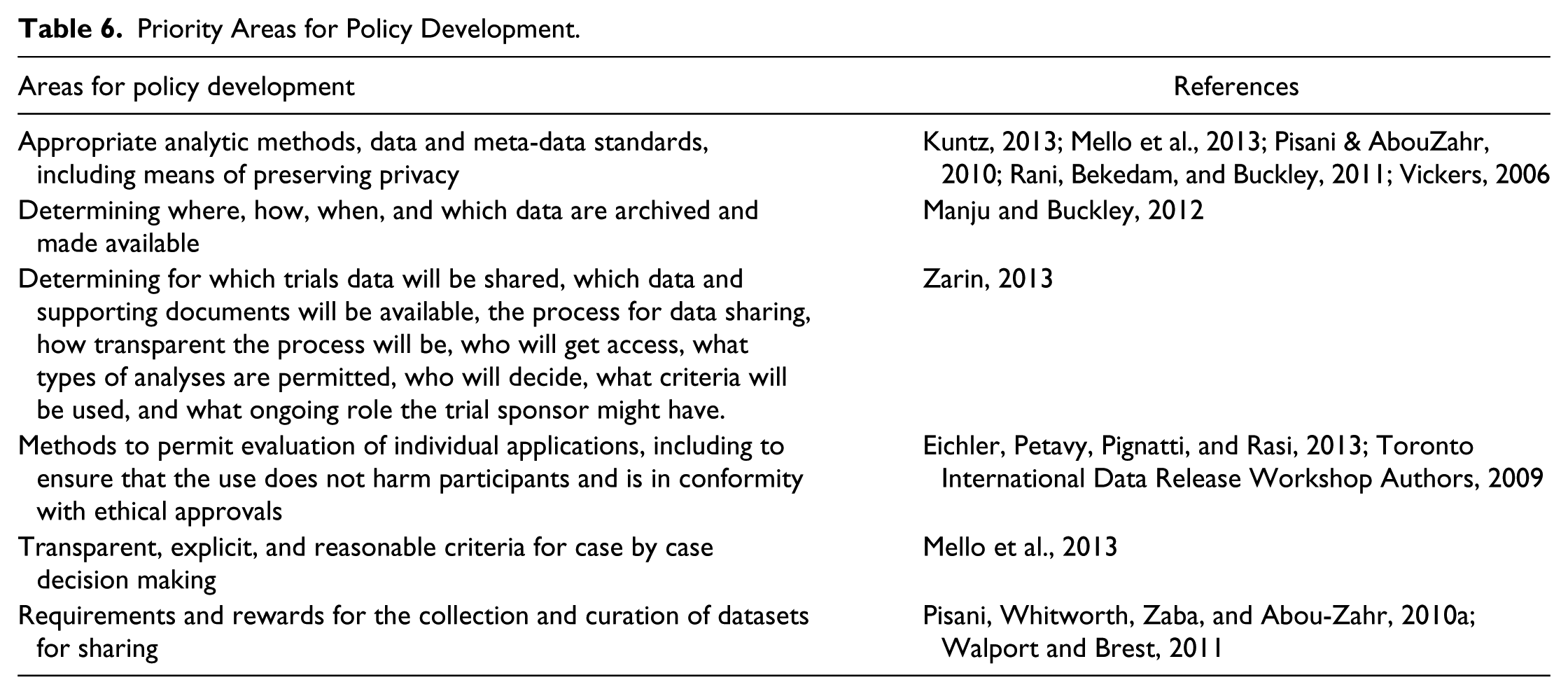
To guide governed data sharing, stakeholders made a number of recommendations about appropriate policy development. The current lack of policies or inconsistent policies in some settings was considered both frustrating and inefficient, as well as providing loopholes for researchers who did not want to share data (Manju & Buckley, 2012). A number of papers recommended that harmonized policies with broad applicability be developed, following consultation with a broad range of stakeholders, including policy makers, researchers, patients, patient advocates, privacy experts, funders, research institutions, journal editors, ethicists, NGOs, and governments (Estabrooks & Romyn, 1995; Hrynaszkiewicz & Altman, 2009; Manju & Buckley, 2012; Mello et al., 2013; Vallance & Chalmers, 2013; Whitworth, 2010). These could be complemented by institutional policies where appropriate (Manju & Buckley, 2012; Piwowar et al., 2008). Areas to be addressed in the policies are outlined in Table 6. Some commentators questioned the effectiveness of guidelines and policies encouraging data sharing to date (Gotzsche, 2012; Mello et al., 2013; Savage & Vickers, 2009; Vickers, 2006) and suggested legal requirements for data sharing be implemented (Gotzsche, 2012; Vickers, 2006).
Priority Areas for Policy Development.
Best Practices in Sharing Data From Low- and Middle-Income Settings
In both the discussion of potential advantages and disadvantages of data sharing in the introductory section of this article, and the discussion of perspectives about best practices above, the views of authors discussing data sharing in low- and middle-income settings were similar to those expressed in the more substantial body of literature from higher income settings. In contrast to lower and middle-income settings, articles from higher income settings had more discussion about ways in which these issues had been addressed and data shared to date. When discussing how to provide resources for best practices in data sharing, and how to balance the interests of stakeholders in the data sharing process (particularly those generating datasets), views remained similar, but some different emphases also emerged.
The importance of balancing the interests of primary researchers and secondary data users has received considerable attention in the reviewed literature. Stakeholders from higher and lower income settings commented on the importance of ensuing that researchers received appropriate recognition for producing datasets in the subsequent publications by secondary analysts, in professional assessments, and in funding applications (Kuntz, 2013; Manju & Buckley, 2012; Pisani & AbouZahr, 2010; Pisani et al., 2010a; Piwowar et al., 2008; Rani et al., 2011; Rathi et al., 2012; Ross & Krumholz, 2013; G. D. Smith, 1994; C. T. Smith et al., 2014; Walport & Brest, 2011; Whitworth, 2010). Perspectives on authorship differed. Some commentators suggested that co-authorship or at least the chance to publish an associated response or commentary should be offered to the researchers who produced the dataset (Pearce & Smith, 2011; Savage & Vickers, 2009; Vickers, 2006). Others noted that the contribution of data creators may not be sufficient to warrant co-authorship of the secondary analysis (Anderson & Merry, 2009; Gotzsche, 2011b).
Although some commentators considered the value of releasing data prior to publication (Toronto International Data Release Workshop Authors, 2009), others noted the value of exclusive fair use periods for researchers in higher and lower income settings (Geller et al., 2004; Gotzsche, 2011b; Manju & Buckley, 2012; Pearce & Smith, 2011; Pisani & AbouZahr, 2010; Pisani et al., 2010a; Rathi et al., 2012; Ross, Lehman, & Gross, 2012; Savage & Vickers, 2009; Tangcharoensathien et al., 2010; Vickers, 2006). Such periods ranged from 12 months from the end of data collection to unspecified lengths of time, which were, in some cases, linked to the publication of an article with primary findings.
Although limited resources may be a hindrance to data sharing in higher income settings, they were identified as a very significant barrier in lower income settings (Manju & Buckley, 2012; Pisani & AbouZahr, 2010; Pisani et al., 2010a; Pisani, Whitworth, Zaba, & AbouZahr, 2010b; Rani et al., 2011; Sankoh & Ijsselmuiden, 2011; Tangcharoensathien et al., 2010; Walport & Brest, 2011; Whitworth, 2010). For high-quality individual-level data to be shared in databases with long-term sustainability, significant investment in human resources, technology, and infrastructure will be required. Training, mentoring, and career pathways need to be provided for a range of specialist support staff who will document and curate datasets and manage data release processes. Where data archives are hosted within low- and middle-income settings, expertise in managing biomedical information will be required in addition to the development of storage infrastructure.
Commentators have noted that it would be unfair to develop capacity to share data in low- and middle-income settings without also developing the capacity for data generators and secondary users from such settings to analyze that data (Pisani et al., 2010a; Sankoh & Ijsselmuiden, 2011; Walport & Brest, 2011; Whitworth, 2010). Collaboration between primary and secondary data users was discussed as a potential means of improving the quality of analyses in both higher and lower income settings (Geller et al., 2004; Kuntz, 2013; Pearce & Smith, 2011; Spertus, 2012). Stakeholders from lower income settings also focused on the value of such collaborations to build capacity among researchers generating datasets (Manju & Buckley, 2012; Pisani et al., 2010a; Tangcharoensathien et al., 2010; Whitworth, 2010).
Discussion
The reviewed literature demonstrated considerable support for sharing individual-level data from clinical and public health research. As discussed above, numerous recommendations have been made for best practices in governing such sharing, to ensure that potential benefits are promoted and potential harms are managed appropriately. Although significant consensus about some aspects of best practice is evident, such as the need to protect the privacy of research participants, there are differences of opinion about practical achievement of these, such as the measures needed to protect privacy and the extent to which privacy can be assured (Gotzsche, 2011b; Mello et al., 2013; Nisen & Rockhold, 2013). In other areas, there is less consensus about best practices. Opinions differ, for example, about the need for and length of protected time primary researchers should have with data before they are shared (Geller et al., 2004; Toronto International Data Release Workshop Authors., 2009), and the nature of consent required, if any, for sharing de-identified data (de Wolf et al., 2005; Pearce & Smith, 2011).
Commentators have suggested that gaps and inconsistencies in policies and practices for data sharing are frustrating and inefficient, and have recommended that consensus be sought on developing harmonized policies and processes for sharing individual-level data which are informed by stakeholders’ views (Manju & Buckley, 2012; Whitworth, 2010).
This review identified just five examples of empirical literature into stakeholders’ experiences of and views about sharing individual-level data, all of which focused on the views of data producers and reviewers, primarily from higher income settings (Kirwan, 1997; Rathi et al., 2012; Reidpath & Allotey, 2001; Savage & Vickers, 2009; C. T. Smith et al., 2014). Four of the five studies have sample sizes of 30 or less, and three are five or more years old. Although the findings from these articles provide interesting insights into researchers’ opinions and practices of sharing data, some of the perspectives are dated, and differences in the research questions and approaches mean that views of best practices have not been systematically elicited.
This review was unable to identify any empirical research into research participants’ perspectives about sharing individual-level data from clinical and public health research that does not involve genetic, genomic, or biobank research. In addition, no research into stakeholders’ experiences and perspectives of best practices in sharing clinical data in low- and middle-income settings was found. To develop best practices in data sharing that are appropriate in low- and middle-income settings, empirical research into the perspectives of stakeholders from such settings is needed. We suggest that research into the perspectives of research participants, community representatives, researchers, research ethics committees, and data managers be made a priority to inform current policy development initiatives. The following five articles in this special issue begin to address this gap in the literature and report on the results of empirical studies of stakeholders’ perspectives in India, Kenya, Thailand, South Africa, and Vietnam (Cheah et al., 2015; Denny, Silaigwana, Wassenaar, Bull, & Parker, 2015; Hate et al., 2015; Jao et al., 2015; Merson et al., 2015).
Eight of the conceptual articles in this scoping review focused on the perspectives of stakeholders from low- and middle-income settings (Manju & Buckley, 2012; Pisani & AbouZahr, 2010; Pisani et al., 2010a, 2010b; Rani et al., 2011; Sankoh & Ijsselmuiden, 2011; Tangcharoensathien et al., 2010; Whitworth, 2010). These articles suggest that challenges raised by sharing individual-level data from low- and middle-income settings can differ in important and morally significant ways from those arising in high-income settings. An example is the critical importance of building capacity to generate, curate, share, and analyze high-quality datasets if data are to be shared effectively and fairly. Further theoretical analysis will be valuable to evaluate additional issues arising when sharing individual-level data in low- and middle-income settings, and to inform how best to address them (Bull, Cheah et al., 2015).
Limitations of the Review
Although double screening of all materials is desirable in systematic reviews, it was not possible in this case due to the volume of potential references identified and the complexity of determining the relevance of papers from the supplied abstracts. To minimize error and bias, 20% of abstracts were co-reviewed, and the strategy for a structured approach to analysis was discussed by the co-authors with the collaborating partners in this study. A second limitation of this review is that it was confined to literature in peer-reviewed publications. A valuable addition to the findings of this review would be a review of policies and processes currently in place for curating and sharing individual-level data from clinical and public health research.
Footnotes
Acknowledgements
The authors acknowledge and greatly appreciate the contributions of partners in the multi-site empirical study, particularly Spencer Denny, toward the initial co-review of abstracts.
Authors’ Note
The views expressed here are the opinions of the authors and not of the University of Oxford.
Declaration of conflict of interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Wellcome Trust Strategic Award 096527, on behalf of the Public Health Research Data Forum. The Forum brings together more than 20 health research funders, who are committed to increasing the availability of health research data in ways that are equitable, ethical, and efficient, and will accelerate improvements in public health (![]() ).
).