
Abstract
Ms. Braun, a new Special Education Director in the Baso Unified School District, is under pressure to curtail district expenditures on special education services. In her quest to understand why special education enrollment has increased, Ms. Braun learns about the challenges students face when accessing physical and mental health services at school and in the community. This case illustrates how initiatives for improving special education intersect with other district priorities and sheds light on the challenges education and health administrators face in fostering effective cross-sector collaboration.
Keywords
With the increasing prevalence of anxiety and depression among young people (Mental Health America, 2022), education leaders are recognizing the crucial role schools play in promoting students’ physical and mental well-being. The Biden–Harris administration has made addressing the mental health crisis a key part of its agenda (The White House, 2022) and the U.S. Department of Education (U.S. DOE) has invested hundreds of millions of dollars in grants to local educational agencies to increase access to school-based mental health services (U.S. DOE, 2023). State governments nationwide are similarly enacting legislation in the fields of education and public health in response to concerns about the mental health of children and adolescents (Palacios et al., 2023).
These legislative efforts often emphasize cooperative approaches in fostering cross-sector collaboration between health care and education. In California, recent significant investments in cross-sector cooperation include grants for local educational agencies to initiate school-based health care programs, incentives for health care plans to collaborate with school districts in delivering school-based health care, and a newly established state office of school-based health to facilitate cross-sector collaboration (California Department of Education [CDE] et al., 2021). As policymakers in California and throughout the country allocate substantial taxpayer funds to support health care services in schools, local health and education agencies are faced with the responsibility of working together to meet the academic and health needs of students. School-based health partnerships, including mental health care in schools, often require this type of cross-sector collaboration. Establishing and maintaining direct partnerships between school districts, community organizations, local hospitals, and/or school-based health centers can present complex challenges. The following case delves into the intricacies of this complexity within the Baso Unified School District (BUSD).
Case Background
The BUSD covers nearly 150 square miles in the southeastern part of California. BUSD is a large school district serving more than 50,000 children and adolescents, including many who live in rural communities. More than 80% of the district’s students are eligible for free or reduced price lunch, 25% are emergent bilingual students, and nearly 20% are considered “chronically absent” because they are absent more than 10% of the school year. Over the past 5 years, enrollment at BUSD has declined due to attrition from the community as young adults leave the county to seek employment in urban areas. The expansion of charter schools has also contributed to declining enrollment at BUSD. Charters now enroll close to 10% of the children and adolescents in BUSD’s attendance area. As these factors erode BUSD’s overall student enrollment, the percentage of students who receive special education services has increased from 11% to 14% over the past 5 years. Declining enrollment has also reduced financial assistance from the state which is a key source of revenue for BUSD.
Important Individuals
Ms. Braun: BUSD Special Education Director
Ms. Braun is a first-year special education director at BUSD. Prior to earning her administrative credential and accepting the Special Education Director position, Ms. Braun was a special education teacher for 10 years in an urban area near Baso County. Ms. Braun is an advocate for children with disabilities, including her own son who attends a special day class at one of Baso’s large high schools. Ms. Braun is especially passionate about helping students with disabilities participate in general education. Her strong relationships and high expectations for students helped her expand inclusive practices at her former district. In her new role as an administrator in an unfamiliar county, Ms. Braun is just beginning to build relationships at work and in the community that will help her improve special education at BUSD.
Mr. Norbit: Director of Baso County Mental Health Department
Mr. Norbit has been the Director of the Baso County Mental Health Department for nearly 25 years. He is preparing to retire after a long career as a mental health professional and program administrator. Mr. Norbit has many relationships in the county but none with education administrators. He has tried to build connections in the education sector but found that the high rates of turnover in schools and districts stymied relationship building.
Dr. Salazar: BUSD Superintendent
Dr. Salazar is in his fifth year as superintendent at BUSD. He is a former general education high school teacher and middle school principal. His priority at BUSD relates to improving services and outcomes for emergent bilingual students. Dr. Salazar has little experience in special education and sometimes feels it is unfair to spend so much of the district’s resources to serve such a small percentage of the student population. He hired Ms. Braun because of her success developing inclusive practices for students with disabilities at her former district. He hopes that serving more students with disabilities in inclusive settings will help reduce special education costs for BUSD.
Case Narrative
While overall enrollment is declining at BUSD, special education enrollment and its associated costs are rising. BUSD’s Special Education Director, Ms. Braun, is feeling the pressure from her superintendent, Dr. Salazar, to address the high cost of special education. She knows that special education referrals have gone up in recent years resulting in higher rates of students receiving special education and related services. She compiles data on the disability categories of students in special education over time to learn more about how rates within disability categories have changed (Table 1).
Disability Categories of Students in Special Education at BUSD.
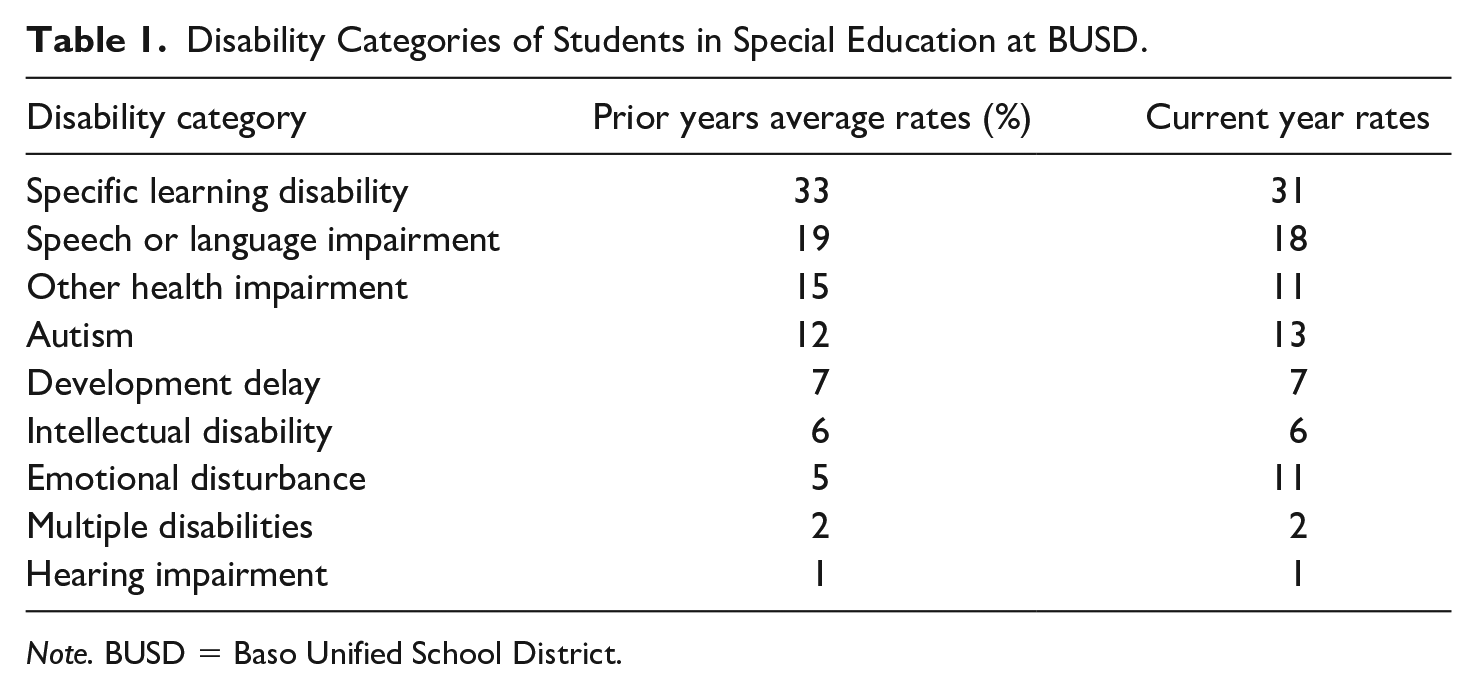
Note. BUSD = Baso Unified School District.
Ms. Braun notices that the current year rates by disability category are different than prior year averages but she is not sure what has caused the changes.
Especially concerning to Ms. Braun is the rise in students found eligible for special education under the category of emotional disturbance. Under the Individuals with Disabilities Education Act (IDEA), emotional disturbance is characterized by long-term behavioral patterns that adversely affect a child’s educational performance, such as trouble building and maintaining interpersonal relationships and frequently displaying inappropriate behavior or feelings. Ms. Braun worries it may be difficult for practitioners to distinguish between behavior resulting from an emotional disability and symptoms of chronic stress stemming from abuse, neglect, or substance abuse. She wonders if some students’ lack of access to mental health support is causing their stress to become unmanageable. She worries teachers may misidentify behavior and feeling resulting from chronic stress as emotional disturbance, ultimately contributing to high rates of special education referral.
Ms. Braun raises her concerns about the rising rates of students identified with emotional disturbance with Dr. Salazar and the district’s Chief Business Officer. She wonders aloud if the district can hire additional counselors to provide mental health support for students before they are referred for special education. The Chief Business officer shows her that the budget for mental health services in the district is squeezed so tightly that some counselors cover more than 1,000 children and adolescents across multiple school sites. While this finding suggests Ms. Braun’s concerns about service access are valid, Dr. Salazar is clear that there are no additional funds available to hire more counselors.
Ms. Braun reaches out to the County Office of Education and connects with Mr. Norbit, the Director of County Mental Health, within the County Mental Health Department. Curious about the options available to students in BUSD, Ms. Braun inquires whether they can access mental health care through community organizations or the County Mental Health Department. Mr. Norbit acknowledges that many students in BUSD are either enrolled in or eligible for Medi-Cal, California’s Medicaid program, which covers both their physical and mental health needs. However, he explains that despite this coverage, many of these children do not receive the mental health services they require due to challenges their parents or guardians face in navigating the complex Medi-Cal enrollment process. Moreover, he highlights that transportation becomes a significant obstacle, as parents often struggle to transport students long distances to access mental health treatment from Medi-Cal providers. Mr. Norbit emphasizes that these persistent barriers to treatment may explain why community providers encounter difficulties in identifying and serving the children and adolescents who qualify for mental health care through Medi-Cal.
Mr. Norbit also notes that because of challenges with treatment access in the community, youth who are eligible for Medi-Cal and/or who do not have health insurance benefit from access to health care through schools. When Ms. Braun inquires about school–health partnerships in Baso County, Mr. Norbit explains that the turnover in administrators at BUSD makes it difficult to build working relationships. When she probes further about what it takes for health and education systems to work together, Mr. Norbit starts speaking in unfamiliar terms related to medical billing, treatment plans, and Medicaid policy.
When she hangs up, Ms. Braun is grateful to Mr. Norbit for the information but feels overwhelmed. Mr. Norbit’s department is struggling to provide mental health services to the community too but for different reasons. He also seems aware that schools could help him reach young people but seems burned out from recurring failed partnerships with schools over the course of his career. Ms. Braun has no experience working in health care and after an initial internet search she realizes that the world of health care policy is just as complex and full of jargon as the special education field. She does find evidence that schools can effectively partner with federally qualified health centers, local government agencies, universities, medical providers, community-based organizations, and/or foundations to help finance school-based health care programs. She also notes that schools can become Medi-Cal providers through the state and then bill for the services they provide to students, potentially receiving up to 50% of the costs back in federal reimbursement.
The myriad options for health and education partnerships and the complexity of medical billing add to her overwhelm, but she schedules a meeting with Dr. Salazar to discuss what she has learned so far. When Ms. Braun takes the information to Dr. Salazar, he seems exasperated. He reiterates that there is no money to hire additional mental health professionals and that she needs to focus on reducing costs for special education, not hiring more providers. Dr. Salazar is clear that the district priorities are improving academic outcomes, especially for emergent bilingual students, and reducing the overreliance on special education to provide remediation to struggling students.
That afternoon, Ms. Braun picks up her son from his high school. She mentions access to mental health services to her son’s teacher who tells her it is not just mental health services that the students need. The teacher explains that many of the students on her caseload over the years have lacked access to regular physical health and dental care too. She says many children are not identified with developmental delays until they come to kindergarten because of their lack of access to health screenings. As a result, they miss out on their right to special education services during early childhood. Moreover, she feels that poor health in the community contributes to the chronic absenteeism she observes with her students.
Ms. Braun returns home with the information from the day swirling in her head. She knows that getting Dr. Salazar to agree to hire more mental health professionals will be an uphill battle. She wants to figure out if the school district can partner with other youth-serving agencies so students can get the physical and mental health services they need without increasing the cost to BUSD. Ms. Braun also knows that she has not clearly articulated how health and special education spending might be linked, nor how the population of emergent bilingual students that Dr. Salazar is passionate about helping could benefit from health services provided at school.
Teaching Notes
Ms. Braun thinks there is a way for school–health partnerships to both support the population of emergent bilingual students and reduce special education costs in the long term. She struggles to frame the value proposition to Dr. Salazar without a clear understanding of school-based health care, Medicaid reimbursement, and cross-sector collaboration.
School-Based Health Care
Research evidence has demonstrated the connection between student health and student academic achievement. Studies have established that better physical health contributes to higher academic achievement (Coe et al., 2013; Ickovics et al., 2014) and test score gains across student groups over time (Hanson et al., 2004). Better student and parent health can also mediate the effects of socioeconomic status on academic achievement (Barr, 2015), positioning access to health care as a potential avenue for schools to address opportunity gaps.
School-based health care services, offered on school campuses by health care providers affiliated with Pre-K–12 public schools or postsecondary institutions, are organized and provided in various ways. One evidence-based approach to support students’ health within schools is the establishment of school-based health care centers (Michael et al., 2015). These health clinics on school campuses have been associated with a multitude of positive educational and health outcomes. Students attending schools with school-based health centers experience improved grade point averages, attendance rates, vaccination rates, reproductive health, and mental well-being (Knopf et al., 2016). In addition, school-based health centers have shown effectiveness in enhancing school connectedness among adolescents from low socioeconomic backgrounds (Bersamin et al., 2018).
Medicaid Reimbursement
While the positive outcomes associated with school-based health care underscore its importance, funding remains a significant obstacle to implementing health care services within schools. In California, as well as in other states, a significant portion of the funding allocated to school districts is directed toward essential services such as classroom instruction (CDE, 2021). Only a fraction of the available funding specifically earmarked for school-based health services directly reaches school districts (CDE, 2021). To overcome these barriers, many school districts establish partnerships with federally qualified health centers, local government agencies, universities, Medicaid providers, community-based organizations, and/or foundations to help finance school-based health care programs (Dunfee, 2020).
Medicaid reimbursement offers another source of financial support for school-based health care services. Medicaid is a public health insurance program that covers health care services to individuals who meet income or other eligibility requirements. Medicaid billing programs can help reimburse local agencies for the services they provide to Medicaid-eligible students under certain circumstances, such as when the child who receives the service is enrolled in Medicaid (Centers for Medicare and Medicaid Services [CMS], 2023). Reimbursable services may include medical care, mental health care, dental care, health education, and substance abuse counseling (CMS, 2023). Many special education and related services that schools provide to students with disabilities are eligible for Medicaid reimbursement (CMS, 2023). Notably, children and adolescents who are eligible for Medicaid and/or who do not have health insurance are the most likely groups to access health care through schools (Amaral et al., 2011; Koenig et al., 2016), underscoring the critical importance of school-based health care for educational and health equity.
Cross-Sector Collaboration and Sustainability
Medicaid requirements are governed by federal laws and regulations and administered by state departments of health, not state departments of education. As a result, school-based health care often necessitates cross-sector collaboration with other state agencies and other local youth-serving agencies that are familiar with health care and Medicaid requirements. This cross-sector collaboration can pose challenges for school districts, including that other agencies might use different language to describe the same idea or process (e.g., an individual education program vs. a treatment plan) which can hinder cross-sector understanding. In addition, staff turnover can prevent partnerships from maturing into robust physical and mental health partnerships. School districts can also face technical challenges such as extensive paperwork, opaque auditing processes, and long wait periods for reimbursement when they bill Medicaid.
Despite the challenges that come from working across sectors, formal and informal collaboration is widespread in education (Henig et al., 2016). The formal collaboration between health and education systems described in this case is just one of the many kinds of partnerships in education. Common partnership models in education include community schools, collective impact initiatives, school–family–community partnerships, cradle to career initiatives, and public–private partnerships. While the specifics of these models may be different, successful cross-sector partnerships in education share some common features. One feature of successful partnerships is a common vision, agenda, and plan of action for solving a specific social problem (Henig et al., 2015; Kania & Kramer, 2011). Successful partners also have a shared data and/or measurement system that helps them align their efforts and ensure measurable impact (Henig et al., 2016; Kania & Kramer, 2011). Finally, partners have opportunities to consistently collaborate and build trusting relationships (Henig et al., 2015; Kania & Kramer, 2011). Even with these features in place, successful cross-sector collaboration is difficult to establish and sustain over time because of many of issues touched on in this case such as staff turnover, shifting priorities, and resource constraints (Bryson et al., 2015; Henig et al., 2015; Karp & Lundy-Wagner, 2016).
Community schools commonly include school-based health centers and are thus an illustrative example of cross-sector collaboration for the Baso County case (Maier et al., 2017). Community schools, which operate through the collective efforts of community members, families, and students, facilitate opportunities for collaboration and resource sharing to address the needs of children and adolescents in a community. A strong evidence base demonstrates that implementing comprehensive community schools with fidelity can enhance student attendance, behavior, social skills, and academic achievement (Kirp, 2011; Maier et al., 2017; National Research Council & Institute of Medicine, 2004). Longer-running community schools tend to be more effective (Maier et al., 2017), indicating that sustained investment and consistent staffing is critically important to a successful community school and an effective school-based health program.
Classroom Activities and Discussion Questions
Despite the strong evidence base to support school-based health care, the implementation of school-based health policy is complex. It often involves multi-agency collaboration and knowledge of Medicaid billing programs. The circumstances of this case reflect how improvement efforts in special education intersect with other district priorities and illustrate the complexity of building cross-sector partnerships in education. The case specifically discusses school–health partnerships, but similar challenges might apply to other partnerships in education such as for after school programs or preschool services.
Have a large group discussion to identify the challenges in the case. What factors in Baso County and BUSD might make solving these challenges especially complex?
Have a small group discussion about problem construction and data use. How does Ms. Braun conceptualize the root causes of the problem that BUSD needs to solve? Do you agree with her conclusion? What other data should Ms. Braun collect or review as she considers root causes?
In small groups create a systems or network map using a county you are familiar with. Brainstorm all the key actors in the county that may get involved in coordinating, designing, or administering a school–health partnership. Draw lines of connection among the actors. If it were up to your group, who would you talk with first and what questions would you ask?
Using your system map, identify a potential community partner and conduct an interview with someone who works there. Develop interview questions about the services they provide, any opportunities to collaborate with schools, and their experience with cross-sector collaboration.
In small groups consider how Ms. Braun should approach her superintendent. Should she engage other district staff in the next meeting? If so, who might she prioritize? What information might she bring to the next meeting? How might she present her ideas? What considerations inform your answer?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.