
Abstract
Background
Near-infrared fluorescence (NIF)-mapping with indocyanine green dye (ICG) facilitates the identification of the intersegmental plane during minimally invasive segmentectomy. Our pilot study showed that ICG is associated with an increase in oncological margin distance from the tumour, greater than the surgeon’s best judgment. We hypothesized that, with greater experience, the surgeon’s judgement will improve, and the benefit of ICG will diminish.
Methods
This is a phase 2 single-arm trial of patients undergoing robotic-assisted segmentectomy for NSCLC tumours less than 3 cm. After isolating the diseased segment(s), the predicted intersegmental plane (Dp) was identified by the thoracic surgeon. After intravenous ICG injection, the true intersegmental plane (Dt) was revealed using NIF. The primary outcome was the average distance between Dt and Dp (Dt-Dp). Comparisons were performed across 3 temporal tertiles: tertile 1 (t1) comprised of the first 30 participants, and the remaining participants were divided equally for tertiles 2 (t2) and 3 (t3). Kruskal-Wallis test was used to compare differences between tertiles (α = 0.05).
Results
A total of 190 patients were enrolled from October 2016 to June 2021. The median age was 68 (interquartile range:62-72), and 57.37%(109/190) were women. ICG injection occurred in 60.53%(115/190) of the participants, and intersegmental plane visualization was achieved in 88.70%(102/115). Dt-Dp diminished significantly across tertiles: t1 = 20.65 ± 15.82 mm, t2 = 2.42 ± 15.49 mm, and t3 = 1.36 ± 9.87 mm (P = 0.0001). Locally estimated scatterplot smoothing revealed that this distance approaches zero as the surgeon performs more cases.
Conclusion
In our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added value of NIF-mapping with ICG diminishes with surgeon experience.
Keywords
Introduction
Near-infrared fluorescence (NIF)-mapping with indocyanine green dye (ICG) is a useful intraoperative adjunct that provides a clear demarcation of the intersegmental plane during minimally invasive segmentectomy. 1 This technique involves the isolation of the target segment by ligation of the bronchus, vein, and artery within the hilum of the lung. ICG is then injected intravenously and perfuses all lung tissue except for the isolated segment. A thoracoscope equipped with an NIF light source is then used to visualize the lung, and the entire lung will appear to fluoresce in green, except for the target segment isolated from the blood supply, which remains dark black. This provides a clear demarcation of the intersegmental plane between the green lung and the dark segment.
Previous retrospective studies have analyzed the impact of ICG in minimally invasive thoracic surgery.2-4 A more recent retrospective study comparing the perioperative outcomes of patients who underwent minimally invasive segmentectomy using either the deflation-inflation method or the ICG technique at a single-site from 2020-2023 found no significant differences in clinical effectiveness nor postoperative complications, and no added value of ICG on the perioperative results, 2 while previous single-site retrospective studies found that the ICG group had a significantly shorter operative time,3,4 and a significantly lower incidence of postoperative prolonged air leaks. 4
In a pilot study conducted at our center, we assessed the reproducibility of NIF-mapping, and determined whether it provided any additional oncological margin distance from the tumour to the staple line, compared to the surgeon’s best judgment. 5 We demonstrated that NIF-mapping resulted in an average increase in the oncological margin distance by approximately 2 centimeters in most cases where it was used. 5 Given that this study reflected our early experience in robotic-assisted segmentectomy, we postulated that this effect may have been observed due to the learning curve associated with the procedure. 6 We hypothesized that as more cases are performed, and surgeon experience is gained, the location of the intersegmental plane predicted by the surgeon will become closer to the true plane mapped by ICG, and the added benefit of NIF-mapping will diminish.
Materials and Methods
Study Design
This is a prospective, single-arm, single centre continuous case series of NIF-guided robotic-assisted pulmonary segmental resections for non-small cell lung cancer (NSCLC).
Study Population
Patients were enrolled between October 2016 and June 2021. Inclusion criteria included the following: age 18 years or greater; tumour size less than 3 cm; clinical stage 1 NSCLC; and computed tomography (CT)-imaging confirming that the tumour is confined to 1 broncho-pulmonary segment, rendering the patient a candidate for segmental resection. Exclusion criteria included the following: hypersensitivity or allergy to ICG, sodium iodide, or iodine; and women who were currently pregnant or breastfeeding, or of childbearing potential who were not currently taking adequate birth control. Informed consent was obtained from all participants. Patients were prospectively enrolled in the study and were followed for 3 weeks post-operatively.
Research Ethics Approval and Trial Registration
This study was granted a no objection letter from Health Canada authorizing the off-label use of ICG (#184323), was approved by the Hamilton Integrated Research Ethics Board (#0101), and was conducted in compliance with the Canadian Tri-Council Policy Statement on Ethical Conduct for Research Involving Human Subjects. 7 This trial was registered on ClinicalTrials.gov (#NCT02570815).
Surgical Technique
Operations were conducted by 1 thoracic surgeon on the DaVinci Si and Xi (Intuitive Surgical, Sunnyvale, California, USA) robotic platform, using the Completely Portal 4-Arm approach, 8 and the Firefly Fluorescence Imaging camera (Intuitive Surgical) as an NIF light source. All cases were attempted robotically at the beginning of the operation. Intraoperative conversion to lobectomy was mandated when N1 disease was suspected or confirmed on intraoperative frozen section, when positive margins were suspected on the resection specimen, or when the tumour was not found in the resection specimen. Conversion to thoracotomy occurred due to intraoperative complications or inability to progress robotically.
Following ligation of the corresponding segmental artery, vein, and bronchus, the surgeon identified the predicted intersegmental plane (Dp), which was then marked by cautery for future reference. Next, ICG was reconstituted into distilled water to produce a 2.5 mg/mL solution, and a volume of 6 to 10 mL (dose of 15-20 mg) was injected in a peripheral intravenous catheter, followed by a 10 mL flush of sterile normal saline. After injection, the surgical field was visualized with the integrated fluorescence imaging capability of the Firefly camera. The target segment, isolated from the pulmonary vasculature, exhibited no fluorescence, and remained dark. The remainder of the lung, perfused with ICG, exhibited bright green fluorescence. The true intersegmental plane (Dt) was then identified as the line separating the dark lung parenchyma from the green lung parenchyma. The Dt was then marked by cautery and stapled across to complete the division of the lung, and extract the diseased tissue.
Intraoperative Outcome Measures
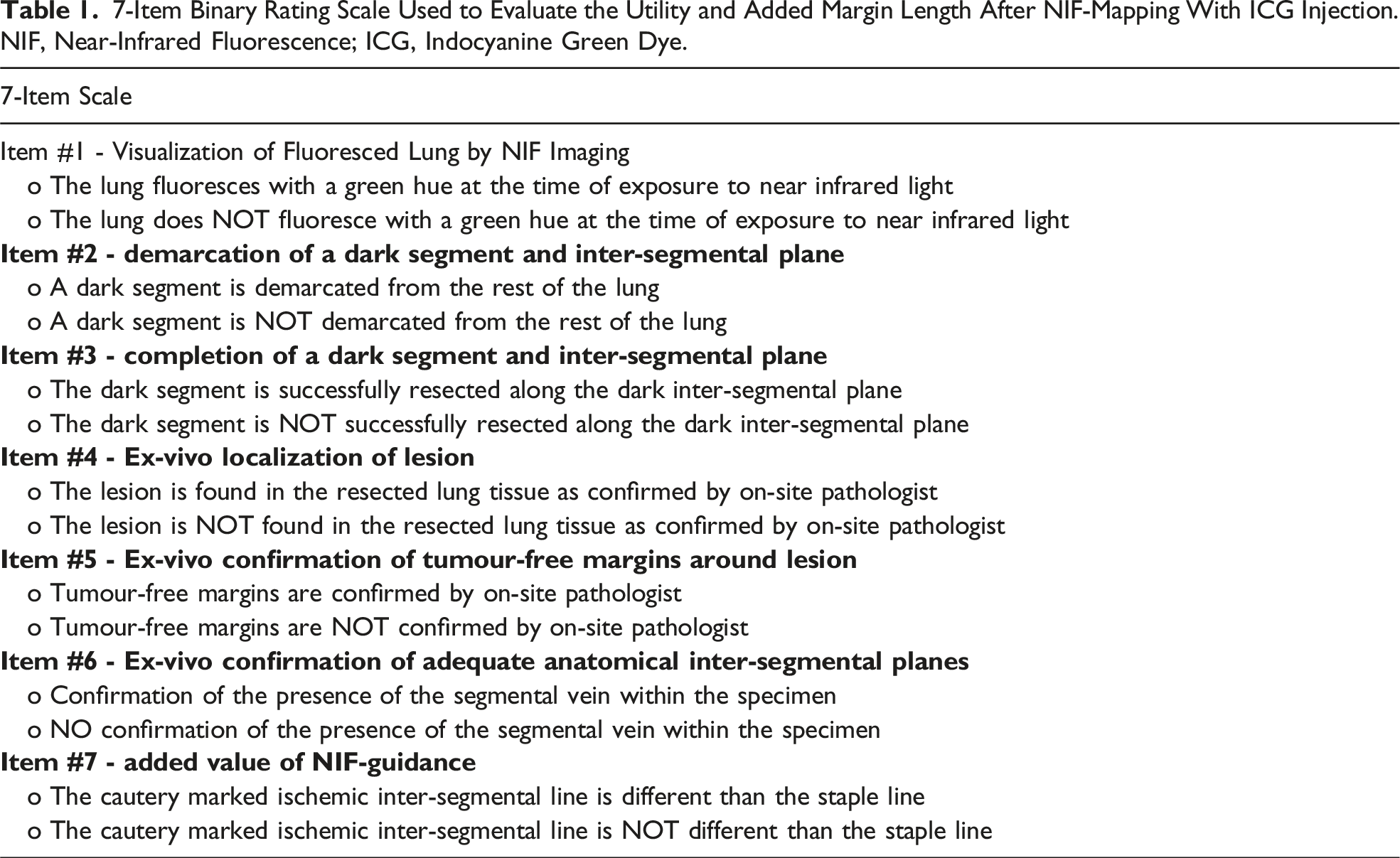
7-Item Binary Rating Scale Used to Evaluate the Utility and Added Margin Length After NIF-Mapping With ICG Injection. NIF, Near-Infrared Fluorescence; ICG, Indocyanine Green Dye.
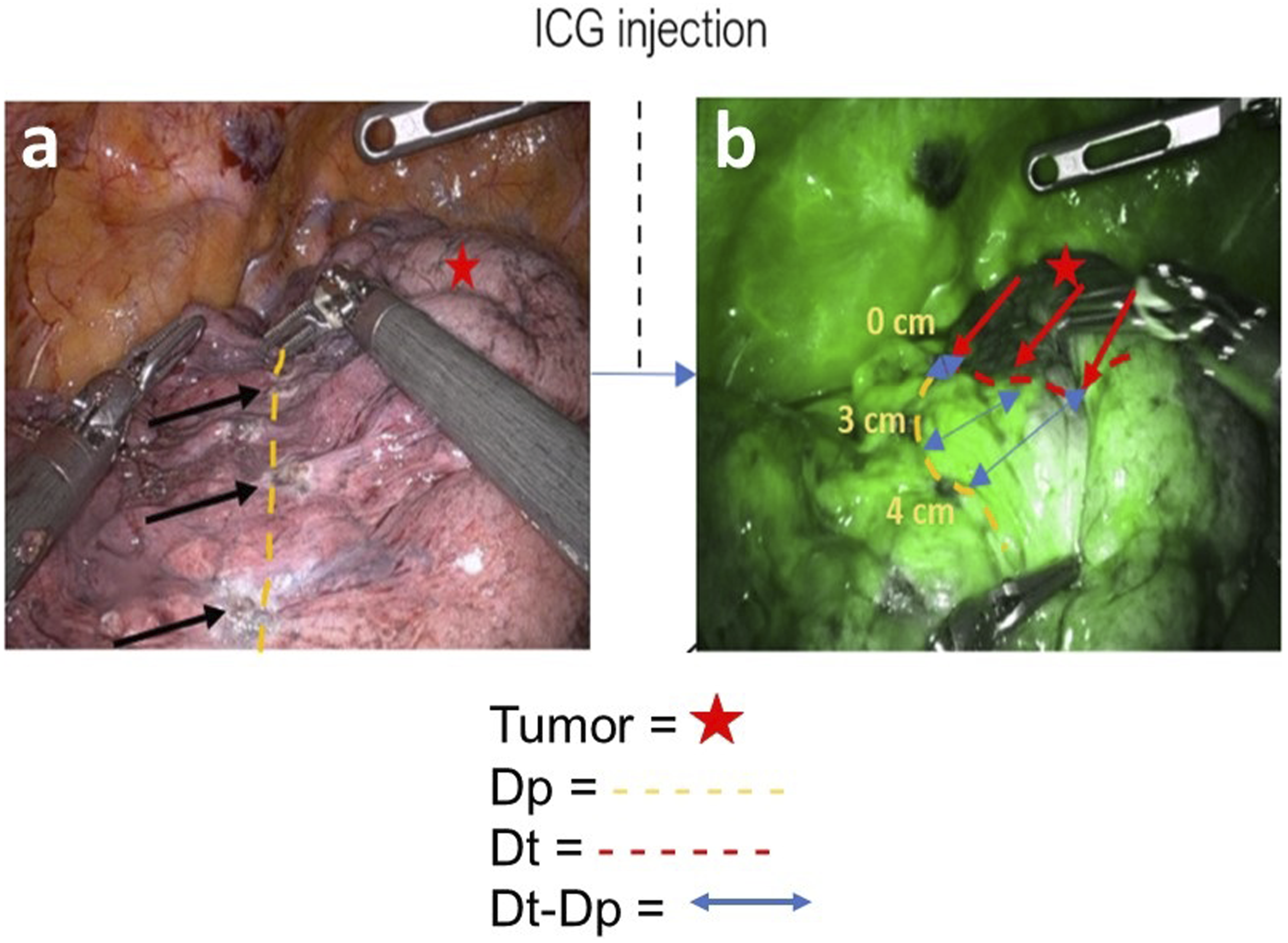
ICG Injection and Outcome Measurement Protocol. The primary outcome of this study was the average distance between the true plane and the predicted plane (Dt-Dp). After ligation of the vasculature, the predicted intersegmental plane (Dp) was marked with cautery by the surgeon, which is depicted as yellow dashes in Figure 1(A). After intravascular injection of indocyanine green dye, near-infrared fluorescence mapping delineates the actual intersegmental plane (Dt), depicted in red dashes in Figure 1(B), between the excluded segment (dark) and remaining lung (green). The blue arrows demonstrate the difference between the predicted plane and the true plane (Dt-Dp).
Data Items
Following enrollment, baseline data on patient demographic characteristics, medical history, social history, diagnosis, preoperative tests, and preoperative staging were collected. Preoperative variables included age, sex, smoking status, medical history, tumour size and location, pulmonary function, planned resection and complexity. Target segments were sub-categorized as “simple” or “complex”. Segmentectomy that creates 1 linear intersegmental plane was defined as simple - this includes the superior segment (S6) on either laterality, lingula (S4 + S5) and left upper lobe divisions (S1+S2+S3). Segmentectomy that creates several or intricate intersegmental planes was defined as complex, and included all non-simple segments. The allocation to the “simple” or “complex” sub-category was made a priori based on the preoperative imaging plan. Intraoperative variables included date of operation, post-operative diagnosis, tumour stage and maximal diameter, pulmonary resection type, additional resections, conversions to lobectomy, conversions to open thoracotomy, additional resections, total operative time, and operative time on the robotic console. Any serious adverse events resulting as a direct consequence of ICG administration were to be reported to the local institutional review board. Postoperative variables included hospital length of stay, duration of chest tube drainage, pathological staging, and postoperative complications and/or adverse events for up to 3 weeks post-operatively (assessed using the Ottawa Thoracic Morbidity & Mortality System). 9
Statistical Analysis
A per-protocol analysis was used, analyzing patients who received the ICG intervention. Descriptive statistics were presented as median [interquartile range (IQR)]. The percentage of successful cases was calculated as the sum of the number of cases scoring either a 6 or a 7 on the rating scale, divided by the total number of procedures where ICG was used. Cases were divided into 3 temporal intervals: Tertile 1 (t1) comprised the first 30 “training” cases, and the remaining cases were divided evenly between Tertile 2 (t2) and Tertile 3 (t3). Kruskal-Wallis test was used to compare differences between tertiles for non-parametric data and one-way analysis of variance for parametric data. A Chi-square test was used to compare categorical variables across tertiles. To observe the effects of a learning curve on Dt-Dp, a locally estimated scatterplot smoothing (LOESS) was performed where ICG case number was plotted on the x-axis against Dt-Dp. Statistical tests were two-sided, and the level of significance was set at α = 0.05.
Results
Study Population
Baseline Demographics and Clinical Characteristics of Entire Study Population.
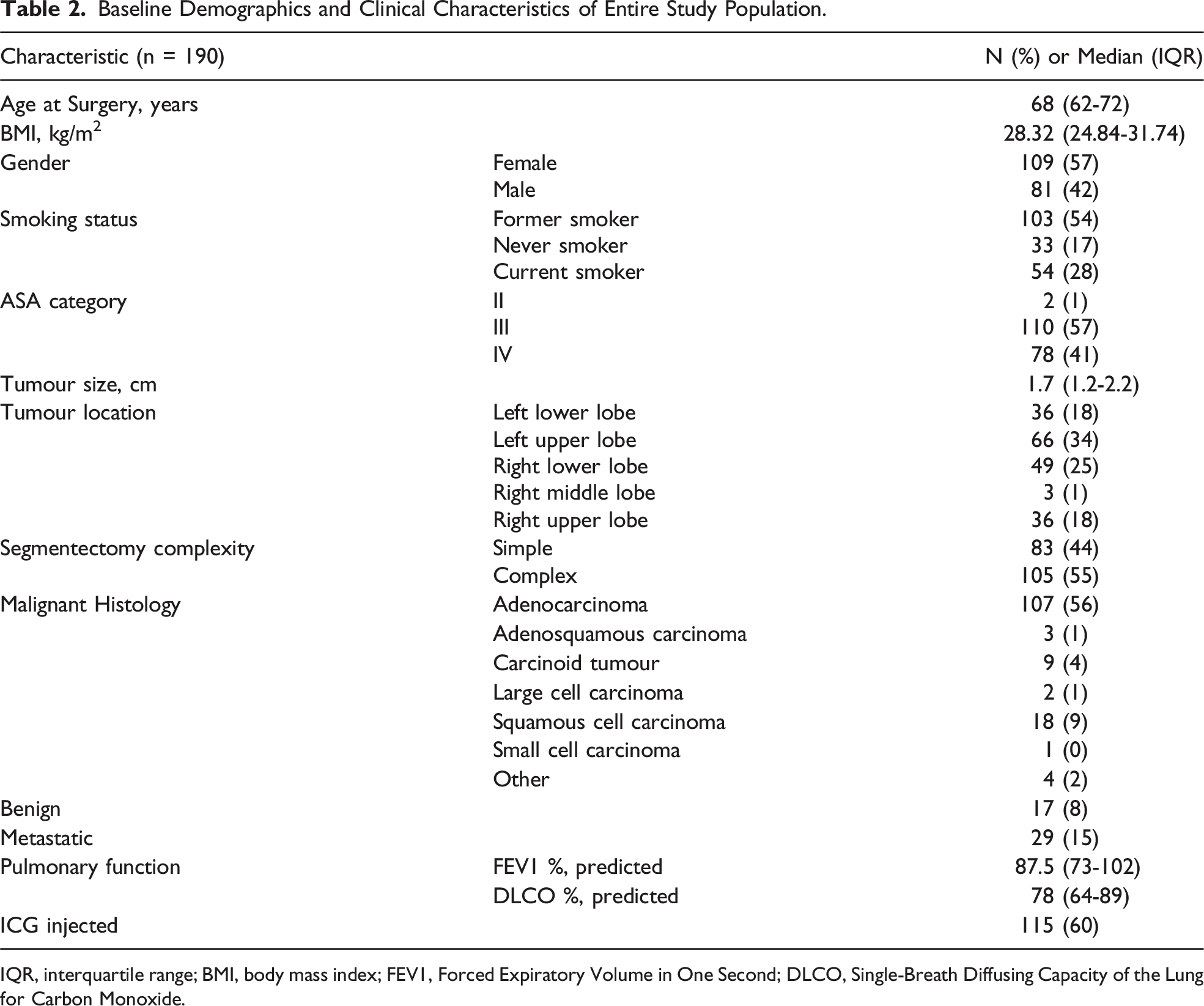
IQR, interquartile range; BMI, body mass index; FEV1, Forced Expiratory Volume in One Second; DLCO, Single-Breath Diffusing Capacity of the Lung for Carbon Monoxide.
Perioperative Outcomes of Entire Study Population Across Tertiles
The first tertile (t1) comprised of 30 cases (October 2016 – January 2018; 454 days), the second tertile (t2) comprised of 80 cases (January 2018 – December 2019; 713 days) and the third tertile (t3) comprised the remaining 80 cases (December 2019 – June 2021; 525 days). The median length of hospital stay (LOS) was 3 (IQR: 2-5) days and the median duration of chest tube drainage was 2 (IQR: 1-4) days. Operating room time [t1 = 174 (156-192) minutes; t2 = 171 (152-199) minutes; t3 = 164 (147-187) minutes; P = 0.20], skin-to-skin procedure time [t1 = 130 (108-149) minutes; t2 = 127 (103-157) minutes; t3 = 117 (101-139) minutes; P = 0.10], and console time [t1 = 88 (70-97) minutes; t2 = 92 (70-112) minutes; t3 = 87 (68-103) minutes; P = 0.67] did not differ significantly across tertiles. Twenty-nine participants underwent completion lobectomy [15.26%; (29/190): n = 20 via robotic and n = 9 via open thoracotomy), and the proportion of completion lobectomies decreased significantly across tertiles, with 30.00% (9/30), 13.75% (11/80) and 11.25% (9/80) occurring in t1, t2, and t3, respectively (P = 0.046). There were 19/190 (10.00%) conversions to open thoracotomy, and there was no significant difference in the proportions across tertiles [t1 = 13.33% (4/30); t2 = 13.75% (11/80); t3 = 5.00% (4/80); P = 0.15]. Conversions to thoracotomy occurred primarily due to dense adhesions or inability of patient to tolerate single-lung ventilation (4.74%; 9/190). Conversion to open thoracotomy also occurred due to vascular injury in 6/190 (3.16%); 1 in t1, 5 in t2, 0 in t3. Intraoperative complications occurred in 5.79% (11/190) of patients (n = 6: vascular injury causing bleeding which did not require a transfusion; n = 1: vascular injury causing bleeding which did require a transfusion; n = 1: chyle leak; n = 1: hypoxemia; n = 1 injury to airway; and n = 1 injury to lung/intraoperative air leak), and there was no significant difference in the incidence of intraoperative complications across tertiles [t1 = 3.33% (1/30); t2 = 7.50% (6/80); t3 = 5.00% (4/80); P = 0.77]. Post-operatively, major complications of Grade 3b or greater occurred in 3.68% (7/190) of participants, and there was no significant difference in the incidence of major postoperative complications across tertiles [t1 = 0% (0/30); t2 = 6.25% (5/80); t3 = 2.50% (2/80); P = 0.38]. There was 1 participant who suffered a Grade 5 adverse event, and this participant died 3 days after surgery due to a left middle cerebral artery stroke.
Baseline Characteristics and Perioperative Outcomes of ICG Patients Across Tertiles
Baseline Demographics and Clinical Characteristics of the Included Sample Across Tertiles.
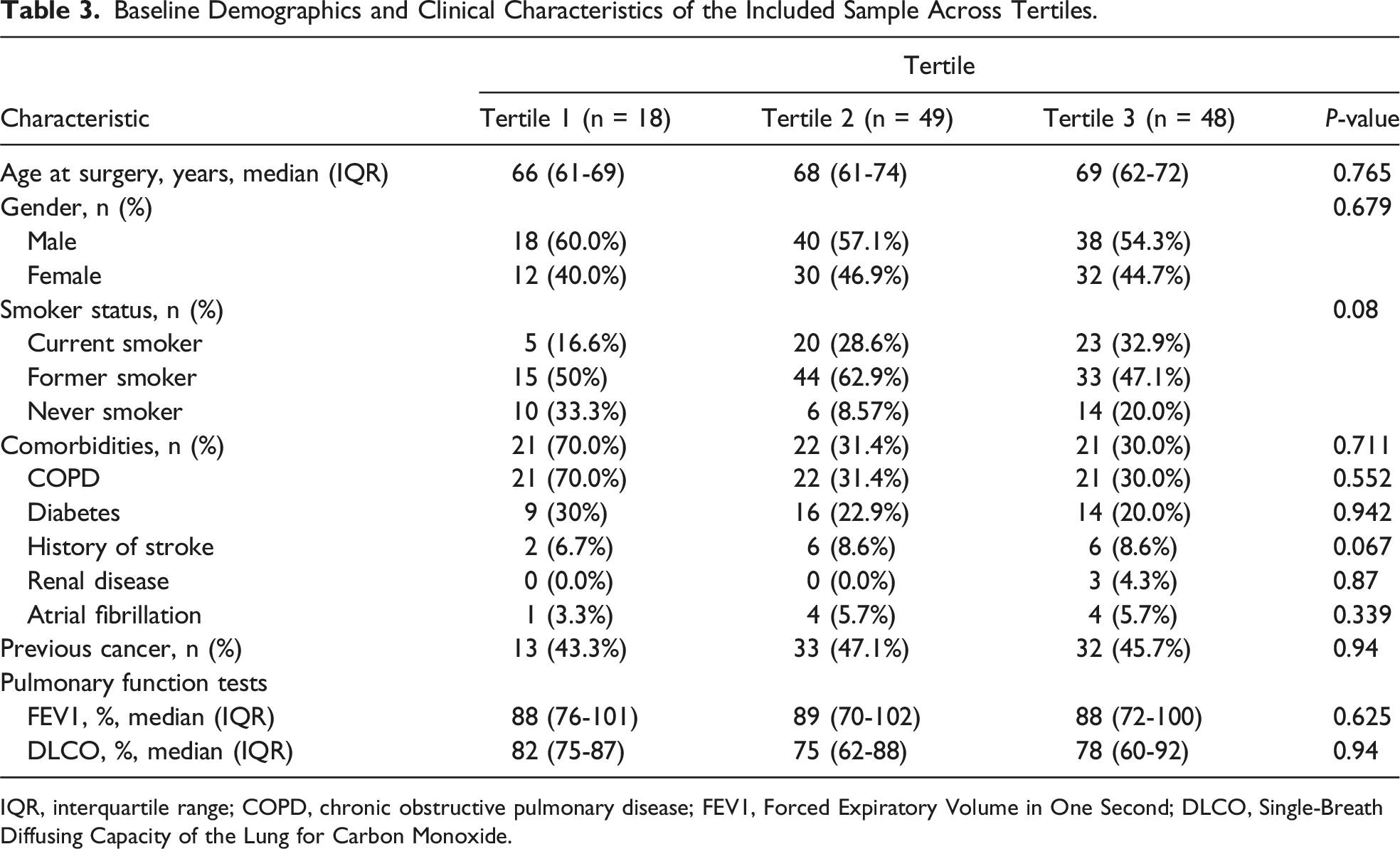
IQR, interquartile range; COPD, chronic obstructive pulmonary disease; FEV1, Forced Expiratory Volume in One Second; DLCO, Single-Breath Diffusing Capacity of the Lung for Carbon Monoxide.
Operative and ICG Outcomes of the Included Sample Across Tertiles.
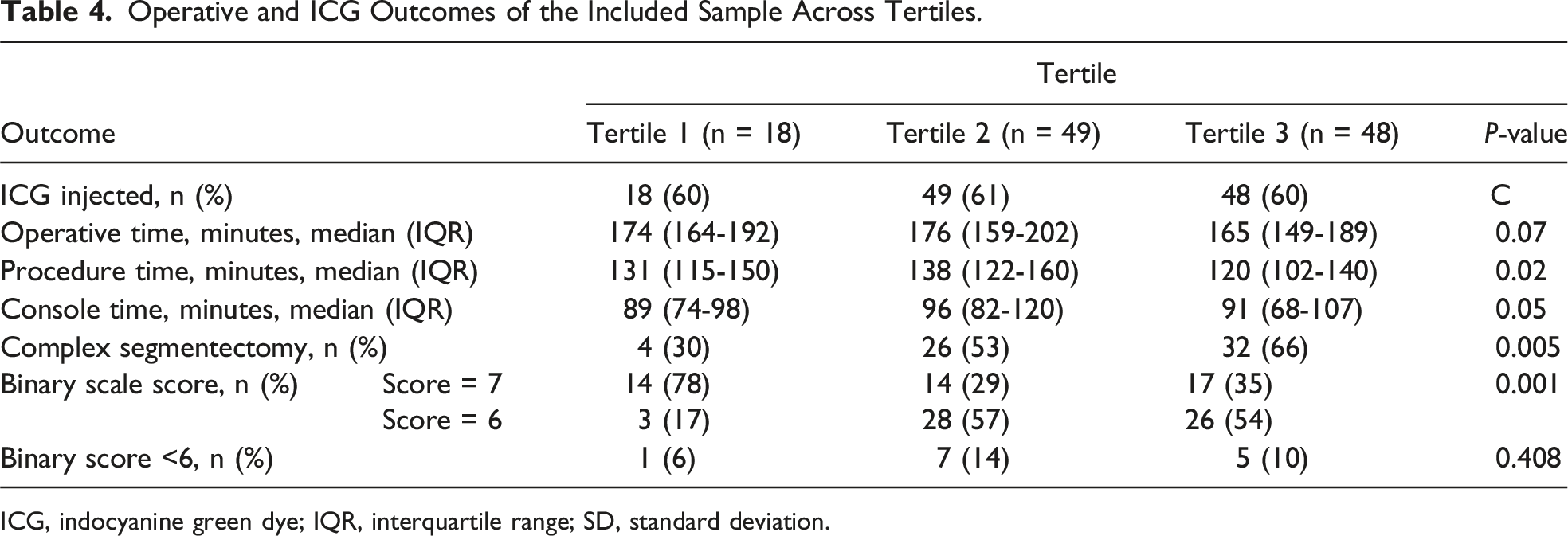
ICG, indocyanine green dye; IQR, interquartile range; SD, standard deviation.
There were no significant differences in the number of patients who received ICG in each tertile (t1 = 60.00% (18/30); t2 = 61.25% (49/80); t3 = 60.00% (48/80); P = 0.99). Successful intersegmental plane visualization using ICG was achieved in 102 out of 115 participants (88.70%), indicated by a score of 6 or 7 out of 7 on the binary scale, and there were no significant differences in the number of successful intersegmental plane visualizations using ICG across tertiles (t1 = 94.44% (17/18); t2 = 85.71% (42/49); t3 = 89.58% (43/48); P = 0.73). Unsuccessful intersegmental plane visualization occurred in 11.30% (13/115) of cases due to: no demarcation of a dark segment after ICG injection (n = 5), inability to resect along the dark intersegmental plane (n = 1), inability to localize tumour in resected specimen (n = 5), no confirmation of tumour-free margins by the on-site pathologist (n = 1), and no confirmation of the segmental vein within the resected specimen (n = 1). Most unsuccessful cases were for right-sided resections - primarily in the right lower lobe (n = 8), followed by right upper lobe (n = 3), and left lower lobe (n = 2).
Added Value of NIF-Guided ICG Mapping
All cases were scored using a 7-item binary scale and a score of 7/7 was achieved in 45 out of 102 (44.12%) successful cases. The proportion of cases scoring 7/7 decreased significantly across tertiles (t1 = 77.78% (14/18); t2 = 28.57% (14/49); t3 = 35.42% (17/48); P = 0.001). In these 45 cases, ICG corrected the surgeon’s estimate of the intersegmental plane by a median of 13.33 (IQR: 10.00-23.33) mm away from the tumour. This distance diminished significantly in t3 [10.00 (IQR: 6.67-10.00) mm], when compared to t1 and t2 [20.00 (IQR: 13.33-30.33) mm and 21.50 (IQR: 13.33-26.70) mm, respectively (P = 0.003)] (Figure 2). A score of 6/7 was achieved in the remaining 57 out of 102 (55.88%) cases, meaning ICG did not add any distance from the tumour compared to the surgeon’s initial estimate of the location of the intersegmental plane. When considering all 102 cases with successful NIF-mapping, ICG increased the added distance from the tumour by a mean of 4.86 ± 14.98 mm away from the tumour. This distance diminished significantly across all tertiles, initially at 20.65 ± 15.82 mm in t1, to 2.42 ± 15.49 mm in t2, and 1.36 ± 9.87 mm in t3 (P = 0.0001). Average Dt-Dp Across Tertiles. In the 45 cases in which ICG corrected the surgeon’s estimate of the intersegmental plane (score of 7/7 on the 7-item binary scale), the average Dt-Dp diminished significantly in Tertile 3 [10.00 (IQR: 6.67-10.00) mm], when compared to t1 and t2 [20.00 (IQR: 13.33-30.33) mm and 21.50 (IQR: 13.33-26.70) mm, respectively (P = 0.003)].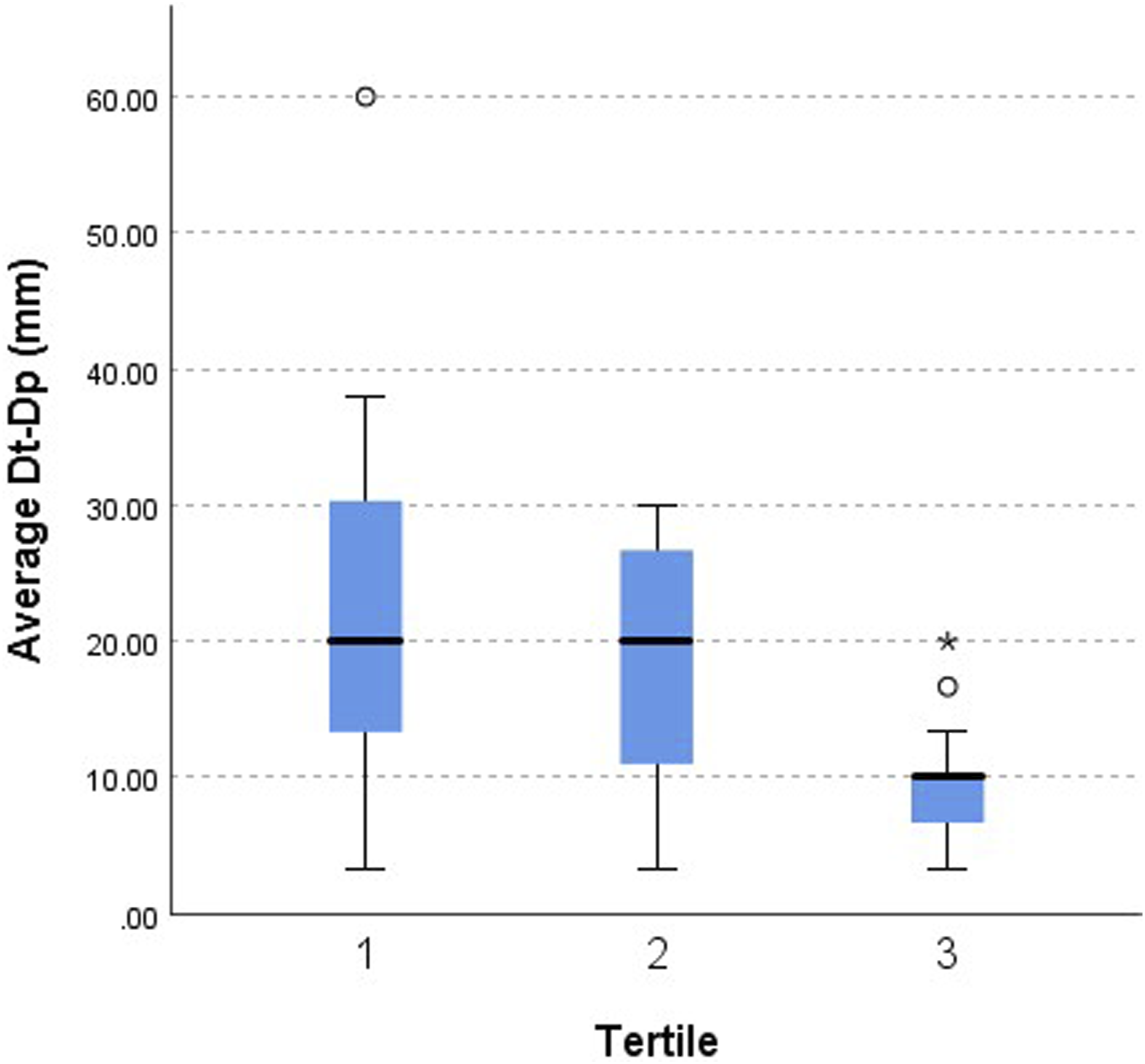
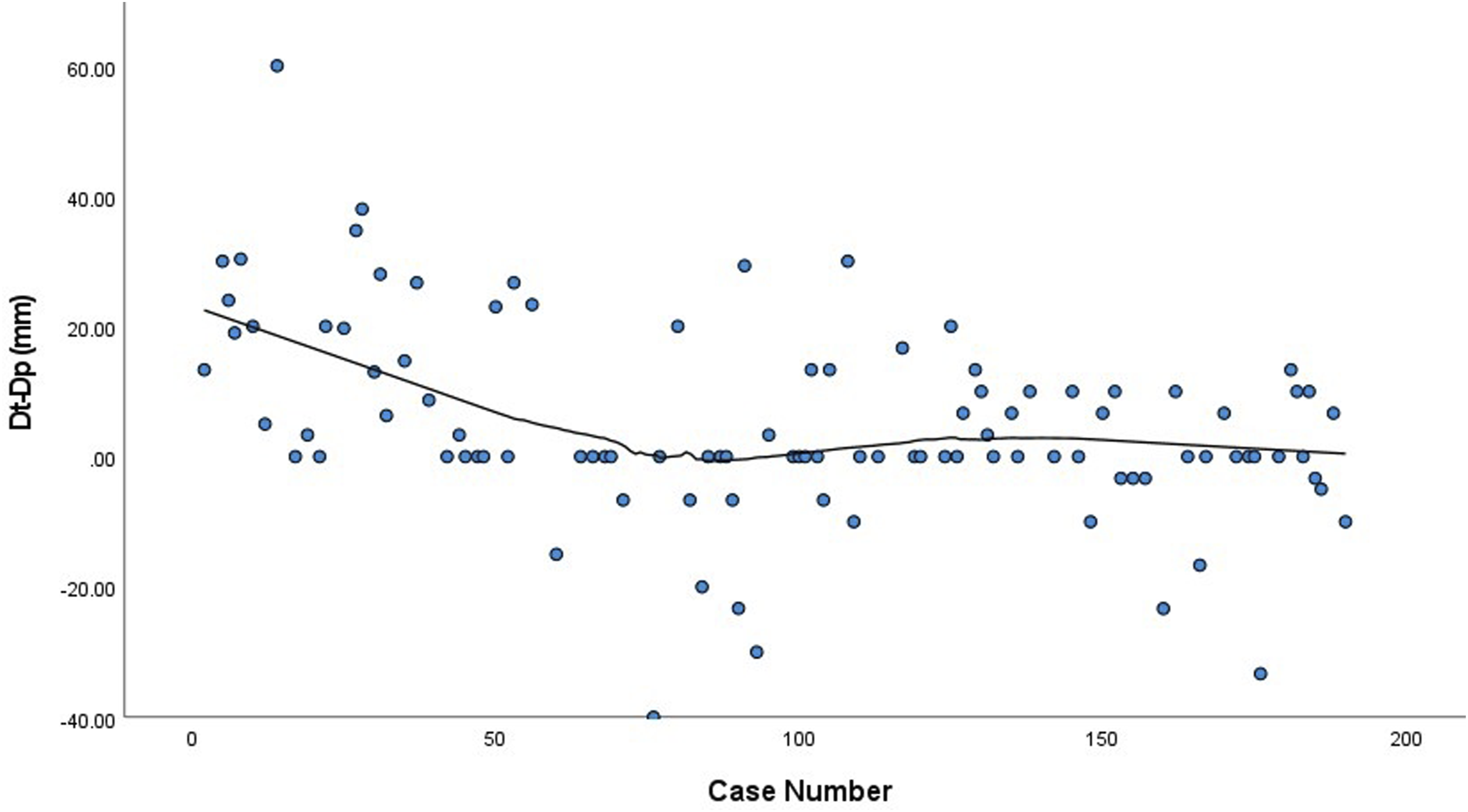
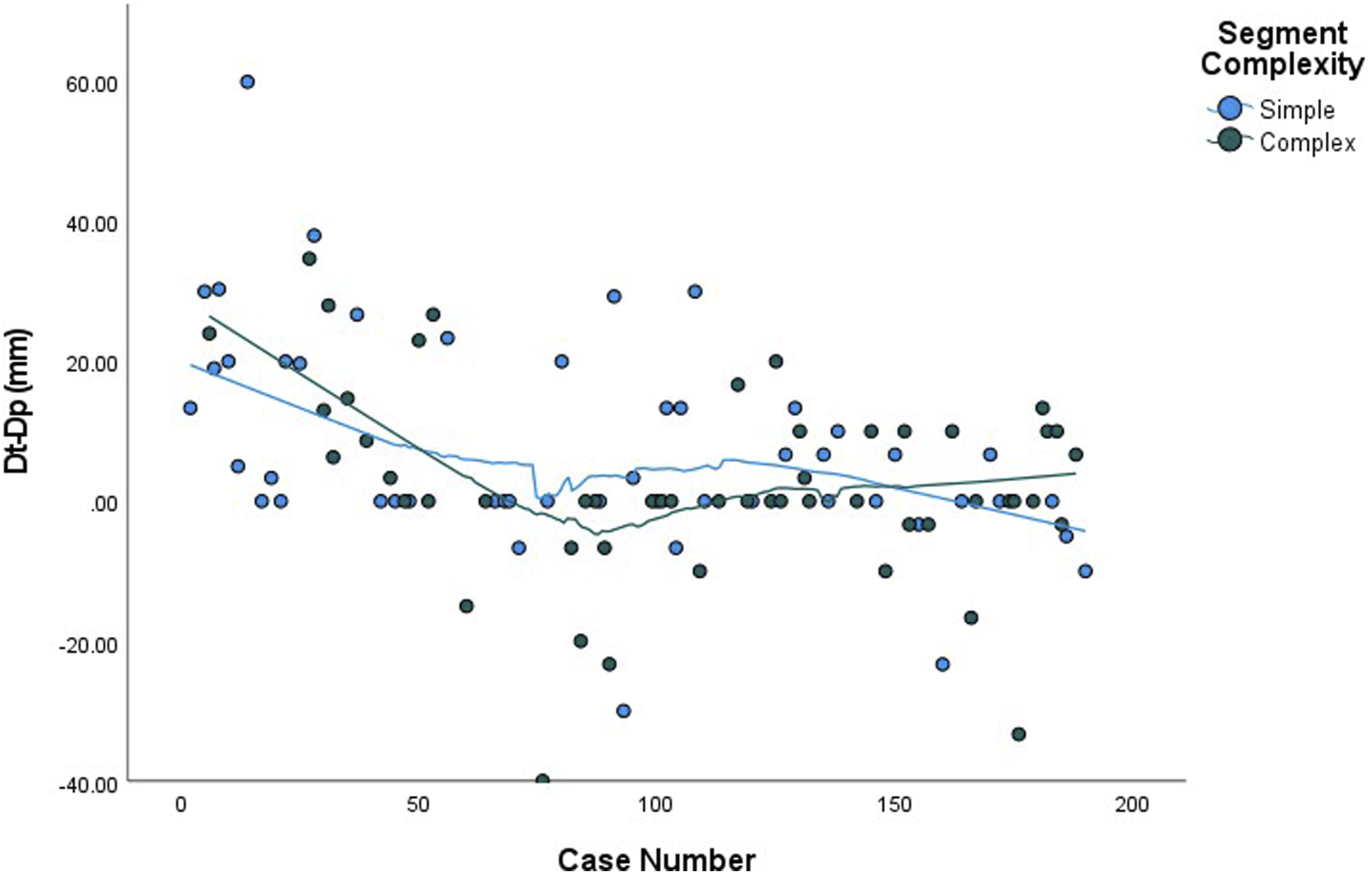
A locally estimated scatterplot smoothing (LOESS) was performed with ICG case number as the independent variable to examine the relationship between surgeon experience with ICG and the ability to predict the location of the invisible intersegmental plane (Figure 3). The plot shows a steady decline in Dt-Dp until approximately the 42nd case where ICG was used (case number 77), followed by a local minimum at 0.00 mm from the 43rd to the 62nd cases where ICG was used (case number 78-103). There is a subsequent increase in Dt-Dp by a few millimeters above zero around the 80th case where ICG was used (max 3.3 mm) before returning to 0.00 mm. Linear regression analysis revealed a strong negative association in Dt-Dp and ICG case number, when ICG case number was less than 42. Specifically, Dt-Dp decreased by a mean of 0.82 ± 0.41 mm/case until the 42nd consecutive case with ICG (P < 0.0001). After the 42nd case, this finding was no longer significant (P = 0.727). There is also a slight subsequent increase and increased variability in Dt-Dp in the second tertile (cases 18-67). A LOESS plot stratified by segment complexity (Figure 4) showed that this increase was mostly associated with simple, and not complex, segmentectomy. Added Value of Indocyanine Green Dye Over Surgeon’s Case Number. A locally estimated scatterplot smoothing was performed with ICG case number as the independent variable to examine the relationship between surgeon experience with ICG and the ability to predict the location of the invisible intersegmental plane. Added Value of Indocyanine Green Dye Stratified by Segment Complexity. A locally estimated scatterplot smoothing plot stratified by segment complexity showing that the slight increase in Dt-Dp in the second tertile was mostly associated with simple, and not complex, segmentectomy.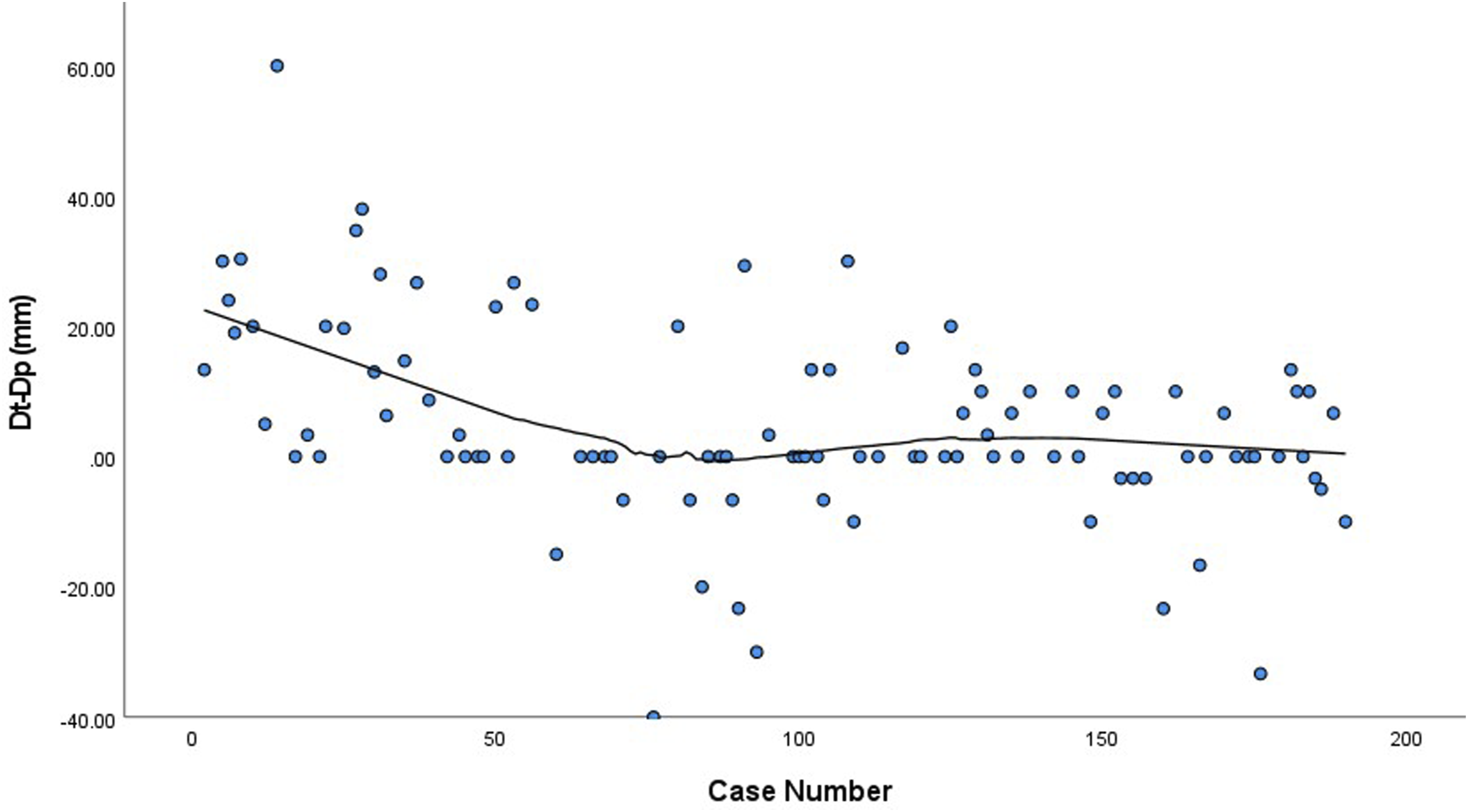
Discussion
Other fields have investigated the clinical benefits of NIF and found that NIF with ICG dye: is a useful tool for the laparoscopic treatment of some benign gynecologic conditions 10 ; increases nodal yield during laparoscopic distal gastrectomy for gastric cancer 11 ; potentially offers better short-term renal functional outcomes after robotic-assisted partial nephrectomy 12 ; and improves detection of hepatic, LN, and peritoneal metastases in colorectal cancer patients which may allow for better staging and more complete surgical resection. 13
Segmentectomy for lung cancer is difficult to perform because of the high level of dissection into the lung parenchyma required to isolate the diseased segment, and the lack of visible pulmonary intersegmental planes. Furthermore, variations in segmental anatomy add a layer of complexity to the operation.14,15 In previous work, we had demonstrated that NIF-mapping with intravenous ICG injection for robotic segmental resection was safe, feasible, and reproducible, and that it was also associated with an increased oncological margin distance from the tumor to the staple line. 5 In follow-up, the aim of this study was to examine the utility of NIF-mapping with ICG injection during robotic-assisted segmentectomy beyond the learning period, as more cases are performed and surgeon experience is acquired. To our knowledge, this is the first study to report on this. We determined that NIF-mapping with ICG injection increased the oncological margin distance from the tumor to the staple line, however, this distance diminished significantly across all tertiles. This is likely because the added benefit of NIF-mapping with ICG diminishes with greater surgeon experience. We also found that the clinical utility of NIF-mapping with ICG diminished after 42 cases with ICG, demonstrating that surgeon experience is likely associated with an improved ability in accurately and consistently identifying the invisible pulmonary intersegmental plane without ICG injection and NIF-mapping.
One of the apparent caveats in segmentectomy are patients requiring complex resections, and the debates to perform segmentectomy or lobectomy in these cases remain ongoing. 16 In this study, the first 2 complex resections of the right upper lobe were included on the 43rd and 65th cases. In these 2 cases, ICG could not be used due to difficulties in vascular isolation of the target segment. On the 85th case, later in tertile 2, the first successful right upper complex segmentectomy with ICG was performed with adequate intersegmental plane prediction. In approximately half of unsuccessful right upper lobe segmental resections, ligation of the corresponding pulmonary veins proved difficult, which prompted an intraoperative switch to lobectomy or wedge resection to complete the operation. This finding points to the potential value of preoperative planning and intraoperative utility of three-dimensional reconstruction technology for right upper lobe and other complex segmental resections. 17
A noticeable finding in our study is the reproducible utility of ICG for simple resections of the superior segment (S6) in both the left and right lung. In this subset, ICG corrected the surgeon’s estimate of the intersegmental plane by nearly a centimeter, and its added utility persisted for these tumours even after proficiency was achieved. This may have been observed due to the inherently simple nature of this resection procedure, leaving minimal clues for surgeons to accurately locate the intersegmental plane and ensure adequate margins. Since correct identification and dissection of pulmonary veins is far simpler in S6 resections, evidenced by a high success rate of these cases in our sample, it appeared that ICG injection may be sufficient on its own as an intraoperative adjunct. Overall, simple cases benefited most from NIF-mapping across our study period, and its added benefit persisted to a certain degree after the learning curve was overcome.
Our study is strengthened by its large sample size and reproducibility. We also present a modification of the 7-item rating scale to objectify the clinical value of ICG solely to when it increases the oncological margin length from the tumour. This instrument allowed us to fully capture the added benefit of NIF-mapping with respect to segment complexity, highlighting areas where technological advancements and imaging techniques could improve our ability to plan and perform segmental resections.
There are limitations to be addressed. Primarily, this study reflects a single-surgeon experience, potentially limiting the generalizability of our findings to other surgeons seeking to train in segmentectomy. The specific number of cases to achieve proficiency in robotic segmental resection ranges between 25-49 cases.6,18,19 While our study does highlight the presence of a learning curve, a more rigorous analysis for segmentectomy may be helpful to determine the utility of ICG as an educational tool. Our study also lacked a control group and had a short follow-up duration, preventing cost-utility analyses.
In our single-surgeon experience with robotic segmentectomy for lung cancer, the added value of NIF-mapping with ICG diminishes with surgeon experience. NIF-guided mapping is a useful tool early in surgical experience. Future studies may also highlight the potential benefit of ICG as an educational tool for teaching segmentectomy to surgical trainees.
Footnotes
Acknowledgement
Honourable mention to Jacob Alaichi, MSc., for his assistance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Waël C. Hanna is on the Advisory Board and Speakers Bureau for Astra Zeneca; Data Safety Monitoring Committee for Roche/Genentech; and Speakers Bureau for Minogue Medical. He also received Grant Funding from Intuitive Surgical. Drs. Marko Simunovic and Forough Farrokhyar and Ms. Yogita S. Patel have no conflicts of interest or financial ties to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Intuitive Surgical (Clinical Research Grant).
IRB Approval
The trial was reviewed and given approval by the Hamilton Integrated Research Ethics Board (HiREB), Project #0101.
Informed Patient Consent
Informed patient consent was obtained.
Meeting Presentation
Conference: 2022 The Society of Thoracic Surgeons (STS) 58th Annual Meeting. Location: National Virtual Event Dates: January 29-30, 2022
Central Picture Legend
Added benefit of indocyanine green dye diminishes with surgeon experience.
Central Message
In our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added benefit of near-infrared-mapping with indocyanine green dye diminishes with surgeon experience.
Perspective Statement
This trial demonstrates that in our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added benefit of near-infrared-mapping with indocyanine green dye diminishes as the surgeon gains experience, suggesting that this technique may be a useful learning and training tool for thoracic surgeons early on in their career to gain proficiency in performing segmentectomies.