
Abstract
Background
In recent years, numerous innovative yet challenging surgeries, such as minimally invasive procedures, have introduced an overwhelming amount of new technologies, increasing the cognitive load for surgeons and potentially diluting their attention. Cognitive support technologies (CSTs) have been in development to reduce surgeons’ cognitive load and minimize errors. Despite its huge demands, it still lacks a systematic review.
Methods
Literature was searched up until May 21st, 2021. Pubmed, Web of Science, and IEEExplore. Studies that aimed at reducing the cognitive load of surgeons were included. Additionally, studies that contained an experimental trial with real patients and real surgeons were prioritized, although phantom and animal studies were also included. Major outcomes that were assessed included surgical error, anatomical localization accuracy, total procedural time, and patient outcome.
Results
A total of 37 studies were included. Overall, the implementation of CSTs had better surgical performance than the traditional methods. Most studies reported decreased error rate and increased efficiency. In terms of accuracy, most CSTs had over 90% accuracy in identifying anatomical markers with an error margin below 5 mm. Most studies reported a decrease in surgical time, although some were statistically insignificant.
Discussion
CSTs have been shown to reduce the mental workload of surgeons. However, the limited ergonomic design of current CSTs has hindered their widespread use in the clinical setting. Overall, more clinical data on actual patients is needed to provide concrete evidence before the ubiquitous implementation of CSTs.
Introduction
Modern surgery has come a long way. From the first successful open surgery to the laparoscopic and robotic-assisted procedures standard in today’s operating room, the success of modern surgery is no anomaly; it is deeply entwined with the development of surgical technology. Ranging from aseptic techniques to intra-operative imaging, technology has always been an effective support for surgeons. 1 Novel surgical procedures such as minimally invasive surgery (MIS) also benefit the patients, as it is often associated with lower patient morbidity, infection, and a shorter hospital stay.2-4 However, it is important to highlight that surgical techniques today have increased in complexity compared to previous decades. Procedures like endoscopic or laparoscopic surgery have restricted the surgeon’s visual field to 2-D instead of the traditional 3-D view in open surgeries. The disparity in the visual field introduces problems such as image-reality incompatibility, loss of depth perception, and abnormal haptic feedback; additionally, novel surgical techniques also require new machines to be introduced to the operating room (OR), which may lead to extra staff to monitor the devices. The mental strain caused by MIS and excessive signals present in the working environment of the surgeon may lead to cognitive overload, which causes surgeon performance to decrease 5 ; this induces surgical errors while also extending operational time.6,7 Another potential cause to surgical errors involves communication. Irrelevant conversations within the OR are associated with poorer team collaboration and performance,8,9 while also extending operational time; equipment-related distractions is associated with higher stress and cognitive load. 8 Compared to open surgery, communication in MIS is more unclear and more frequently directed at equipment instead of the procedure, likely due to the increased equipment and staff used to support the MIS. 10 . Parker et al 11 reported a longer duration of open transforaminal lumbar interbody fusion surgery when comparing MIS to standard open surgery. Experiments that mimicked both MIS and open surgery environments reported a decreased efficiency in task completion and an increased mental workload. 12 Accompanying the increased cognitive load are increased probability of adverse events. In the top 559 hospitals located in the US, close to 81.7% of intraoperative errors are related to surgeons’ cognition being overwhelmed, each offense could cause up to 125,000$ in penalty. Thus, fatigue-related events, such as retained foreign objects or wrong surgical sites would be significantly reduced if surgeons received cognitive support. 13 To counteract the increased cognitive load of surgeons and to reduce surgical errors, cognitive support technology (CST) has developed since the early 2000s and has seen significant growth in recent years to aid the decision-making of physicians and surgeons. However, despite its importance, technology in this field lacks a systematic review and assessment of the impacts on surgical performance. We aim to review the current status and trends of CST in surgery. CSTs covered in this review pertains to information presentation for diagnostic support and visualization for enhancing performance. Specifically, we include the software and hardware employed for data presentation, analysis in surgery, and impact on surgeon performance and patient outcome.
Method
Search Criteria
The inclusion criteria include a list of terms that can be categorized into three major groups: cognitive support, surgery, and digital reality. A figure of an example search in PubMed is provided. Related terms are connected with Boolean operators; terms in a column are connected with the “OR” operator, while terms in a row are connected with the “AND” operator (Figure 1). A CST is a technology that reaches a high level of innovation and technological complexity, often involving programming or robotic design aimed at reducing cognitive load of surgeons. Exclusion criteria were set to be checklist articles because an overwhelming number of checklists was included in the literature search. In this review, a checklist defined as a digital or non-digital element used to verify aspects of the surgery in the OR. Surgical checklists were often specific to a large variety of surgeries which required a large amount of background information. There were also additional checklists assessing other checklists which were too complicated for the purpose of this review. Literature included in this review was gathered through a literature search in medical databases, including the Web of Science, PubMed, and IEEExplore, articles published until May 21, 2021 were included. An effort was made to search for clinical trials or randomized controlled trials, but a few exceptional model and architectural articles are included to provide a framework understanding of the topic. The article search and selection process was completed by a single reviewer (ZSZ). Mendeley reference manager (Relx, New York, USA) was used to organize the references. Studies were included in this review if it targeted the peri-operative phase in surgery, contained the development software or device that aimed to reduce surgeons’ cognitive load, and experimental trials that assessed the efficacy of the technology. Studies that only included a phantom trial, an animal trial, or used synthetic patients were included. Articles were first screened by title and abstract assessments. The remaining articles then underwent full-text analysis to further evaluate relevant articles. Advance search criteria for PubMed.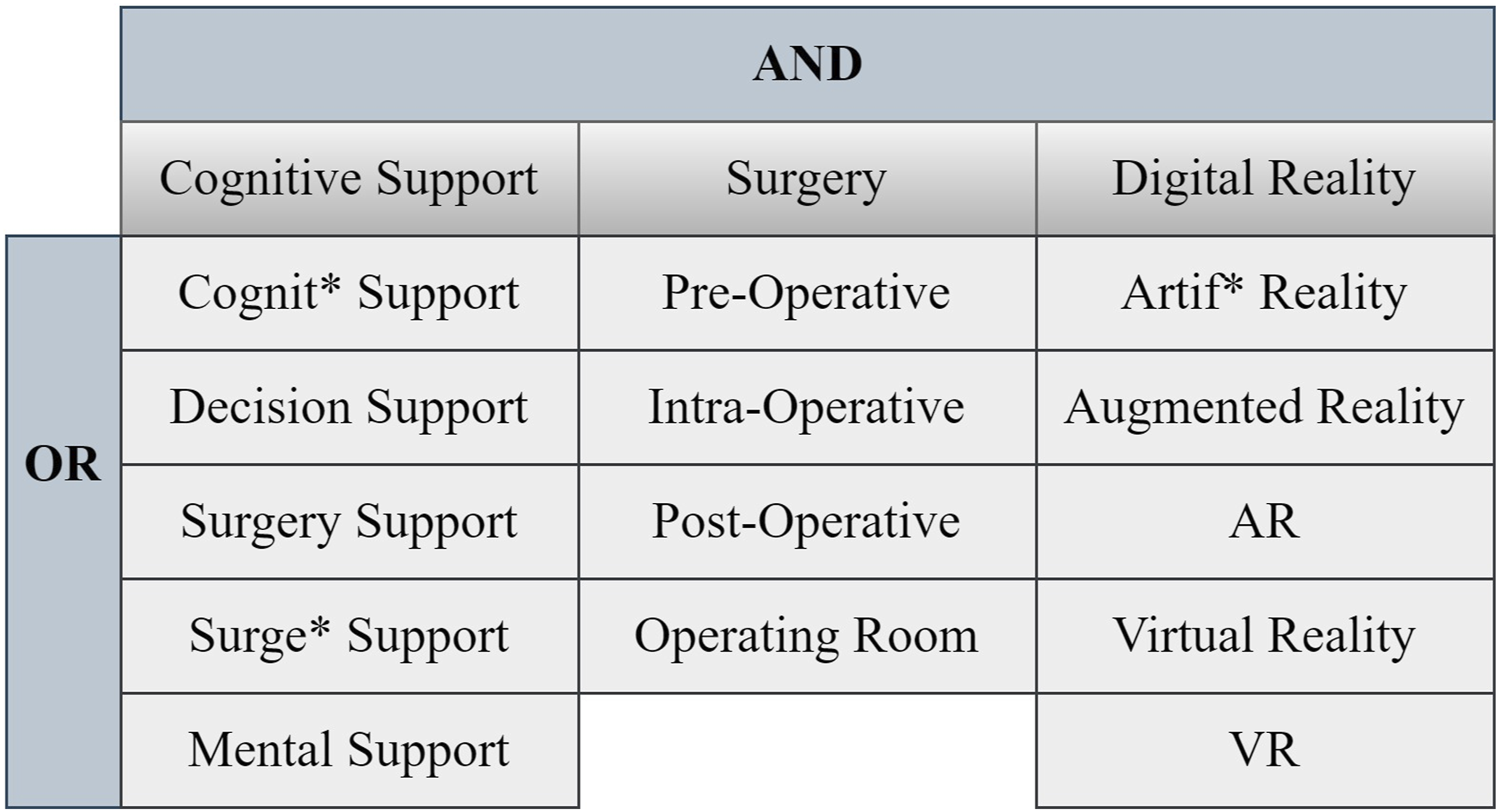
Data Analysis
A single reviewer (ZSZ) examined key characteristics of each article including data source, development status, experiment type, sample size, phase of surgery, and the type of procedure. Full-text articles selected were organized with Microsoft Excel (Microsoft Corporation, WA, USA). Papers were further stratified into different subgroups by the parameters they measured; clinical outcomes, patient outcomes, and OR time variations were all taken into consideration. Discussion of the advantages and disadvantages of CSTs were gathered from the discussion and conclusion of the articles. Interpretation of the study results was based on the result section of each paper. A secondary reviewer (YW) verified the accuracy of the content. In events where the article cannot be classified into a set group, or parameters on the article was unclear, then a discussion was to occur with two other reviewers (BZ, WL) until an agreement was made.
Results
Overall, 481 citations were found throughout the literature search; after electronically removing 22 duplicates using Endnote (Clarivate, London), 459 remaining articles underwent further screening. Two independent reviewers (ZSZ, LW) screened the citations based on title and abstract, 369 articles were removed, leaving 35 for full-text review. During full-text review, 14 articles were removed: seven lacked quantitative data; six were overview articles; one was a checklist. An additional 19 articles were found through relevant searching, summing the total number of articles included in this review to be 40 articles. Each article had at least one relevant data describing cognitive load reduction. The complete article evaluation process is outlined as Figure 2. Flow chat of the article selection process.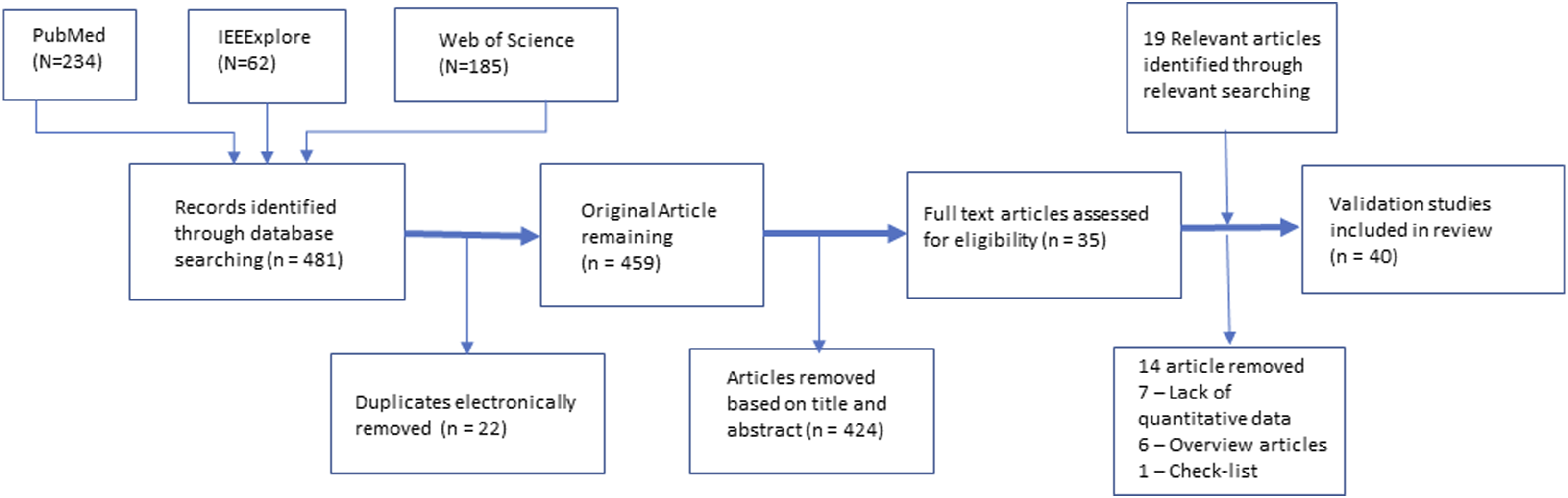
Data Source
Characteristics of Included Studies.
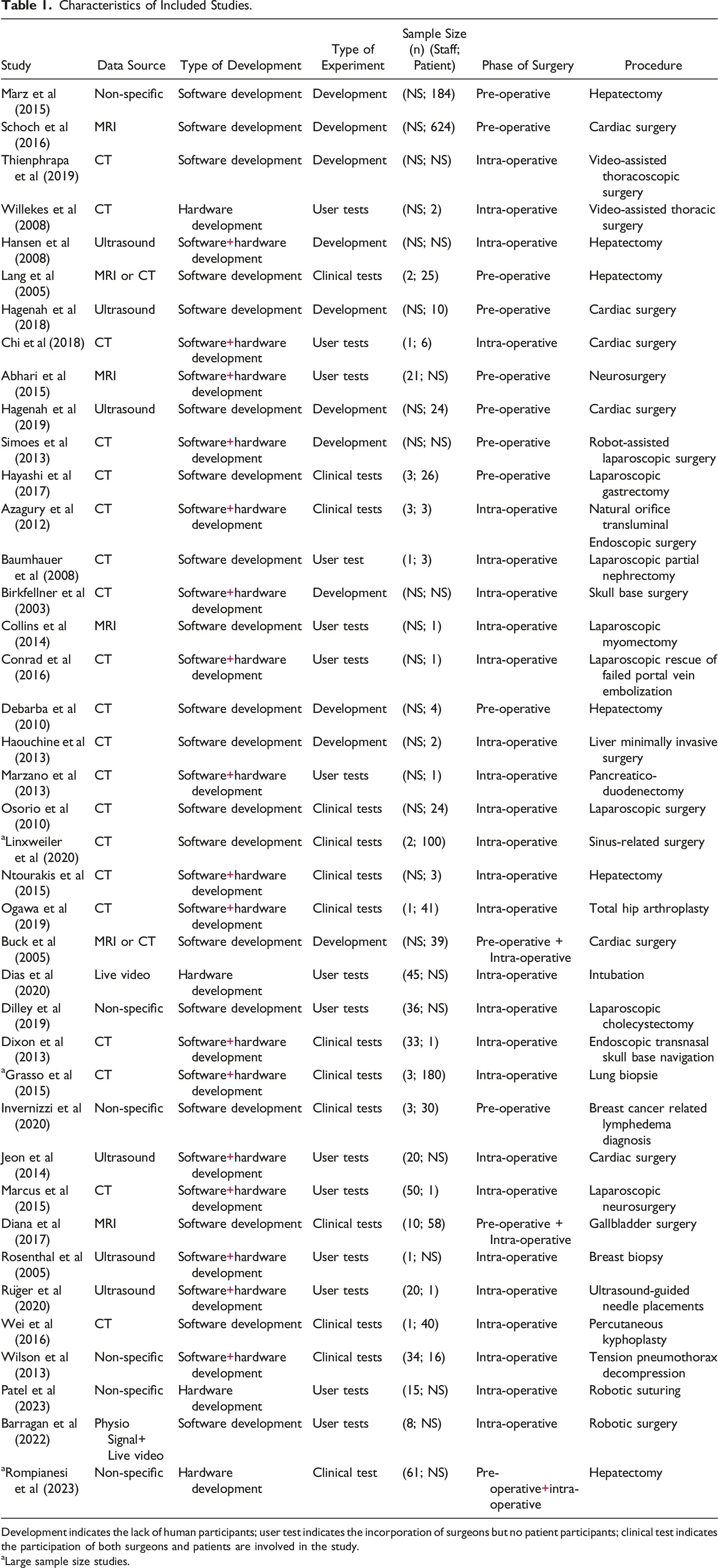
Development indicates the lack of human participants; user test indicates the incorporation of surgeons but no patient participants; clinical test indicates the participation of both surgeons and patients are involved in the study.
aLarge sample size studies.
Phase of Surgery
Different CSTs act on three main phases of surgery: preoperative, intraoperative, and post-operative. Preoperative includes all planning activities before the onset of the surgery; intraoperative refers to surgical performance during an operation. CSTs categorized to the different phases of surgery act as interventions or visual assistance to the surgeon. 12 (32%) CSTs are responsible for preoperative interventions and 27 (73%) CSTs are responsible for intraoperative interventions. No CST was found to assist in patient rehabilitation after the surgery had been completed.
Types of Surgery
CSTs are present in a wide variety of procedures. General surgery, thoracic surgery, neurosurgery, urology surgery, otolaryngology surgery (ENT), and orthopedic surgery are all applicable for CST use. While it is difficult to categorize them into specific groups, it is certainly clear that there is an emphasis on MIS (n = 11) (Table 1).
Surgical Performance Outcome
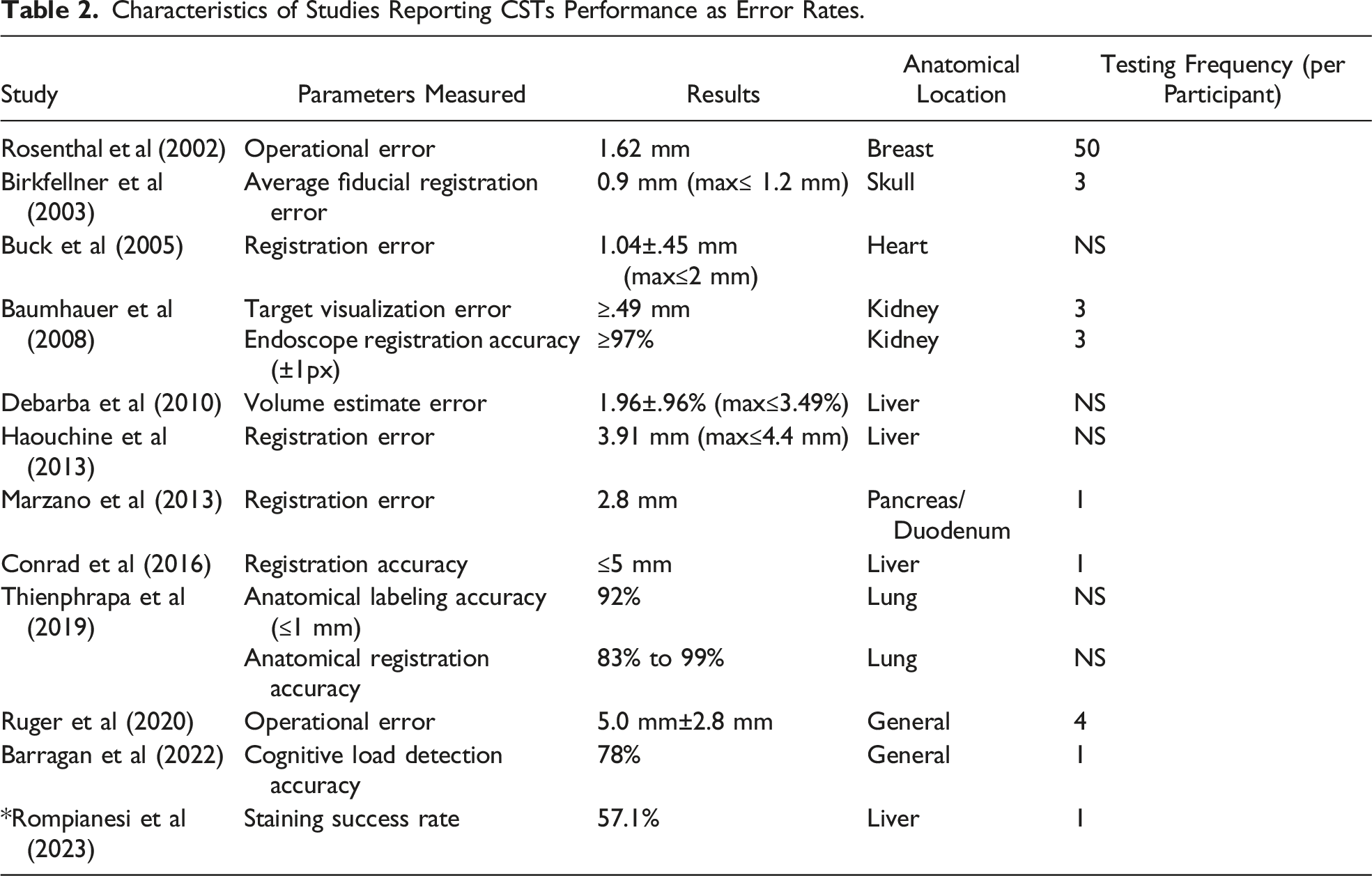
Characteristics of Studies Reporting CSTs Performance as Error Rates.
Characteristics of Studies Reporting Surgeons’ Performances With the Employment of CSTs.
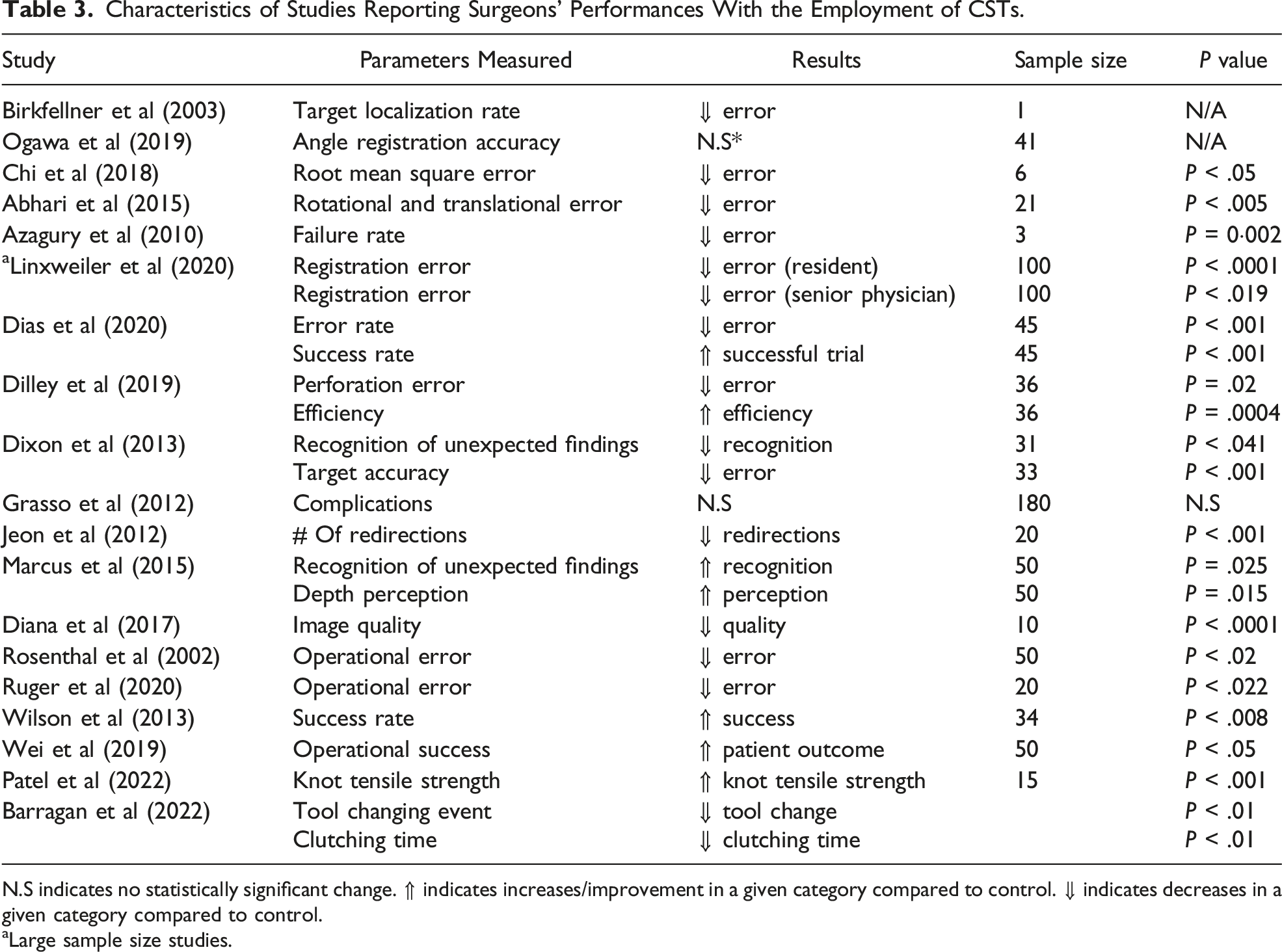
N.S indicates no statistically significant change. ⇑ indicates increases/improvement in a given category compared to control. ⇓ indicates decreases in a given category compared to control.
aLarge sample size studies.
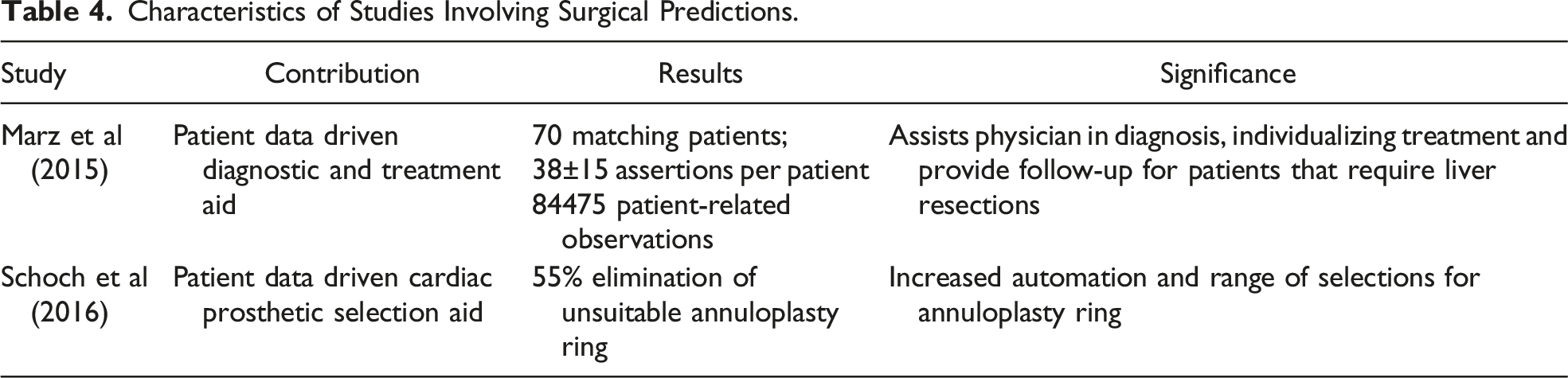
Characteristics of Studies Involving Surgical Predictions.
Patient Outcome
Characteristics of Studies Reporting Patients’ Outcomes With the Employment of CSTs.
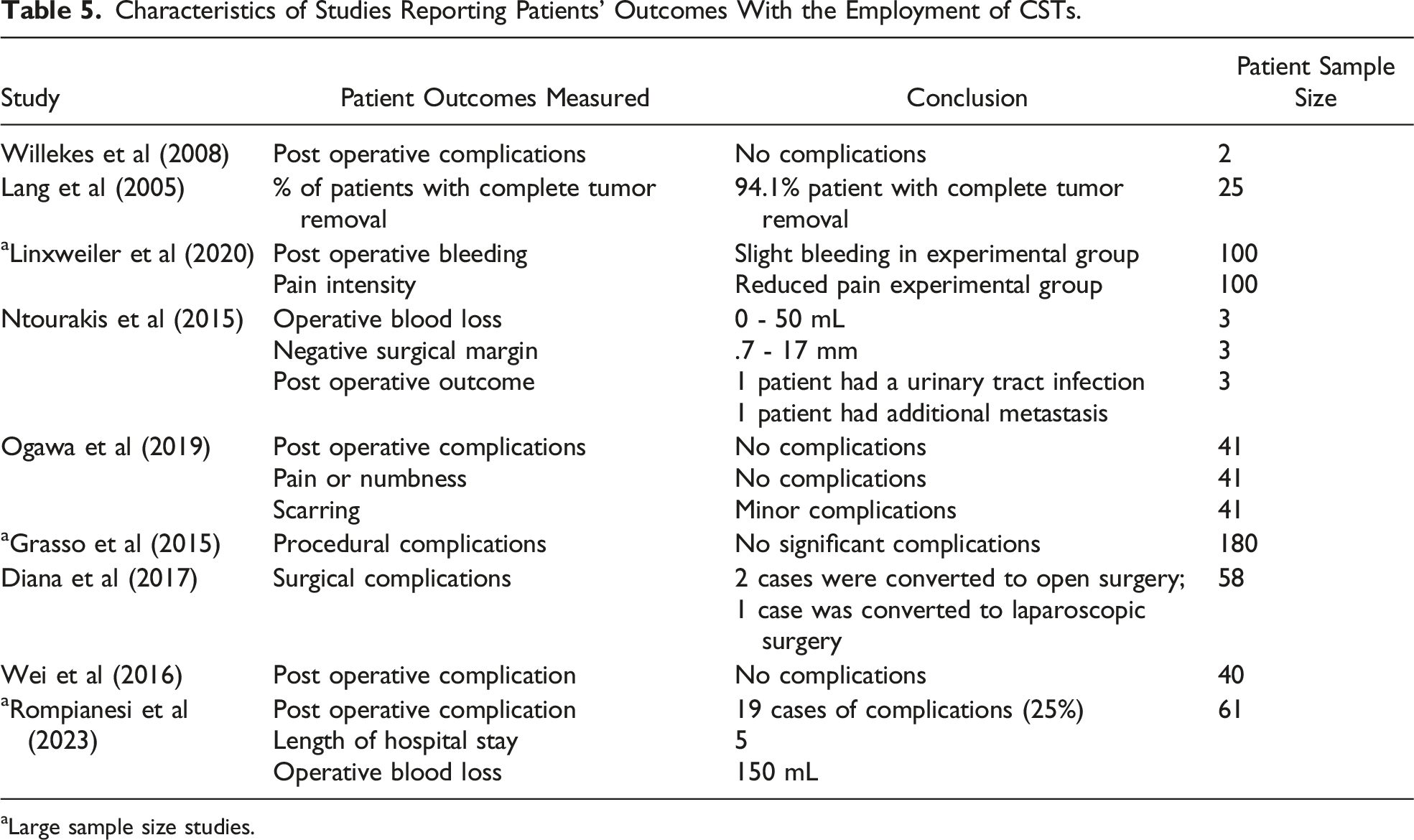
aLarge sample size studies.
OR Time Variation
Characteristics of Studies Reporting Operation Time Changes With the Employment of CSTs.
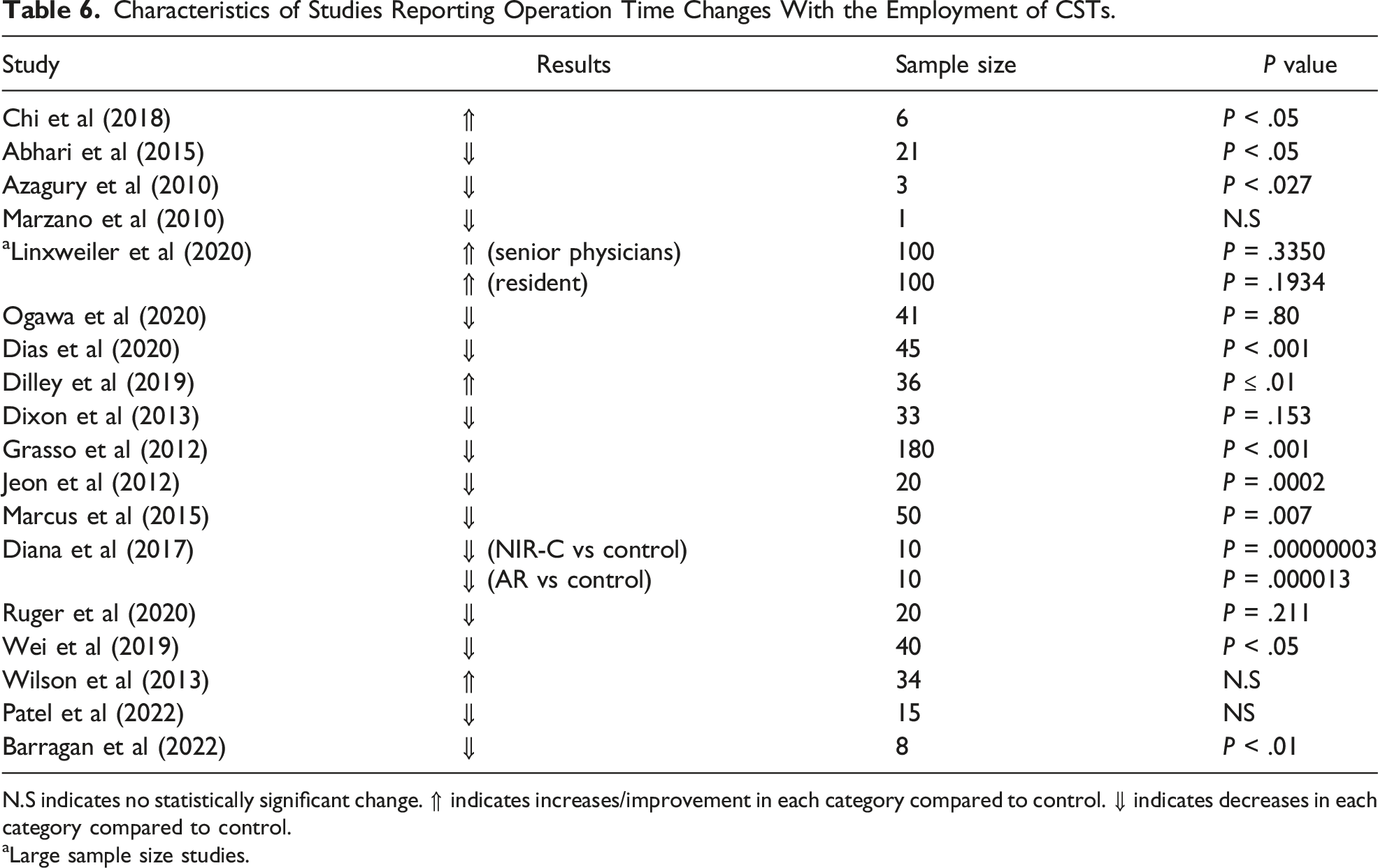
N.S indicates no statistically significant change. ⇑ indicates increases/improvement in each category compared to control. ⇓ indicates decreases in each category compared to control.
aLarge sample size studies.
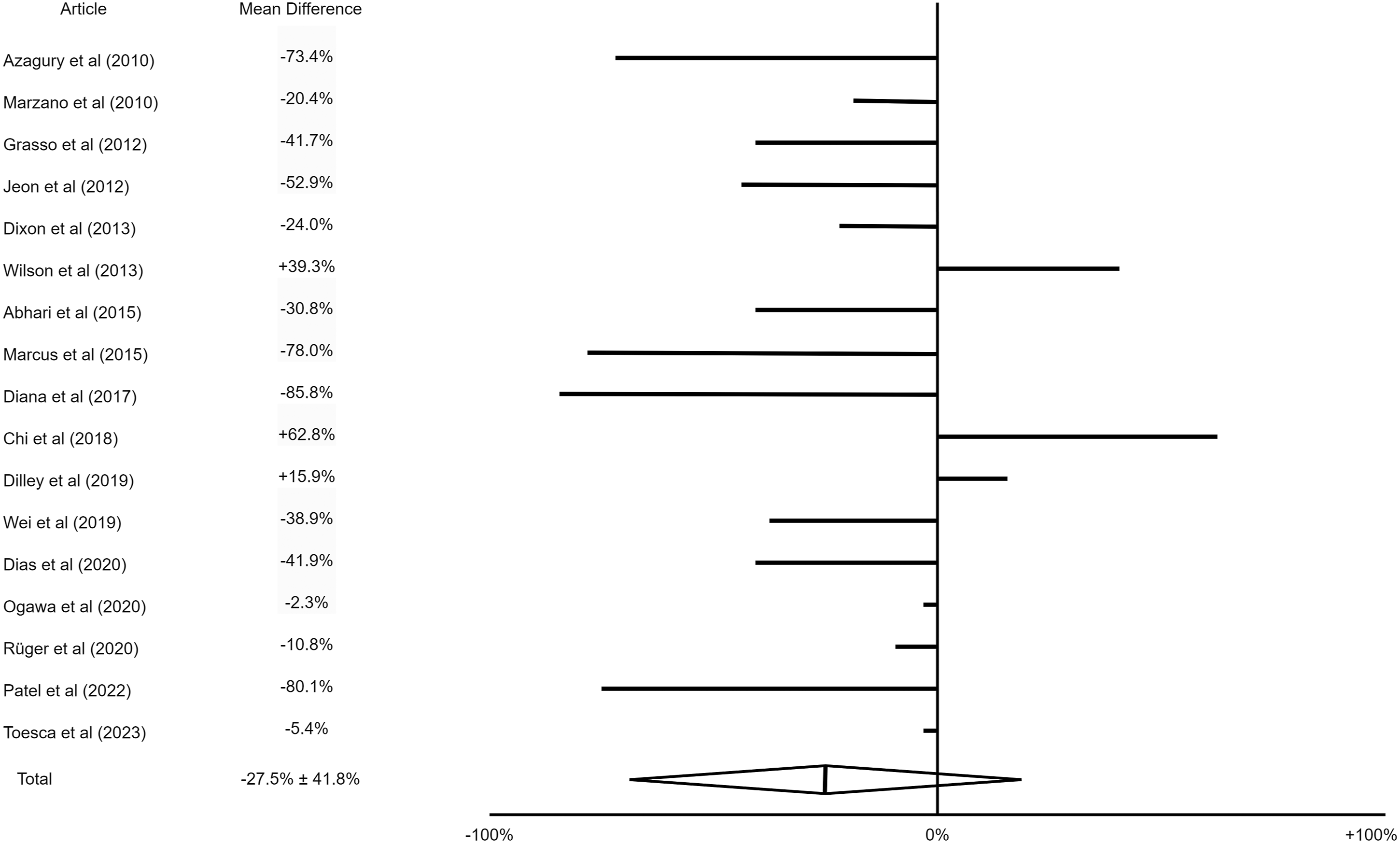
Procedure duration change with the implementation of CSTs.
Discussion
Medical imaging such as X-rays, CT scans, MRIs, and ultrasound data are widely used in surgical planning and intraoperative guidance. Augmented or mixed reality technologies utilize these images to create visual 3-D models for visual enhancement. However, tissue deformation during surgery can cause inaccuracies in these models. In actual surgery, target registrations are primarily done during the end-exhalation plateau phase of the patient’s respiratory cycle to ensure accurate markers for anatomical structures. 26 The margin of error for surgery registration ranges from 1 mm to 15 mm.27,28
Most CSTs are developed for specific types of surgeries, such as hepatic (ablation) cardiac surgery, vascular surgery with cannulation and catheterization technologies, laparoscopic surgery, lung surgery, and arthroplasty. One of the most important functions of CSTs for surgeons is visual assistance. Clinically, one of the procedures that considerably benefit from visual aid is liver resection, because portal blood vessels may be difficult to visualize under the liver, residual liver volume is hard to estimate, and there may be hidden tumours that are not detected initially.25,26,29,30 Patient-specific virtual reality anatomical models may be built through preoperative or intra-operative images depending on data availability.26,30,31 During planning, surgeons may freely rotate the model to detect unexpected tumours and adjust the resection plane accordingly; based on the resection plane, the software returns the residual liver volume as well as security margins around the liver for surgeons to analyze the validity of the plan.26,30 Patient-specific digital models can be generated to support valve replacement in heart surgeries.32,33 Trajectory optimization done by machine learning can reduce the risks in cannulation and catheterization procedures. 34 In laparoscopic gastrectomy, CSTs serve to recommend ideal port locations for increased tool maneuverability. 35 Current CSTs developed for lung biopsy assist the operator by providing a real-time augmented reality video displaying the position of the needle and surrounding tissue. 19 Regardless of the type of operation, CSTs aim to reduce surgeons' cognitive load and decrease surgical complications. Preoperative and intra-operative cognitive support technologies (CSTs) have been developed to reduce the cognitive load of surgeons during surgical procedures. Preoperative CSTs simplify anatomical complexities, aid in prosthetic selection, and provide visualization; the major intended role of preoperative CSTs is to aid the surgeon accurately and efficiently in patient diagnosis and surgical planning. For example, in mitral valve replacement surgery, an algorithm was created to reduce commercial mitral valve options based on patient-specific heart dimensions and medical history. 14 In neurosurgery planning, a CST was developed to create a dynamic 3D model of a patient's brain and pathology, providing recommendations for surgical procedures.22,36 CSTs should progress from cognitive support for individual surgeons to support for the entire surgical team, utilizing virtual and augmented reality to improve communication and decision-making efficiency. During the intraoperative phase, the consequences of overloading the surgeon’s cognition are often more serious, leading to poorer adverse patient outcomes. Intraoperative cognitive overload primarily comes from visual disturbances, unexpected events, and variable environmental factors.24,37-39 Thus, the primary role of intraoperative CSTs is to alleviate these problems and to stabilize the surgeon’s cognitive workload. , For example, to address the problem of intraoperative visual disturbances in endoscopic-related surgeries, CSTs that provide a 3D visualization of an endoscope tip and software that allows for navigation aids were often prioritized; this type of assistance is especially beneficial for surgeries that contain a trans-nasal component because navigation is difficult in this subset of surgeries.24,37,38 In variable and intense environments like the battlefield, Auditory guidance headsets with micro-speaker have been developed to treat needle decompression of tension pneumothoraxes for combat medics. 39 Robotic innovations like the Da Vinci robot and the Xi robot are being implemented in an increasing amount of surgical specialties. Innovations in surgical robotics have shown to improve motion stability and decrease tissue destruction.40,41 Simple CSTs, such as tattooing with methylene markers, have also been developed to aid in target localization. 42 Robotic surgery can also be combined with intraoperative fluorescent markers to provide surgeons with improved visualization of the anatomical structures around the resection plane and tumour location. 43 To assess the cognition levels of surgeons during robotic surgery, machine learning-based CSTs are able to analyze physiological parameters such as electroencephalogram and eye behaviour to detect moments of high cognitive load; in response to cognitive overload, the semi-autonomous program may take control of simple tasks such as blood suction and irrigation. 44 More invasive neurostimulation techniques were also tested; transcranial direct current stimulation on surgeons completing a knot typing task in robotic surgery was reported to have increased knot tensile strength. 45 Cognitive surgical technologies (CSTs) incorporating augmented reality (AR) and image guidance have shown promising results in improving precision and reducing errors in various surgical procedures. Similar to other visual aid CSTs, AR-based CSTs also rely on radiology images to create a patient-specific 3-D model. Intraoperatively, anatomical landmarks around the surgical site and security margin are labelled to the surgeons to aid their incisions; clarifications are given to surgeons around complex anatomical regions, and some CSTs provide procedural instruction during the operation. Studies have reported increased accuracy rates in AR or voice-guided surgery, with decreased error rates of up to 10%.15,16,24,27,34,36,37,46,47 AR-based CSTs have been effective in treating hepatocellular carcinoma, neonatal intubation, laparoscopic nephrectomy, and needle biopsies, resulting in increased success rates and reduced error rates.15,19,29,48 However, in some procedures like total hip arthroplasty and breast cancer-related lymphedema diagnoses, the implementation of CSTs did not result in significant differences.18,49 The presence of CST may also influence procedure time, with increased distraction or unfamiliarity with the device potentially reducing efficiency.24,34,39,46 However, there is insufficient evidence available on intraoperative CSTs to support the conclusion that it significantly lowers cognitive load and boosts performance, future research should focus on this area. With more development, CSTs may be crucial in reducing the cognitive load of surgeons during surgical procedures, improving communication and decision-making efficiency, and ensuring patient safety. The development of CSTs should continue to focus on reducing procedure complexity, reducing error rates, and aiding intraoperative decision-making to improve surgical outcomes. Current CSTs have limitations that hinder their widespread use in the OR. One major problem is the inadequacy of existing VR and AR technology to handle tissue deformation and organ fluctuation, requiring the intervention of expert computer scientists during surgery.25,28,38 Additionally, there is a lack of randomized controlled trials and sufficient clinical data due to the disconnection between medical staff and computer scientists, leading to outsourcing clinical trials to actual hospitals after CST development. Furthermore, CSTs often lack ergonomic design for effective surgical implementation, affecting navigation, reducing the field of view, and other ergonomics-related problems.16,36 Surgeons also have a preference for traditional techniques, and CSTs are often expensive, limiting their use in routine procedures. Learning curve problems and the potential for attentional blindness also pose challenges to CST use. CSTs may be more suitable for complex procedures requiring cognitive assistance, and future development should prioritize ergonomic design to improve usability and maneuverability. Overall, CSTs require further research and development to improve their effectiveness and gain wider acceptance in the ORs.
Conclusion
This review suggests that CSTs have shown promising results in improving surgical performance and reducing errors by increasing surgeons' visual fields. CSTs are currently in development for a wide variety of surgery specialties, and its purpose are often multi-dimensional, aiding surgeons in different areas before and during the procedure. Some advantages of CST, such as accuracy-based parameters, are supported with more evidence than other. However, several challenges still need to be addressed, including inaccuracies in accounting for tissue deformation, a lack of clinical data, particularly patient data, and ergonomic issues with bulky equipment. When developing these CSTs, adequate consideration must also be given to the possibility that the addition of CSTs would fatigue the surgical operator and cause them to regress in performance. Despite these limitations, the potential benefits of CSTs make them a promising area for further development and research, in today’s innovative age, improvements in hardware, software and design could overcome these technological challenges, furthering improving the medical field with interdisciplinary efforts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Zhong Shi Zhang has been funded by Alberta Innovate Summer Studentship for this research.