
Abstract
Background
Breast-conserving surgery combined with oncoplastic breast surgery has become the standard surgical treatment for early breast cancer.
Objective
The purpose of this study was to investigate the safety and efficacy of the thoracodorsal artery perforator flap (TDAPF) in breast-conserving reconstruction of T2 breast cancer.
Methods
Thirty patients with T2 breast cancer admitted to our hospital from January 2019 to December 2020 were enrolled to receive pedicled TDAPF for repairing breast defects after breast-conserving surgery. Intraoperative conditions, postoperative complications, and shape satisfaction after breast reconstruction were recorded.
Results
The operation was successfully completed in all 30 patients, with an operation time of 177.77 ± 24.39 min, bleeding of 44.17 ± 7.67 mL, and length of hospital stay of 5.23 ± .97 d. There was no deformity or seroma at the donor site. Breast shape recovered well after operation. After operation, one patient had fat liquefaction in the recipient site, which healed well after wound treatment. The incidence of postoperative complications was 3.33%. Postoperative follow-up lasted 16-28 months, with a median of 22 months. The Breast-Q score for breast satisfaction was 61.83 ± 12.87 at 6 months after operation, compared to 62.07 ± 11.78 before operation (P > .05).
Conclusions
TDAPF, featuring a high survival rate, moderate flap area, fewer postoperative complications, and high satisfaction with breast shape after operation. For east asian women with moderate breast size, TDAPF is a safe, effective choice for repairing defects in breast-conserving surgery for T2 breast cancer.
Introduction
Breast cancer is the most common cancer in women. The incidence and mortality of breast cancer in women worldwide were 46.3/105 and 13.0/105, respectively in 2018, both showing an increasing trend. 1 Although the incidence (36.1/105) and mortality (8.8/105) of breast cancer in Chinese women are relatively low, 2 with the economic development of China and the changes in people's lifestyle and diet, the incidence of breast cancer is increasing year by year. It is also showing a younger trend, seriously endangering the life and health of Chinese women. In recent years, with the improvement of imaging technology and the enhancement of people's health awareness, the proportion of early-detected breast cancer has gradually increased, and with it the breast-conserving rate has gone up.
Breast-conserving surgery has become the standard surgical treatment for early breast cancer, which is combined with adjuvant radiotherapy after operation. Although it has a slightly higher local recurrence rate than total mastectomy, their overall survival rates are similar. 3 In addition, it maintains the basic shape of the breast and improves the quality of life of patients. For T2 tumours (2 < longest diameter ≤5 cm), quadrantectomy can significantly reduce the local recurrence rate compared with extended resection. 4 In case of a large breast size, satisfactory breast shape can be obtained through remodelling by glandular flap displacement. However, East Asian women often have small and medium-sized breasts. 5 Bulstrode et al 6 concluded that when the amount of resected breast tissue is >20%, it is difficult to obtain satisfactory cosmetic results after breast-conserving surgery. Therefore, conventional breast-conserving surgery for T2 breast cancer will not yield a satisfactory breast shape, limiting its application.
With recent advancements in plastic surgery for breast cancer, the application of thoracodorsal artery perforator flap (TDAPF) has greatly expanded the indications of breast-conserving surgery, and has obvious advantages over traditional breast-conserving surgery in terms of safety and cosmetic results. This study investigated the safety and cosmetic results of TDAPF in breast-conserving surgery for T2 breast cancer.
Clinical Data and Methods
Clinical Data
Thirty patients with T2 breast cancer admitted to the Department of Breast Surgery of the Affiliated Hospital of Putian University from January 2019 to December 2020 were enrolled to receive pedicled TDAPF for repairing breast defects after breast-conserving surgery. Inclusion criteria: ① patients with invasive breast cancer (2 < longest diameter ≤5 cm) confirmed by core-needle biopsy or intraoperative rapid frozen pathological examination who were not receiving preoperative neoadjuvant chemotherapy; ②patients with indications for breast-conserving surgery; ③patients with breast defects that could be sufficiently repaired with TDAPF tissue (thickness of subcutaneous fat in the lateral chest wall >10 mm as measured by callipers). Exclusion criteria: ①patients with scar constitution; ②patients with expected breast resection>30%; ③patients combined with serious diseases of the heart, liver, kidney, or other organs; ④patients with a previous history of breast or chest wall radiotherapy; ⑤patients with distant tumour metastasis; ⑥patients with coagulation disorder or other surgical contraindications. All patients and their families were informed and signed the informed consent form, and the study was approved by the Ethics Committee of our hospital. All content and procedures described within conform to the principles out- lined in the Declaration of Helsinki.
Follow-Up
The median follow-up time was 22 months, ranging from 16 to 28 months. Routine follow-ups consisted of physical examinations, laboratory tests, chest radiography, and abdominal ultrasonography or CT scans. All patients were regularly followed-up through phone calls and outpatient services, and the final follow-up was conducted in May 2022. The primary endpoint of this study was perioperative (recent complications) evaluation, and the secondary endpoint was postoperative relative long-term evaluation (reconstructed breast morphology, recurrence rate).
Flap Design and Surgical Methods
Preoperative Surface Marking for Thoracodorsal Artery Perforator and Flap Design
The anterior border of the latissimus dorsi was marked while the patient was in the lateral decubitus position before operation. Bedside Doppler ultrasound was used to locate the thoracodorsal artery perforator, and 1-2 dominant perforators with a diameter ≥.5 mm were selected to mark the location of the perforator point. The distance between the flap and the lesion was assessed to ensure that the flap could be transferred tension-free to cover the wound surface.
Extent of tumour resection: Quadrantectomy was performed by removing the primary tumour plus at least 2 cm of normal tissue around the lesion. The shape and size of the flap were marked using the mapping method, with the extent of lesion resection as the template and the location of the perforator point as the pivot point (Figure 1). Preoperative marking. (A) Location of thoracodorsal artery perforator points detected by doppler ultrasound; (B): Preoperative flap design.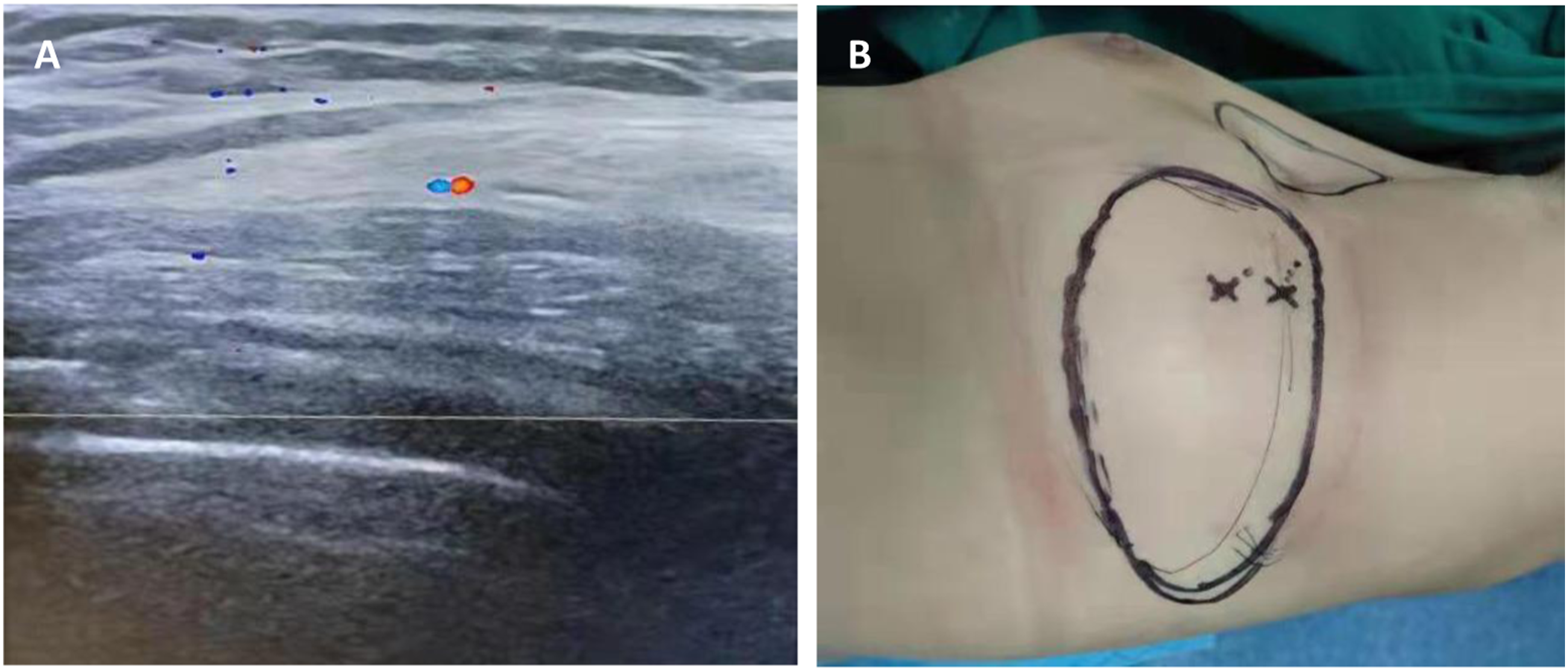
Surgical Methods
Recipient Site
An oval-shaped incision was made, including the puncture point of a hollow needle. With the line between the tumour centre and the apex of the nipple as the central axis, about 1/4 of the breast tissue was removed in a fan shape (Figure 2A). The resection range was the tumour plus >2 cm of tissue around the lesion, including the skin and the pectoralis major fascia. The upper, lower, inner, outer, and basal margins of the lesion were resected and sent for intraoperative rapid frozen pathological examination to ensure negative resection margins. Schematic diagram of operation process. (A) With the line between the tumour centre and the apex of the nipple as the central axis, about 1/4 of the breast tissue was removed in a fan shape; B): Expose the perforating vessels of thoracodorsal artery and complete the production of TDAPF; C): A subcutaneous tunnel between the donor site and the recipient site was cut, and the flap was transferred to the breast defect through the tunnel; D): Free the flaps at both ends of the donor site defect to reduce tension and directly suture the incision.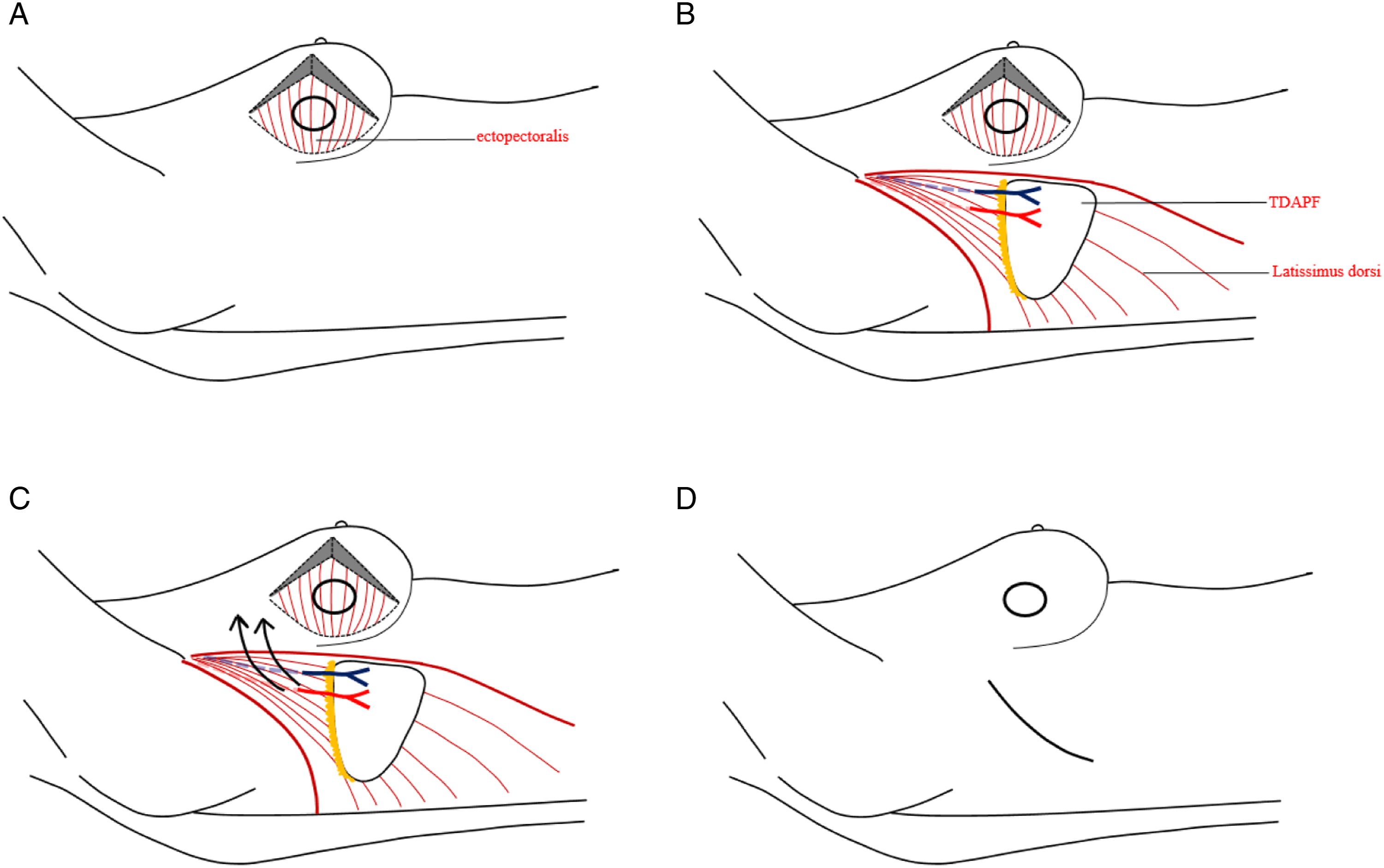
Donor Site
According to the shape of the flap designed preoperatively, an incision of 8-10 cm in length along the long axis of the flap was made. The skin and subcutaneous tissue were incised and dissected down to the superficial layer of the latissimus dorsi sarcolemma. The anterior edge of the latissimus dorsi was found along the level of the latissimus dorsi fascia, and Doppler ultrasound was used to locate the descending branch of the thoracodorsal artery, which was generally parallel to this edge, with a distance of ≤ 2-4 cm that was approximately identical to the distance between the proximal end of the perforator and the lateral border of the latissimus dorsi. Combined with the perforator location detected preoperatively by ultrasound, this allowed us to locate the perforator definitively (Figure 3A). At least two or more perforators were retained during the operation. The perforators were carefully separated from the latissimus dorsi, the muscles between the perforators should be separated, and a sufficiently long vascular pedicle should be retained (Figure 2B). Attention was paid to protect the nervus thoracodorsalis during operation. The flap was incised according to the preoperatively designed range. In the process of dissecting the flap and perforator, we paid attention to the blood supply of the flap. The flap could be lifted from the distal end to observe the blood supply of the distal end. The observation of continuous fresh bleeding was a good sign that the perforators were found correctly. In some cases, the transverse branch of the thoracodorsal artery could be ligated to increase the range of motion of the vascular pedicle. Intraoperative physical image of TDAPF reconstruction. (A) Exposed thoracodorsal artery perforator. Flap plasty; B): Reconstruction for repair (case1); C): When the skin in the recipient site is sufficient, the skin flap can be de-epidermal; D): Reconstruction for repair (case2).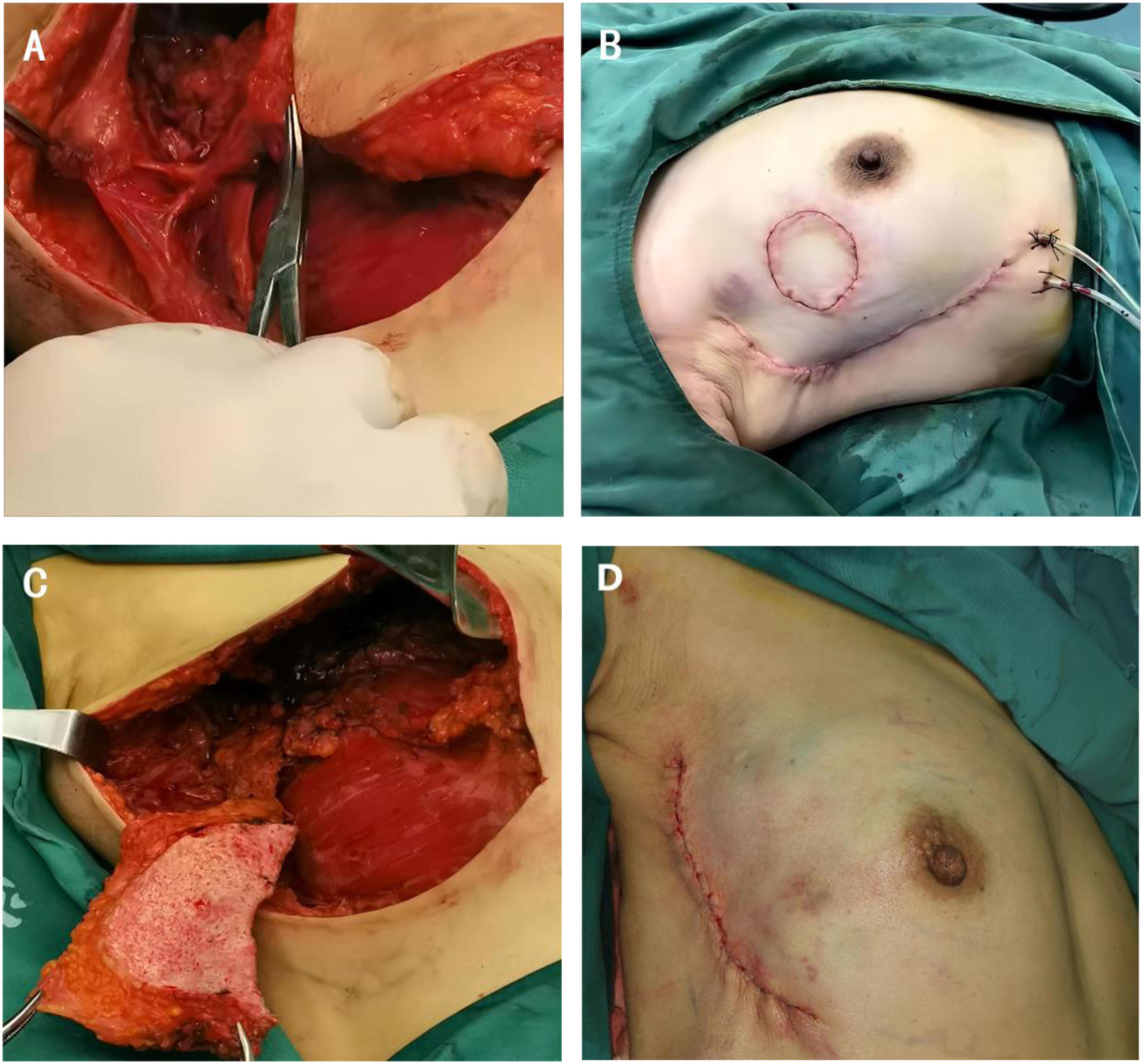
Repair
A subcutaneous tunnel between the donor site and the recipient site was cut, and the flap was transferred to the breast defect through the tunnel (Figure 2C). After TDAPF was transferred to the recipient area, was formed according to the size and shape of the defect, we retained the required area of the skin island, the excess skin of the flap was de-epidermalized and covered by normal breast skin in the recipient site. It was sutured with the breast tissue around the defect to ensure that the vascular pedicle had no torsion and tension. Tension to the flaps on both sides of the defect at the donor site was reduced for direct suture (Figures 2D and 3).
Treatment of Axillary Lymph Nodes
The same incision was used as was used at the donor site. Before removing the lesion and repairing, methylene blue tracing was performed for sentinel node biopsy. If the sentinel lymph node was positive, axillary lymph node dissection was performed.
Observations Indicators
The operation time, intraoperative bleeding, postoperative indwelling time of drainage tubes, postoperative length of hospital stay, and incidence of postoperative complications were recorded. The questionnaire BREAST-Q BCT V2.0 Chinese CN was employed to assess the health-related quality of life of each patient.
Statistical Methods
The BREAST-Q (copyright of Memorial Sloan Kettering Cancer Center and The University of British Columbia) was used to analyze QOL. Raw data were converted to a “Q-score” ranging from 0 to 100. A high score corresponded to a high health-related QOL. Data were processed with SPSS Statistics V22.0 and are expressed as ‾x ± s. The paired t test compared the two time points within the group. P < .05 indicated that a difference was statistically significant.
Results
Clinical Baseline Characteristics and Surgical results of Included Patients.
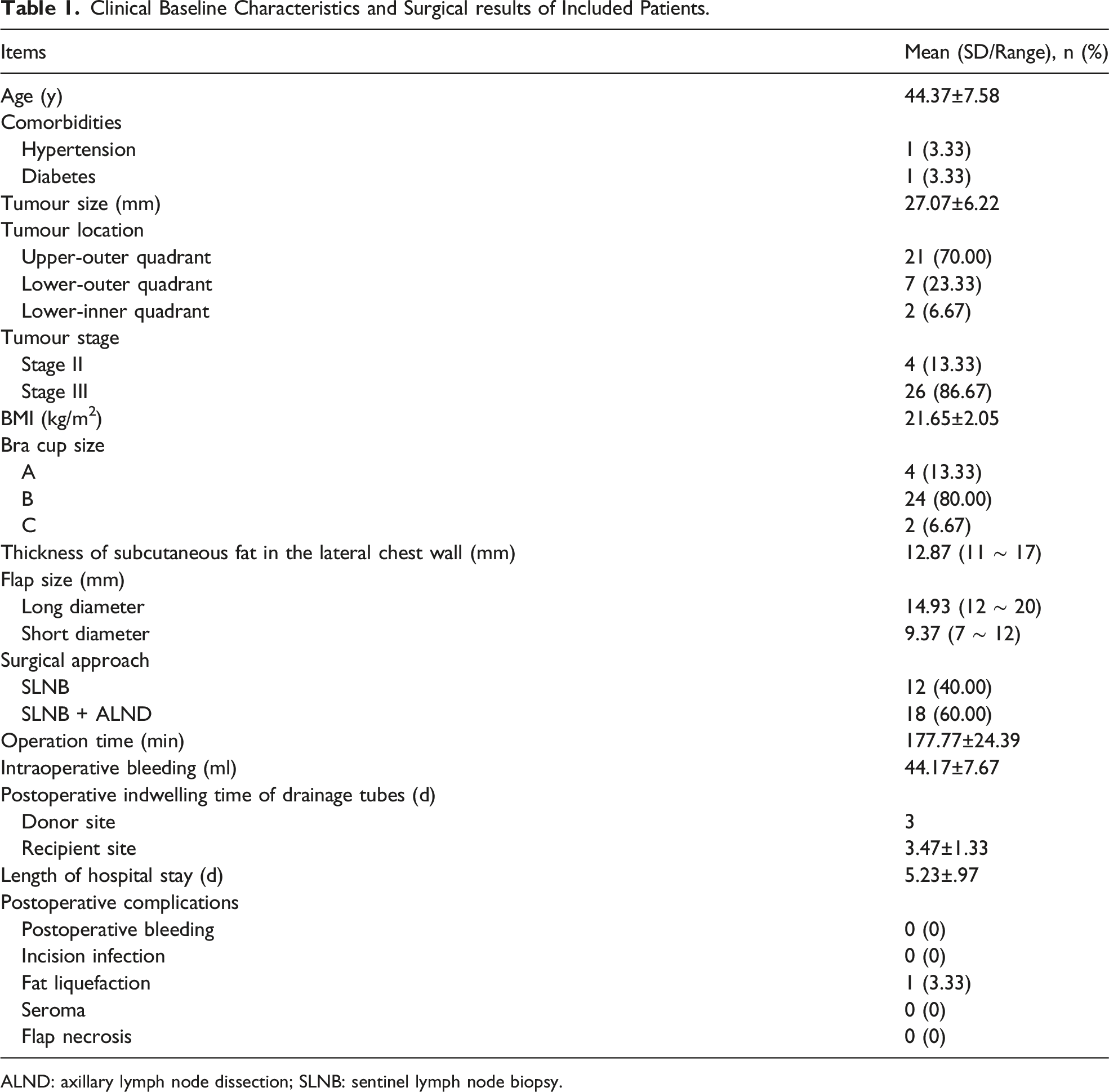
ALND: axillary lymph node dissection; SLNB: sentinel lymph node biopsy.
Breast-Q Satisfaction Score After breast Reconstruction.
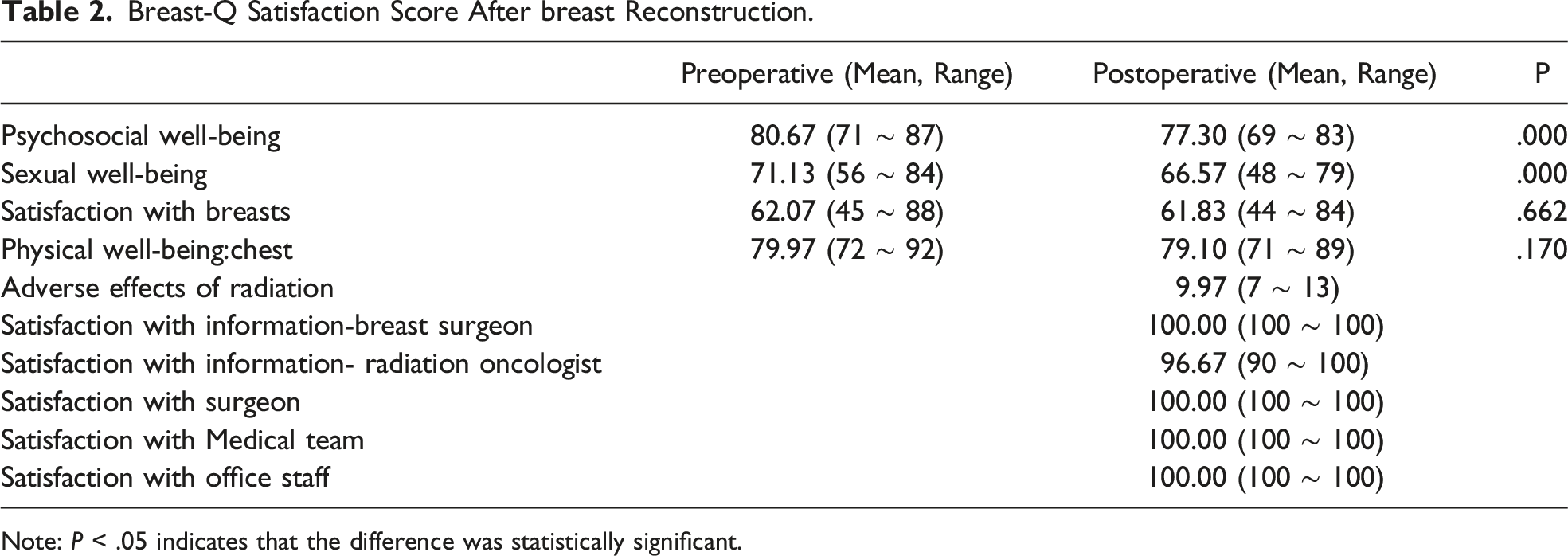
Note: P < .05 indicates that the difference was statistically significant.
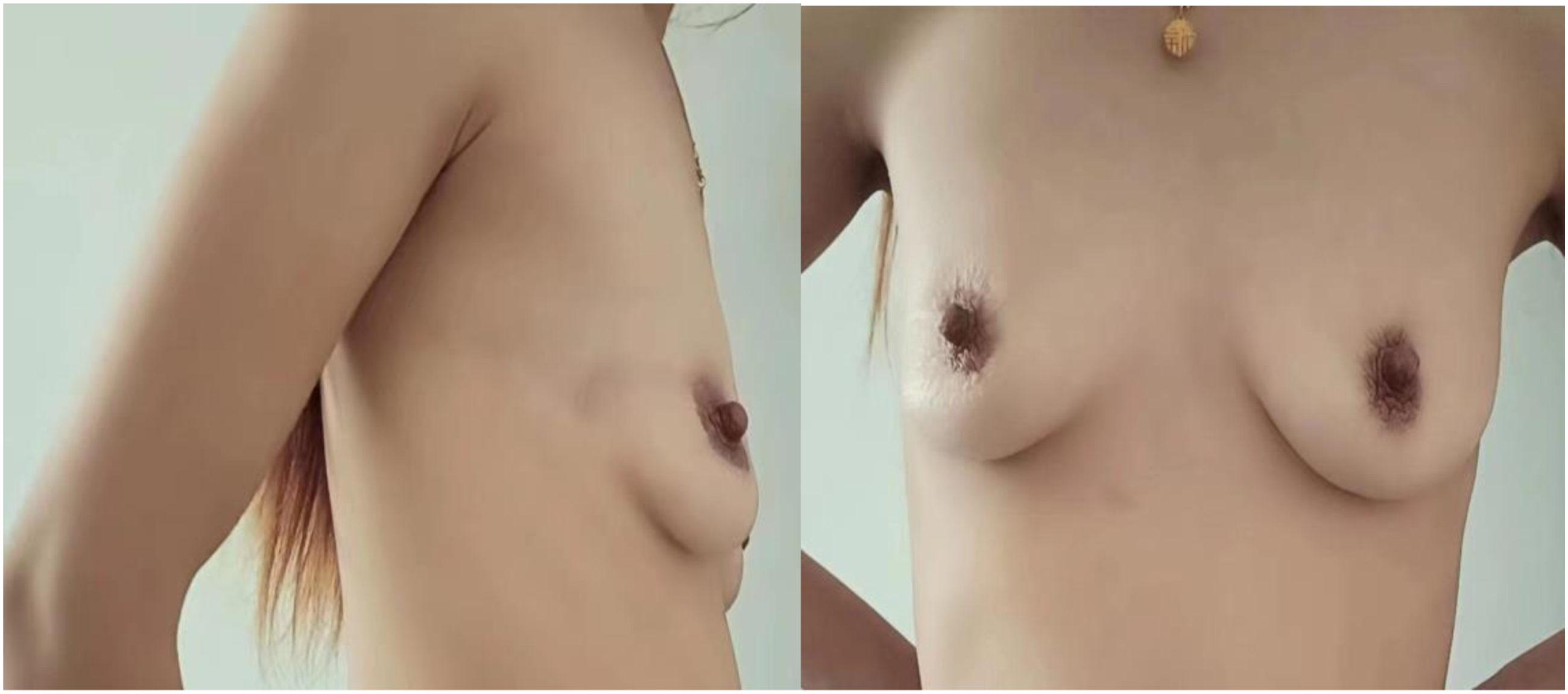
Through 16-28 months of postoperative follow-up, the breasts still had good shape, with no obvious deformity at the donor site (Figures 4 and 5), and there was no local recurrence or distant metastasis. Effect after breast reconstruction. (case 3). Breast appearance 18 months after surgery. Effect after breast reconstruction. (case 4). Breast appearance 18 months after surgery.
Discussion
At present, most domestic experts regard the surgical margin>5 mm as the safe margin standard for breast conserving surgery, but for T2-stage tumors, 20% of the patients with conventional breast conserving surgery have a surgical margin<2 mm, with a positive margin rate of 8.0%-16.6%. 7 Oncoplastic breast surgery can remove more breast volume, more easily obtain a negative margin, and further reduce the local recurrence rate, Clough et al showed that the 5-year local recurrence rate of breast cancer patients after conventional breast conserving surgery is 9.4%, and the 5-year local recurrence rate after oncoplastic breast surgery is 3%. In this study, breast quadrant resection was performed in breast conserving surgery, the scope of resection includes 2 cm of the tumor edge, surface skin, and pectoralis major fascia, and pectoralis major fascia and all patients did not have positive margins. Due to the short follow-up time, there was no case of local recurrence at present.
On the small and medium-sized breasts of women in East Asia, the volume of breast that needs to be removed for breast conservation of T2 breast cancer is more than 10%-30%. Some studies have confirmed that 8 breast deformity and breast asymmetry are likely to occur when the volume of the removed breast is more than 20%. Even though the residual cavity can be closed by direct suture of the residual breast tissue, breast gland tissue flap transfer and other methods, although the shape of the patient's breast can be improved to a certain extent, the repair of the residual cavity is actually redistribution of breast glands. In essence, there is still a reduction of breast glands, and it is difficult to avoid the destruction of bilateral breast symmetry, It is reported in the literature that the dissatisfaction of patients after traditional breast-conserving surgery is as high as 35%. 8
The technique of using a latissimus dorsi myocutaneous flap (LDMF) for repairing breast defects and breast reconstruction has matured, but it sacrifices the normal physiological function of the latissimus dorsi, It is reported that the incidence of postoperative serum swelling in the donor site is as high as 20%,9,10 and the incidence of postoperative shoulder mobility limitation is as high as 25%. 11 The muscle-sparing latissimus dorsi flap (MSLDF) has also been described as a substitute for the traditional LD flap, used for whole or partial breast reconstruction. Its advantage is that it does not require detailed vascular anatomy, preserves 75% of the muscles, and significantly reduces the incidence of shoulder mobility limitation and donor site seroma compared to LDMF. 12 However, TDAPFs are a type of flap with less damage to the donor site and fewer complications. With the development of microsurgical techniques, TDAPFs without the latissimus dorsi have become more common. The thoracodorsal artery arises from the subscapular artery, runs downward, and gives off branches such as those that run through the teres major, serratus anterior, and latissimus dorsi, as well as muscular branches and perforators after entering the latissimus dorsi. The lateral branch of the thoracodorsal artery gives off 2-3 perforators. According to current literature,13-15 the first perforator is located roughly 8 cm below the posterior axillary fold and 2-3 cm medial to the lateral border of the latissimus dorsi. The second perforator is generally located 2.5-4 cm below the first perforator, but there are still variations in the location, diameter, and number of perforators between individuals, so the localization of perforators and perforator points requires modern imaging techniques. In practical clinical application, high-frequency colour Doppler ultrasound is more non-invasive, economical, convenient, and accurate than tomography (CT), magnetic resonance imaging (MRI), and angiography. 16 TDAPF consists of skin and superficial fascia. It completely preserves the thoracodorsal artery and thoracodorsal nerve and does not affect the function of the latissimus dorsi. Compared with LDMF or even MSLDF, TDAPF has a significantly reduced incidence of seroma and limitation of shoulder movement. 11 The wound can be directly sutured, which is more aesthetic and concealed. TDAPF has a reliable blood supply and long vascular pedicle, and it provides a flap with a maximum area of 15 × 25 cm. 17 In this study, the average flap area was 9.37 × 14.93 cm, and the maximum flap area was 12 × 20 cm, which is easily enough for the repair of defects after breast-conserving surgery for T2 breast cancer.
Summary of Articles in Classifcation.
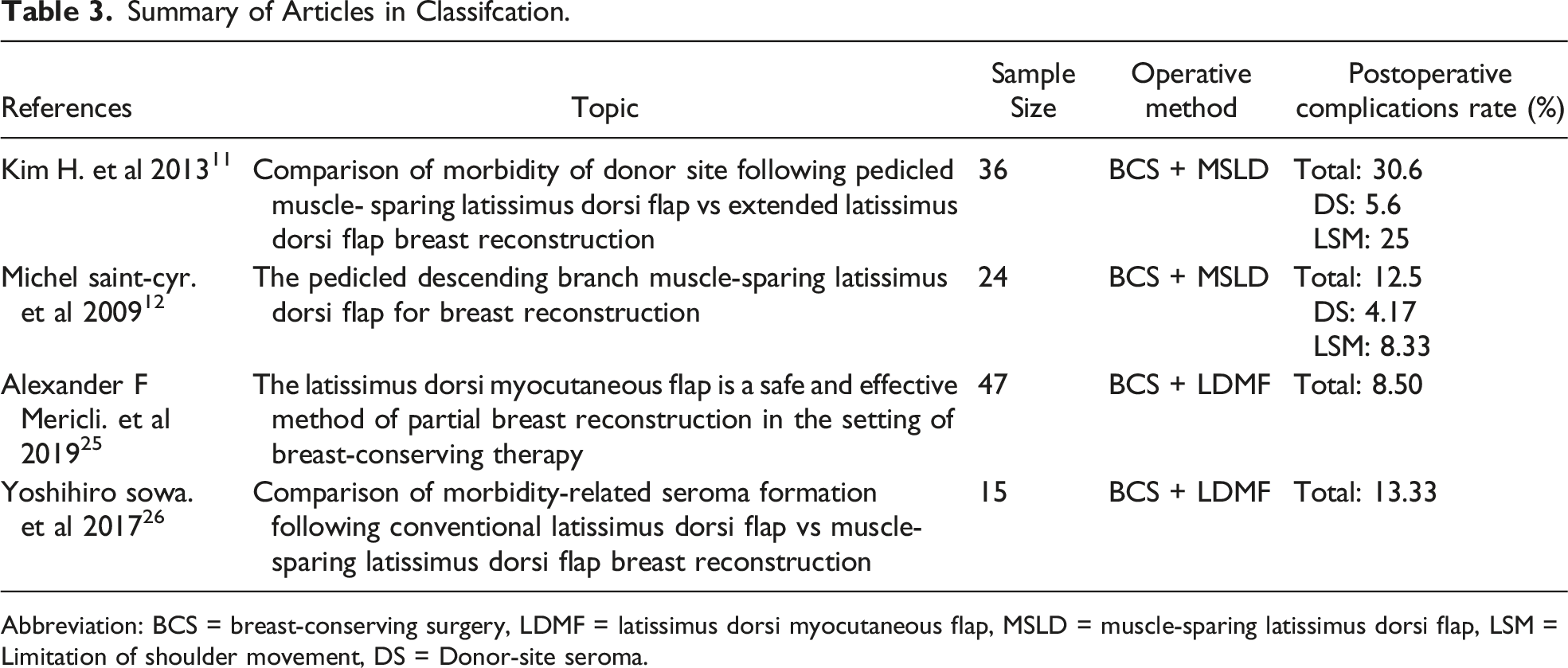
Abbreviation: BCS = breast-conserving surgery, LDMF = latissimus dorsi myocutaneous flap, MSLD = muscle-sparing latissimus dorsi flap, LSM = Limitation of shoulder movement, DS = Donor-site seroma.
All patients in this study underwent immediate reconstruction and underwent adjuvant radiation therapy after surgery, Immediate reconstruction of autologous tissue followed by adjuvant radiotherapy may lead to complications of some skin flaps, including skin flap volume atrophy, fat necrosis, fibrosis, etc. Although delayed reconstruction can avoid skin flap complications caused by radiotherapy, immediate reconstruction can bring better appearance, reduce the number of surgeries, and increase patient satisfaction with breast appearance. 27 We believe that immediate autologous skin flap reconstruction is more widely used.
For the evaluation of patient satisfaction after breast-conserving reconstruction, the mainstream methods at present are patient-reported outcome measurement tools (PROMs), mainly including EORTCQLQ-BR23, FACT-B, BIBCQ, HBIS, and BREAST-Q,28,29 of which BREAST-Q has been widely applied in various clinical practices and studies abroad since its introduction in 2009 because of its surgical specificity, wide scope of application, and good measurement performance. In this study, BREAST-Q (BCT module) was selected to evaluate the physical health satisfaction, psychosocial satisfaction, breast satisfaction, sexual satisfaction, chest satisfaction, etc. of the women. The results showed that the scores of psychosocial satisfaction and sexual satisfaction at 6 months after operation were significantly lower than those before operation (P < .05). The breast satisfaction at 6 months after operation was slightly lower than that before operation, but with no significant difference. The scores of chest wall and breast discomfort at 6 months after operation were slightly lower than those before operation, but with no significant difference. In this study, the scores of postoperative breast satisfaction and chest satisfaction of patients were slightly lower than those before surgery, but the difference between preoperative and postoperative was not statistically significant. Thanks to the application of TDAPF breast preservation reconstruction, the appearance of postoperative breast was higher than that before surgery, and the degree of satisfaction of patients with breast was close to the state before surgery. In this study, the scores of patients' psychosocial satisfaction and sexual life satisfaction after surgery were significantly lower than those before surgery. The reason is that patients with breast cancer face not only psychosomatic changes caused by surgery, but also multiple shocks such as side effects of postoperative radiotherapy, chemotherapy and adjuvant endocrine therapy, resulting in the emergence of psychosocial and sexual dysfunction in most patients with diverse manifestations and varying degrees.
Limitations
Certainly, this technique still has some limitations. It requires a higher technical level for surgeons and has a longer operation time than traditional breast-conserving surgery. Therefore, it is still not widely carried out in breast centres in China. For patients with a small amount of subcutaneous tissue in the lateral chest wall, it cannot provide enough repair volume. In our study, flap area was the quantitative index by which we assessed flap size, which does not accurately substitute for volume. Next, we will explore the methods for assessing breast and flap volume with 3D reconstruction techniques. Lastly, with only one patient reported to have fat liquification, and sample size is too small to allow us to make an objective assessment of the incidence of this complication.
Conclusion
TDAPF, featuring a high survival rate, moderate flap area, fewer postoperative complications, and high satisfaction with breast shape after operation. For East Asian women with moderate breast size, TDAPF is a safe, effective choice for repairing defects in breast-conserving surgery for T2 breast cancer.
Footnotes
Author Contributions
Li-sheng Lin conceived and designed the study, led the graphics. Shuang-qi Li interpreted and analyzed the results, and wrote the manuscript. Zi-fang Zheng collected the patients' data. Hang Li and Jin-fan Zhang analysed data. Yan Zheng assist with graphics. All authors reviewed the clinical information presented and collaborated with manuscript writing. All authors were accountable for all aspects of the work and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project supported by the Natural Science Foundation of Fujian Province (NO.2019J01586). Open Foundation of Engineering Research Center of Big Data Application in Private Health Medicine, Fujian Province University (No.KF2020008).