
Abstract
Introduction
Cholelithiasis is one of the most common diseases encountered in gastroenterology. Laparoscopic cholecystectomy can be labelled as difficult if the surgery continues for more than 60 minutes or if the cystic artery is injured before ligation or clipping. Predicting difficult laparoscopic cholecystectomy can help the surgeon to be prepared for intraoperative challenges such as adhesions in triangle of Calot, injury to cystic artery or gall stone spillage; and improve patient counseling.
Methods
In this cross-sectional study, we evaluated 269 patients with diagnosed cholelithiasis and planned for laparoscopic cholecystectomy in the general surgery department of Civil Hospital Karachi. After approval of the institution review board of the Civil Hospital, the data of all the patients was collected along with informed consent. The patients were selected via nonprobability, consecutive sampling.
Results
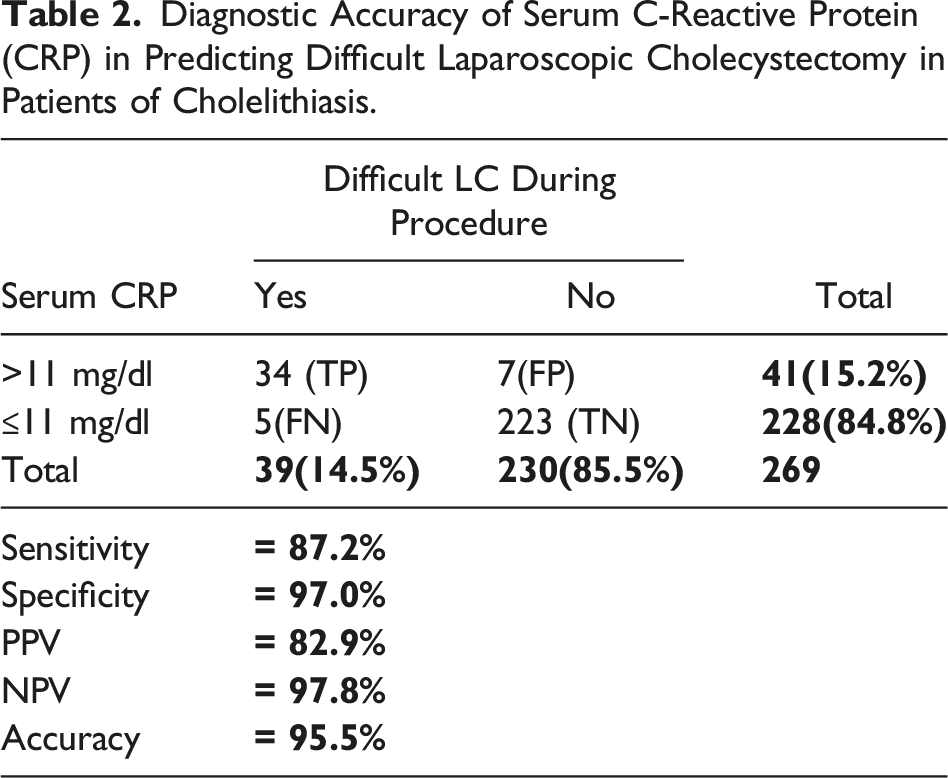
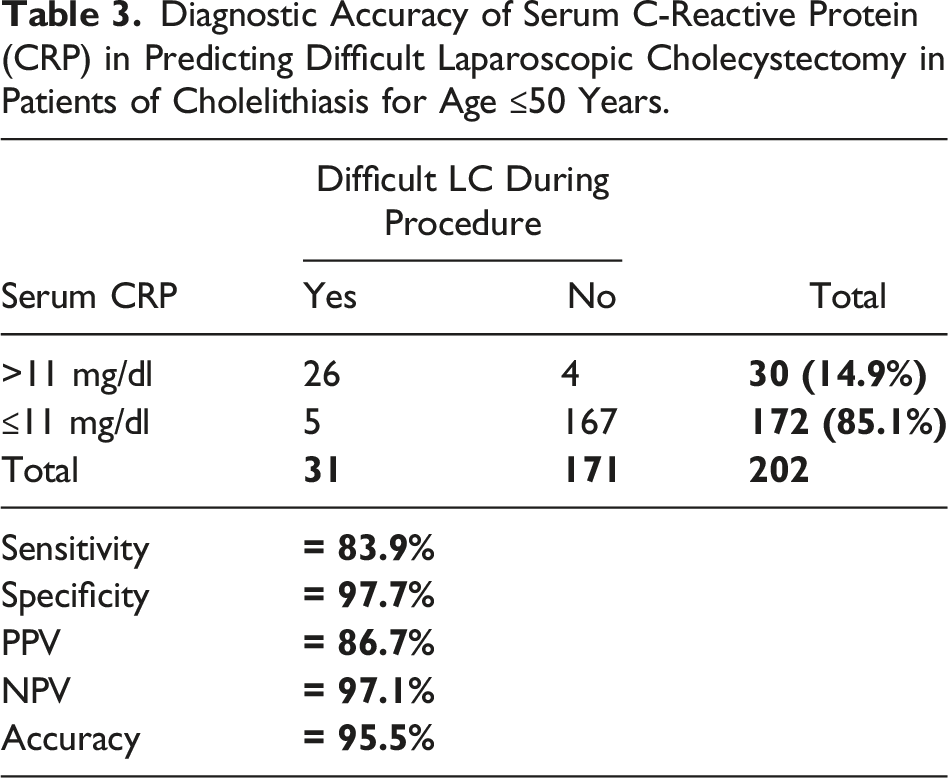
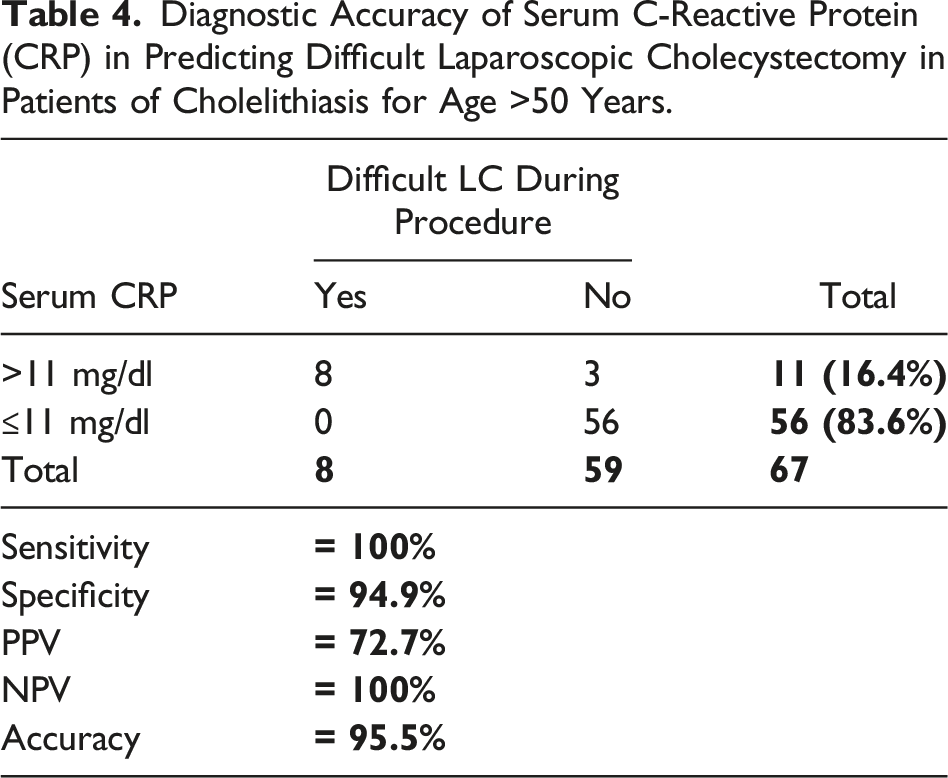
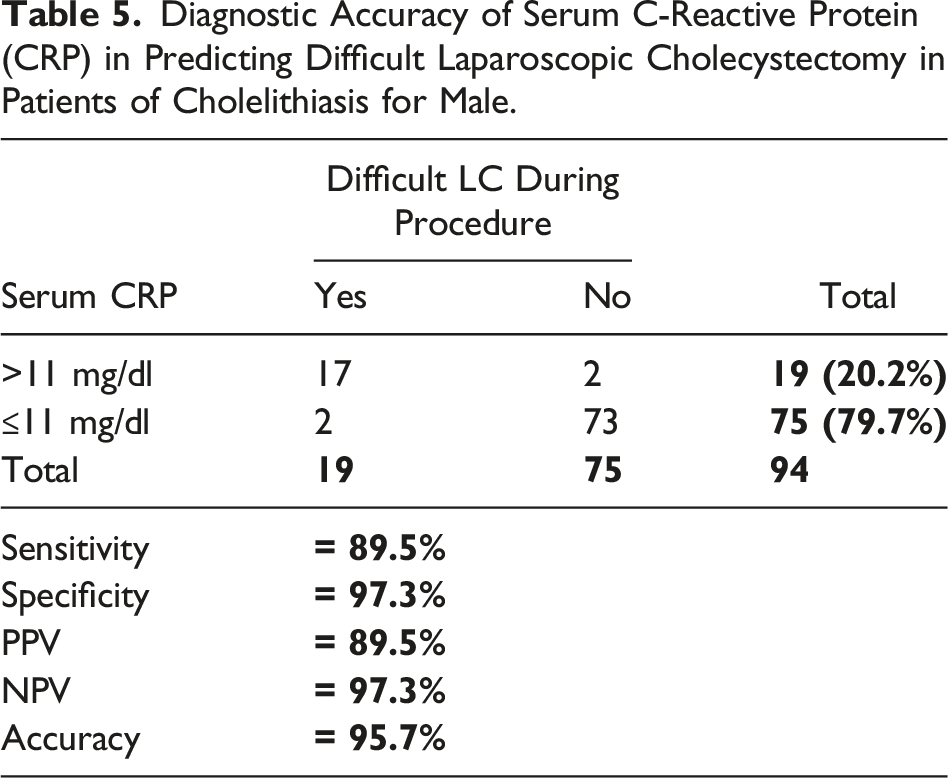
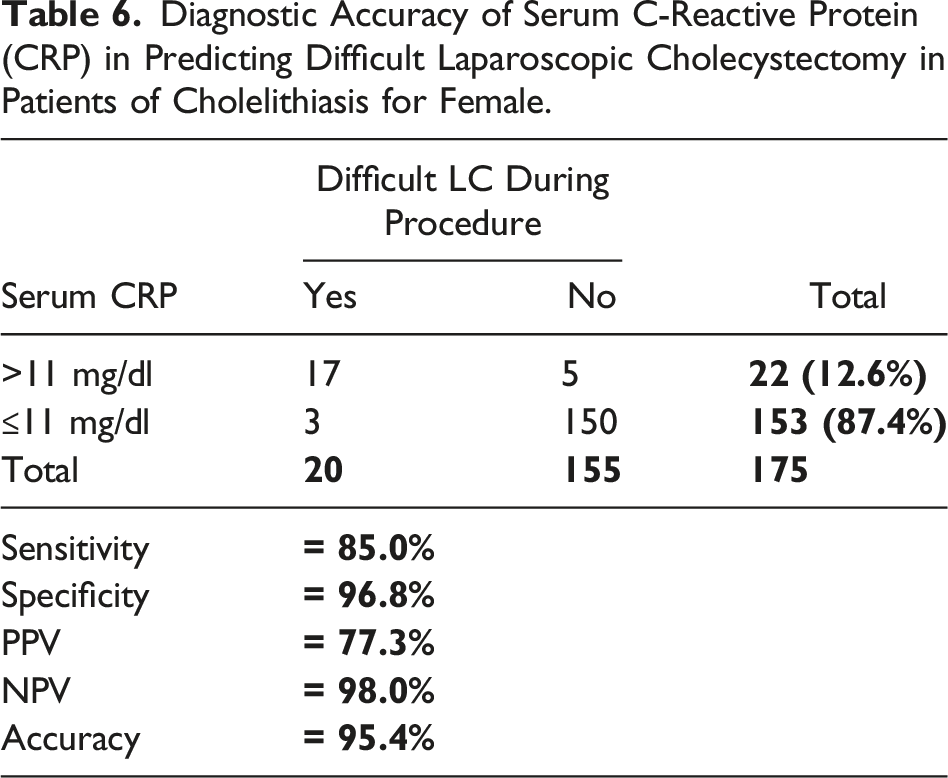
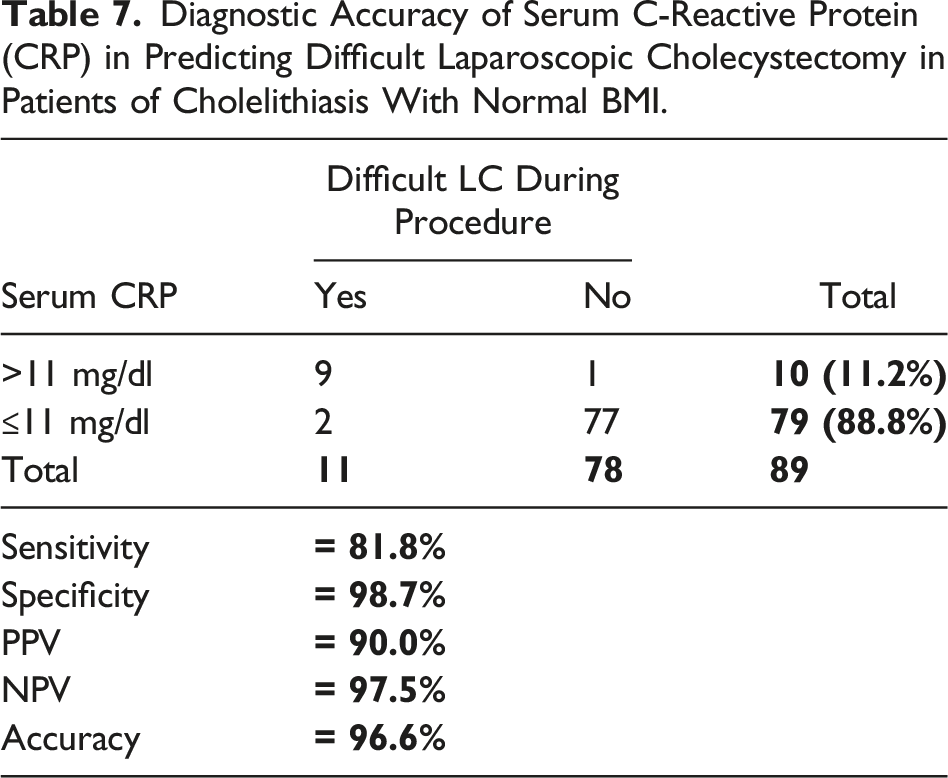
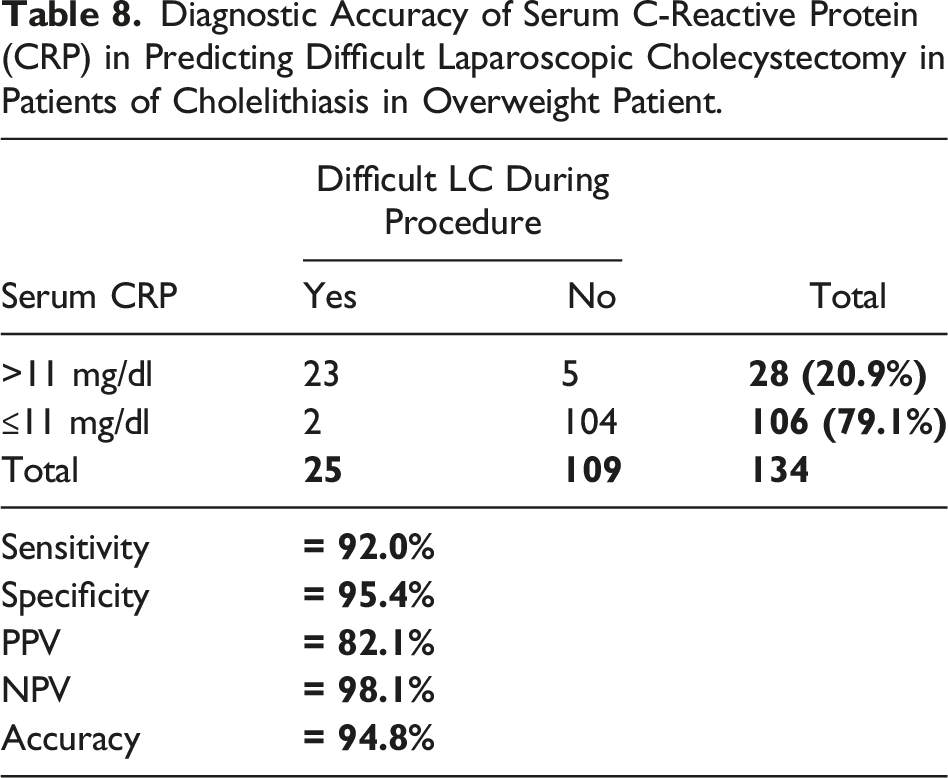
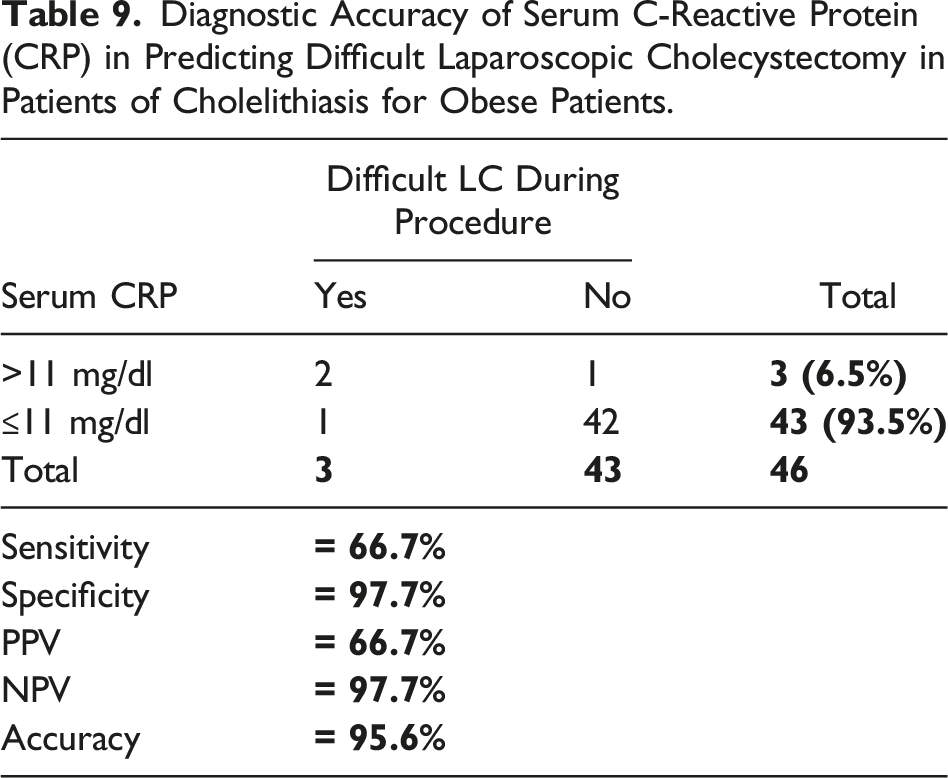
The prevalence of difficult LC during procedure was 14.5% (39/269). Contingency table showed the true positive, negative and false positive and negative observation and using these observation to compute accuracy. Sensitivity, specificity, PPV, NPV and accuracy of serum c-reactive protein (CRP) in predicting the difficult laparoscopic cholecystectomy in patients of cholelithiasis was 87.2%, 97%, 82.9%, 97.8% and 95.5% respectively. Effect modifiers like age, gender and BMI were controlled by stratification analysis and observed that diagnostic accuracy was above 90% in all stratified groups as presented in the following tables. 175 (65.06%) of 279 patients were females indicating female predominance. In general, 41 patients (15.05%) had CRP serum levels greater than 11 mg/dL out of which 34 patients had to undergo difficult laparoscopic cholecystectomy (DLC), while 223 out of 228 patients with serum CRP levels of less than 11 mg/dL did not face any difficulty during their cholecystectomy. Similar results have been acquired across all age groups and both genders.
Conclusion
C Reactive Protein is a potent predictor of difficult laparoscopic cholecystectomy and its conversion preoperatively. Patients with preoperatively high C Reactive Protein CRP levels in serum have more chances of complication intraoperatively and increased chances of conversion from laparoscopic to open surgery. Preoperative C Reactive Protein (CRP) with values >11 mg/dL was associated with the highest odds of presenting difficult laparoscopic cholecystectomy (DLC) in our study. This value possesses good sensitivity, specificity, PPV, and NPV for predicting DLC in our population.
Introduction
Cholelithiasis is one of the most common diseases encountered in gastroenterology 1 If the symptoms of cholelithiasis are persistent and recurrent then cholecystectomy is the gold standard procedure. If the diagnosis is established, then it is recommended that the individual should be referred to a surgeon within two weeks regardless of the severity of the symptoms. 1 Laparoscopic cholecystectomy (LC) is the gold standard procedure for cholecystectomy in patients with gall stones. 2 Difficult laparoscopic cholecystectomy (DLC) is faced in about 2-7% cases of laparoscopic cholecystectomy procedures. 3
Different definitions exist, but the conversion rate and iatrogenic injuries are considered frequently as indicators of a difficult procedure.4,5 Laparoscopic cholecystectomy can be labelled as difficult if the surgery continues for more than 60 minutes or if the cystic artery is injured before ligation or clipping. 4 Predicting Difficult laparoscopic cholecystectomy can help the surgeon to be prepared for intraoperative challenges such as adhesions in triangle of Calot, injury to cystic artery or gall stone spillage; and improve patient counseling. 4
Previous studies have identified predictors for Difficult laparoscopic cholecystectomy, these predictors are as follows: male sex, advanced age, acute and chronic cholecystitis, obesity, liver cirrhosis and surgical experience whereas laboratory parameters as leucocyte count and c-reactive protein. 2 There are some existing scales that evaluate the risk of conversion from laparoscopic to open surgery,6-8 but few scales that predict Difficult laparoscopic cholecystectomy. 9
C-reactive protein (CRP) is one identified as predictor of such complications. C-Reactive Protein is the first acute-phase protein to be described and is an exquisitely sensitive systemic marker of inflammation and tissue damage. 10
The aim of the present study is to determine the diagnostic accuracy of C-Reactive protein predicting difficult laparoscopic cholecystectomy in patients with cholelithiasis. There are studies which show that C-Reactive Protein is a predictor of difficult laparoscopic cholecystectomy in some cases.11-13
Materials and Methodology
Diagnostic accuracy of serum CRP was measured by using following formulae; ➢ Sensitivity = ➢ Specificity = ➢ Positive Predictive Value (PPV) = ➢ Negative Predictive Value =
Where: ➢ True Positive (TP): Patients with serum CRP >11 mg/dL and labelled as difficult LC by surgeon. ➢ True negative (TN): Patients with serum CRP ≤11 mg/dL and labelled as difficult LC by surgeon. ➢ False Positive (FP): Patients with serum CRP >11 mg/dL and labelled as normal LC by surgeon. ➢ False Negative (FN): Patients with serum CRP ≤11 mg/dL and labelled as difficult LC by surgeon.
The cut off value of serum CRP levels which predict difficult laparoscopic cholecystectomy is 11 mg/dL as determined by Receiver-operating characteristic (ROC) curve with a confidence interval of .96 in the study conducted in 2017. 3 There are major discrepancies in the selection of cut off values across the literature mainly due to different inclusion criteria and complications of cholecystitis which may elevate the CRP to more than 100 mg/dL. Since we have included grade I and II (Tokyo guideline) we selected this value proven in the aforementioned study. Furthermore there is a dearth of literature on DLC.
Moreover, the criteria set for DLC in this study closely resembles the one set in the study by Díaz-Flores, A. et al. 3
Study Design
In this cross-sectional study, we evaluated 269 patients with diagnosed cholelithiasis and planned for laparoscopic cholecystectomy in the general surgery department of Civil Hospital Karachi. After approval of the institution review board of the Civil Hospital, the data of all the patients was collected along with informed consent. The patients were selected via non probability, consecutive sampling.
Patients who were included were male and female between the ages 18-60 years old. Only those with an established diagnosis of cholelithiasis (by clinical and laboratory parameters) and planned for laparoscopic intervention were included. Those with liver cirrhosis or who were on immunosuppression drugs were excluded from this study. All emergency cases such as empyema of the gall bladder, perforated or gangrenous gall bladder were also excluded from this study.
Laparoscopic cholecystectomy that took more than 120 minutes (2 hours) and was performed upon grade I (mild) and II (moderate) of Tokyo guidelines with any incidence of bleeding was labelled as difficult laparoscopic cholecystectomy (DLC) in our study. This criterion was set keeping in mind the technical expertise of the operating surgeon and technical difficulties during the procedure. There is no set definition of DLC in the literature and it is highly subjective.
Before laparoscopic cholecystectomy (LC) venous blood samples were taken and sent to the central laboratory of the hospital for measurement of serum CRP levels. LC was done in all patients by consultant general having a minimum 3 years of laparoscopic surgeries experience or surgical residents under direct supervision of a surgeon with 3 years of laparoscopic surgery experience. Difficult LC on the basis of serum CRP levels and during surgery was labelled according to the criteria given in the operational definitions. Data regarding patient’s age, gender and body mass index (BMI) will also be noted. All the gathered information was noted on a pre-designed Proforma (Annexure-I).
Data Analysis
Data collected was analyzed through computer software SPSS 20.0. Mean and standard deviation was calculated for quantitative variables i.e. age. Frequency and percentage was calculated for qualitative variables i.e. gender, difficult LC on CRP and during surgery. 2 × 2 contingency table was used to calculate sensitivity, specificity, positive predictive value, negative predictive value of serum CRP in predicting difficult LC. Effect modifiers such as age, gender, BMI was controlled through stratification. Post-stratification sensitivity, specificity, PPV, NPV and diagnostic accuracy was calculated again using 2 × 2 contingency table.
Results
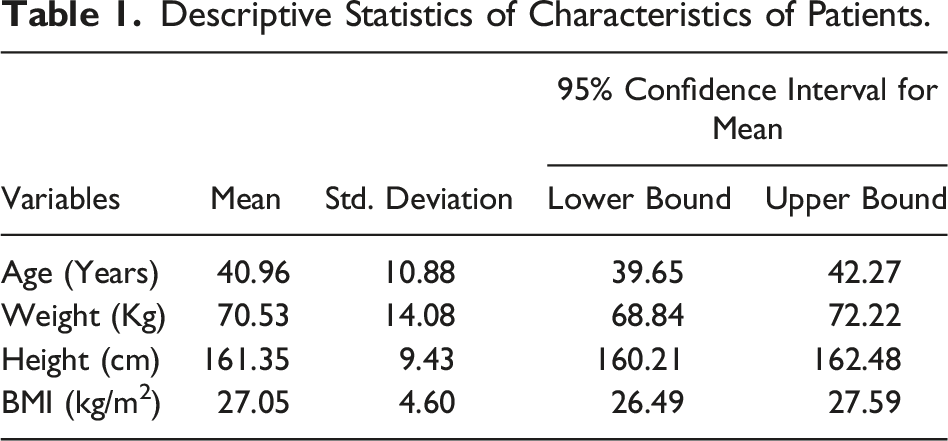
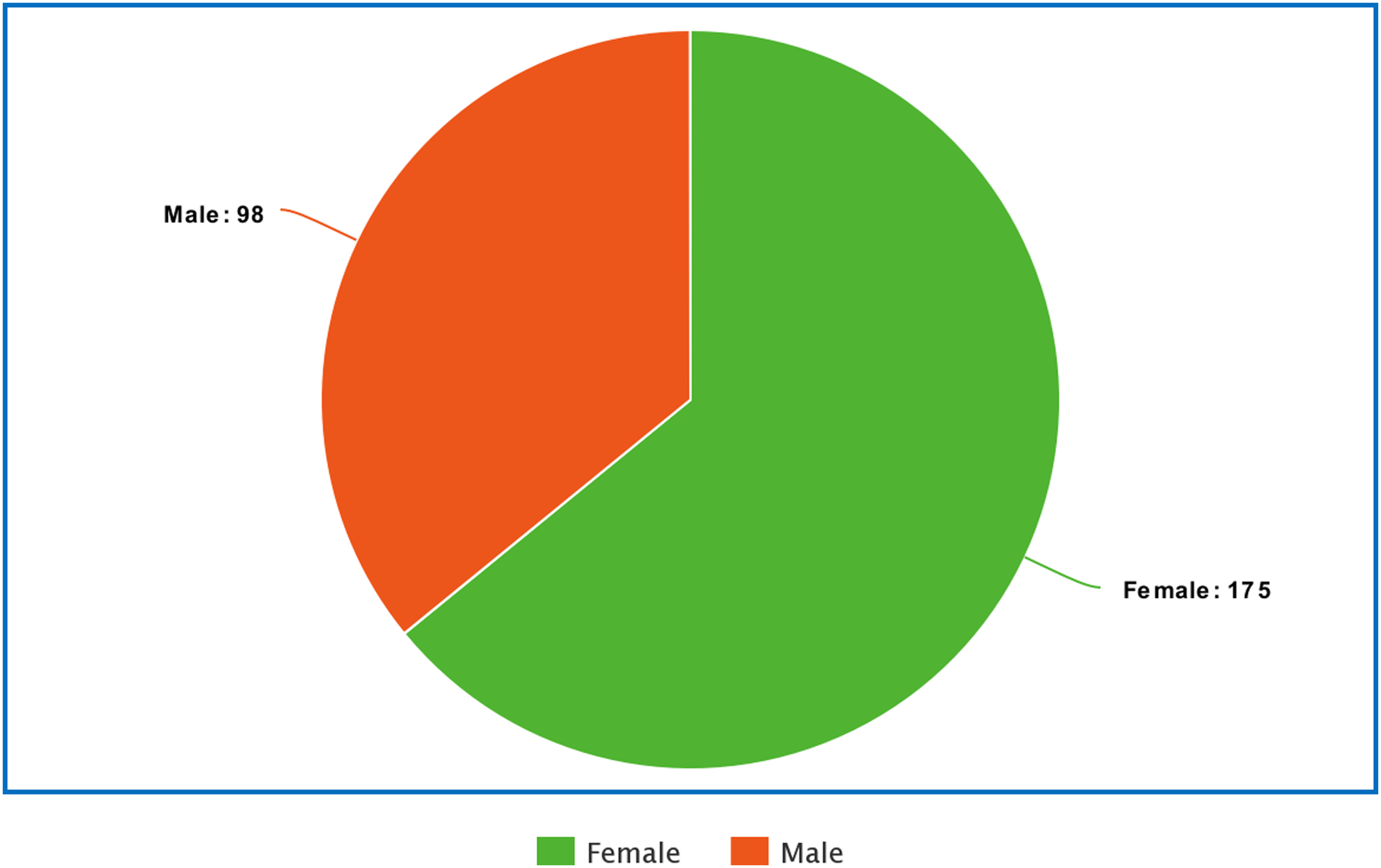
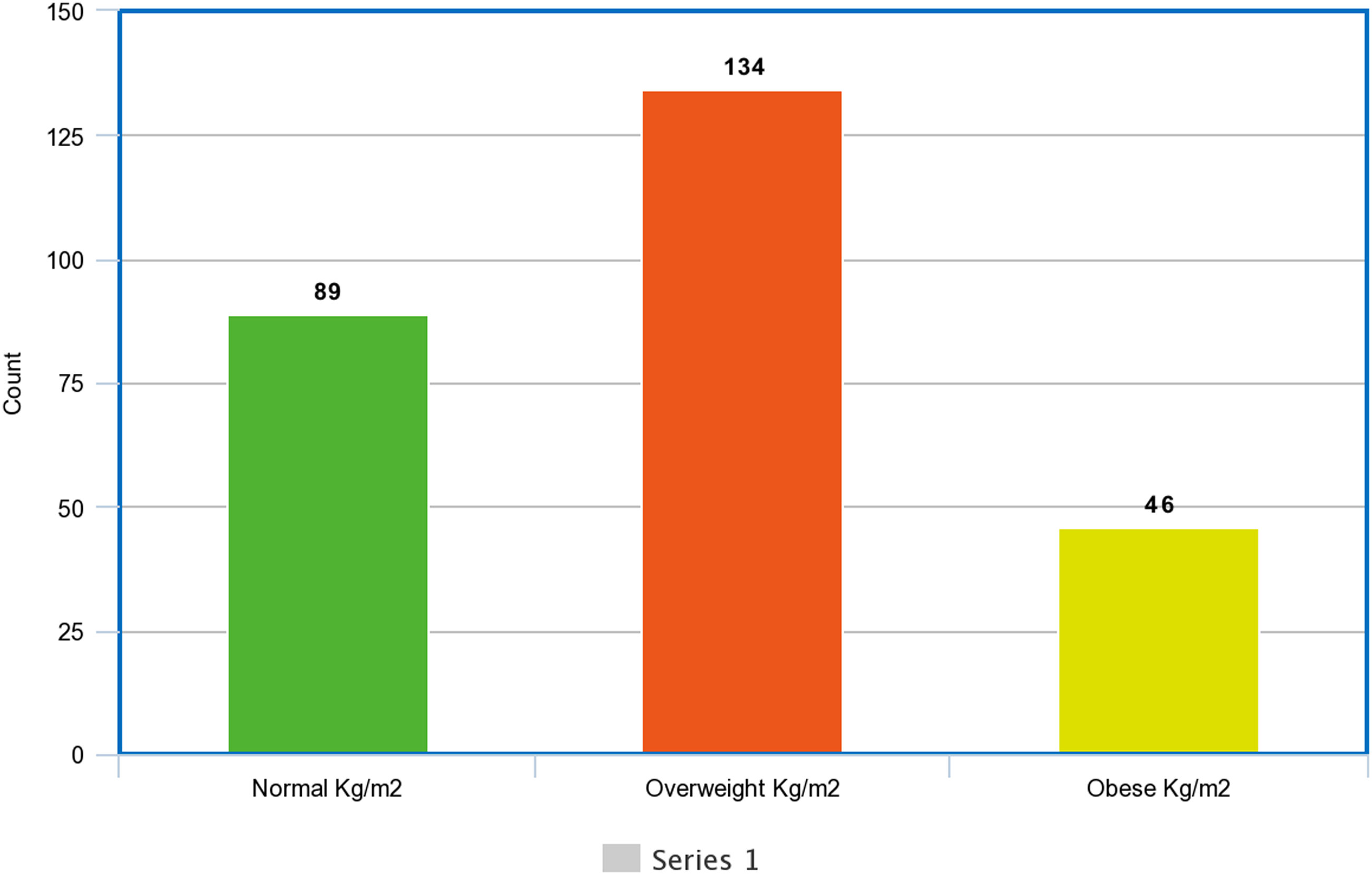
Two hundred and sixty-nine patients admitted with cholelithiasis and planned for laparoscopic cholecystectomy were included in this study. Age distribution of the patients is shown in Figure 1. The average age of the patients was 40.96 ± 10.88 years and mean BMI of the patients was 27.05 ± 4.06 kg/m2 (Table 1). There were 94 (34.94%) male and 175 (65.06%) female as shown in Figure 1. Figure 2 About 50% of the patients were overweight (Figure 3). Age distribution of the study n = 269. Descriptive Statistics of Characteristics of Patients. Gender distribution of the study n = 269. Body mass index of the study patients n = 269.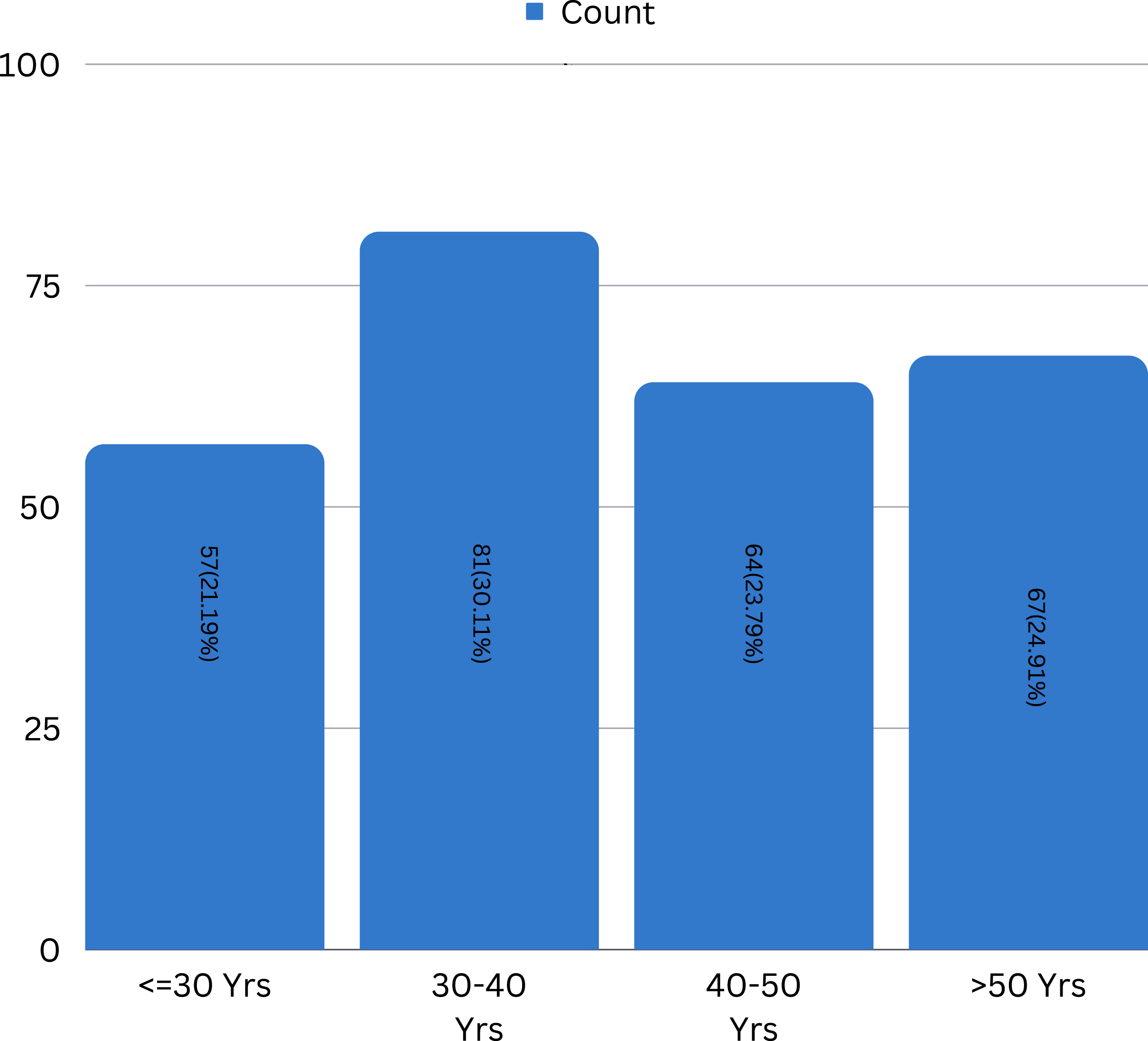
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis.
Discussion
Laparoscopic cholecystectomy is modality of choice for symptomatic cholelithiasis. 14 However, it is not rare to encounter a difficult laparoscopic cholecystectomy in this practice. A lot of studies in the past have been focused upon predicting the conversion of laparoscopic cholecystectomy into open cholecystectomy. Predicting a difficult laparoscopic cholecystectomy (DLC) can be of great value to the patient and the surgeon both by enhancing the counselling, preparing in advance for open cholecystectomy can also save time and resources of the operating team. With advancements in laparoscopic skills, conversion rates to open cholecystectomy can be further decreased if difficult laparoscopic cholecystectomy is reliably predicted.
Karim ST et al. has defined a DLC as a cholecystectomy with dense adhesions at the Calot’s triangle, inflamed gall bladder, fibrotic or contracted gall bladder, cholecystoenteric fistula or gangrenous gall bladder. 15 In his study, Lal P considered any laparoscopic cholecystectomy with tear of gall bladder, spillage of stones or consuming more than 20 minutes to dissect the Calot’s triangle as difficult. 16 Several studies argue against the timing of the surgery attributing it to the expertise or lack thereof of the surgeon.17-19 We managed to eliminate this aspect by collecting data of patients operated upon by surgeon with an experience of 5 years or residents under direct supervision of that surgeon. There are already a multitude of studies seeking key predictors of DLC in emergency procedures including age, gender, previous attacks of cholelithiasis, ultrasonography etc.9,11,13,14 Amongst the lab parameters, CRP appears to be an important predictor of DLC. However, using CRP as a predictor of DLC in elective cases is not common.
CRP is an acute phase reactant synthesized by liver under the action of Interleukin-6 and other inflammatory cytokines. Its surge can be observed in infection, inflammation, tumor, tissue infarction and several other inflammatory conditions making it a non-specific inflammatory marker. 14
In their study Diaz-Flores et al, they explored the role of CRP as a predictor of difficult laparoscopic cholecystectomy and set a cut off value of CRP serum levels of 11 mg/dL, derived by Area under the curve of ROC. 20 In his study, Karim ST has identified a lot of predictors for DLC including age, raised BMI, male gender, multiple attacks of acute cholecystitis, previous abdominal surgeries and palpable gall bladder at the time of examination. 15 Our study compares these factors as well however it fails to show a positive correlation with other factors such as age, gender, raised BMI and had a stronger correlation with CRP levels. Another study by Bhandari TR et al further affirms the aforementioned risk factors for predicting a DLC. 21 Nidoni R considers 4 factors for the prediction of DLC; Gall bladder thickness, previous attacks, pericholecystic fluid collection and TLC count of more than 11000. Gregory GC et al set a cut off value of CRP greater than 100 to predict cholecystectomy in emergency, highlighting the significance of CRP, concluding that CRP can reliably and independently predict a DLC. In contrast, our study demonstrates the value of CRP in elective cases.
Hence this study further affirms that CRP can be used to predict DLC, with an accuracy of more than 95% across all categories regardless of age, BMI, and gender.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis for Age ≤50 Years.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis for Age >50 Years.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis for Male.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis for Female.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis With Normal BMI.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis in Overweight Patient.
Diagnostic Accuracy of Serum C-Reactive Protein (CRP) in Predicting Difficult Laparoscopic Cholecystectomy in Patients of Cholelithiasis for Obese Patients.
Conclusion
C Reactive Protein is a potent predictor of difficult laparoscopic cholecystectomy. Patients with preoperatively high C Reactive Protein CRP levels in serum have more chances of complication intraoperatively. Preoperative C Reactive Protein (CRP) with values >11 mg/dL was associated with the highest odds of presenting difficult laparoscopic cholecystectomy (DLC) in our study. This value possesses good sensitivity, specificity, PPV, and NPV for predicting DLC in our population.
Footnotes
Author Contributions
Data Curation and collection: Dr Khadija Anees, Dr Ayesha Anees
Data Analysis: Dr Ayesha Anees, Dr Komal Faheem
Conceptualization: Dr Muhammad Faizan, Dr Sarush ahmed Siddiqui
Manuscript writing: Dr Muhammad Faizan, Dr Umer Bin Shoaib
Manuscript review: Dr Ayesha Anees, Dr Sarush Ahmed Siddiqui
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.