
Abstract
Objective
Clamshell thoracotomy (CST) is an emergency procedure performed during traumatic cardiac arrest. Emergency physicians and surgeons are expected to perform this procedure in the Emergency Department. However, the procedure has a low occurrence rate, therefore physicians are often poorly prepared. Current teaching methods include expensive simulators and anatomically inaccurate animal models. The goal of this study was to design, produce and test, a low-cost, high-fidelity model for the teaching of CST.
Design, Setting and Participants
The model was produced from inexpensive, commercially available materials as well as ADAMgel; a custom, recyclable, inexpensive tissue analogue. The model was tested across 19 physicians, mostly consultants and senior registrars in emergency medicine, anaesthesia and surgery. Participants completed comparative questionnaires before and after testing the model. The questionnaires were adapted from previous anaesthetic-based simulation studies and used a modified Likert scale to assess prior knowledge, anatomical realism and the teaching benefits of the model.
Results
Participants had varied prior knowledge and experience before testing the model. Results showed that 89.47% (n = 17) of trainees felt the model was a reasonable substitute for practice and 100% (n = 19) agreed that the model was a good training aid for inexperienced trainees and would recommend it to others.
Conclusions
The model proved a successful teaching tool, improving physicians’ knowledge and confidence with performing CST. This high fidelity, low cost model demonstrated that a high standard simulation teaching tool can be made which improves teaching of CST.
Introduction and Objectives
Clamshell thoracotomy (CST) is a high-acuity intervention that is indicated in resuscitation of patients in traumatic cardiac arrest, particularly those who have suffered a penetrating thoracic injury.1,2 In order to achieve good outcomes for this patient population, CST must be performed within a short time of cardiac arrest.3-5 However, the clinicians present at this time are usually emergency physicians and rarely have a background in thoracic surgery. Courses such as the Advanced Trauma Life Support course (ATLS) reference CST, but do not routinely teach the procedure, in part due to a lack of accessible simulation options.6,7 Additionally, CST is classified as a High Acuity Low Occurrence (HALO) procedure, meaning it is a ‘high-stakes’ procedure with very limited opportunities for observation or practice.2,8,9
Given these factors, it is important to explore other avenues by which clinicians may become comfortable with CST. While options for simulation of CST do exist, commercially available models are expensive and this can inhibit widespread use.7,8,10 Cadaveric teaching has also been suggested as a solution; however this is limited by the inability to perform certain interventions on cadavers (e.g., haemorrhage control),2,9 the need for specialist facilities, and that the embalming of tissue can limit realism. Animal models, while less expensive and requiring less specialist resources, have limited benefit due to anatomical limitations. 11
Objective
The objective of this study was to produce a model that could be used for simulation training of CST for emergency clinicians. The model would be anatomically accurate with appropriate tactility, reusable, and easily recreated using low-cost supplies. It would allow clinicians to simulate finger thoracostamies, the clamshell thoracostomy itself, pericardial incision and clearance, aortic compression and ‘delivery’ of the heart to facilitate cardiac compression.
Approval
The project protocol was reviewed by the Brighton and Sussex Medical School Committee for Individual Research Project (4th year medical student) and was approved as a training improvement project.
Methods
Model Design
The model was designed to be compatible with a commercially available Airway Management Trainer, such as those made by Laerdal (Figure 1). This would allow training in CST to include other interventions, such as intubation, during the same scenario, improving realism. Materials were to be low cost and readily available. We avoided the use of specialist equipment such as 3D-printed components or artificial tissues in order to promote accessibility and reproducibility. The CST model assembled without the tissue covering. The descending aorta can be seen attached to the base, the heart and pericardium are in situ, the lungs are wrapped in plastic film and the sternum is closed with zip ties.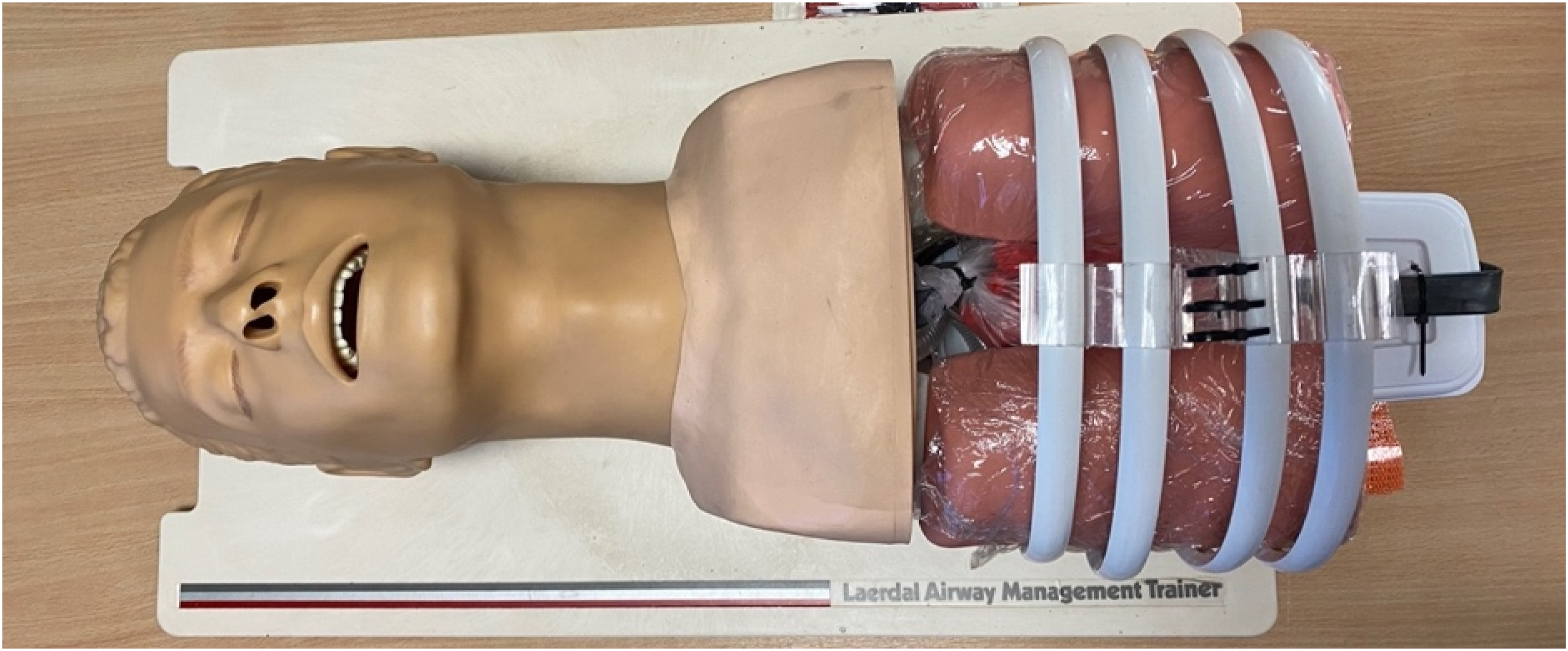
Bony Structures
Individual ribs were cut from 15 mm PVC Quadrant trim. This featured a realistic cross-sectional area (18 mm x 8 mm), a posterior groove similar to the costal groove, and could be moulded with heat to an appropriate curvature. The spinal column was simulated with a 290 mm x 120 mm × 60 mm Tupperware® box, which allowed easy insertion and adjustment of ‘ribs’. Ribs were spaced to give an intercostal space of 18 mm, which is that found in human sonographic studies. 12 The sternum was simulated with two pieces of plastic conservatory roofing material, which were joined with zip ties at the nominal 5th intercostal space. The zip ties could be replaced after each use of the model.
Viscera
To allow for trainees to practice the various intrathoracic procedures undertaken during CST, the heart and descending aorta were built into the model. The heart was simulated using a commercially available rubber model which allowed simulated compressions and was slightly larger than an actual human heart. 13 The pericardium was simulated using a polyethylene bag measuring 190 × 215 mm which could be filled with simulated blood or a simulated clot and could be easily replaced. The ascending and descending aorta were constructed using a rubber tube of 20 mm diameter. The ‘descending’ segment was filled with water using a syringe and three-way tap to simulate the compressibility of the vessel. The lungs were part of the Airway Management Trainer model, but were wrapped in polyethylene food wrap in order to simulate the visceral pleura and to create the pleural ligament.
Soft Tissues
The soft tissues were simulated using Aqueous Dietary fibre Antifreeze Mix gel (ADAMgel), a recyclable, highly realistic and low cost tissue analogue that is easily made using standard kitchen facilities.
14
Two layers of ADAMgel of differing thickness backed with muslin cotton formed the subcutaneous tissue, while the superficial skin was a simulated using an ADAMgel/gellan mixture on a muslin backing (Figure 2). These layers were self-adherent, forming a single sheet, and this was clipped to the chest model using ‘bulldog’ clips. The layers of the model’s soft tissue covering. Top – gellan and ADAMgel on muslin, ‘skin’ layer. Middle – thick ADAMgel layer on muslin. Lower – thin ADAMgel layer on muslin.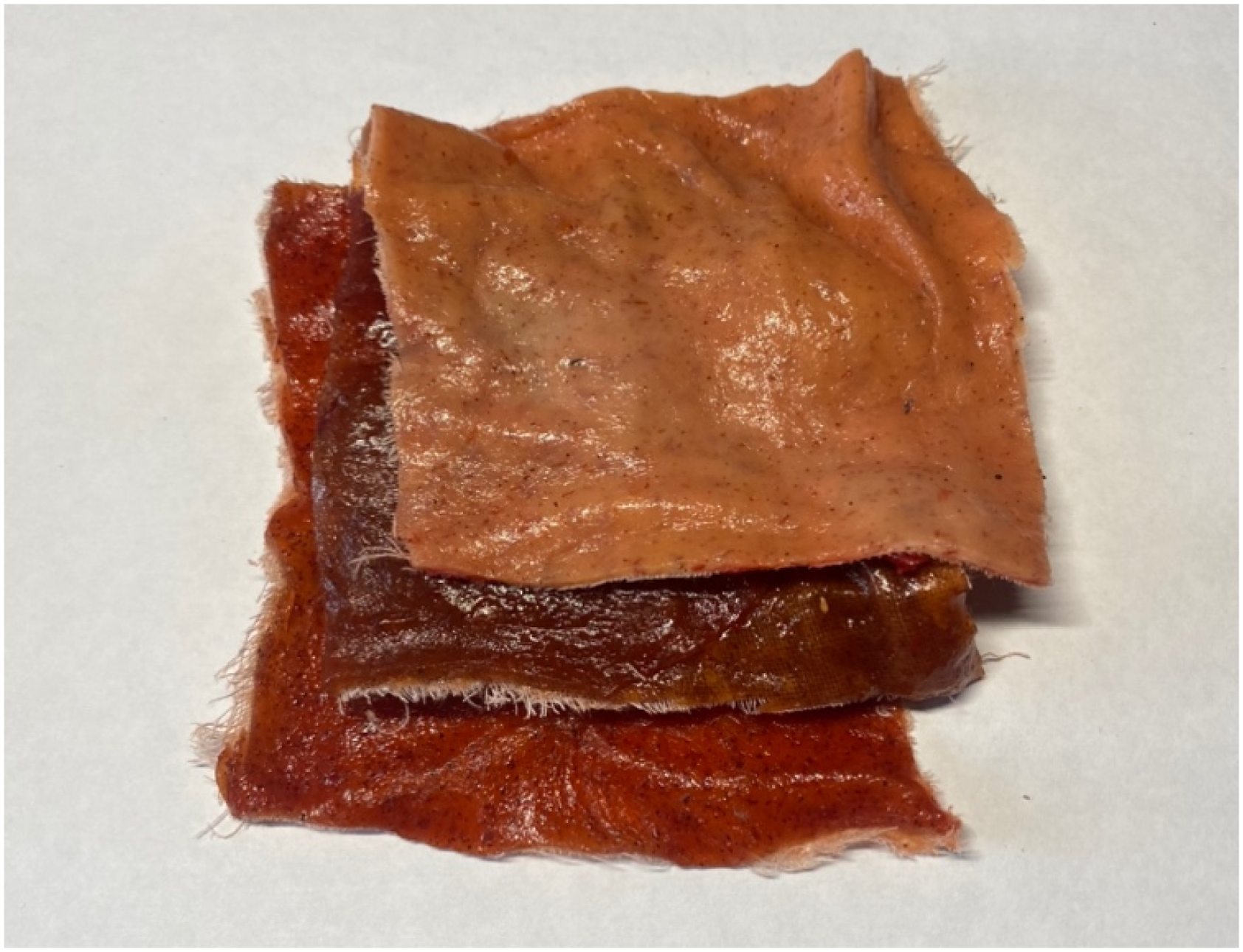
Assessment of Model
The model was assessed across two sessions. The first was a formal teaching session facilitated by an emergency medicine consultant. Trainees were asked to complete two questionnaires, one containing six ‘before’ questions and another with nine ‘after’ questions. The questions were modified from a verified questionnaire used in the previous assessments of simulation models. 15 The ‘before’ questions assessed trainees’ knowledge and confidence surrounding CST. The second questionnaire containing the ‘after’ questions was the same, however included three questions where trainees were asked to evaluate the model. The questions were in the form of statements and trainees were asked to answer questions using a modified Likert scale (1-Strongly disagree, 5-Strongly agree). The second testing session was conducted with a mix of surgical, anaesthetic and emergency medicine physicians. The session was informal and served to collect further data on the model. Physicians were asked to complete the same questionnaires as used in the previous teaching session.
Statistics
Likert data must be treated as ordinal rather than interval. Therefore, non-parametric statistical analysis is more appropriate than parametric. A Wilcoxon signed rank test was performed with the comparative data in order to ascertain statistical significance. All statistics were processed using Microsoft Excel.
Results
Model Evaluation
Evaluation of the Model’s Efficacy as a Training aid.
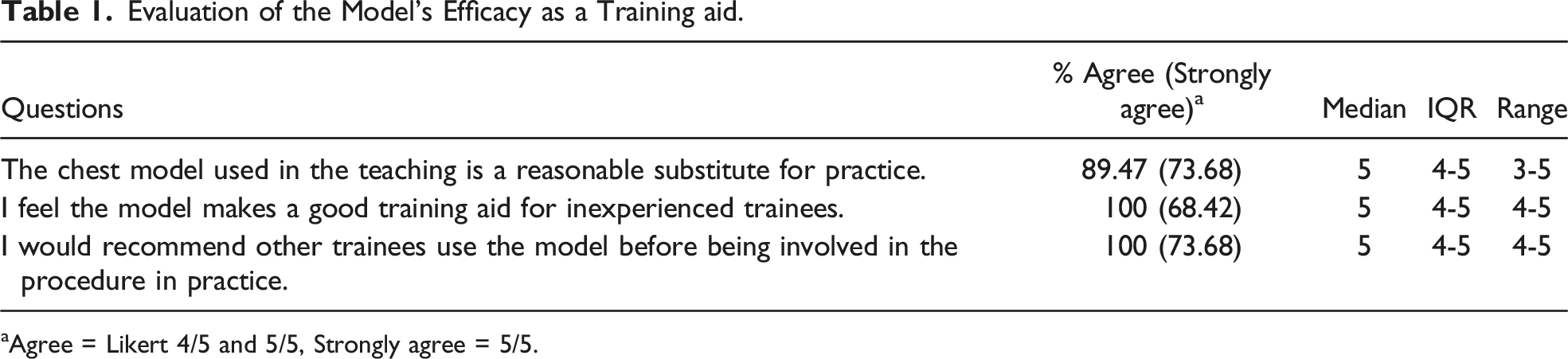
aAgree = Likert 4/5 and 5/5, Strongly agree = 5/5.
Trainee Knowledge Assessment
At both model testing sessions, physicians and trainees were asked to answer questions regarding their confidence in performing CST. There were 15 responses to these questions across both sessions, 10 from the first and five from the second. There were fewer responses to the comparative questions than to the model evaluation questions. This was due to participant error in completing the first questionnaire, prior to using the model.
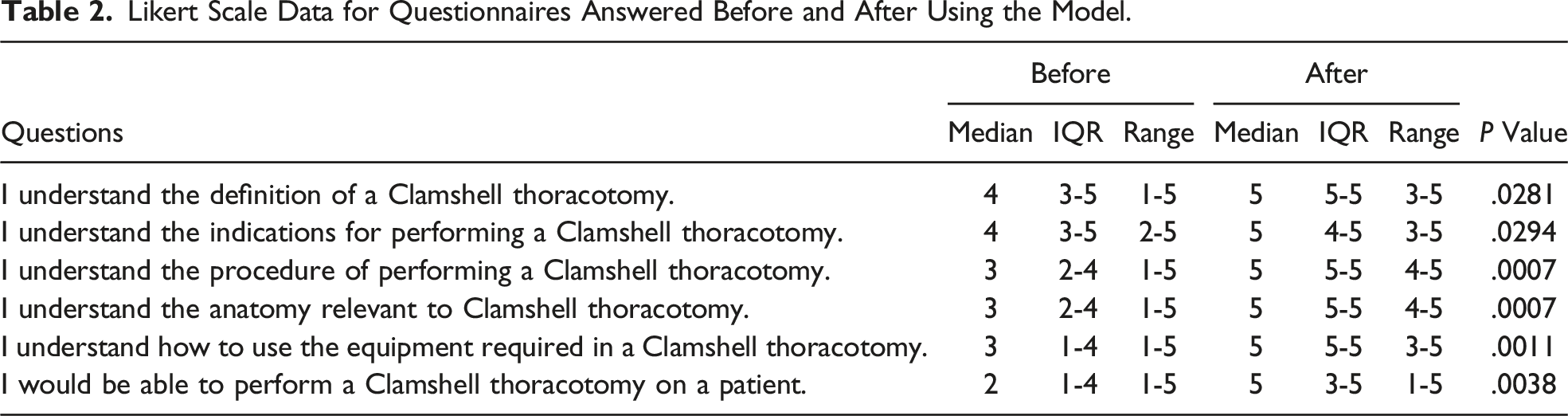
Likert Scale Data for Questionnaires Answered Before and After Using the Model.
Discussion and Conclusion
CST is a HALO procedure where simulation and education may be difficult and expensive for trainees to access, despite its timely and correct performance having the potential to be immediately life-saving. Our model is designed to assist in bridging this gap. Previous studies have shown that the use of high-fidelity simulation models in trauma and critical care can have significant benefit,10,16,17 and that non-biological models are a non-inferior method for teaching trauma skills. 18
Our results showed that participants unanimously agreed that the model was useful for inexperienced clinicians, and that it should be used before undertaking the procedure on a live patient. This is reinforced by the comparative data that shows the model improved understanding of anatomy, equipment and the steps required to undertake the procedure. Crucially, when combined with other equipment such as the Laerdal Airway Management Trainer, the model also allows simulation and teaching of the other technical and non-technical procedures required in performing CST such as intubation and crew resource management (Figure 3). The CST model being used in conjunction with other commonly available simulation equipment, allowing trainees to practice a complete traumatic cardiac arrest scenario.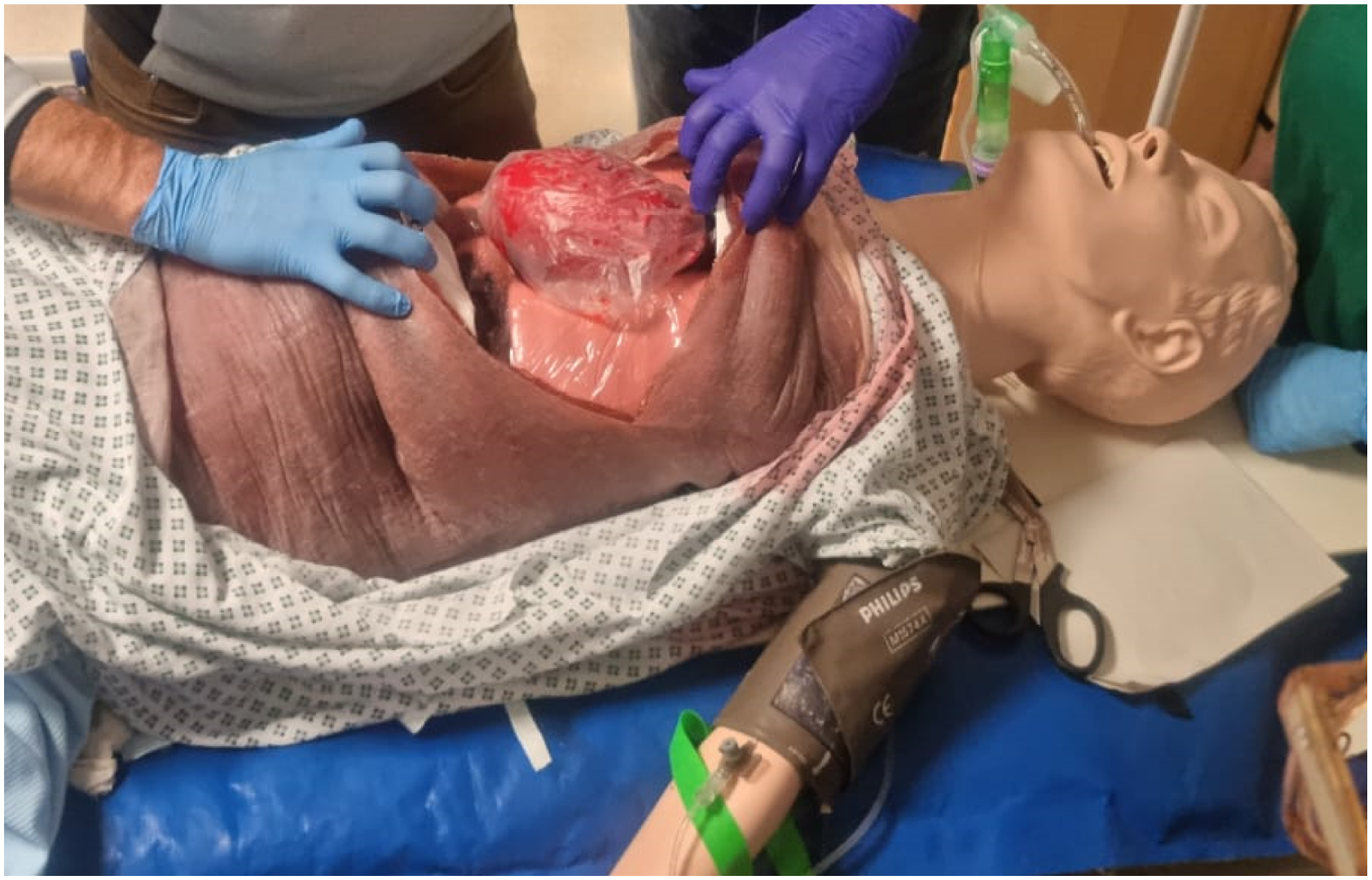
The process of designing the model centred around the steps involved in performing CST and recreating the anatomy around them. The design process aimed to incorporate realistic features, such as the ‘posterior groove’ on the PVC quadrant trim without resorting to over-complicated or expensive materials. The use of ADAMgel to create a realistic tissue analogue and filling the ‘aorta’ with liquid rather than air were other examples of this approach. Questionnaire responses do not indicate a requirement to increase the anatomical or tactile accuracy of the model. Indeed, previous simulation studies have suggested that, at a certain point increasing anatomical accuracy only further complicates the model’s assembly and increases cost.
Sustainability, ease of assembly and cost were all key considerations in the model’s design. While commercial models are available to train CST, they are expensive and limited in reusability, factors which combine to reduce both widespread access to the model and regularity of practice for those who do so.19,20 Infrequent simulation has been shown to limit the efficacy of training. 21 Our model ensured the sternum, pericardium and chest wall could be easily ‘reset’ so that another user could practice on the model shortly afterwards. Once the thoracotomy incision had been made across the tissue covering, the ADAMgel could be separated from the muslin and reused to create further coverings. This makes the soft tissue element of the model entirely reusable and recyclable. The elements of the model that could not be recycled between uses (such as the pericardium or sternal zip-ties) were deliberately designed to be low-cost and easily available.
Limitations
There are limitations of the study to consider. Firstly, there are factors pertinent to the sample. As a small pilot study, there were no calculations to ascertain the most appropriate sample size. Nonetheless, statistical significance was demonstrated across all comparative questions. The small sample size reflected the small pool of trainees available, as the study was based at one centre. Given this small size, type II errors cannot be ruled out. However, given this model was developed as a pilot study, the small sample size is not as significant a factor. The study aimed to demonstrate that a viable CST simulation model could be created using inexpensive materials. This was demonstrated through the results achieved.
It should be acknowledged that the infrequency of the procedure makes in vivo research exceptionally challenging. Therefore, trainee confidence levels and ability to assess the model may be impeded by their lack of exposure to the procedure clinically. Even experienced trainees and consultants cannot expect to be performing the procedure regularly. Therefore, it would be difficult to obtain comparative data as to whether use of the model results in improved clinical acumen.
Conclusion
Overall, the model proved a successful teaching aid for inexperienced trainees. The model maximised anatomical and tactile realism, whilst using inexpensive, widely available materials. Trainees highly recommended the model and found their knowledge and confidence surrounding CST improved following its use. Supplementary incremental design of such a model would further enhance trainees experience, and greater research into the implementation of simulation teaching of CST is required to understand its impact on clinical practice. Careful consideration of how such a teaching model is implemented within educational practices ensures that CST can be taught effectively, alongside other key facets of major trauma management.
Footnotes
Author Contributions
GC and JW conceived the project. EC constructed the model, with assistance and advice from FS, GC and JW. EC and FS drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was developed as an Individual Research Project, undertaken as part of the BMB Sprogramme, and was funded by Brighton and Sussex Medical School.